
Abstract
Autistic children are at higher risk of experiencing adverse childhood experiences, which lead to negative health outcomes such as sleep difficulties. In the general population, family resilience can help reduce the negative impact of adverse childhood experiences on child functioning. The aim of this study was to examine the impact of adverse childhood experiences on sleep duration, and whether family resilience moderates this impact in autistic children. With data from 2882 caregivers of children with autism from the National Survey of Children’s Health, we examined the role of family resilience on the relationship between adverse childhood experiences and sleep duration. As shown in previous findings, there was a main effect of adverse childhood experiences on sleep duration. There was no significant main effect of family resilience on sleep duration. Results also show that family resilience moderates the relationship between adverse childhood experiences and sleep duration, possibly serving as a protective factor.
Lay abstract
Autistic children are more likely to have sleep difficulties and to experience adverse childhood experiences. Adverse childhood experiences can include parental divorce, bullying, or witnessing violence. We also know that children in families who are resilient (e.g. families who are connected, work together, and help each other) are less impacted by adverse childhood experiences. Our study examined whether there was a relationship between adverse childhood experiences and sleep duration in autistic children. We also wanted to find out whether family resilience protects from the negative impact of adverse childhood experiences on sleep duration. We used data from 3247 parent surveys about their children that we got from the National Survey of Children’s Health. We found that children with adverse childhood experiences are more likely to get less sleep. We also found that children with resilient families were more likely to get more sleep. Our results show that family resilience helps weaken the relationship between adverse childhood experiences and sleep, so it is important to help families build resilience.
Introduction
Autism affects 1 in 36 children (Maenner, 2023). Autism is characterized by social communication difficulties and restricted and repetitive behaviors (American Psychiatric Association, 2013). Although autism is primarily characterized by difficulties in two core domains, it is also associated with many co-occurring medical and behavioral conditions, with over 95% of autistic children having one or more co-occurring conditions (e.g. anxiety, epilepsy/seizure disorder, attention-deficit/hyperactivity disorder; Soke et al., 2018). Among these co-occurring conditions, sleep problems are especially common in autistic children, with 50%–80% experiencing significant sleep difficulties (Aathira et al., 2017; Couturier et al., 2005; Richdale & Schreck, 2009).
Sleep problems
Sleep is critical for healthy development, and sleep problems in childhood are associated with worse developmental, cognitive, and emotional outcomes in the general population (El-Sheikh & Sadeh, 2015; Pyper et al., 2017). Notably, autistic children take longer to fall asleep, have decreased sleep efficiency, and generally obtain fewer hours of sleep than neurotypical children (Elrod & Hood, 2015; Fadini et al., 2015; Tse et al., 2020). A longitudinal study indicated that neurotypical children with elevated autistic traits (as measured by a cut-off score on the Autism Spectrum Screening Questionnaire) were more likely to develop sleep problems and have a lower likelihood of remission of sleep problems than children without those elevated symptoms (Sivertsen et al., 2012). While neurotypical children’s sleep difficulties are more likely to improve with age, autistic children are more likely to have worsening sleep problems over time (Verhoeff et al., 2018).
Sleep problems in autistic children are heterogenous and include sleep disordered breathing, parasomnias (e.g. sleep walking, sleep terrors), insomnia, and nocturnal enuresis (Fadini et al., 2015; Richdale & Schreck, 2009). Most sleep difficulties result in decreased overall sleep duration (Fadini et al., 2015). In autistic children, poor sleep can have significant impacts on daytime functioning (Han et al., 2022). Sleep difficulties in autistic children have been associated with externalizing behaviors including aggression, hyperactivity (Mazurek & Sohl, 2016), and self-injurious behavior (Cohen et al., 2014; Oliver et al., 2017; Park et al., 2012). Sleep disturbances in autistic children have also been associated with internalizing symptoms including anxiety (May et al., 2015; Mazurek & Petroski, 2015), depressive symptoms, and mood variability (Mannion & Leader, 2014; Mayes & Calhoun, 2009). Numerous studies have also linked sleep difficulties with higher severity of core autism symptoms (i.e. social communication difficulties and restricted and repetitive behavior; (Sadikova et al., 2022; Tudor et al., 2012). Other aspects of functioning such as adaptive behavior (Taylor et al., 2012) and quality of life (Delahaye et al., 2014; Lawson et al., 2020) have also been associated with sleep problems in autistic individuals. Ultimately sleep problems result in decreased sleep duration (Veatch et al., 2017). Improvement in sleep duration in autistic children is associated with improvement in daytime functioning, including reduction in internalizing problems and increased quality of life (for systematic review, see J. E. Hunter et al., 2020). Overall, sleep duration impacts almost every aspect of day-to-day functioning in autistic children. Thereby, it is critical to identify factors that affect sleep duration in autistic children.
