
Abstract
Childhood adversities have been linked to externalizing problems in adolescence. However, studies focusing on early adolescence are rare. Even less empirical attention has been given to the unique and joint influences of children’s and maternal childhood adversity on children’s externalizing behavior, particularly with a keen focus on the nature of adversities. This study examined the influences of children’s and maternal childhood adversities on children’s externalizing problems in early adolescence, delineating domains of childhood adversities. The data came from a longitudinal study of teen mothers and their children (N = 495). The findings reveal children’s childhood maltreatment experience was associated with externalizing problems in early adolescence. Further, maternal childhood maltreatment functioned as an additive risk source for target adolescents’ externalizing problems. These findings support the need to delineate adversity domains to further clarify the link between childhood adversity and externalizing problems. Our findings also support a multigenerational approach in pediatric settings.
Keywords
Introduction
Experiences of adversity in childhood are well-established risk factors for negative health outcomes later in life (Hughes et al., 2017; Kalmakis & Chandler, 2015; McLaughlin, 2016), including externalizing problems in adolescence (Fava et al., 2019; Negriff, 2020). Childhood adversities include risk factors before age 18, such as child maltreatment and household dysfunction (e.g., domestic violence, parental mental health problems; Felitti et al., 1998).
Despite shedding important light on the role of childhood adversity, the existing science base is limited in three important ways. First, studies focusing on early adolescence (10–14 years old) are rare, with very few exceptions (e.g., Fava et al., 2019). Yet early adolescence represents a critical developmental juncture for externalizing problems. The onset of puberty, signaling biological maturation, typically occurs in early adolescence (National Center for Biotechnology Information, 2011) and profound physical and cognitive changes follow (Blakemore et al., 2010; Steinberg, 2019). Such rapid biological changes likely trigger the “maturity gap” between biological and social maturation in early adolescence, which has been identified as the key driver behind increased engagement in externalizing problems (Agnew, 2003; Bloch & Niederhoffer, 1958; Moffitt, 1993). Consistently, these behavioral problems start emerging more prominently during this developmental period (Figge et al., 2018). Considering that early detection and timely intervention are arguably the most effective strategies to curb the emergence and escalation of externalizing problems across multiple life spans, focusing on externalizing problems in early adolescence and clarifying the role of childhood adversities in these behavioral problems are important.
Second, prior studies have typically operationalized childhood adversity using the cumulative risk approach (Rutter, 1979; Sameroff, 2000)—adversity items are summed to form a cumulative adversity index without reference to specific type or source of adversity (Centers for Disease Control and Prevention, 2016; Evans et al., 2013). A summative risk approach features the ability to capture constellations of risk factors, parsimony, and relative robustness against possible collinearity among adversity measures and to represent intensity of adversity exposure (Elkins et al., 2019; Evans et al., 2013). However, a summative cumulative risk index incurs a distinct disadvantage—it implies that each childhood adversity equally contributes to the outcome without any reference to the specific nature of childhood adversities (Evans et al., 2013; McLaughlin & Sheridan, 2016). Consequently, specific implications for the design of effective service and intervention strategies can be easily obscured (Evans et al., 2013; McLaughlin & Sheridan, 2016).
With this reflection, the field increasingly has emphasized the importance of unpacking the nature of childhood adversities (Greeson et al., 2014; Negriff, 2020) and encouraged scholars to move beyond the traditional cumulative risk index approach (Evans et al., 2013; McLaughlin & Sheridan, 2016). A dimensional (McLaughlin & Sheridan, 2016) or risk domain (Evans et al., 2013) approach has been proposed as a convincing alternative, which organizes the range of childhood adversity measures into a few higher-order constructs of cumulative risk. This approach retains the advantages of the cumulative risk approach, such as parsimony and relative robustness against possible collinearity among adversity measures, without completely obscuring the nature of a given childhood adversity measure. Building on the dimensions identified (Felitti et al., 1998) and adopted (e.g., Negriff, 2020; Ryan et al., 2000) in the literature on childhood adversities, the current study delineated childhood adversities into two dimensions—child maltreatment and household dysfunction.
