
Abstract
Peer victimization is a widespread phenomenon especially prevalent in early adolescence. This study investigates the prevalence of peer victimization and its association with mental health problems and impact on everyday life, and the possible mediating effect of parental and peer support. Data are based on a cross-sectional health survey (N = 9,707) among adolescents (10-13 years) and their parents (N = 8,210). The Strengths and Difficulties Questionnaire was used to measure mental health problems, as well as impact on everyday life. Approximately, 17.6% of boys and 15.3% of girls reported being peer victimized. Both genders had higher symptoms of emotional problems, conduct problems, and hyperactivity than non-peer victimized adolescents. Boys had higher symptoms of emotional problems than girls. All symptom scales were strongly associated with perceived impact on everyday life. Peer and parental support buffer mental health problems among the victimized. Study indicates the importance of interventions strengthening peer support among victimized early adolescents.
Early Adolescence
The age between 10 and 14 years is often referred to as early adolescence (Adams, Bartlett, & Bukowski, 2010). According to Stanley Hall (1904), this phase is a time of storm and thunder. It is dynamic and characterized by great changes within himself or herself such as hormonal and pubertal as well as changes in relation to social structures. The quantum leap into a higher level of cognitive functioning makes life exciting and intriguing. At the same time, many early adolescents experience the fear of becoming small or insignificant (Lerner & Foch, 1987).
Peer Victimization Among Early Adolescents
Peer victimization is a widespread phenomenon in childhood (Gini & Pozzoli, 2009). According to Olweus (1991), a person is victimized when he or she is exposed, repeatedly and over time, to negative actions of one or more powerful peers. Notably, peer victimization is especially prevalent in early adolescence up to 15 years of age and decreases as the children get older (Rigby, 1996). Prevalence of peer victimization varies across schools, cultures, and countries. Roughly 10% of youth are regularly victimized by peers (Olweus, 1993). Gender differences have been observed in peer victimization; boys are more likely than girls to be bullies as well as victims (Scheithauer, Hayer, Petermann, & Jugert, 2006).
Frequent victimization is associated with internalizing mental health problems, such as being unhappy and developing symptoms of depression, anxiety, and suicidal ideation (Menesini, Modena, & Tani, 2009; Winsper, Lereya, Zanarini, & Wolke, 2012; You & Bellmore, 2012). Peer victimization is also associated with having externalizing mental health problems, such as being aggressive, disruptive, having attention problems and antisocial behavior over time (Hanish & Guerra, 2002; Troop-Gorden & Ladd, 2005). Peer victimization impacts the adolescents’ everyday life of both boys and girls. However, based on the longitudinal study by Hanish and Guerra (2002), it seems that gender differences should be considered when predicting the severity of peer victimization consequences such as internalizing and externalizing and social problems. The internalizing problems and fear of negative evaluation from peers may lead to social avoidance. This in turn may limit the victimized adolescent’s positive interactions with peers, for example, in leisure activities, which then influences poor development of social skills (Zarbatany, Hartmann, & Rankin, 1990). Experiences of peer victimization have been found to be associated with poorer academic performance (Kochenderfer & Ladd, 1996; Schwartz, Gorman, Nakamoto, & Toblin, 2005) and increase in school avoidance (Buhs, Ladd, & Herald, 2006; Gastic, 2008).
Parental and Peer Support
Parental warmth is important in the socialization process. A study by Bowes, Maughan, Caspi, Moffitt, and Arseneault (2010) concluded that warm family relationships and positive home environments help buffer children from the negative outcomes associated with peer victimization. Emotional closeness and time spent with parents decrease during early adolescence (Larson, Richards, Moneta, Holbeck, & Duckett, 1996), and although adolescents strive for more independence, they also require emotional closeness and rely on them for guidance and support in critical situations (Gutman & Eccles, 2007). Supportive parent-child relationships, measured by supervision, involvement, and support, and parental warmth were found to reduce externalizing behavioral problems (Ravens-Sieberer, Wille, & Erhart, 2007). There are few things that are more important to early adolescents than acceptance by their peers. Good experiences can lay the foundation for healthy adult social interactions, but bad ones can lay a heavy burden on the developing early adolescents (Hetherington, Parke, & Locke, 1999). According to Boivin, Hymel, and Hodges (2001), supportive peer relations following aversive peer experiences portend fewer internalizing and externalizing behavior problems.
