
Abstract
Background
PET-CT is widely used for evaluation and follow-up of malignancy. Incidental hypermetabolic lesions are often found on PET-CT, some of which are confirmed to be malignant.
Purpose
To estimate the role of combined Breast Imaging-Reporting and Data System (BI-RADS) assessment using mammography and sonography for evaluation of incidental hypermetabolic lesions on 18F-FDG PET-CT and to determine an appropriate next step.
Material and Methods
This study included incidental hypermetabolic lesions found in the breasts of 7594 women who underwent PET-CT at three university-affiliated hospitals between January 2006 and December 2011. We reviewed the maximum standardized uptake value (SUVmax) of incidental lesions, combined BI-RADS assessment of mammography and sonography, and final results. We analyzed the negative predictive values of the probably benign (categories 1–3) group and the sensitivity of suspicious (categories 4 and 5) groups according to combined BI-RADS assessment.
Results
Forty-three patients (0.6%) had 49 incidental hypermetabolic lesions in the breast. Histologic diagnosis in 17 patients confirmed nine breast cancers (27.3%). Sixteen patients underwent imaging follow-up for at least 2 years; no breast cancer was detected. Thirteen patients were lost to follow-up and were excluded. For the suspicious (n = 14) and probably benign (n = 19) groups according to combined BI-RADS assessment, both the sensitivity and negative predictive values were 100%. Using an optimal diagnostic cut-off value of 2.15, the malignancy rate was not significantly different (16.7% vs. 45.5%, respectively, in the group with SUVmax < 2.15 and the group with SUVmax ≥ 2.15; P > 0.05). The SUVmax of the confirmed malignant and assumed benign groups were not significantly different (3.1% vs. 2.2%, respectively; P > 0.05).
Conclusion
Both mammography and sonography should be considered the next step to evaluate incidental hypermetabolic lesions on 18F-FDG PET-CT because combined BI-RADS assessment provides an excellent negative predictive value for excluding malignancy.
Introduction
The clinical use of combined positron emission tomography (PET) and computed tomography (CT) with 18F-fluorodeoxyglucose (FDG) has been expanded over the last decade (1–4). 18F-FDG PET-CT can provide both functional and anatomical information concerning malignancies and has been an important imaging modality in clinical oncology. 18F-FDG PET-CT is commonly used for the initial staging, management of recurrent disease, and monitoring the response to therapy of malignancies; additionally, it is also useful for determination of activities in breast cancers such as locoregional status and distant metastasis (1–6).
With the increasing use of PET-CT in clinical oncology, hypermetabolic lesions detected in unexpected parts of the body may represent a synchronous cancer (7–11). The rate of incidental hypermetabolic lesions was reported to be 1.1–12.3%, and that of the second primary malignancy was reported to be 8.0–27.8% (7–10). Recently, PET-CT has also been used for cancer screening in asymptomatic healthy individuals with an incidental malignancy rate of 0.8–1.2% (12–15).
The rate of incidental hypermetabolic lesions in the breast has been reported to be 0.4–1.1% with a malignancy rate of 37.5–83.3% (16–21). However, uptake is not specific for malignancy, and may also include infection, fat necrosis, lactation, and benign breast tumors. Because the accuracy of the prediction of malignancy among incidental hypermetabolic lesions is limited, use of additional methods is required to reduce false-positive biopsies. Some researchers have attempted to evaluate hypermetabolic lesions using CT or sonography; however, the results were not promising (17,19).
During the past decade, the Breast Imaging-Reporting and Data System (BI-RADS) has been accepted worldwide, and it is known to provide a reasonable assessment of cancer risk (22). To our knowledge, however, no study concerning the role of BI-RADS in the evaluation of incidental hypermetabolic lesions has been reported. Thus, we aimed to estimate the role of combined BI-RADS assessment using mammography and sonography for evaluation of incidental hypermetabolic lesions on 18F-FDG PET-CT and to determine the appropriate next step.
Material and Methods
Patient selection
We received approval from the institutional review board of our institution, and the need for informed patient consent was waived. The study complied with HIPAA requirements.
We retrospectively reviewed the electronic medical records of 7594 consecutive women who underwent 18F-FDG PET-CT from January 2006 to December 2011 at three university-affiliated hospitals to identify incidental hypermetabolic lesions in the breast. PET-CT was performed to evaluate distant metastasis in patients with underlying malignancy (underlying malignancy group) or to screen malignancy in asymptomatic women during their health check-up (screening group). We excluded patients previously diagnosed with breast cancer. Among those with incidental hypermetabolic lesions in the breast, we also excluded patients without histologic confirmation and with an imaging follow-up of less than 2 years.