Prior relevant studies adopting the dimensional approach have generated mixed findings. Some studies have reported that child maltreatment shows stronger effects on adolescent externalizing problems (Negriff, 2020), whereas others reported that household dysfunction does (Higgins & McCab, 2003; Ryan et al., 2000). The equivalent predictive capacity of child maltreatment and household dysfunction for externalizing behavior problems in adolescence has also been observed (McLaughlin et al., 2012; Schilling et al., 2008). It is feasible that the two domains of childhood adversities may have varying predictive capacity for externalizing problems in early adolescence, but existing evidence regarding adolescence is inconclusive and evidence with a keen focus on early adolescence does not exist. By improving our understanding of the predictive validity of different domains of childhood adversities and externalizing problems in early adolescence, the current study contributes to the emerging goal of “unpacking risk factors” (Greeson et al., 2014; Layne et al., 2010) and contextualizes this goal in early adolescence.
Third, less empirical attention has been given to the influences of maternal childhood adversity on the next generation (Stargel & Easterbrooks, 2020; Stepleton et al., 2018). The life course perspective (Braveman & Barclay, 2009; Hertzman & Power, 2003) and developmental psychopathology (Cicchetti & Toth, 2009; Sroufe, 2007) suggest that maternal childhood adversities, which are distal in time, may contribute to the linkage between offspring’s childhood adversities, which are proximal in time, and mental health in adolescence. Mothers’ childhood adversity may be a key distal factor, shaping children’s developmental outcomes by biological factors (e.g., compromised allostasis and neural functioning and elevated inflammation in mothers; Danese & McEwen, 2011; Perry & Pollard, 1998), epigenetic ramifications (Lindsay et al., 2020; Monk et al., 2012), or maternal psychosocial distress (Doi et al., 2020; Letourneau et al., 2019; Russotti et al., 2021). Consistently, an emerging body of literature has documented the predictive capacity of maternal childhood adversity for externalizing problems in children at age 8 (Stargel & Easterbrooks, 2020; Stepleton et al., 2018) and age 9 (Schickedanz et al., 2018; Stepleton et al., 2018) and between ages 5 and 13 (Lee et al., 2022). None of these studies has focused on early adolescence. Even fewer studies have examined whether different domains of maternal childhood adversity (i.e., child maltreatment vs. household dysfunction) have differential associations with children’s externalizing problems, with few exceptions. For instance, Stargel and Easterbrooks (2020) showed that mothers’ childhood experience with household dysfunction might be particularly salient for children’s externalizing problems. The equivalent predictive capacity of mothers’ childhood maltreatment and household dysfunction has been also reported for children’s behavioral health problems (yet not specific to externalizing problems; Schickedanz et al., 2018).
The scientific base for maternal adversity and its role in how their children’s adversity shapes externalizing problems beyond childhood is scarce. Relatedly, it is unknown in what functional ways maternal childhood adversity plays a role. Two hypotheses can guide an inquiry into the interplay between proximal (i.e., offspring’s childhood adversities) and distal (i.e., maternal childhood adversities) risk factors—common determinant and additive effect hypotheses. The common determinant hypothesis (Ben-Shlomo & Kuh, 2002; Kuh et al., 2003; Sroufe, 2007) suggests that maternal childhood adversities might function as shared risk sources that drive offspring’s earlier adversities and externalizing problems in early adolescence. The additive effect hypothesis (Braveman & Barclay, 2009; Hertzman & Power, 2003; Kuh et al., 2003) suggests that maternal childhood adversities have an independent impact on offspring’s externalizing problems in early adolescence beyond their childhood adversities. No identified studies have empirically evaluated these possibilities, let alone with a keen focus on offspring’s early adolescence, leaving untapped an opportunity to reveal a novel intervention target for externalizing problems during early adolescence.
Further, few relevant studies have focused on early adolescents born to teen mothers. Despite substantially declining during the past 2 decades, the U.S. teen birth rate (per 1,000 girls aged 15–19 years) remained at 16.7 in 2019 (Martin et al., 2021), placing the United States at the highest risk of teen pregnancy among other Western countries (Sedgh et al., 2015). Around the globe, an estimated 15% of young women give birth as a teenager (United Nations Department of Economic and Social Affairs Population Division, 2021). Youth born to teen mothers experience increased risk of externalizing problems (Lee et al., 2020) and childhood adversities (Easterbrooks et al., 2019). Further, young mothers are more likely than older mothers to experience childhood adversity (Hillis et al., 2004; Madigan et al., 2014). Thus, this population features youth with substantially high risk and enables meaningful examination of the complex interplay of offspring’s and maternal childhood adversities and offspring’s externalizing problems in early adolescence, contributing to the science base regarding the intergenerational influences of adversities on mental health among high-risk youth.