Statement of the Problem
To our knowledge, prior studies have primarily based their results on peer victimization on small populations, and used parents or teachers as sources of information. Being peer victimized often occurs when parents or teachers are not around, and most early adolescents are cautious of disclosing such events (Cassidy, 2009). Self-reports are therefore important and likely to be reliable sources on these matters (Solberg, 2010). The first aim of this study is therefore to investigate the (a) self-reported prevalence of peer victimization in female and male early adolescents in a large and representative sample of early adolescents in Norway. Despite profound documentation of negative influence on mental health problems contributed by peer victimization, few studies have examined gender differences on effects of internalizing and externalizing problems and the impact of these difficulties in everyday life. Hence, the second aim of this study is to (b) measure peer victimization’s association with externalizing problems such as conduct and hyperactivity/inattention problems, and internalizing problems such as emotional problems. Although identifying factors that protect adolescents from maladaptive development might be useful for developing more effective intervention strategies, we also want to investigate the impact of problems on home life, friendships, leisure activities, and classroom learning. Therefore, finally we examine whether (c) peer victimized early adolescents are protected from the negative influence on mental health by parental and peer support. The present study will expand the knowledge on the impact of peer victimization on everyday life among early adolescent boys and girls, and more closely examine factors that can protect against detrimental outcomes for the sufferers.
Method
Participants and Procedure
This study is based on data from a cross-sectional health survey, undertaken in Akershus County in Norway in 2002 by the Norwegian Health Services Research Centre. Pupils (n = 11,153) in fifth to seventh grade and their parents were invited to participate in the study. Totally 9,707 (87, 2%) early adolescents (aged 10-14, Mage = 11.5 boys: 50.7%) and 8,210 parents (74%) responded to the questionnaire. To obtain a representative sample of the County, classes at each school level were selected randomly. Participation in the study was voluntary, and the parents were asked to give their consent. The adolescents were filling in the questionnaire at school under teacher supervision. The adolescents also received one questionnaire to take home to their parents for them to fill in and return back in a sealed envelope. To match the questionnaires for each child and their parent without violating the anonymity of the participants, the same registration number was used. All information was treated anonymously. The study was approved by the Norwegian regional committees for medical research ethics. The variables peer victimization, externalizing and internalizing mental health problems, its impact on everyday life, as well as parental support and peer support were all collected from the adolescent questionnaire. The demographic variables were collected from the parent questionnaire.
Measures
This study is based on a heath profile survey that was broad based to investigate many facets of the lives of adolescents and youth. Therefore, especially due the young age of this group, the survey needed to be kept as short as possible, so that it was possible to complete for all students, in a usual class hour. Therefore, there are not many questions pertaining to each facet.
Peer victimization
To assess peer victimization, the two available items were used. The first being “Have other students at school bullied you?” Responses were given on a 3-point scale (0 = almost never or never, 1 = yes, sometimes, 2 = yes, often). The second item was chosen from the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) referring to how things have been over the last 6 months: “Other children or young people pick on me or bully me.” Responses were given on a 3-point scale (0 = not true, 1 = somewhat true, 2 = certainly true). Scores on the two questions were summed, responses varying from 0 to 4. In the analysis, due to the young age of the respondents and the tendency to underreport, it was decided to accept a broad range in the yes score, thus scores ≥2 were classified as being peer victimized when dichotomizing the variable.
