
Abstract
Inconsistencies exist regarding the relation between physical activity (PA) and internalizing symptomology in early adolescence, and there is need for investigation of potential moderators that may account for these discrepancies. The current study utilized a Self-Determination Theory Framework to investigate the main effects of five key motivations to exercise and their moderating effects between PA and internalizing problems in an underserved sample of adolescents (n = 167; mean age = 12.19 years; 73% African American). Analyses showed that intrinsic motivations were negatively related to internalizing problems and extrinsic motivations were positively related. PA was only protective against internalizing problems when intrinsic motivations were high and had iatrogenic effects when these were low. Exploratory analyses further delineated the unique effects of motivational orientations. Clinical implications and future research directions are discussed.
Early adolescence represents a time in which there are declines in overall mental health and high risk for initial onset and lifelong struggles with depression and anxiety (Kessler et al., 2007). Approximately 36.7% of American Adolescents (aged 9-16) meet criteria for at least one internalizing disorder (Costello, Mustillo, Erkanli, Keeler, & Angold, 2003), with the incidence of internalizing disorders increasing across the last two decades, especially for girls (Bor, Dean, Najman, & Hayatbakhsh, 2014), and suicide accounting for approximately 8.5% of adolescent deaths (World Health Organization, 2017). Experiencing these disorders in adolescence has been shown to predict a two- to threefold increased risk of experiencing a disorder again in adulthood (Pine, Cohen, Gurley, Brook, & Ma, 1998). Research suggests that increasing physical activity (PA) in adolescence can serve to reduce the risk of depressive symptoms, buffer the effects of environmental stressors (e.g., family conflict) on internalizing problems (Sigfusdottir, Asgeirsdottir, Sigurdsson, & Gudjonsson, 2011), and increase psychological functioning across the life span (Brand et al., 2017; Ussher, Owen, Cook, & Whincup, 2007; Wiles et al., 2008). However, inconsistencies in these relations across studies has led some researchers to assert that motivations (e.g., mastery, appearance) youth have for their regular engagement in PA may influence the degree in which PA is beneficial for mental health (Brand et al., 2016; Skrove, Romundstad, & Indredavik, 2013; Spruit, Assink, van Vugt, van der Put, & Stams, 2016; Szabo, 2000). A sizable increase in PA initiatives and interventions for adolescents have been prompted in recent years as a result of the distinct decline observed in time spent engaged in PA at this developmental period (Belcher et al., 2010), particularly for females (Madsen, McCulloch, & Crawford, 2009), and the alarming high and stable rates of adolescent inactivity (Marques & Gaspar de Matos, 2014) and obesity (Ogden, Carroll, Kit, & Flegal, 2012). Examining motivational processes by which we can promote youth mental health, along with increasing PA, can contribute to developing highly efficacious cost-effective interventions that address two primary health issues among today’s adolescents. The current study aims to address inconsistencies found in the relation between PA and internalizing problems in early adolescence through examination of the influence of youth exercise motivations.
Research suggests that anxiety and depression are the most common disorders seen in adolescents (Merikangas et al., 2010) and that persistent or escalating stressful events which occur in adolescence may increase the risk for internalizing disorder onset in early adulthood through their direct association with high or increasing symptom levels (Rueter, Scaramella, Wallace, & Conger, 1999). Furthermore, there are several neuronal changes (e.g., the executive network and the dopaminergic system) that occur during adolescence that increase the risk of developing psychological difficulties (Giedd, Keshavan, & Paus, 2008). Positive effects of PA on psychological well-being have been well documented in adult samples (Penedo & Dahn, 2005) but somewhat inconsistent among adolescents (Biddle & Asare, 2011; Biddle, Fox, & Boutcher, 2003; Brand et al., 2017; Brand et al., 2016; Sigfusdottir et al., 2011; Skrove et al., 2013; Spruit et al., 2016). For example, one study of adolescents (aged 13-16), Ussher et al. (2007) found that lower levels of self-reported PA and higher levels of self-reported sedentary behavior were associated with higher amounts of total difficulties as represented by the Strengths and Difficulties Questionnaire (SDQ). Similarly, Brand and colleagues (2017) found that self-reported PA was associated with improved psychological or sleep functioning (another construct closely tied to general well-being) and Wiles and colleagues (2008) found that youth who reported participating in at least 60 minutes per day of PA were less likely to have emotional problems at a 1-year follow-up than youth who did not meet PA recommendations. In contrast, three large-scale studies showed that overall, the effects of PA on psychosocial outcomes in children and adolescents (ages 10-21) were small to moderate and generally inconsistent (Biddle & Asare, 2011; Brand et al., 2016; Spruit et al., 2016), with several studies not showing any significant positive effects of PA or, in some instances, even showing iatrogenic effects on mental health. Szabo (2000) posited that the motivational profile of an individual, a critical moderator typically left unexplored, may be imperative to assess to understand how exercise positively or negatively impacts mental well-being. The goal of the current study was to examine intrinsic and extrinsic motivations as critical mechanisms that may moderate the relation between PA and internalizing symptomology among early adolescents.
Self-Determination Theory (SDT) has been frequently used as a framework for understanding human motivation in various contexts (e.g., Early et al., 2016; Ryan & Deci, 2007). A basic premise of SDT is that humans share an innate need to satisfy three basic psychological needs: competence, relatedness, and autonomy (Deci, Vallerand, Pelletier, & Ryan, 1991). Intrinsically motivated behaviors may satisfy one or more of the three basic needs or give an individual some other form of inherent pleasure. These behaviors are done through an individual’s own sense of volition void of specific external rewards for performing the activity. On the opposing side of the continuum are purely extrinsic motivations which are those that are thought to be instrumental for another purpose. Purely extrinsically motivated behaviors are dependent on specific contingencies and do not satisfy the inherent basic needs. A multitude of studies have applied SDT as a framework for investigating how intrinsic and extrinsic motivations relate to exercise adherence (see Teixeira, Carraça, Markland, Silva, & Ryan, 2012 for a review). In particular, the Motivations for Physical Activity Measure–Revised (MPAM-R; Frederick & Ryan, 1993; Ryan, Frederick, Lepes, Rubio, & Sheldon, 1997) identified five key PA motivations for exercise adherence that can be categorized as either more intrinsic (i.e., competence, social, and enjoyment) or extrinsic (i.e., appearance based and fitness/health) in nature. Among adults (mean age = 39) Frederick and Ryan (1993) showed that intrinsic motivations predicted fewer symptoms of depression and anxiety while both fitness/health and appearance-related motivations to exercise predicted higher amounts of these internalizing problems.