Current Study
Childhood adversity has been consistently recognized as a risk factor for externalizing problems in adolescence. However, influences of childhood adversity on externalizing problems during early adolescence have received less empirical attention, let alone among early adolescents born to teen mothers. Further, even less empirical attention has been given to the unique and joint influences of maternal childhood adversity on the next generation, although maternal childhood adversity may be an important yet understudied distal factor affecting the association between a child’s earlier adversity and externalizing problems in early adolescence.
To fill these critical gaps in prior studies, the current study examined unique and joint influences of children’s and maternal childhood adversities on externalizing problems among early adolescents born to teen mothers. The current study evaluated two central research aims. First, it tested the impacts of two childhood adversity domains for the target children—child maltreatment (e.g., child physical abuse) and household dysfunction (e.g., domestic violence, parental substance use)—on externalizing problems in early adolescence among high-risk youth. Considering mixed empirical evidence on the differential associations of two domains on youth’s externalizing problems, we did not formulate a directional hypothesis regarding the domains of childhood adversity. Second, the current study evaluated whether maternal childhood adversity contributed to the association between target children’s childhood adversity and externalizing problems in early adolescence and if so, in what functional ways (i.e., common determinant vs. additive risk). The common determinant hypothesis posits that maternal childhood adversities might function as a shared source that drives both childhood adversities and externalizing problems in early adolescence for the target children. The additive risk hypothesis suggests that maternal childhood adversities will function as an independent risk source for the target children’s externalizing problems in early adolescence beyond the children’s childhood adversities. Because few studies have incorporated both children’s and mothers’ childhood adversity in the context of children’s developmental outcomes, a specific directional hypothesis could not be generated.
Method
Study Design and Sample
Recruitment
The data were from the Young Women and Child Development Study, a longitudinal panel study examining the comprehensive developmental outcomes of two cohorts of teen mothers and their offspring (Lee et al., 2017; Yoon et al., 2019). Data collection began in 1988 for Cohort 1 (C1) and 1992 for Cohort 2 (C2) and concluded for both cohorts in 2007. Recruitment for participants occurred in health and social services agencies in three urbanized counties in a northwest region of the United States. Eligibility criteria for enrollment were pregnant adolescents aged 17 years or younger, unmarried, planning to carry their baby to term at the time of enrollment, and able to speak English. The study enrolled 495 pregnant adolescents (n = 240 for C1; n = 255 for C2).
Participants
At the initial interview, the participants were 16.07 years old on average (SD = 1.01), 71.5% did not have any prior pregnancy, 81% used public assistance as their main financial source, and they reported 9.31 (SD = 1.30) years of schooling on average. No significant cohort differences were found regarding racial and ethnic composition of people of color, χ2 (1) = 2.541, p = .111; average age at intake, t (493) = 0.775, p = .439; prior pregnancies, χ2 (1) = 0.005, p = .942; and having mothers who dropped out of high school, a proxy measure for socioeconomic status in the family of origin, χ2 (1) = 0.799, p = .371. The current study focused on data collected at pregnancy and 4.5, 6, 10.5, and 11.5 years. At these follow-up points, 84%, 82%, 81%, and 83%, respectively, of the original sample was retained across the two cohorts. No systematic association was found between nonparticipation at each wave and race and ethnicity (racial and ethnic minority vs. not), maternal age, and grandmothers’ educational attainment (high school dropout vs. not). The sample was racially diverse (34.2% White, 24.8% African American, 10.9% Hispanic, and 30.1% mixed or other racial groups), but had slightly lower representation of girls among children (41.8%).
Procedure
Assessments were conducted at participants’ home or by telephone. Mothers were interviewed using a structured study questionnaire preprogrammed on laptop computers. Interviews typically took approximately 2 hours. The current analysis used a subset of the questionnaires. Parental or guardian consent was obtained for participants who were not emancipated minors. The study was approved by the human subjects review committee at the affiliated universities.
Measures
Target Child’s Childhood Adversity (Ages 4.5, 6, and 10.5)
Childhood Adversity Constructs and Measures.