Mental health problems
SDQ was used to assess mental health problems (Goodman, 1997). The questionnaire has a total difficulties score, consisting of four subscales with five items each: Emotional Problems, Conduct Problems, Hyperactivity/Inattention Problems, and Peer Problems. The latter was not included as the symptoms of peer problems correlate highly with being peer victimized. The respondents were asked to rate the occurrence of various psychopathological symptoms within the last 6 months. Internalizing problems were operationalized as emotional problems, whereas externalizing problems were operationalized as conduct or hyperactive/inattention problems. Responses were given on 3-point scales (for negatively worded items, 0 = not true, 1 = somewhat true, 2 = certainly true; for positively worded items, the scoring is reversed). For each of the subscales, items were summed to generate subscore (range = 0-10). Cronbach’s alpha for emotional problems was .61; for conduct problems, it was .43; and for hyperactivity/inattention problems, it was .60. Norwegian cutoffs taken from Van Roy (2010) were used to band the population into 10% high-risk group, 10% borderline, and 80% low-risk group, using the same statistical banding as Goodman (1997). Cutoff points for conduct problems are low risk = 0-2, borderline = 3, high risk = 4-10; for hyperactivity/inattention problems are low risk = 0-4, borderline = 5, high risk = 6-10; and for emotional problems are low risk = 0-2, borderline = 3, high risk = 4-10. These variables were dichotomized into “normal” and “borderline/high risk.” A total difficulties score was constructed by the sum of the subscales, Emotional Problems, Conduct Problems, and Hyperactivity/Inattention Problems, leading to scores that ranged from 0 to 30. Cronbach’s alpha was .70. Cutoff points that were equivalent to the banding suggested by Goodman were for the lowest 80% (low risk = 0-11), next 10% (borderline = 12-13), and 10% highest score (high risk = 14-30). The total difficulties score was dichotomized into “normal” and “borderline/high risk.” To assess the impact of mental health problems on everyday life, the extended version of the SDQ which includes a “total impact score” was used, scores ranging between 0 and 10. A series of questions were included concerning whether the respondent thinks he has a problem, and if he does, how this might interfere with relations to family, friends, learning situation, and leisure activities. Responses to the five questions provided four alternatives but coded on a 3-point scale (0 = no or little, 1 = quite a lot, 2 = a great deal), resulting in a possible range of 0 to 10 when the five questions were summed. According to Goodman (1999), a total impact score of 2 or more (of a 10-point scale) defines abnormal/caseness. The impact score is also dichotomized into “normal” and “borderline/high-risk” group. For the impact score, Cronbach’s alpha was .97. For the individual items in the impact score, they were dichotomized for analysis, such that no or a little was no, and quite a lot or a great deal was yes.
Peer support
To assess peer support, four items were chosen from the subscales of the SDQ questionnaire that were not used in assessing mental health. For the items “I am usually on my own, I do things alone” and “I get on better with adults than with people my age,” responses were given on a 3-point scale (0 = not true, 1 = somewhat true, 2 = certainly true). For the two items “I have one good friend or more” and “Other people my age generally like me,” responses were given on a 3-point scale (2 = not true, 1 = somewhat true, 0 = certainly true). These four items were reversed so as to be in a positive direction. The scores for each of the four positive items were dichotomized prior to making the index, such that low and a little support = 0 and high support = 1. The dichotomous variables were summarized to make the index for peer support, leading to values ranging from 0 to 4.
Parental support
We measured parental support by using a single question “Do you feel that someone at home cares about what you do?” Responses were given on a 4-point scale (0 = no, 1 = a little, 2 = yes, 3 = don’t know). This variable was dichotomized, adolescents who answered “yes” were classified as having good support at home, meanwhile adolescents who responded to the other response alternatives were classified as not having good support at home. To limit the length of the questionnaire, only this question was asked to the younger adolescents. However, in the study with slightly older children, this question was supplemented with five extra questions concerning parental concern and involvement. Examining the relationship between this single question and the five more detailed questions revealed a significant and very high correlation between all five questions and the single question (data not shown), verifying the precision of this question. Parental support and peer support questions were used as covariates in the analysis to see if they effect on the possible associations between peer victimization and mental health problems.
Demographic variables
Early adolescents’ gender, age, family income, and family structure were included. Information about family structure and family income was provided by the questionnaire filled in by the parents. Family structure was measured by asking if the early adolescent lives with both parents (0 = no, 1 = yes). Family income was measured by asking how well off the parents think their family income is, responses given on a 5-point scale (1 = very good, 2 = good, 3 = average, 4 = not very good, 5 = poor). This variable was reversed, higher number meaning feeling more well off.
Analyses
The Statistical Package for the Social Sciences (SPSS for Windows, Version 22) was used for the data analyses. To analyze the association between early adolescents’ self-report of peer victimization and the outcome of mental health variables (total difficulties score as well as emotional problems, conduct problems, hyperactivity/inattention problems, and impact score), a multivariate logistic regression model was used to estimate odds ratios. Analyses were adjusted for demographic information, including gender, age, family income, and family structure. When including the variables family income and family structure which were answered by the parents, nearly 1,600 cases were not selected due to missing because of the parents’ lower response rate compared to their children. Missing data were excluded casewise, such that only cases with complete data were used in the statistical analyses. Hosmer and Lemeshow test and Omnibus Tests of Model Coefficients indicated good support for the model.