Studies have found numerous predictors of sleep problems in autistic children, including mental health difficulties, higher autism symptoms, and sensory sensitivities (Hollway et al., 2013; Sivertsen et al., 2012). Yet, most studies have focused on the individual characteristics of the child, without considering the role of family or contextual factors in sleep among autistic children. In a recent literature review, Schreck and Richdale (2020) reported that environmental factors can have significant impacts on sleep duration in autistic children, but are understudied.
Adverse childhood experiences and sleep
Adverse childhood experiences (ACEs), such as maltreatment, parental divorce, bullying, exposure to neighborhood violence, or discrimination based on race/ethnicity are associated with sleep difficulties in neurotypical individuals (Chapman et al., 2013; S. C. Hunter et al., 2014). Kelly and colleagues (2020) also conducted a systematic review and found an association between ACEs and childhood sleep problems in the general population. Furthermore, there is evidence that these sleep difficulties persist into adulthood. In another systematic review of 30 studies, Kajeepeta and colleagues (2015) found that ACEs in childhood were strongly associated with adult sleep disorders. In the general population, ACEs have been an important factor to consider in the context of sleep. However, the reason for the relationship between ACEs and sleep in the general population is less known. These mechanisms have been suggested to be biological (e.g. cortisol-releasing hormone disruption after experiencing ACEs that impacts sleep), psychological (e.g. trait anxiety resultant from ACEs impacts sleep), and social (e.g. ACEs disrupt family functioning that impacts a child’s sleep; Kajeepeta et al., 2015).
Notably, autistic children are more vulnerable to ACEs than neurotypical children (Hoover & Kaufman, 2018; Rigles, 2017). Autistic children are more likely to experience bullying (Maïano et al., 2016) and maltreatment (McDonnell et al., 2019). In addition, autistic individuals who have other intersecting marginalized identities (e.g. being Black and autistic) may experience discrimination and additional barriers to existing systems (Bishop-Fitzpatrick & Kind, 2017; Straiton & Sridhar, 2022). Discrimination is also consistently associated with poorer sleep outcomes (for review, see Slopen et al., 2016). Although autistic children are more vulnerable to ACEs, only one study has examined the impact of ACEs on sleep in autistic children (Sadikova & Mazurek, in press). Sadikova and Mazurek (in press) found a relationship between ACEs and sleep duration in autistic children. Yet, the relationship between ACEs and sleep is nuanced and complex (Kajeepeta et al., 2015), and the factors that may affect the strength of this relationship have not been previously examined in the context of autism.
Family resilience
In the general population, the impact of ACEs on developmental outcomes has been described within different theoretical models. For example, stress buffering models suggest that family functioning factors, such as family resilience, can buffer (i.e. protect against) the negative impacts of ACEs (Banyard et al., 2001; Masten et al., 1999). Family resilience is the process by which family members use their strengths and connection to one another to cope with adversity (Black & Lobo, 2008; Walsh, 2012). In fact, family resilience has been shown to moderate the relationship between ACEs and various health outcomes in the general population (Okwori, 2022; Uddin et al., 2020). Using the National Survey of Children’s Health (NSCH), Uddin and colleagues (2020) found that family resilience moderated the impact of ACEs on negative mental health outcomes (e.g. anxiety, depression). Similarly, Balistreri and Alvira-Hammond (2016) also used the NSCH dataset and found that family functioning moderated the relationship between ACEs and global mental and physical health functioning in adolescents. When a child experiences ACEs, they experience stress that impacts physiological arousal (e.g. hypervigilance), and in turn, sleep, which is the opposite state of arousal (Bucci et al., 2016). Yet, family connection and resilience may “buffer” the impact of toxic stress on development, and thereby may moderate the impact of ACEs on sleep. Families of autistic children often show evidence of resilience by pulling on resources together, being connected, making meaning of adversity and affirming their strengths, and becoming more compassionate (Bayat, 2007). However, no studies have examined whether family resilience may protect against the negative impacts of ACEs in autistic children.