aPositive endorsement of any item was coded as 1 (i.e., exposure to a given adversity).
Teen Mothers’ Childhood Adversity (Before Age 19.5)
As with the offspring’s childhood adversity measure, the definition of childhood adversity in the original ACEs study (Anda et al., 2002) guided the operationalization of maternal childhood adversity. Nine items, reported by mothers, mapped onto the original 10 ACEs items (see Table 1 for items). Maternal childhood adversity was assessed prior to the maternal age 19.5 assessment that captured mothers’ experiences prior to age 18.5, except for three retrospective items about physical abuse, parental substance use, and being in foster care for C1 and one retrospective item about sexual abuse in childhood for C2. When mothers positively endorsed a given adversity item, the item was coded as 1, indicating that mothers experienced that adversity at a given data point. These dichotomized measures were then summed into a single indicator across waves, representing mothers’ exposure to a given childhood adversity across the assessment periods. Finally, these items were summed to create a total maternal childhood adversity score, which ranged from 0 to 8. Two domains of maternal childhood adversity were also created.
Children’s Externalizing Problems during Early Adolescence (Target Child’s Age 11.5)
Externalizing problems were measured using the Child Behavior Checklist (Achenbach, 1991), a widely used 118-item parent-reported assessment tool for children’s functioning, when children were aged 4–18. Each item was rated on a 3-point scale (0 = not true, 1 = somewhat or sometimes true, and 2 = very true or often true), summed to raw scores, and then converted to t-scores for externalizing problems (α = .89, M = 55.20, SD = 10.95).
Covariates
Covariates included child’s gender, race (racial and ethnic minority vs. not), cohort group (C1 vs. C2), and grandmother’s educational attainment (high school dropout vs. not) as a proxy for socioeconomic status in the family of origin. Youth externalizing problems at age 4.5, the earliest assessment available, were added as a covariate.
Analyses
The analysis strategy was divided into two parts. First, the study tested the main effect of two domains of the target children’s childhood adversity (i.e., maltreatment vs. household dysfunction) on their externalizing problems during early adolescence (age 11.5). Second, maternal childhood adversity was added to the models with the target children’s adversity. This analysis examined whether maternal childhood adversity functioned as a common determinant or additive factor in the association between children’s earlier adversity and externalizing problems during early adolescence. If the coefficient for children’s adversity substantially attenuated and lost its statistical significance when maternal childhood adversity was added, such results would support the common determinant hypothesis. On the other hand, if the coefficient for children’s adversity remained unchanged and the coefficient for maternal childhood adversity was statistically significant beyond the children’s adversity measure, then the additive effective hypothesis would be supported (Hertzman & Power, 2003; Kuh et al., 2003). For all analyses, multiple regression was used and all covariates (i.e., gender, race, grandmother’s educational attainment, and earlier externalizing problems at age 4.5) were included. Missing data were handled with full information likelihood estimation, as recommended (Schlomer et al., 2010). Given that the retention rate was high, no systematic attrition pattern was found, and full information likelihood estimation was used, estimation bias due to attrition is highly unlikely. All analyses were conducted in Mplus version 8 (Muthén & Muthén, 2017).
Results
Descriptive Statistics of Childhood Adversity (N = 495).

aMaltreatment for children = emotional abuse and physical abuse. Maltreatment for mothers = emotional abuse, physical abuse, sexual abuse.
bHousehold dysfunction for children = food or money insecurity, parental divorce, intimate partner violence, maternal substance use, maternal depression, and maternal arrest. Household dysfunction for mothers = food or money insecurity, parental divorce, parental substance use, parental death, parental incarceration, and being in foster care.
Correlations among Study Variables.