Parental support and peer support (potential mediators) were entered separately at the final step and one at a time. Hierarchal logistic regression was used to measure changes in the association between peer victimization and mental health problems before and after addition of the mediating variables. A mediating effect of parental and peer support was first tested using the classical methods described by Baron and Kenny (1986) and later more specifically by Kim, Kaye, and Wright (2001). This method is based on testing for a significant change in the odds ratio for the relationship between peer victimization and mental health problems before and after the inclusion of the mediators in the model. This method of testing for mediation is limited to the assumption that no other variables are mediating or moderating the associations between the independent or mediator and the dependent variable (Hayes, 2013).
Mediation, more specifically parallel mediation, was tested using the total model, the bootstrap method for the indirect pathway, and the Sobel test both provided in the PROCESS module for SPSS (Model 4). Model fit was evaluated using R-squares, which were significant for both the analyses for total symptom problems and for impact.
Multicollinearity was used to identify if the independent variables showed some relationship with the dependent variable. Tolerance and variance inflation factor (VIF) did not violate the multicollinearity assumption (tolerance value less than 0.1 and VIF value above 10). Precision of the associations (odds ratios) was assessed using 95% confidence intervals (CIs).
Results
Table 1 shows the prevalence of self-reported peer victimization, mental health problems (SDQ), as well as demographic variables. Totally 707 (17.6%) of the boys and 618 (15.3%) of the girls reported that they had been peer victimized. There are gender differences in symptoms of mental health problems associated with peer victimization and its impact on everyday life.
Characteristics of the Early Adolescents in Fifth to Seventh Grade, With and Without Being Peer Victimized, According to Self-Report.
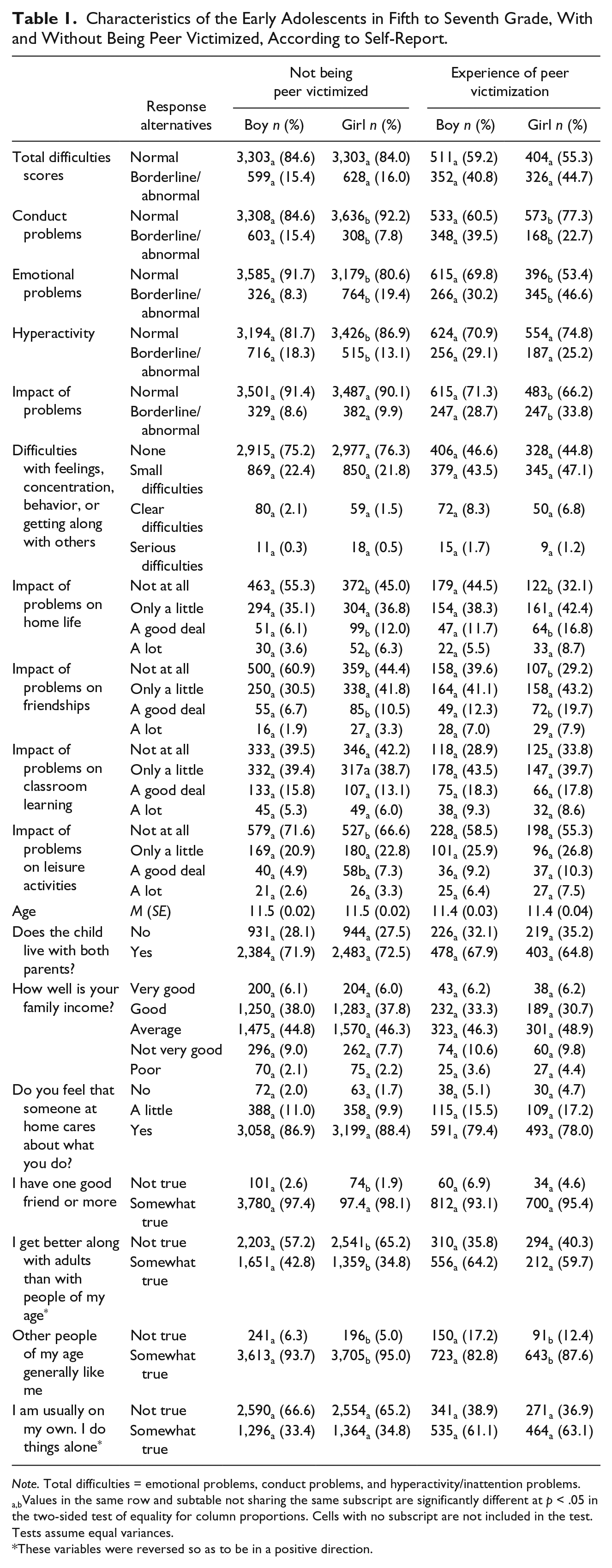
Note. Total difficulties = emotional problems, conduct problems, and hyperactivity/inattention problems.
a,bValues in the same row and subtable not sharing the same subscript are significantly different at p < .05 in the two-sided test of equality for column proportions. Cells with no subscript are not included in the test. Tests assume equal variances.