Purpose
Despite emerging evidence from neurotypical populations on the impact of ACEs on sleep difficulties and the moderating role of resilience, no study has examined these associations in autistic children. The aim of this study was to examine the potential moderating/protective effects of family resilience on ACEs with regard to sleep duration in autistic children, while also accounting for the effects of age, sex, race, anxiety, autism severity, overall health, and other environmental factors that could impact sleep, including school and neighborhood safety.
Methods
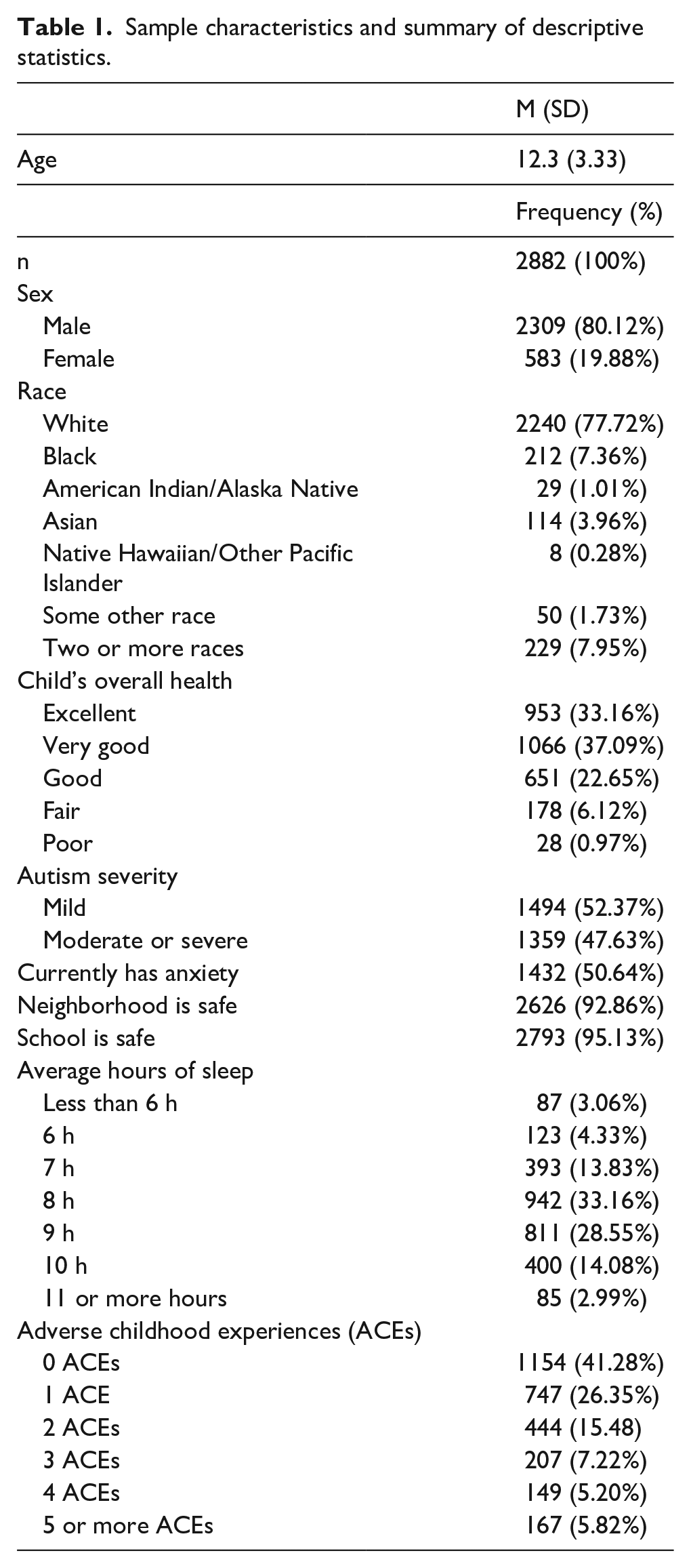
The sample included 2882 children between the ages of 6 and 17 years (M = 11.22, SD = 4.07) with parent-reported autism from the combined 2016, 2017, 2018, and 2019 NSCH (United States Census Bureau, 2016, 2017, 2018, 2019). The NSCH is a nationally distributed survey completed by caregivers of youth in the United States. Households are randomly sampled and mailed a screening survey to determine if they have children living in the household. Those with children were then invited to the full questionnaire either via mail or online. If more than one child was present in the household, a child was randomly chosen to be the subject of the questionnaire, except for children with special healthcare needs (e.g. autism), who were oversampled. Only children with a parent-reported autism diagnosis were included in the current analyses. All participants provided informed consent. There was no community involvement in the study. For sample characteristics, see Table 1.