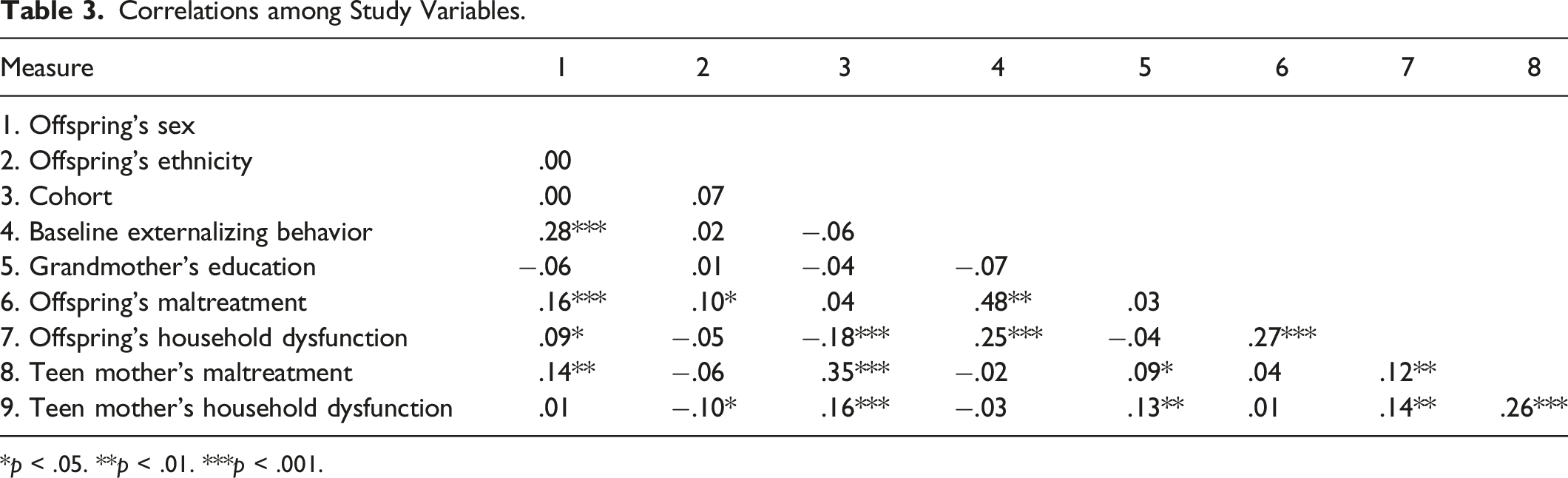
*p < .05. **p < .01. ***p < .001.
Multiple Regression of Testing the Effect of Offspring’s and Maternal Childhood Adversity on Children’s Externalizing Behavior at Age 11.5, Standardized (β) and Unstandardized (b) Coefficients.

Note. All covariates (i.e., gender, race, grandmother’s educational attainment, and earlier internalizing or externalizing problems at age 4.5) were controlled for in all models.
*p < .01. **p < .001.
Model 2 expanded Model 1 by including maternal childhood adversity to evaluate whether this led to substantial changes in the association between target child’s childhood adversity and externalizing problems at age 11.5 (i.e., common determinant) or functioned as an additional source of risk (i.e., additive effect). Mothers’ childhood maltreatment experiences emerged as a statistically significant predictor for externalizing problems (β = .11, p < .01), beyond the target children’s childhood maltreatment, which remained statistically significant without any substantial changes in the magnitude of corresponding coefficient.
Discussion
The current findings reveal child maltreatment prior to age 10.5 was associated with externalizing problems among young adolescents. Further, maternal child maltreatment functioned as an additive risk source for externalizing problems among youth.
Consistent with prior studies (Negriff, 2020) but in contrast to others (Ryan et al., 2000), target children’s childhood maltreatment, not household dysfunction, was predictive of children’s externalizing problems in early adolescence. The current study findings add to an emerging body of literature by demonstrating the need to explore more nuanced associations between types of childhood adversities and mental health (Ryan et al., 2000). This work contributes to prior efforts to understand risk source (Greeson et al., 2014) and take a dimensional (McLaughlin & Sheridan, 2016) or risk domain (Evans et al., 2013) approach (i.e., delineating child maltreatment vs. household dysfunction in the current study) to identify targets for primary prevention to reduce the impact of childhood adversities on children’s developmental outcomes in early adolescence. Various possible mechanisms have been suggested to explain the link between childhood maltreatment and externalizing behavior problems (Jaffee, 2017), such as compromised competence to respond to social provocations (Kay & Green, 2016), biased attention to negative emotion (Shackman & Pollak, 2014), and challenges with emotion regulation (Heleniak et al., 2016). Evaluating these possible mechanisms among early adolescents born to teen mothers might be a fruitful future direction to locate targets for secondary prevention strategies for these high-risk youth.