These variables were reversed so as to be in a positive direction.
In Table 2, the association between self-reported peer victimization and total symptom problem, in addition to the subscales for internalizing and externalizing mental health problems, is shown. The adolescents who report being peer victimized have nearly 4 times larger odds for boys and 4 times for girls of mental health problems measured with the total SDQ score than early adolescents who do not report being peer victimized. There is a significant association between peer victimization and internalizing problems, emotional problems and externalizing problems, conduct problems and hyperactivity/inattention problems, where both boys and girls who report being peer victimized have more mental health problems than their counterparts who are not being victimized. Boys reported having more emotional problems when peer victimized than girls, with nearly 1.4 higher odds ratios of emotional problems.
Logistic Regression Analysis Examining Associations Between Early Adolescents Self-Report on Peer Victimization and the Three Subscales of SDQ Total Symptom Scale: Emotional Problems, Conduct Problems, and Hyperactivity.

Note. Adjusted for demographic information: gender, age, family income, and family structure. Reference group are early adolescents who are not peer victimized. Total symptom problems is dichotomized normal versus borderline/abnormal. Reference is normal. SDQ = Strengths and Difficulties Questionnaire; OR = odds ratio; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
The impact on everyday life of adolescents who are being peer victimized is high (Table 3). Adolescents (both boys and girls) who have been peer victimized have more than double the risk of experiencing mental health problems and social impairment related to family, friends, classroom learning, and leisure activities. The relationships between the individual items and peer victimization, although relatively equal, are slightly greater for the domains of friends and weakest for classroom learning for boys and home life for girls.