Among the few studies investigating SDT-based exercise motivations among adolescent samples, intrinsically motivated exercise has been shown to predict indicators of psychological well-being (e.g., Gillison, Standage, & Skevington, 2006). One study of early adolescents (mean age = 12.53) found that motivation orientations related to fulfilling the need for competency in PA predicted a more positive physical self-concept, and those related to fulfilling the need for relatedness in PA (social) and intrinsic motivations for exercise (enjoyment) were associated with more adaptive emotional functioning (Standage, Gillison, Ntoumanis, & Treasure, 2012). In contrast, two types of extrinsic motivations (relating to obtaining a specific reward and protecting one’s self-image, respectively; Ryan & Deci, 2000) were related to maladaptive emotional functioning. Another study (Sicilia, Sáenz-Alvarez, González-Cutre, & Ferriz, 2014) also evidenced that introjected regulations (e.g., “I feel guilty when I don’t exercise”), an extrinsic motivation, positively predicted higher amounts of anxiety related to one’s appearance, whereas competence motivations negatively predicted this appearance-related anxiety in adolescents aged 12 to 19. Extrinsic motivations linked to appearance/body image may be particularly problematic among adolescents, who experience rapid physical changes (including weight gain) due to pubertal development and heightened self-consciousness. Although much of the research on body dissatisfaction has highlighted cultural and interpersonal variations (Altabe, 1998), with the largest prevalence among White adolescent female populations, research investigating differences in body dissatisfaction across gender and ethnicities shows small effect sizes across different populations (Grabe & Hyde, 2006) and provides evidence that low socioeconomic status (SES) African Americans are also at-risk of developing body dissatisfaction (Paxton, Eisenberg, & Neumark-Sztainer, 2006) and equally prone to identify with extrinsic PA motivations (Gillison et al., 2006). Given body dissatisfaction and extrinsic PA motivations have each been associated with a higher amount and a greater severity of depressive symptoms in past studies (Almeida, Severo, Araújo, Lopes, & Ramos, 2012; Mueller et al., 1995; Paxton, Neumark-Sztainer, Hannan, & Eisenberg, 2006; Frederick & Ryan, 1993; Tiggemann & Dyer, 1995), appearance-related motivations for PA are particularly maladaptive for adolescents, and may differentially impact the girls in the study sample given females’ greater likelihood of endorsing this motivational orientation for PA (Polivy & Herman, 2004).
Mixed findings between adolescent PA and mental health may also be due, at least partially, to the lack of rigor in methodology across studies. The vast majority of studies that have examined the relations between PA and youth mental health have relied on self-report measures of PA which are less effective in determining actual time spent in PA compared with more objective assessments, like the use of omnidirectional accelerometers (Bassett, Mahar, Rowe, & Morrow, 2008; Lang et al., 2016). Nor have the majority of these studies considered important mediators/moderators, such as youth PA motivation orientations, even though previous research has indicated PA motivations may impact youth mental health. Similarly, the majority of studies that have examined the direct relation between PA motivation and youth mental health do not account for youth PA in their models (e.g., Sicilia et al., 2014), and the few that do include PA have not used accelerometry data (e.g., Gillison et al., 2006; Standage et al., 2012). Furthermore, none of these studies have looked exclusively at underserved samples of early adolescents, a high-risk population for both higher rates of inactivity/obesity and the onset of internalizing problems (Young-Hyman, Schlundt, Herman-Wenderoth, & Bozylinski, 2003; Gaylord-Harden, & Cunningham, 2009).
To address the gaps in the literature, the current study used a SDT framework to examine the moderating effects of intrinsic and extrinsic motivations to engage in PA on the relations between early adolescents’ moderate-to-vigorous physical activity (MVPA) and internalizing problems. This involved a three-step model. First, we examined the main effect of MVPA on internalizing problems. Second, we tested the main effect of motivations for PA on internalizing after controlling for PA, whereby we expected intrinsic motivations would predict fewer internalizing problems and extrinsic motivations would predict more. Third, we tested whether motivations for PA would moderate the effect of MVPA on internalizing problems. It was hypothesized that high rates of youth PA would have differing effects on internalizing depending on whether an individual has greater intrinsic or extrinsic motivations to exercise; youth with intrinsic motivations to exercise were expected to report fewer internalizing problems compared with all others whereby similarly active youth with extrinsic motivations to exercise would not show any benefits of PA on internalizing problems (rates of internalizing symptomology would be similar to inactive youth) or iatrogenic effects (higher rates of internalizing compared with inactive youth). Among inactive youth (low rates of MVPA) we expected high rates of internalizing symptomology despite youth exercise motivations. Finally, exploratory analyses examined whether the five individual subscales that comprise the broader extrinsic and intrinsic composite scales (competence, social relatedness, enjoyment, fitness/health, and appearance) would provide additional contributions to our understanding of what critical motivational mechanisms are necessary for PA interventions to support mental health along with physical health in our sample of underserved early adolescents. Given the major physical, cognitive, social, and psychological changes that characterize early adolescence (Graber & Brooks-Gunn, 1996), we expected that some PA motivations may have a greater impact on youth internalizing problems than others. For example, because of the heightened importance of one’s social world during adolescence (Nelson, Leibenluft, McClure, & Pine, 2005), social motivations for PA may stand out as a particularly influential intrinsic motivation for promoting mental health. Likewise, heightened salience of one’s appearance as youth manage the physical changes associated with puberty, may result in appearance motivations for PA having a greater impact on internalizing symptoms at this age than extrinsic motivations oriented around health/fitness. By examining each motivational dimension separately/uniquely, the current study will be able to identify whether any of the dimensions are particularly critical to target in future intervention given their greater impact on internalizing problems.