Sample characteristics and summary of descriptive statistics.
Measures
All measures were caregiver reported from the NSCH.
Demographic information
Demographic information collected included age, sex, and race. Age was measured in years and was entered as a continuous variable. Sex was a male/female binary variable. Race options included Black, White, American Indian/Alaska Native, Asian, Native Hawaiian/Other Pacific Islander, some other race, and two or more races. Race was entered as a nominal variable using dummy coding.
Autism diagnosis and severity
Caregivers indicated whether their child had autism spectrum disorder, Asperger’s syndrome, autistic disorder, or pervasive developmental disorder as told by a healthcare professional. Only those who indicated yes and that their child currently had the condition were included in the analyses. Caregivers also reported the severity of their child’s autism as mild, moderate, or severe.
Anxiety
Caregivers were asked whether a doctor or a healthcare provider told them that their child had “anxiety problems” and whether these problems were current. Dichotomized responses (i.e. current anxiety problems, and no current anxiety problems) were used as a covariate variable in the analysis.
Neighborhood safety
Caregivers were presented with the statement “[My] child is safe in our neighborhood” and selected whether they definitely agree, somewhat agree, somewhat disagree, or definitely disagree. The responses were dichotomized (i.e. agree or disagree).
School safety
Caregivers reported whether they definitely agree, somewhat agree, somewhat disagree, or definitely disagree with the statement “[My] child is safe at school.” The responses were dichotomized (i.e. agree or disagree).
Overall health
Caregivers reported whether their child’s overall health was excellent, very good, good, fair, or poor on a single Likert-type question on the NSCH.
Sleep duration
Caregivers were asked how many hours of sleep their child received on average per night. The options were less than 6 hours, 6 hours, 7 hours, 8 hours, 9 hours, 10 hours, and 11 or more hours.
ACEs
Caregivers were asked to select whether their child had experienced any of the following ACEs: parent or guardian divorced or separated; parent or guardian died; parent or guardian served time in jail; saw or heard parents or adults slap, hit, or kick punch one another in the home; was a victim of violence or witnessed violence in their neighborhood; lived with anyone who was mentally ill, suicidal, or severely depressed; lived with anyone who had a problem with alcohol or drugs; treated or judged unfairly due to race/ethnicity; and severe poverty (family not having enough income to cover basics like food or housing). The answers were then summed and reported as 0 ACEs, 1 ACE, 2 ACEs, 3 ACEs, 4 ACEs, and so on.
Family resilience
Family resilience comprised four indicators. Indicators were when the family faces a problem, how often they (1) talk together about what to do, (2) work together to solve their problems, (3) know they have strengths to draw on, and (4) stay hopeful even in difficult times. The answer choices included none of the time, some of the time, most of the time, or all of the time. After examining the factor structure underlying the item responses, item response theory (IRT) was used to produce scores (described in the next section).