Logistic Regression Analysis Examining Associations Between Early Adolescents’ Self-Report on Peer Victimization and the Four Items of Impact Domain of SDQ Impact Scale: Home Life, With Friends, Classroom Learning, and Leisure Activities.
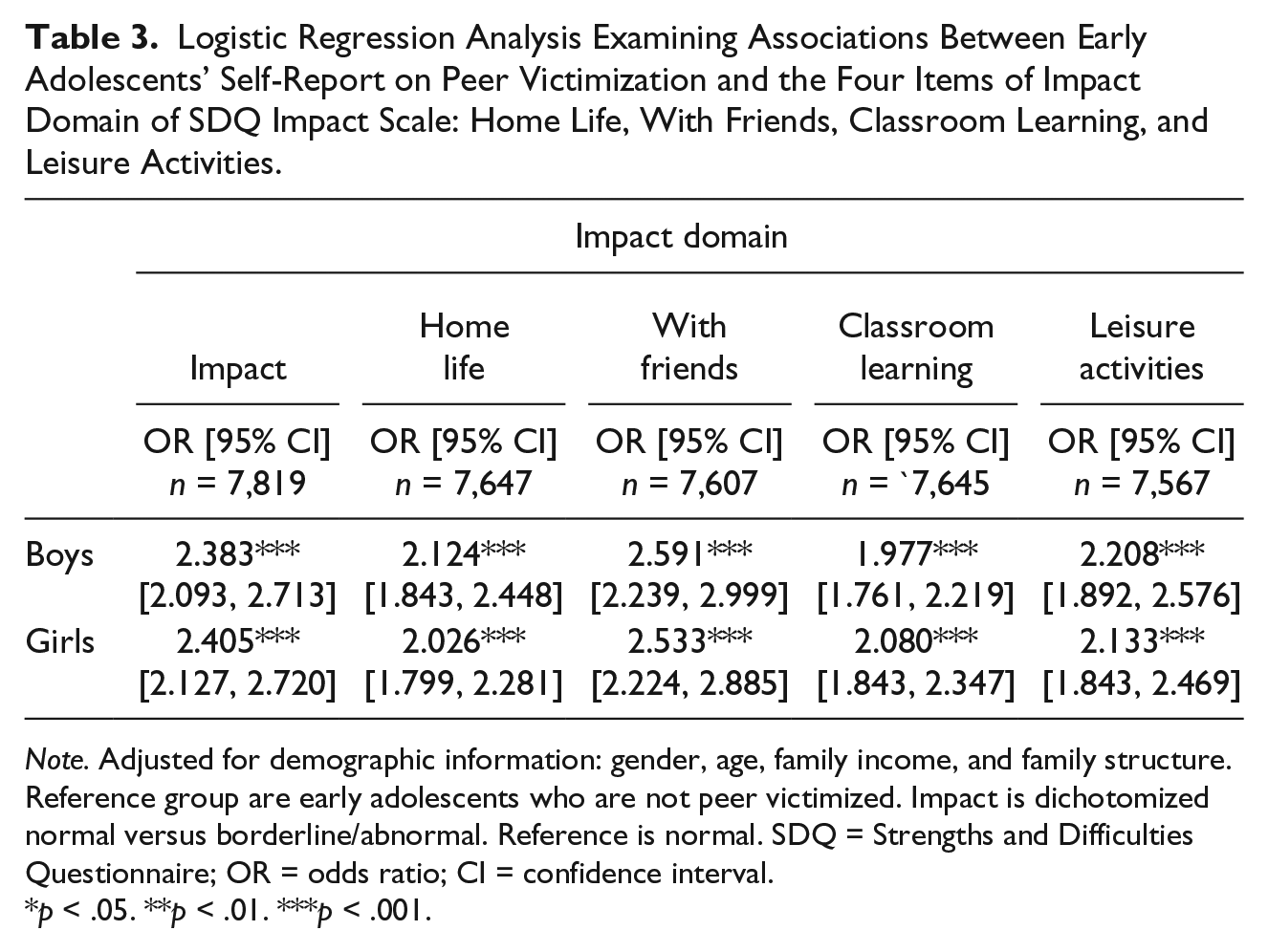
Note. Adjusted for demographic information: gender, age, family income, and family structure. Reference group are early adolescents who are not peer victimized. Impact is dichotomized normal versus borderline/abnormal. Reference is normal. SDQ = Strengths and Difficulties Questionnaire; OR = odds ratio; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
As shown in Figures 1 and 2, both parental and peer support serve as significant mediators in the association between peer victimization and both total symptom problems, and the impact of these problems on daily life. Being peer victimized is negatively associated with both peer and parental support, with the relationship for peer support being the strongest. The relationship between both parental support and peer support and both total symptom problems and the impact of these problems is relatively equal and negative. The total indirect effect of peer support is 6 times greater than the indirect effect of parental support. Considering that mental health is relatively highly inherited and dominated by personality factors, the R2 of .10 to .15 (which is highly significant) can be considered substantial (Bergen, Gardner, & Kendler, 2007). This is supported by a much greater fall in odds ratio when peer support is entered in hierarchal logistic regression than when parental support is entered both for total symptom problems and for impact (Tables 4 and 5).
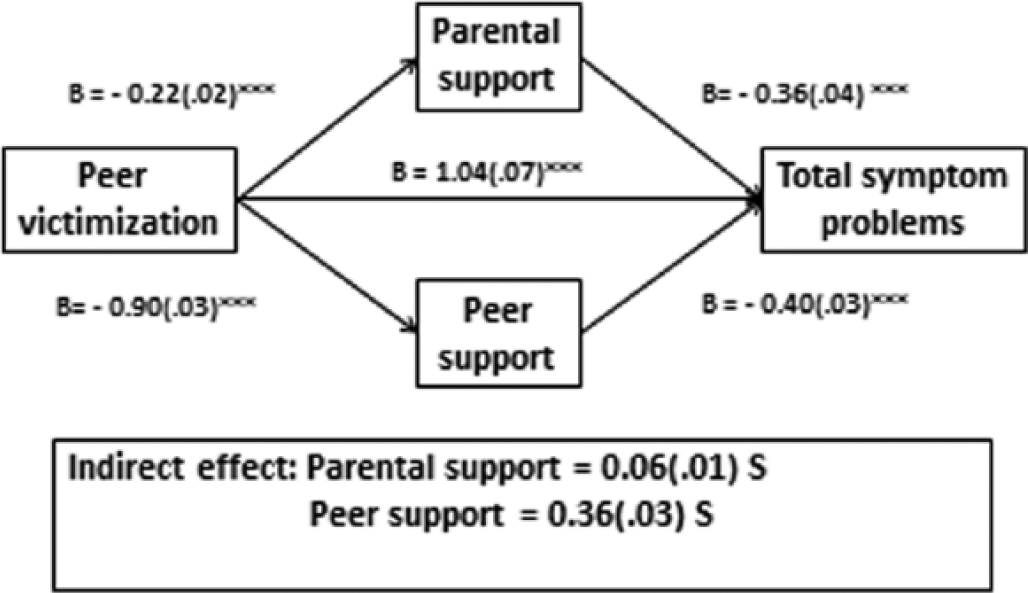
Mediation analysis using logistic regression examining associations between early adolescents’ self-report on peer victimization and SDQ Total Symptom Scale and the mediating role of parental and peer support.