The current study addresses several gaps in previous research with the goal of understanding inconsistencies in the literature regarding the relation between youth PA and well-being (Spruit et al., 2016). We are one of only a few studies using a SDT framework (see Owen, Smith, Lubans, Ng, & Lonsdale, 2014 for a review) to utilize omnidirectional accelerometers in a sample of adolescents and the first of these to assess the unique contributions of all five of these motivational orientations for exercise. Furthermore, the current study examines these relations among an underrepresented/understudied early adolescent sample of primarily low-income African American youth, a population identified as at particularly high risk for obesity and the development of internalizing problems (Young-Hyman et al., 2003; Gaylord-Harden, & Cunningham, 2009). The findings of this study will inform the development of future PA interventions that are better equipped to support both physical and mental health of this study’s at-risk population of youth, by targeting and facilitating healthy motivational orientations for exercise.
Method
The data were collected in six middle school after-school programs (ASPs). The current study analyzed baseline data from the Connect through positive leisure activities for youth (PLAY) (PI: Nicole Zarrett) feasibility trial (September, 2014-March, 2017). The intervention provided services to six middle school ASPs comprised of a primarily underserved population of youth (defined by minority status and % receiving free/reduced lunch). The current study utilized youth self-report questionnaires, objectively measured anthropometrics (height/weight), and 1-week accelerometer data collected at baseline prior to sites being randomized to intervention or wait-list control. Institutional review board (IRB) approval was granted for the study.
Participants
Two hundred twenty-five sixth to eighth grade students between the ages of 11 and 14 assented to the study and received parental consent to participate. No students dropped out of the study, however, 57 of the participants included missing self-report data on one of the variables being examined (i.e., SDQ Peer Problems or Emotional Problems subscales; see below for details and imputation procedures for missing accelerometer data). These cases were excluded in a list-wise manner from the analysis leaving a final sample size of 167 participants (mean age = 12.19 years; 97 female students). Chi-square tests showed no significant difference for race (p = .752) or gender (p = .195) for this missing data. A one-way analysis of variance (ANOVA) predicting Z-body mass index (BMI) showed that there was no significant difference in Z-BMI score between participants who had missing SDQ data in comparison with those with non-missing data (p = .243). The sample was primarily non-Hispanic African American (73.6%), with 15.5% identifying as White (13.8% non-Hispanic; 3.0% Hispanic), 2.4% identifying as Multiracial, and the remaining 8.5% as “other.” The schools’ free or reduced lunch eligibility rates ranged from 57% to 98%.
Procedure
All measures included in the current study were collected at baseline. Youth were asked to complete a battery of self-report measures and report on key demographics (e.g., gender, race/ethnicity, age, grade, free/reduced lunch status). Height and weight were measured at baseline using a Shorr Height Measuring Board and a SECA 880 digital scale. Participants also wore an omnidirectional Actical accelerometer (Mini Mitter, OR) for one full week (seven consecutive days) to track PA. Research assistants provided assistance to any youth who had questions or needed help reading/comprehending self-report questionnaire items and provided detailed instructions and assistance to youth on how to properly wear the accelerometer throughout the week.
Measures
PA
Measurement of free-living PA using omnidirectional accelerometry estimates have been established as a more objective measurement of PA that is less susceptible to bias than self-report measures (Bassett et al., 2008; Sallis & Saelens, 2000). Accelerometer belts were worn at the hip and collected data on the students’ energy expenditure (i.e., duration and intensity) in metabolic equivalents (METs; ratio of the metabolic rate to the resting metabolic rate). The data were processed using Actiware Version 6.0.8. and managed using SAS version 9.4. Data were recorded in 60 second epochs and raw activity data were converted into time spent in moderate (3-5.9 METs), vigorous (6-8.9 METs), and MVPA (3-8.9 METs) based on activity count thresholds for children (Puyua, Adolph, Vohra, Zakeri, & Butte, 2004).
Participants’ data were coded for missingness in SAS based on wear criteria established in previous literature (Mitchell, Monaghan, & O’Connor, 2013; Troiano et al., 2008). Data were used only if participants had at least 10 hours of wear (600 total minutes) on 3 out of the 7 days they were in possession of the belts. Approximately 17% of participants (n = 29) did not meet these wear criteria. Missing data were dealt with using multiple imputation using the multivariate imputation via chained equations (mice) R package (van Buuren & Groothuis-Oudshoorn, 2011). All available demographic and psychosocial data were included in imputations for each time point aside from the data collected on the SDQ (Peer Problems and Emotional Problems Subscales were utilized in the current study). Twenty imputations were completed for baseline data and one of these imputations was selected for analyses using a random number generator. Data from the SDQ were merged into this data set and it was used for subsequent analyses.
PA motivation
For the current study, youth motivation orientations for PA were measured using the MPAM-R (Ryan et al., 1997), and the Intrinsic Motivation Inventory (IMI; Duda & Nicholls, 1992). The MPAM-R was designed using a SDT framework and contains five subscales: Appearance, Competence, Enjoyment, Fitness/Health, and Social. Previous research has demonstrated adequate reliability (Cronbach’s α coefficients of subscales ranging from .78 to .92; Ryan et al., 1997) and construct validity (e.g., Achenbach, McConaughy, & Howell, 1987). The version of the measure used in the study included 23 items (1 = “Not at all true for me”; 5 = “Very true for me”) with Cronbach’s Alpha of the subscales ranging from .79 to .92. Recognized as the primary measure of intrinsic motivation, the Enjoyment Subscale of the IMI was used in the current study instead of The Enjoyment Subscale from the MPAM-R. The IMI Enjoyment Subscale (adapted for PA-specific tasks) has shown adequate levels of internal consistency in previous research (α = .78; McAuley, Duncan, & Tammen, 1989) and in the current study (α = .92). The measure includes 11 items (e.g., “When I am active I find it fun”) rated on a 5-point scale (1 = “very false”; 5 = “very true”).