Statistical analyses
Data analyses were conducted with Stata 16.1 and MPlus (8.3). To model family resilience as a latent construct, we conducted a confirmatory factor analysis (CFA) to assess the factor structure. Specifically, in line with prior research (Child and Adolescent Health Measurement Initiative (CAHMI), 2020; Menezes et al., 2023; Zhang et al., 2021) and our prior theory, we fit a one-factor model and tested the fit. As expected, the unidimensional model had adequate fit (comparative fit index (CFI) = 0.986, root mean square error of approximation (RMSEA) = 0.096, standardized root mean square residual (SRMR) = 0.024). Given the results of the CFA, we calibrated item parameters and produced scores using a unidimensional 2 parameter logistic (2 PL) IRT model. We then produced scores with that model using expected a posteriori (EAP) scoring, which is a Bayesian shrinkage estimator (Bock & Mislevy, 1982). These individual IRT-based scores served as our estimate of the latent trait (i.e. family resilience). This approach is preferrable to simply summing the four family resilience indicators because it allows each item to have its own weight when producing scores and, thereby, avoids a host of assumptions implicit in sum scores that often are not warranted (McNeish & Wolf, 2020; Soland et al., 2022). Once family resilience scores were produced for each individual, we then used a multiple regression model to examine the association between the variables of interest. The sleep duration variable (i.e. parents selected less than 6 hours, 6 hours, 7 hours, 8 hours, 9 hours, 10 hours, and 11 or more hours) was normally distributed (|skewness values| < 1.0) and thereby did not require any transformation. Furthermore, visual inspection of probability and kernel density plots indicated that the regression residual values were also normally distributed.
Sleep duration (in hours) was regressed on the number of ACEs, with family resilience serving as a moderator. The regression model also accounted for the effects of age, sex, race, anxiety, autism severity, overall health, and school and neighborhood safety. Robust standard errors were calculated with Huber–White sandwich estimators to account for possible heteroskedasticity. As a sensitivity check of the findings from our main model, results did not change significantly when sleep was treated as categorical rather than continuous. All data analyzed were cross-sectional; therefore, causality cannot be ascertained.
Results
In our sample, 41.3% of autistic children presented with no ACEs, 26.3% of children presented with one ACE, 15.5% had two ACEs, 7.2% had three ACEs, and 10.7% had four or more ACEs. With regard to sleep duration, 7.4% of autistic children in our sample obtained 6 h of sleep or less, 13.8% obtained 7 h of sleep on average, 33.16% obtained 8 h of sleep, and 46.6% obtained 9 or more hours of sleep. Family resilience descriptive statistics are listed in Table 2.
Descriptive statistics of family resilience indicators.

Evaluation of whether ACEs and family resilience were associated with sleep duration, and whether family resilience moderated the relationship between ACEs and sleep duration were examined through ordinary least squares multiple regression. Results indicated that the full model accounted for a statistically significant and meaningful amount of variance for sleep duration, R2 = 0.10, F(16, 2679) = 16.45, p < 0.001 (See Table 3). We observed significant effects of age (β = −0.230, p < 0.001), overall health (β = −0.073, p = 0.001), and autism severity (β = −0.049, p = 0.012) on sleep duration in autistic children. In addition, Black (β = −0.386, p < 0.001) and Pacific Islander children (β = −0.066, p = 0.017) obtained significantly less sleep than White children. Sex, neighborhood safety, school safety, and anxiety were not associated with sleep duration. Controlling for all model covariates, the number of ACEs was statistically related to sleep duration (β = −0.066, p = 0.002), but family resilience was not (β = 0.054, p = 0.42). Notably, the interaction between the number of ACEs and family resilience was statistically significant (β = 0.041, p = 0.04). As Figure 1 shows, the relationship between ACEs and sleep duration was stronger when family resilience was low (i.e. 1.5 SDs below the mean). When family resilience is average (i.e. equals to 0) or above average (i.e. 1.5 SDs above the mean), the slope between ACEs and sleep duration is flatter, signifying a weaker relationship. Therefore, as family resilience decreases, the negative association between ACEs and sleep duration becomes stronger.
Multiple linear regression results showing the variables associated with sleep duration in autistic children.