It is puzzling why the target children’s childhood maltreatment experience, but not household dysfunction, influenced their externalizing problems in early adolescence. Considering that the strategy of unpacking risk factors is relatively nascent in the context of childhood adversities, it is hard to pinpoint what leads child maltreatment to drive the link between target children’s childhood adversities and their externalizing problems. However, there might be two possibilities. First, it might be the unique nature of this population and its highly elevated rates of risks related to household dysfunction. For example, 35.8% of the study sample witnessed domestic violence, a household dysfunction item, compared to 6% in a nationally representative sample (Sacks & Murphey, 2018). Such high risk in the household dysfunction domain may limit its predictive capacity in a high-risk sample (i.e., youth born to low-resourced teen mothers). A prior study documenting that child maltreatment drives the link between childhood adversities and children’s externalizing behavior problem also relied on a sample with elevated rates of household dysfunction (38% reported domestic violence, for example; Negriff, 2020). It is feasible that child maltreatment is a prominent predictor, particularly in high-risk samples. Second, the two domains of childhood adversities may map onto different types of mental health outcomes across stages of adolescence (e.g., early adolescence vs. later adolescence). Child maltreatment, for example, was more strongly associated with internalizing behavior problems, whereas household dysfunction was a stronger predictor of externalizing behavior problems among older adolescents (mean age = 16.44; Ryan et al., 2000). Evaluating this inquiry in a general population with both externalizing and internalizing outcomes across adolescence might be a fruitful future direction to further evaluate the salience of household dysfunction items.
Expanding on prior studies documenting the linkage between mothers’ childhood adversity and children’s externalizing problems in earlier developmental periods (Letourneau et al., 2019; Schickedanz et al., 2018; Stargel & Easterbrooks, 2020; Stepleton et al., 2018), the current study revealed that the effects of maternal childhood adversity on offspring extended into early adolescence. Specifically, the current findings support the additive effect hypothesis, suggesting that maternal childhood adversity may function as another risk source that generates unique influences on the next generation’s externalizing problems.
As with the target children’s childhood adversity, our study findings suggest that mothers’ experiences with child maltreatment may drive the intergenerational impact of childhood adversity. Because the strategy of unpacking risk factors in the context of intergenerational influences of childhood adversities is highly rare, it is hard to determine precisely why maternal childhood maltreatment experience emerged as a driving force. In addition to the speculations offered previously in the context of target children’s childhood adversity, the intergenerational impact of maternal childhood maltreatment can be seen through other lenses. Mothers with a history of childhood maltreatment may experience a “chain of risk” and struggles throughout their life course transitions (Boden et al., 2008), such as elevated mental distress that can compromise children’s developmental outcomes including externalizing problems (Doi et al., 2020; Letourneau et al., 2019; Russotti et al., 2021). A biological mechanism might be also feasible. Disrupted allostasis and neural functioning and elevated inflammation in mothers with childhood maltreatment (Danese & McEwen, 2011; Perry & Pollard, 1998) may trigger an epigenetic process in children that leads to compromised developmental outcomes (Lindsay et al., 2020; Monk et al., 2012), although it remains unclear whether such biological factors function as a mechanism underlying the link between maternal childhood maltreatment and offspring’s externalizing problems specifically. Future studies that collectively evaluate these factors and elucidate the mechanisms underlying these intergenerational influences of maternal childhood maltreatment are warranted. Considering that the additive effect of maternal adversity was present for young adolescents’ externalizing problems in the current study, integrating the developmental nature of externalizing behavior in childhood and adolescence may also further clarify the mechanisms generating the intergenerational influences of maternal adversity.