Internalizing problems: SDQ
The self-report version of the SDQ, a 25-item measure of pro-social behavior and psychopathology for ages 3 to 16 (Goodman, 2001; Van Roy, Veestra, & Clench-Aas, 2008) was used to measure internalizing problems (α = .75). A 1998 study supported a five-factor model with a sufficiently high internal consistency (total scale α = .82) and strong predictive validity (Goodman, Meltzer, & Bailey, 1998). This study utilized the Emotional and Peer Problems Subscales from the SDQ. The Emotional Subscale represents anxious and depressive symptomology (“I am nervous in new situations”; “I easily lose confidence”). The Peer Problems Subscale represents the extent to which individuals have social-relational issues (“Other children/young people pick on me or bully me”). All items are on 3-point scale (1 = “Not true”; 2 = “Somewhat true”; 3 = “Certainly true”). Any items related to positive psychological adjustment are reverse-coded, thus, higher total scores on these scales represent higher amounts of maladaptive psychological symptomology within each domain. For the current study, a cumulative score of the two subscales was used to represent internalizing symptomology, which is consistent with recommendations provided by the developer of the scale (Goodman, Lamping, & Ploubidis, 2010).
Covariates
Students’ height and weight were used to calculate standardized BMI scores in accordance with the Centers for Disease Control and Prevention’s (CDC) growth charts based on an individual’s age and sex (CDC, 2009). The mean Z-BMI percentile of the sample was approximately half of a standard deviation (SD) above a population normed average for their respective age groups (
Analytic Procedures
All analyses were run using SPSS Version 21 software package (IBM Corp., Somers, NY). Initially, bivariate correlational analyses and ANOVA models were run to investigate the relationships between all variables including potential covariates (i.e., Z-BMI, gender, and race) that may contribute added variance to the models. For aim one which involved testing the main effects of MVPA on internalizing problems, the first step of a three-step hierarchical linear regression model was conducted that included MVPA and any covariates that had a significant relationship to MVPA. For Aim 2, Intrinsic and Extrinsic Motivation Scales were entered into Step 2 of the model to test the main effects of motivational orientations to exercise on internalizing problems while controlling for MVPA and covariates. For aim three, which included testing the moderating effects of motivational orientations to exercise on the relation between MVPA and internalizing problems, two interaction terms, one of intrinsic motivations with MVPA and one of extrinsic motivations with MVPA, were entered into the third step of the model.
A similar procedure was used for our exploratory analyses which assessed the main effects and moderating effects of each separate motivational orientation subscale on internalizing problems. Each of the individual intrinsic subscales of the MPAM-R (Competence, and Social Subscales) and the IMI for PA affect (Enjoyment Subscale) were entered into the second step of a hierarchical linear model that controlled for MVPA, the composite Extrinsic Motivation Scale, and other covariates in Step 1. Therefore, the intrinsic motivations model tested the main effects of these motivational orientations on internalizing problems while controlling for the effects of extrinsic motivations, MVPA, and covariates. Similarly, for the extrinsic motivations model tested the main effects of the extrinsic subscales of the MPAM-R (Appearance and Fitness/Health) on internalizing problems while controlling for the effects of intrinsic motivations, MVPA, and other covariates. The final step of these two exploratory models included interaction terms between all of the separate intrinsic and extrinsic subscales.