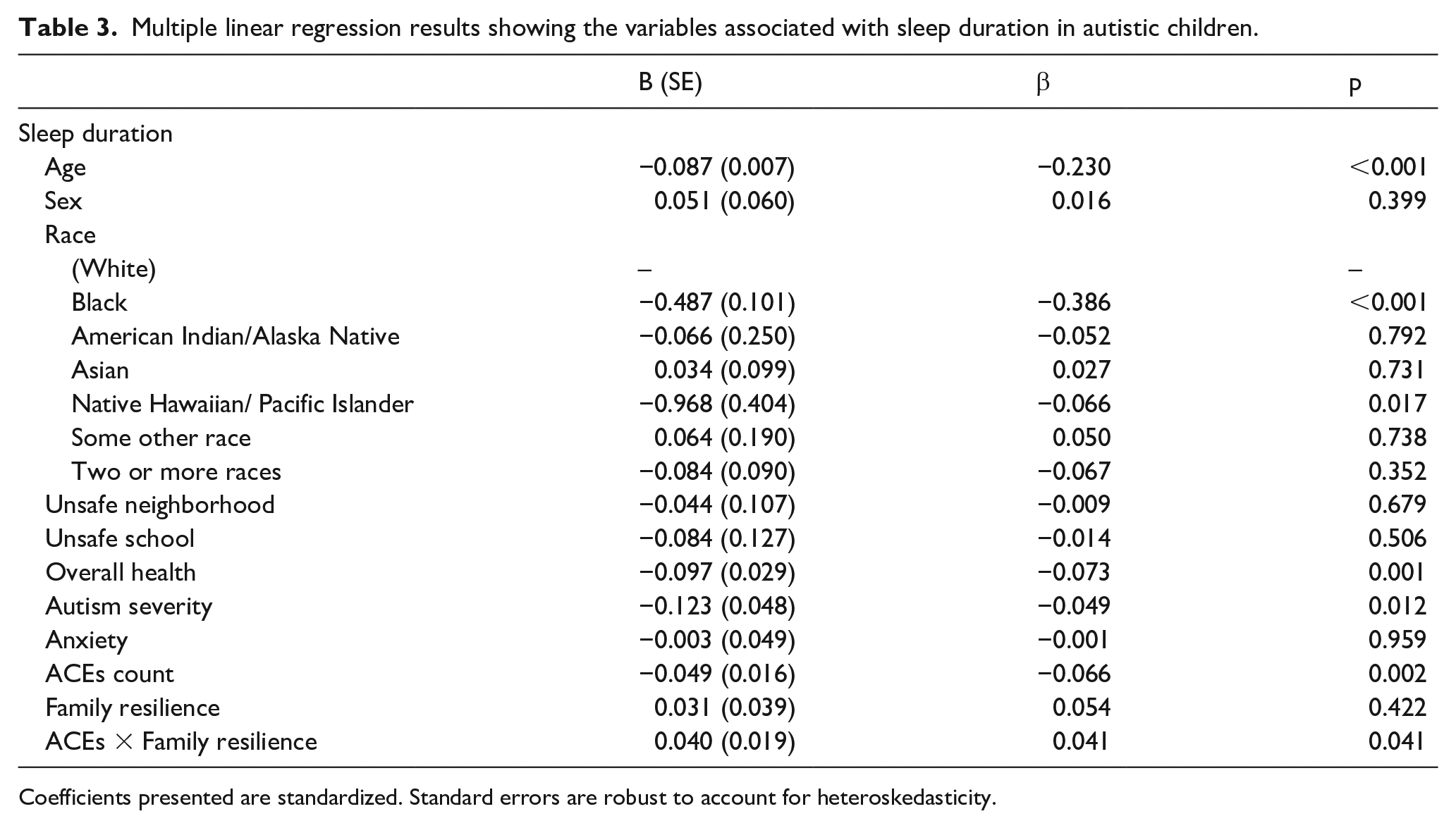
Coefficients presented are standardized. Standard errors are robust to account for heteroskedasticity.

Interaction effect between family resilience and ACEs on sleep duration.