Mediation analysis using logistic regression examining associations between early adolescents’ self-report on peer victimization and SDQ Symptom Impact Scale and the mediating role of parental and peer support.
Logistic Regression Analysis Examining Associations Between Early Adolescents’ Self-Report on Peer Victimization and Their Reports on Total Difficulties Symptoms Controlling for Demographic Information, Parental Support, and Peer Support.

Note. Step 1 = adjusted for demographic information and victimization. Step 2 = adjusted for demographic information and parental support. Step 3 = adjusted for demographic information and peer support. Total difficulties: emotional problems, conduct problems, and hyperactivity/inattention problems. Demographic information: gender, age, family income, and family structure. Total symptoms problem is dichotomized normal versus borderline/abnormal. Reference is normal. Bootstrapping and Sobel test done using the module PROCESS for SPSS. Tot = total effect of X on Y; Bts = bootstrap; Sob = Sobel test; OR = odds ratio; CI = confidence interval; S = significant with bootstrapping.
Reference group are early adolescents who are not peer victimized.
p < .05. **p < .01. ***p < .001.
Logistic Regression Analysis Examining Associations Between Early Adolescents’ Self-Report on Peer Victimization and Their Reports on Impact Controlling for Demographic Information, Parental Support, and Peer Support.

Note. Step 1 = adjusted for demographic information and victimization. Step 2 = adjusted for demographic information and parental support. Step 3 = adjusted for demographic information and peer support. Demographic information: gender, age, family income, and family structure. Impact is dichotomized normal versus borderline/abnormal. Reference is normal. Bootstrapping and Sobel test done using the module PROCESS for SPSS. Tot = total effect of X on Y; Bts = bootstrap; Sob = Sobel test; OR = odds ratio; CI = confidence interval; S = significant with bootstrapping.
Reference group are early adolescents who are not peer victimized.
p < .05. **p < .01. ***p < .001.
Discussion
In this cross-sectional survey, we assessed the frequency of self-report victimization by peers in fifth- to seventh-grade early adolescents and the association with mental health problems. Totally 17.6% of the boys and 15.3% of the girls reported being peer victimized, which does not differ substantially from previous findings of Norwegian schoolchildren (Craig et al., 2009). As expected, the prevalence is less when compared with other non-Scandinavian countries in Europe (Craig et al., 2009). The higher prevalence among boys is consistent with prior studies (Scheithauer et al., 2006). Boys are more physically aggressive than girls, openly aggressive and express more anger, both verbally, through facial expressions and other non-verbal forms of expression (Postigo, Gonzalez, Montoya, & Ordoñez, 2013). The relatively high prevalence of peer victimization indicates that many early adolescents either directly or indirectly suffer from peer victimization, in a period of their lives where peer relationships are crucial for good and healthy development (Zarbatany et al., 1990).
Peer victimization was associated with having mental health problems measured with the total SDQ score, as also reported in other studies (Gini, 2008). Meta-analytic review of cross-sectional studies concerning children who are peer victimized concluded that in both genders, in all age groups and with all subtypes of victimization, there was a correlation with a range of internalizing difficulties, such as poor self-esteem, depression, social anxiety, and loneliness (Hawker & Boulton, 2000). Contrary to earlier findings measuring emotional problems by peer victimization using SDQ (Nabuzoka, Ronning, & Handegard, 2009), our study revealed that peer victimized boys experienced more emotional problems than girls. Hawker and Boulton (2000) found that internalizing difficulties were related to verbal and indirect form of peer victimization. We did not ask what type of peer victimization the adolescents had experienced. It could be that boys scored higher on emotional problems because they had more often than girls experienced being verbally attacked or indirectly been rejected in peer relations.