Results
Preliminary Analysis
Participants reported being more intrinsically motivated (
Correlation Matrix and Descriptive Statistics (n = 167).
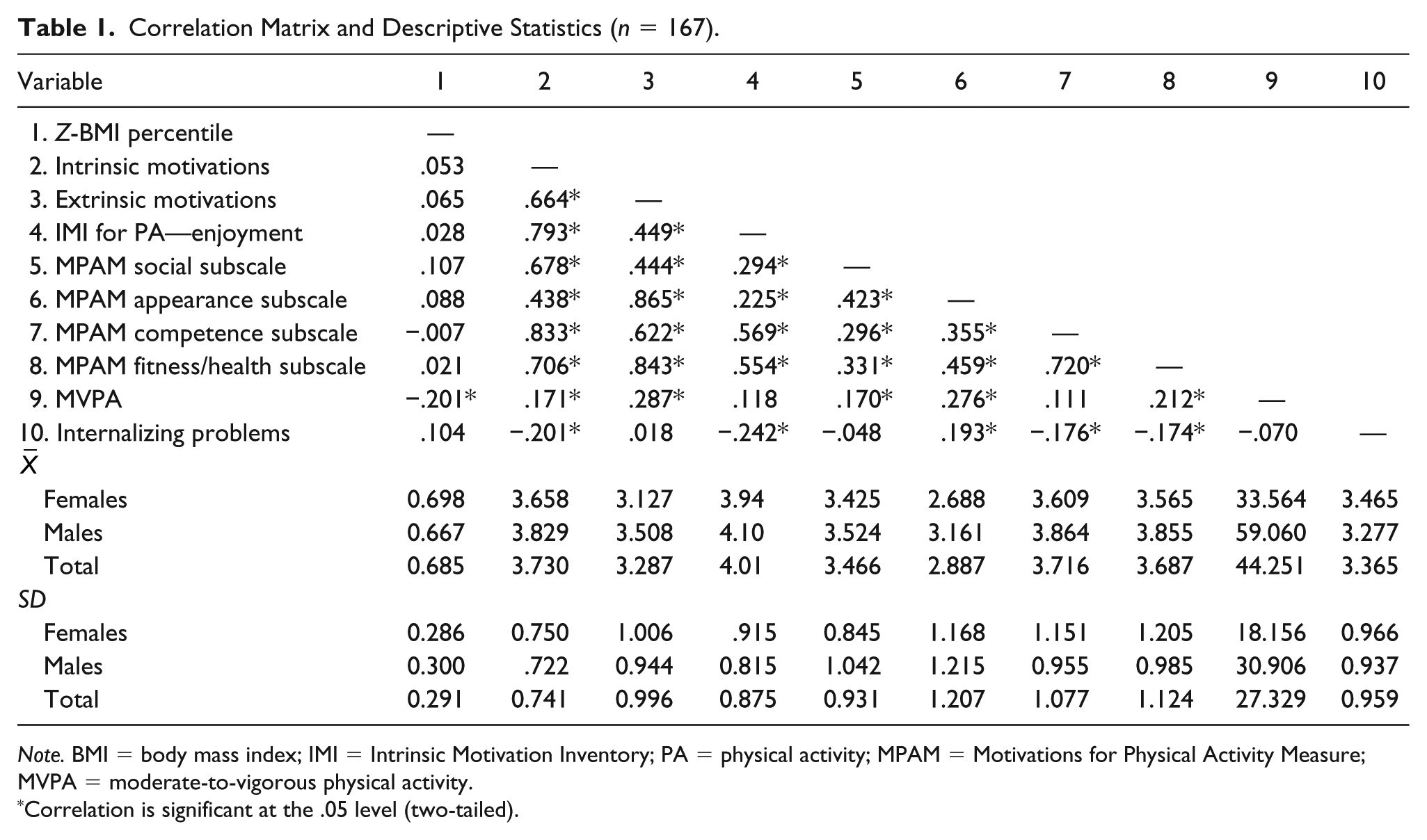
Note. BMI = body mass index; IMI = Intrinsic Motivation Inventory; PA = physical activity; MPAM = Motivations for Physical Activity Measure; MVPA = moderate-to-vigorous physical activity.
Correlation is significant at the .05 level (two-tailed).
Analyses for Primary Aims
MVPA as a predictor of internalizing problems
Contrary to our hypotheses, a linear regression model, controlling for gender and Z-BMI showed that MVPA was not predictive of fewer internalizing problems (p = .620). Neither gender (p = .215) nor Z-BMI (p = .136) were significant.
Intrinsic and extrinsic exercise motivations as a predictor of internalizing problems
Building on the main effects model in aim one, the composite Intrinsic and Extrinsic Motivation Scales were entered in Step 2 of the hierarchical linear regression model to assess the main effects of motivational orientations on internalizing problems, after accounting for MVPA and covariates. This step of the model explained 11.5% of the variance (p < .001; ΔR2 = .034, pδ = .046). As predicted, intrinsic motivations were related to fewer internalizing problems (β = −384, p < .001; see Table 2) and extrinsic motivations were related to more internalizing problems (β = .323, p = .002).
Hierarchical Linear Regression Models predicting Internalizing Problems From Broader Intrinsic and Extrinsic Motivation Variables.

Note. BMI = body mass index; MVPA = moderate-to-vigorous physical activity.
Intrinsic and extrinsic exercise motivations as moderators
The final step of the model that tested the moderating effect of Intrinsic and Extrinsic motivations (Aim 3) explained 14.8% of the variance (p < .001; ΔR2 = .0, pδ = .001). The interaction between intrinsic motivations and MVPA was significant (β = .244, p = .044). A plot of the interaction (see Figure 1) indicated that among youth with high rates of MVPA, those with intrinsic motivations to exercise had significantly fewer internalizing problems than all other youth. However, high rates of MVPA in the absence of intrinsic motivations was related to the greatest instances of internalizing problems. There were minimal differences in internalizing problems among youth low in MVPA despite whether their intrinsic motivation was high or low. Although the interaction between extrinsic motivations and MVPA was not significant (p = .522), there was still a significant main effect whereby extrinsic motivations predicted higher amounts of internalizing problems (β = .378, p = .001). These findings suggest that extrinsic motivations are equally detrimental to the mental health of active and inactive youth.
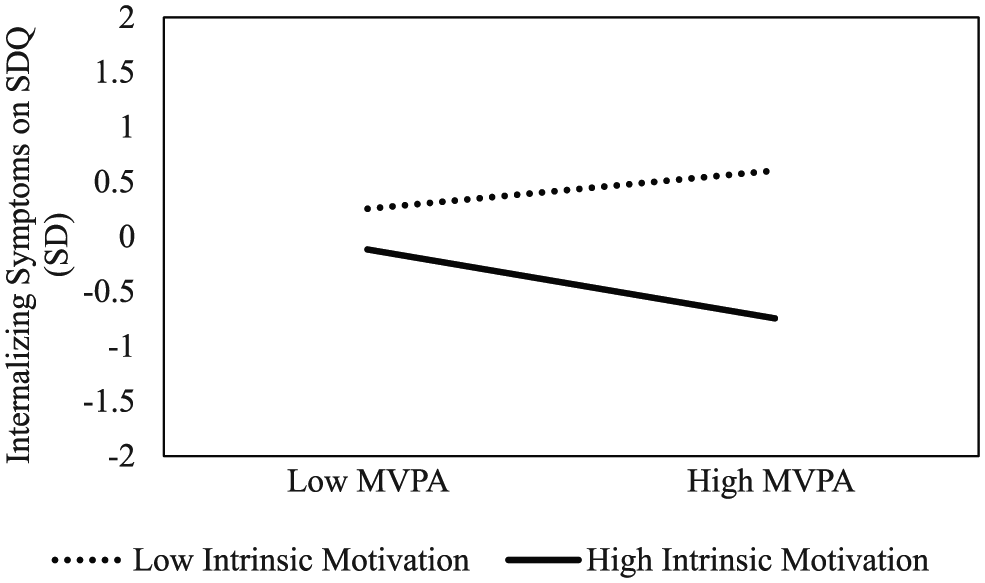
Internalizing problems predicted from MVPA moderated by intrinsic motivations.