Discussion
Autistic children face significant vulnerability with regard to sleep. They are more likely to experience ACEs (Hoover & Kaufman, 2018), have less family and individual resilience (Chang et al., 2019; Roberts et al., 2017), and have more sleep problems (Aathira et al., 2017; Chen et al., 2021; Richdale & Schreck, 2009). Our findings show that ACEs, family resilience, and sleep duration are all associated with each other, in that family resilience moderates the impact of ACEs on sleep duration. We also found that age, race, overall health, and autism severity were all associated with sleep duration in autistic children. Specifically, older children obtained less sleep than younger children, which is supported by the literature (Iglowstein et al., 2003). We also found that Black and Native Hawaiian/Pacific Islander children obtained less sleep than White children. Guglielmo and colleagues (2018) investigated racial and ethnic sleep disparities in the United States and found that Black children get less sleep than children of other races. However, despite conducting a systematic review, they did not report any sleep data on Native Hawaiian or Pacific Islander individuals, and noted that there was a scarcity of data on Asian individuals in their studies (Guglielmo et al., 2018). We also found that overall health was associated with sleep duration, which is consistent with previous findings that autistic children with worse health-related quality of life show significantly more sleep problems than autistic children without health issues (Delahaye et al., 2014). Autism severity was associated with sleep duration, with children with more severe autism symptoms getting significantly less sleep than children with milder autism symptoms. These findings are also unsurprising as there is a long-standing association between autism symptom severity and sleep difficulties (Richdale & Schreck, 2009; Sadikova et al., 2022).
Consistent with previous findings (Sadikova & Mazurek, in press), we found a main effect of ACEs on sleep duration in autistic children. In neurotypical children, the connection between ACEs and negative outcomes such as sleep problems (including decreased sleep duration) is well established (Kajeepeta et al., 2015; Yu et al., 2022), and one study has found the same patterns hold up in autistic children (Sadikova & Mazurek, in press). While the mechanisms by which ACEs impact sleep are not fully known, it has been shown that ACEs may impact cortisol regulation (Heim et al., 2000), including a lack of cortisol decline in the evening (Cicchetti et al., 2010). Neurobiologically, trauma can impact many brain functions and structures including the amygdala and prefrontal cortex, both of which are highly involved in arousal and sleep processes (Gieselmann et al., 2019). As a result of hormonal and neurobiological impacts of trauma and stress, children with ACEs exhibit hyperarousal, which naturally impacts sleep patterns (Woodall, 2021). In autistic children who are already prone to lower sleep duration and sleep problems, ACEs may exacerbate existing sleep problems.
Furthermore, our findings show that family resilience weakens the impact of ACEs on sleep in autistic children. Although studies have also shown a link between resilience and sleep quality in the general population (Arora et al., 2022), not much research has been done with autistic children, who are especially vulnerable to both ACEs and sleep problems. In the general population, the link between resilience and ACEs is generally explained by the stress buffer model, which was first introduced by Cohen and Wills (1985), who posited that social support “buffers” or protects against the negative impacts of stressful and adverse events. Specifically, they reported that rather than a “main effect,” social support has a moderating effect on the “experience of stress and the onset of psychological outcome” (Cohen & Wills, 1985, p. 312). Since then, many studies have found support for stress buffering within the context of ACEs (Brinker & Cheruvu, 2017; Jones et al., 2018; Uddin et al., 2020), though none have been conducted with autistic children. In the general population, family resilience has been shown to play a large role in helping buffer against stressful events (Bhana & Bachoo, 2011). The buffering or protective effect of family resilience comes from not only the social support that families provide but also the individual resilience that they may help foster in the child (Van Seeters, 2019). The connection and attachment that stems from family resilience can reduce the cascading negative effects of trauma and enable re-connection, safety, and recovery (Traub & Boynton-Jarrett, 2017). At a physiological level, the effect of resilience on trauma can be explained by gene–environment interactions, in that adverse events can impact the expression of genes and make an individual more vulnerable or resilient to future experiences (i.e. “steeling” or sensitization effects; Rutter, 2012). Similarly, environmental contexts such as family functioning and family resilience can in turn influence gene expression and biological responses in areas of functioning such as sleep (Bowes & Jaffee, 2013). Our findings show support that the stress buffer model may apply to autistic children as we found a significant effect between ACEs, family resilience, and sleep duration.