The current findings should be contextualized with this study’s methodological limitations. First, the study sample included teen mothers and their children who resided in three urbanized counties in a northwest region of the United States. Focusing on teen mothers and their children in early adolescence was an intended focus of our study to explicate the interplay between children’s and mothers’ childhood adversity in a high-risk sample. However, this intentional focus may limit the generalizability of study findings to a general population due to characteristics unique to the study sample. Teen mothers, for example, may rely on their parents more so than older mothers and thus, the direct association found between teen mothers’ childhood adversity and children’s externalizing behavior might be more prominent in this population. However, in the study sample, by the children’s age of 11.5, 9.2% of mothers lived with a parent figure (i.e., children lived with a grandparent figure), which is comparable to the percentage of children living with a grandparent reported in a representative sample of U.S. families (7%; Dunifon et al., 2018). As such, it is reasonable to think that the influences of grandparents may not introduce bias to the estimation, easing this concern to some degree. Nevertheless, extrapolating the current findings beyond the study sample should be performed with caution, and replicating the study findings using other longitudinal data with a general population might be a fruitful direction in this line of inquiry. Second, all measures relied on mothers’ self-report, which could introduce social desirability bias due to the sensitive nature of childhood adversity. The issue of shared method variance across measures might also have affected results. Third, teen mothers’ earlier externalizing behavior based on the Child Behavior Checklist was not available and thus, could not be controlled. Considering that a link between mothers’ and children’s externalizing problems has been reported (Schulz et al., 2021), incorporating mothers’ externalizing problems in this line of inquiry might be a fruitful future direction. Fourth, as with other studies on teen parents (Mollborn & Lovegrove, 2011), experiences of teen fathers were not considered and thus, the current study might have underestimated the effects of parental childhood adversity on children’s externalizing problems in early adolescence. Although maternal childhood adversity tends to have more prominent influences on child developmental outcomes than paternal childhood adversity, particularly at the higher end of the distribution of childhood adversity (Folger et al., 2018; Schickedanz et al., 2018), disentangling the interplay between these two sources of intergenerational childhood adversity represents an important next step. Fifth, current study findings represent mostly White and Black ethnic and racial groups. Future studies with other ethnic and racial groups, particularly Latinx children born to teen mothers, are imperative. In the United States, disproportionately heightened rates of teen pregnancy have been reported for young Latinas (U.S. Department of Health & Human Services, 2018). Further, Latinx young mothers face a unique set of risk factors, cultural contexts, and gender norms in the United States (Aparicio et al., 2014; Coleman-Minahan, 2017), which may influence the associations examined in the current study.
Despite these caveats, the present study advanced prior research in two important ways. First, it delineated childhood adversity into two subdomains, child maltreatment and household dysfunction; revealed a nuanced association between childhood adversity and externalizing problems in early adolescence; and thus, contributed to the ongoing efforts to unpack the risk source in early adolescence. Second, the role of maternal childhood adversity was evaluated in the context of the target children’s childhood adversity and externalizing problems in early adolescence. Our study findings extend prior studies that examined the intergenerational impact of childhood adversity but have been limited to early childhood and have not considered the target children’s and maternal childhood adversity jointly. As with the target children’s childhood adversity, two domains of maternal childhood adversity were evaluated in our study, further clarifying the complex interplay among maternal childhood adversity, target children’s adversity, and target children’s mental health in early adolescence.
Conclusion
The findings from the current study reveal differential associations between two domains of childhood adversity and externalizing problems in early adolescence, indicating that more effort should be placed on assessing domains of childhood adversity. Specifically, results of this study reveal a more prominent role of maternal experience of childhood maltreatment, supporting the need for reflective dialogues about our current use of childhood adversity without any reference to its domains. Moreover, the findings from the present study reveal the deleterious effects of maternal child maltreatment on externalizing problems in the next generation, even during early adolescence. Our findings support a multigenerational approach in pediatric settings, advocating for the need to add maternal history of childhood trauma to prenatal assessment profiles (Racine et al., 2018; Sun et al., 2017). Further, considering that many young and low-income women receive late, inadequate, or no prenatal care compared to older pregnant women (Child Trends Databank, 2015; Sidebottom et al., 2017; Taylor et al., 2005), the merit of screening maternal childhood adversity during preventive pediatric health care beyond prenatal or postnatal periods, such as early adolescence, should be seriously considered. Developing a body of literature informing a proper form and appropriate implementation of a screening tool for maternal childhood adversity (Anda et al., 2020) is needed to facilitate adding this maternal risk to the assessment profile during preventive pediatric health care and thus, disrupting possible intergenerational influences of maternal childhood adversity.
Footnotes
Acknowledgments
We would like to extend our gratitude to YCDS study participants for their contribution to the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
This study was supported by grants HD097379 from National Institute of Child Health and Human Development, DA05208 from National Institute on Drug Abuse, and MH52400 and MH56599 from National Institute of Mental Health. The content of this paper is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies. The funding agencies played no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit this article for publication.