Exploratory Analyses
Motivation subscales as predictors and moderators of internalizing problems
In order to test the unique effects and moderating effects of each intrinsic subscale (Enjoyment, Competence, and Social) and extrinsic subscale (Appearance and Fitness/Health) on internalizing problems, two additional hierarchical linear regression models were used that controlled for MVPA, gender, and BMI in step one.
The intrinsic motivations main effects model, which explained 13.5% of the variance (p = .001; ΔR2 = .106, pδ = .001), showed that enjoyment and competence motivations to exercise were negatively related to internalizing problems (β = −.234, p = .011 and β = −.214, p = .042, see Table 3). Social motivations to exercise did not significantly predict internalizing problems (p = .780). The final step of the intrinsic motivations model, which tested moderating effects of the intrinsic subscales, explained 18% of the variance (p < .001; ΔR2 = .046, pδ = .037). Only the interaction between enjoyment motivations and MVPA was significant (β = −.204, p = .048). A plot of the interaction (see Figure 2) indicated that youth with high rates of MVPA who report enjoyment motivations for PA are faring better on internalizing symptomology compared with all other youth. In contrast, youth who are engaging in high rates of MVPA who do not report enjoyment motivations for PA experienced higher amounts of internalizing problems than both their high PA/high enjoyment counterparts, and those low on both MVPA and enjoyment motivations. There is minimal difference in internalizing among low MVPA youth despite their level of enjoyment motivations. Overall, low MVPA youth were less well off than their high PA/high enjoyment counterparts but faring better than high PA/low enjoyment youth. The composite of extrinsic motivation remained significantly related to greater amounts of internalizing problems in the final step of the model (β = .351, p = .001).
Hierarchical Linear Regression Models Predicting Internalizing Problems From Separate Intrinsic Motivations and Controlling for Extrinsic Motivations.

Note. BMI = body mass index; MVPA = moderate-to-vigorous physical activity; IMI = intrinsic motivation inventory; MPAM = motivations for physical activity measure.

Internalizing problems predicted from MVPA moderated by enjoyment.
The extrinsic motivations main effect model, which explained 19.8% of the variance (p < .001; ΔR2 = .169, pδ < .001) showed that appearance motivations were related to higher amounts of internalizing problems (β = .435, p < .001; see Table 4), but fitness/health motivations to exercise were not a significant predictor of internalizing problems (p = .098). The final step of the extrinsic motivations model, which tested moderating effects of the extrinsic subscales, did not predict a significant change in variance explained from the previous step (p < .001; ΔR2 = .026, pδ = .076; 22.3% of the variance), nor were either of the interaction terms significant. Appearance motivations (β = .422, p = .002) remained a significant predictor of higher amounts of internalizing problems but fitness and health motivations (β = −.242, p = .025) predicted fewer internalizing problems. Intrinsic motivation was no longer a significant predictor (p = .100) when the interactions were entered into the final step of the model.
Hierarchical Linear Regression Models Predicting Internalizing Problems From Separate Extrinsic Motivations and Controlling for Intrinsic Motivations.
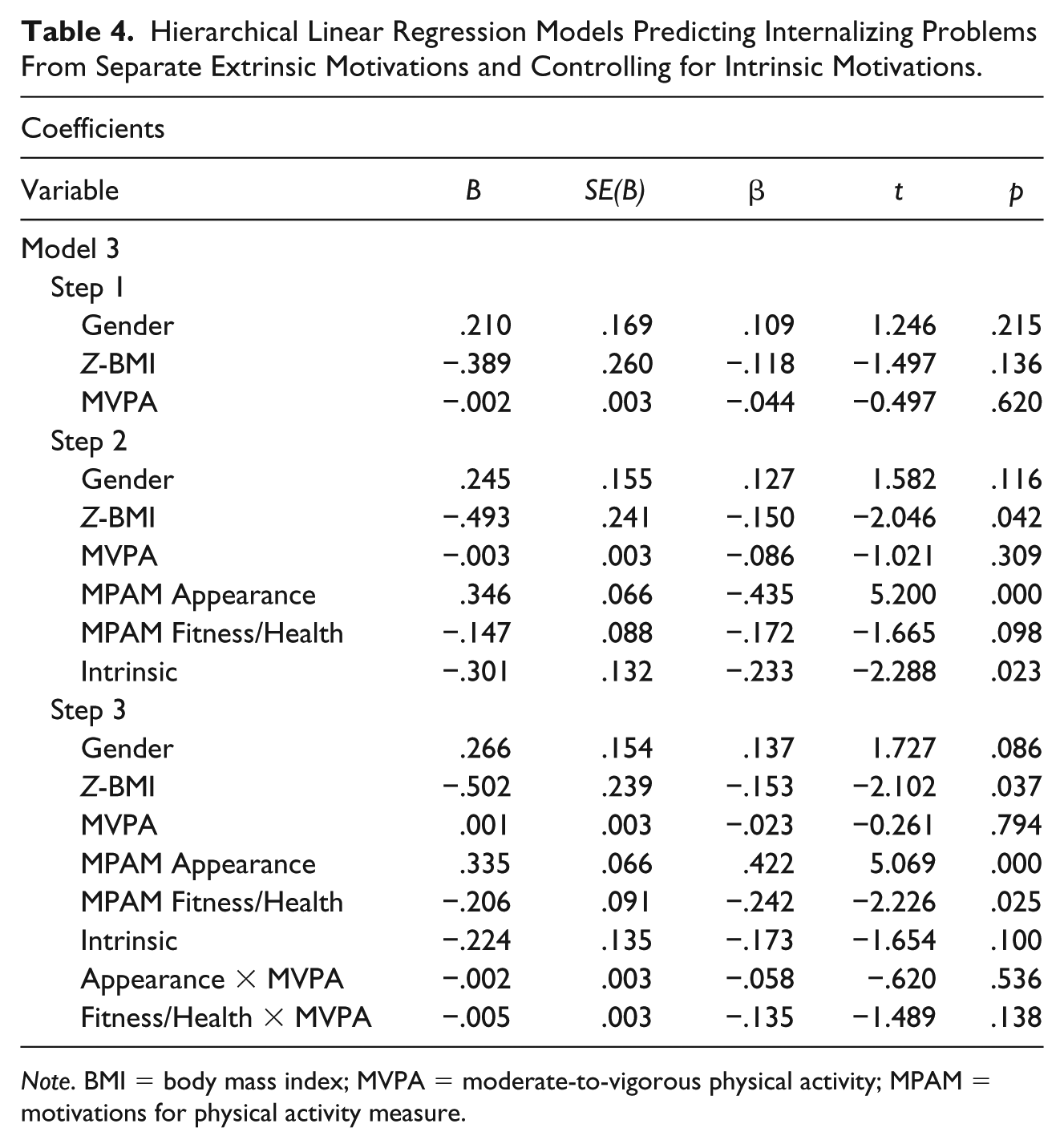
Note. BMI = body mass index; MVPA = moderate-to-vigorous physical activity; MPAM = motivations for physical activity measure.