Notably, the resilience of families with autistic children can be qualitatively different from family resilience in neurotypical families. Roberts and colleagues (2017) used a mixed-methods approach to examine the relationship between resilience and sleep in families with autistic children with sleep problems. Qualitatively, families reported facing family stressors, such as not having the freedom of their own nighttime routine when their child consistently has difficulty falling asleep (Roberts et al., 2017). Despite these challenges, many families adapted and demonstrated resilience. For example, Roberts and colleagues (2017) describe one mother starting to attend early yoga classes since she was already up with her child. Providing families with tools and resources to manage adversity can result in an open feedback loop of gaining resilience skills and strategies (Bayat & Schuntermann, 2013). Other intervention strategies to build family resilience include increasing positive cognitive appraisal (Bekhet et al., 2012).
Our findings indicate that family resilience moderates the relationship between ACEs and sleep. Although outside the scope of this study, evidence shows that family resilience in families of autistic children can be increased with intervention (Kotera et al., 2021). Kotera and colleagues (2021) conducted a literature review of resilience interventions for families of autistic children. The authors found that cognitive factors such as internal locus of control, positive cognitive appraisal, acceptance, self-efficacy, and optimism were strongly associated with resilience and better coping strategies (Kotera et al., 2021). These skills can be developed through various individual and family therapies such as cognitive behavioral therapy (Izadi-Mazidi et al., 2015) and acceptance and commitment therapy (Blackledge & Hayes, 2006). Psychotherapy can also address mental health in family members and provide appropriate intervention (Bayat & Schuntermann, 2013). Bayat and Schuntermann (2013) also recommend parent-to-parent support programs where parents share information with each other. Although the evidence is scant, other resilience building interventions such as mindfulness-based spirituality resilience training and group resilience training can be effective for families with autistic children (Kotera et al., 2021). One of the most important ways to develop resilience is meaning-making from adversity, and it is important for providers and other supports (e.g. clergy persons) to encourage and help develop meaning out of adversity, and spirituality can be an important part of resilience (Bayat & Schuntermann, 2013).
Bayat and Schuntermann (2013) also noted the importance of resilience building for siblings, including mental health–related prevention interventions. Kuhlthau and colleagues piloted a virtual resilience training for parents and siblings of autistic children, and showed promising results in their randomized control trials (Kuhlthau et al., 2020, 2023). Such virtual trainings can even be implemented despite COVID-19 pandemic restrictions and health-related barriers. In fact, the COVID-19 pandemic has especially impacted families with autistic children (Eshraghi et al., 2020), as families faced major disruption of services as well as increased parental stress (Kreysa et al., 2022). Finally, providing families with resources such as positive behavioral supports and strategies to support autistic children is also paramount to developing family resilience (Bayat & Schuntermann, 2013).
Limitations
This study was cross-sectional, and therefore, developmental causal pathways cannot be determined. We used existing theory and literature to build our theoretical model. As this was not a longitudinal study, it is unclear whether increasing family resilience would also increase sleep duration in children. It is possible that there is a reverse association (e.g. increased child sleep duration would result in increased resilience) or that the relationship is bi-directional. Future studies should examine these constructs longitudinally. In addition, all data were parent and caregiver reported. For example, if the child had nighttime wakings that the parents did not know about, parents would not report that on the survey. In addition, while sleep duration and sleep problems are closely linked, the NSCH does not capture specific sleep problems, so extrapolation about the variables of interest on clinically impairing sleep problems is not possible. Similarly, family resilience was based on a single informant in the family. Future studies should use multi-rater reports and objective measures (e.g. actigraphy). The ACEs used in this study also do not capture the breadth of possible adverse experiences that children could have witnessed or faced (e.g. war, natural disaster). In addition, although it is extremely common to sum ACEs, it is nevertheless not necessarily appropriate to equate the impact of different ACEs (e.g. parental divorce and parental death). We recommend future studies to explore the impacts of trauma and various ACEs more deeply.
Conclusion
This is a meaningful study that found that family resilience moderates the relationship between ACEs and sleep in autistic children. These findings are the first to point to a possible moderator in the relationship between ACEs and sleep in autistic children. Resilience has been shown to moderate the negative effects of ACEs in neurotypical children, and our findings support this model in autistic children. Future research should continue exploring the moderating characteristics of family resilience and how to foster and develop it in families of autistic children. Similarly, it is important to understand the multi-faceted sleep difficulties that autistic children face and to provide necessary and individualized supports.
Footnotes
Authors’ note
Identity-first language is used throughout this article per journal guidelines and preferences of the autistic community.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.