For both genders, reporting being peer victimized was associated with higher prevalence of having symptoms of externalizing problems, conduct problems, and hyperactivity/inattention problems. This is in accordance with previous studies showing similar results for conduct problems (Gini, 2008; Nabuzoka et al., 2009) and hyperactivity/inattention problems (Nabuzoka et al., 2009; Shojaei, Wazana, Pitrou, Gilbert, & Kovess, 2009). According to Nabuzoka and colleagues (2009), conduct problems and hyperactivity/inattention problems were associated with reactions of retaliation for both boys and girls. Studies have shown that fighting back only leads to further (stable) peer victimization, rather than reduction (Kochenderfer & Ladd, 1997).
In line with a previous study in a Norwegian population (Ronning, Handegaard, & Sourander, 2004), we found that both genders experienced social impairment, overall the results were not significantly different for boys and girls. The results showed that peer victimization was associated with interference in classroom learning. A recent meta-analysis review of the association between peer victimization and academic achievement revealed that victimization in the peer group is related to concurrent academic functioning difficulties (Nakamoto & Schwartz, 2010). Our findings also revealed that peer victimization interferes with early adolescents’ home life, which is somewhat supported by Ambert (1994) who found that peer victims often bring home their frustration in school and lash out at their parents who may be unaware of their children’s victimization in school. Furthermore, our findings on peer victimization and interference concerning implications for everyday life, such as participation in leisure activities, could be explained by the bully preventing the establishment of friendships by isolating him or her (Hazler & Denham, 2002). This can result in lack of social participation in, for example, leisure activities (Gray, Janicke, Ingerski, & Silverstein, 2008) that may delay and possibly weaken development of social interactions.
Our findings that peer support mediates the effects of peer victimization on mental health problems are as expected. Early adolescents spend considerable amounts of time with their peers, and good peer relations that are developed are important contributions to their self-worth, protecting against negative factors (Postigo et al., 2013). This finding is also supported by Storch and Masia-Warner (2004), who found that peers provide victimized adolescents with support buffered against more loneliness. Our finding that parental support mediates mental health problems among peer victimized is also not surprising. Prior studies have shown that warm family relationships and positive home environments help buffer children from the negative outcomes associated with peer victimization (Stadler, Feifel, Rohrmann, Vermeiren, & Poustka, 2010). However, a study by Cassidy (2009) revealed that victims reported poorer family relations and less encouragement from parents. Our finding that there is a slightly weaker mediator role of parental support in the relationship between peer victimization and mental health problems could be explained by peer victimization that most likely happens at school, so that having supportive peers around at that time helps the peer victimized adolescents cope better. In addition, opening up to parents after school can be harder, according to Olweus (2002), as not all parents know about or talk to their children about peer victimization.
Strengths and Limitations
The present study is based on a large sample of early adolescents, with high response rate and few missing data. These data can also be regarded as representative of large parts of Norway, as Akershus County, surrounding the Norwegian capital of Oslo, has urban, suburban, and rural areas with clear differences in socioeconomic status (Van Roy, 2010). Despite lack of information about ethnicity in the present study, only a small percentage of the population in the studied county have non-Norwegian ethnic background. Excluding those of Nordic or Western European descent, there was only around 3% of the population of non-Norwegian ethnicity. Limitations of the study includes using a cross-sectional design, which makes it impossible to conclude about causation. However, this study presents a clear indication of the links between being peer victimized, having internalizing and externalizing mental health problems among early adolescents aged 10 to 13 years. By definition, peer victimization is a distressing experience that occurs frequently and is often continuous over years (Olweus, 1991). In the health profile questionnaire that was used, the definition of being peer victimized was not given when the early adolescents answered the question of being peer victimized. This might lead to misunderstandings about what peer victimization consists of, and give us incorrect results.
Conclusion and Implications for Practice
This study shows the profound impact peer victimization has on the early adolescents’ everyday life. Both genders had higher symptoms of internalizing and externalizing mental health problems than non-peer victimized adolescents, and victimization was strongly associated with perceived impact on everyday life. Both peer and parental support buffer mental health problems among the victimized. The study indicates the importance of early interventions to strengthen peer support among victimized early adolescents.
Footnotes
Acknowledgements
The authors thank the Norwegian Foundation for Health and Rehabilitation for financial support to the Health profile this study is based on. The Health profile was performed in cooperation with the Norwegian Service Research Centre, now incorporated into the Norwegian Knowledge Centre for Health Services. This research was made possible by the Department of Health Surveillance and Prevention at the Norwegian Institute of Public Health, which gave us access to their data and enabled us to perform this analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.