Discussion
The current study set out to address inconsistencies found in the benefits of PA on youth internalizing problems during early adolescence (Brand et al., 2017; Brand et al., 2016; Skrove et al., 2013; Spruit et al., 2016) by examining the critical role of youth exercise motivations. As one of the first studies to examine these relations within an underserved early adolescent sample and to employ a more rigorous measure of MVPA (using omnidirectional accelerometers), our findings indicate that MVPA, measured by omnidirectional accelerometers, does not significantly predict internalizing problems when controlling for Z-BMI and gender. Szabo (2000) suggested that the underlying motivations for PA in relation to mental health are underresearched in adolescents and may account for the lack of consistent findings between PA and positive mental health outcomes. In addressing this gap, additional findings from our study suggest that youth motivations for exercise are a critical mechanism that directly influences early adolescent psychological functioning and, at times, interacts with PA to result in either promotive or iatrogenic effects.
Main effects of both intrinsic and extrinsic motivations on internalizing problems are in the expected direction such that intrinsic motivations predict fewer amounts of internalizing problems and extrinsic motivations predict higher amounts. In addition, findings from exploratory analyses conducted to gain a more nuanced understanding of the relations between PA motivations and internalizing symptomology indicate some critical variations in these relations by motivation subtypes. Specifically, among intrinsic motivations, enjoyment and competence motivations for PA were particularly protective against internalizing problems, but social motivations for PA did not significantly predict PA.
The competitive nature, and associated teasing, exclusion, and social rejection, as many of the PA activities likely offered in ASPs during the middle school years may wash out the positive effects of having intrinsically driven social motivations for PA (e.g., engage in PA for positive experiences with peers). There is ample support in the literature that the facilitation of a more socially supportive climate for PA could not only increase exercise adherence (Lawman, Wilson, Van Horn, & Zarrett, 2012; Zarrett, Skiles, Wilson, & McClintock, 2012; Zarrett, Sorensen, & Cook, 2015) but may be beneficial for youths’ mental health as well (Yohalem, & Wilson-Ahlstrom, 2010).
Another speculation is that social motivations may be more tightly integrated with extrinsic motivations during early adolescence. The correlations between the Social Motivations subscale and both the Appearance (r =.423) and Fitness/Health Subscales (r = .331) in the current study support this assertion and suggest that there may be some more nuanced externalized components of the social motivations construct that we are not able to identify with the measurement used in this study. For example, measures such as the Social Motivational Orientations in Sport Scale (SMOSS; Allen, 2005) have been designed to differentiate between more intrinsic forms of social motivations (e.g., to facilitate the development of close social bonds) and extrinsic forms of social motivations (e.g., to establish or enhance one’s social standing in a group context). A study examining the validity of the SMOSS among a similar sample of underserved early adolescents (Roberts & Zarrett, 2019), found that affiliation orientations toward PA (similar to the social subscale of MPAM) was intricately intertwined with youth recognition orientation for PA (e.g., receiving praise from friends) at this age (combined as one factor). This may indicate that part of building connection with youth through PA includes receiving the extrinsic feedback of acceptance and praise through sport (Allen, 2003). Thus, there is a need for taking a more nuanced approach when investigating social motivations to exercise among adolescents.
Among extrinsic motivation subscales, results show that appearance motivational orientations to exercise may be particularly harmful as it positively predicts internalizing problems across all youth, regardless of their level of engagement in PA. Such findings warrant significant attention in applied settings. These findings are particularly disconcerting as body dissatisfaction tends to increase throughout adolescence and has been shown to lead to appearance-related (i.e., extrinsic) motivations for exercise and internalizing symptoms; thereby creating a reciprocal maladaptive cycle between physical and mental health (Almeida et al., 2012; Mueller et al., 1995; Paxton et al., 2006; Tiggemann & Dyer, 1995). Given the increased incidence of psychological problems during adolescence observed in recent years (Bor et al., 2014) and the specific neuronal changes that occur in adolescence (Giedd et al., 2008), mitigating all potential factors that can further impact healthy psychological functioning has significant implications for both physical and mental health at a population-level. Furthermore, there is strong evidence supporting the need to address decreasing PA and increasing rates of internalizing during adolescence for females in particular (Belcher et al., 2010; Bor et al., 2014; Madsen et al., 2009). For these reasons, Brand and colleagues (2017) suggest a need to target PA participation among females in particular, as an effective method to combat risks of negative psychological functioning. However, given that our study found females are more likely to report having appearance-related motivations for exercise, concerted efforts to de-emphasize this particularly maladaptive motivational orientation is critical in PA interventions serving adolescent girls to ensure a positive impact of exercise on mental health.
Despite previous literature (Frederick & Ryan, 1993) which has shown that fitness/health motivations are predictive of higher amounts of anxiety and depression in an adult population, among our early underserved adolescent sample, results show that fitness/health motivations (“I exercise because . . . I want to be more physically fit”; “. . . I want to maintain well-being”) are inversely related to internalizing problems. Research suggests that adults’ body image satisfaction is increasingly related to/associated with the competence or functionality of their bodies’ as they age (Reboussin et al., 2000). Although fitness/health and appearance motivations may be interwoven in adults, our findings suggest that youth may not relate body image to physical health as strongly as adults and that fitness/health motivations may be classified as more intrinsic (a form of competency) in this population. The high correlation between fitness/health motivations and intrinsic motivations (r = .706) supports this assertion.
Moderation models further contribute to our understanding of exercise motivations as an important mechanism to consider for understanding the relation between MVPA and internalizing problems during early adolescence. First, our findings demonstrate intrinsic motivations as a critical mechanism to foster in youth PA settings. Specifically, as predicted, results indicate that intrinsic motivations moderate the relation between MVPA and internalizing problems, whereby MVPA is highly protective against internalizing problems when intrinsic motivations are high but could play an iatrogenic role when intrinsic motivations are low. In fact, individuals who engage in high amounts of MVPA but have low intrinsic motivations for PA have the most internalizing problems of any subgroup of youth. These findings expand on the work of past research (Gillison et al., 2006; Standage et al., 2012) as our study is the first to look directly at the effects of internalizing problems in an underserved sample of adolescents and utilize a more rigorous sample of PA (i.e., accelerometers). As expected, our findings also indicate that extrinsic motivational orientations for PA are linked to higher internalizing across youth of all PA levels. That is, among highly active youth, extrinsic motivations appear to undermine any positive impact that PA may have on lowering the risk of youth internalizing.
Further examination of the various types of intrinsic motivations suggests that targeting/fostering enjoyment motivations within a PA setting may have the largest impact on youth well-being. It may be the case that those who do not endorse enjoyment motivations for PA may feel as though the activity in which they engage in PA is a burden to them. Most PA opportunities for youth involve participation in an organized sport and there is literature which suggests that stress, burnout, or parental pressure can all undermine enjoyment (Coakley, 1992; Smith, 1986). Another possibility is that some of those who endorse having less enjoyment-related motivation for PA, but yet are highly active, may be engaging in PA for reasons related to body dissatisfaction and appearance, or another maladaptive motivational orientation that has not been identified in previous theory or research. Future work can be done to assess to further understand the process by which motivations are driving this finding.
There were a few limitations to note in the current study. First, the composite scales used to represent intrinsic and extrinsic motivations were significantly correlated (r = .664, p < .001; see Table 1). The positive relation between intrinsic and extrinsic motivations may be driven primarily by fitness/health motivations which exhibit primarily intrinsic properties despite being utilized to form the composite Extrinsic Motivation Scale. Although this appears to be a limitation of our study, it may also suggest that individuals who are motivated to exercise have a broad motivational profile in which they garner motivation to exercise from various avenues which are both intrinsic and extrinsic. Future research should conduct pattern-centered analyses to identify how these intrinsic and extrinsic motivations may interact in unique ways to influence the relation between PA and internalizing problems. Despite the correlation between motivational orientations, when entered into the model together, the majority of the motivational subscales still contributed unique variance in explaining internalizing problems. There are also limitations in the extent to which the study is generalizable being that the sample is primarily low income and African American (73%). Being that this population is understudied and at particularly high risk for inactivity, obesity, and depression, the current study makes multiple critical and novel contributions to research and practice as it relates to supporting the health and well-being of adolescents in this specific demographic. However, interpretations of these findings should not be generalized broadly across other demographics. Finally, given the cross-sectional nature of the current study, there are limitations in the extent to which causal inferences can be made, however these findings provide preliminary evidence that emphasizes the need for PA interventions to consider motivations. Reducing appearance-related motivations and increasing enjoyment-related motivations will lead to more effective PA interventions that can increase PA (Ryan et al., 1997), mitigate potential iatrogenic effects of maladaptive motivations for PA on youth internalizing, and improve mental health through the facilitation of more adaptive motivations identified in the current study.
Conclusion
The results of the current study provide preliminary evidence to suggest that the inconsistent effects of PA on internalizing problems seen in the literature may be due in part to the moderating effects of motivations to exercise. Specifically, results indicate that PA is only related to fewer internalizing problems when intrinsic motivations are high and may be iatrogenic when intrinsic motivations are low in a sample of underserved early adolescents. Given the increased interest in the development of PA interventions to address the high obesity rates specifically in this population, the findings in the study can be used to guide the development of interventions targeting individuals during the critical early adolescent years. Furthermore, the findings of the current study provide evidence to suggest the importance of assessing and adjusting adolescents’ motivations to exercise given the significant relations between motivations to exercise and internalizing problems. Future studies should assess the effects of motivations, particularly social motivations, using prospective designs and path-centered approaches across broader populations that can expand on these findings and identify the long-term effects of different motivational profiles.
Footnotes
Acknowledgements
We thank our after-school program community partners and our intervention team and measurement team.
Ethical Approval
All procedures performed involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent/assent was obtained from all participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute Of Child Health & Human Development of the National Institutes of Health under Award Number R21HD077357 (Zarrett, PI) the National Institute of Nursing Research of the National Institute of Health under award number 1R01NR018619-01 (Zarrett, PI). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.