Image protocol
All patients underwent whole-body PET-CT using one of two first-generation scanners (Biograph2; Siemens Medical Solutions, Erlangen, Germany) (Gemini; Philips Medical Systems, Milpitas, CA, USA). Patients fasted for at least 6 h before the scan. Prior to injection of 18F-FDG, the blood glucose concentration was verified as <180 mg/dL. PET-CT was commenced 1 h after intravenous injection of 7.4 MBq (0.2 mCi) of 18F-FDG per kg body weight. Scans, including PET and non-enhanced CT, were acquired from the skull base to the proximal thigh from six to eight bed positions. The patient was placed in the supine position with both arms at the sides. PET was performed using an acquisition time of 150 s per bed position. CT was performed using a 5-mm slice thickness, 50 mAs, and 130 kVp. CT data were used for attenuation correction. PET images were reconstructed using a standard three-dimensional (3D) iterative algorithm (ordered subset expectation maximization [OSEM]) providing axial, sagittal, and coronal planes. OSEM reconstruction using two iterations and eight subsets and a post reconstruction Gaussian filter of 5 mm FWHM were applied for matrix sizes of 128 × 128, resulting in an image pixel size of 5.3 × 5.3 mm.
Patients with an incidental hypermetabolic lesion in the breast underwent diagnostic mammography and sonography. Mammography was performed using one of three full-field digital mammography units (Senograph DS®; GE Healthcare, Buc, France) (Senograph 2000D®; GE Healthcare, Buc, France) (Lorad Selenia; Hologic, Danbury, MA, USA). One of three experienced breast radiologists interpreted the mammography, and then performed bilateral whole-breast sonography using one of two high-resolution instruments (iU22®; Philips Medical Systems, Bothell, WA, USA) (LOGIQ E9; GE Healtcare, Milwaukee, WI, USA) with a 5- to 12-MHz linear array transducer.
Imaging interpretation
All PET-CT images were analyzed by one of three experienced nuclear medicine physicians. Visual assessment was performed to detect hypermetabolic lesions because semi-quantitative methods such as those that determine the standardized uptake value (SUV) do not improve the efficacy of visual assessment alone (23). Any focal uptake greater than that of background glandular tissue was considered abnormal, regardless of its intensity.
After detection of the hypermetabolic lesion, the maximum SUV (SUVmax) was obtained for semi-quantitative analysis. SUVmax represents the maximum uptake in the tumor volume of interest (VOI). We applied a 3D VOI using the threshold of 40% of the maximum pixel value of the lesion (24). VOI margins were verified to cover the area of interest in all three (axial, sagittal, and coronal) planes. The SUV calculation was as follows: SUV = region of interest (ROI) value/injected dose (ID)/body weight (BW). The SUV was normalized to the maximum ROI value (KBq/cc), ID (MBq), and BW.
One of three experienced breast radiologists performed sonography and interpreted mammography and sonography according to BI-RADS (22). The definition of BI-RADS assessment is as follows: category 1, negative; category 2, benign finding(s); category 3, probably benign finding – initial short interval follow-up suggested; category 4, suspicious abnormality – biopsy should be considered; category 5, highly suggestive of malignancy – appropriate action should be taken. For magnification mammography and sonography, category 4 lesions are subdivided as follow: 4A, low-suspicious finding; 4B, intermediate-suspicious finding; 4C, moderate-suspicious finding. We obtained combined BI-RADS assessment, indicating adoption of higher mammography and sonography categories. The patients were divided into two groups: those with a combined BI-RADS category 4 or higher (suspicious group) and those with a BI-RADS category 1–3 (probably benign group). The final results of incidental hypermetabolic lesions were obtained from histologic diagnosis or imaging follow-up of more than 2 years.
Statistical analysis
Statistical analysis was performed using the SPSS software, version 17.0 (SPSS Inc., Chicago, IL, USA). The Mann-Whitney test was used to compare the differences in the mean pSUV among the following groups: suspicious vs. probably benign groups according to combined BI-RADS assessment and confirmed malignant vs. assumed benign groups according to the final results. Additionally, the Mann-Whitney test was used to compare the difference in lesion size between the confirmed malignant and assumed benign groups. Receiver-operating curve (ROC) analysis was performed to determine the optimal diagnostic cut-off value of the SUVmax. Pearson’s chi-squared test was performed to compare the final results of suspicious and probably benign groups according to combined BI-RADS assessment. A P value < 0.05 was deemed to indicate a statistically significant difference.
Results
Forty-three patients (0.6%) had incidental hypermetabolic lesions in the breast among the 7594 women who underwent PET-CT. Thirteen patients were lost to imaging follow-up. Finally, 30 patients with 33 incidental hypermetabolic lesions were enrolled in the study (Fig. 1). Three patients had multiple lesions.
Flow chart of the patients with incidental hypermetabolic lesions in the breast. Loss, loss during imaging follow-up; SUVmax, maximum standardized uptake value.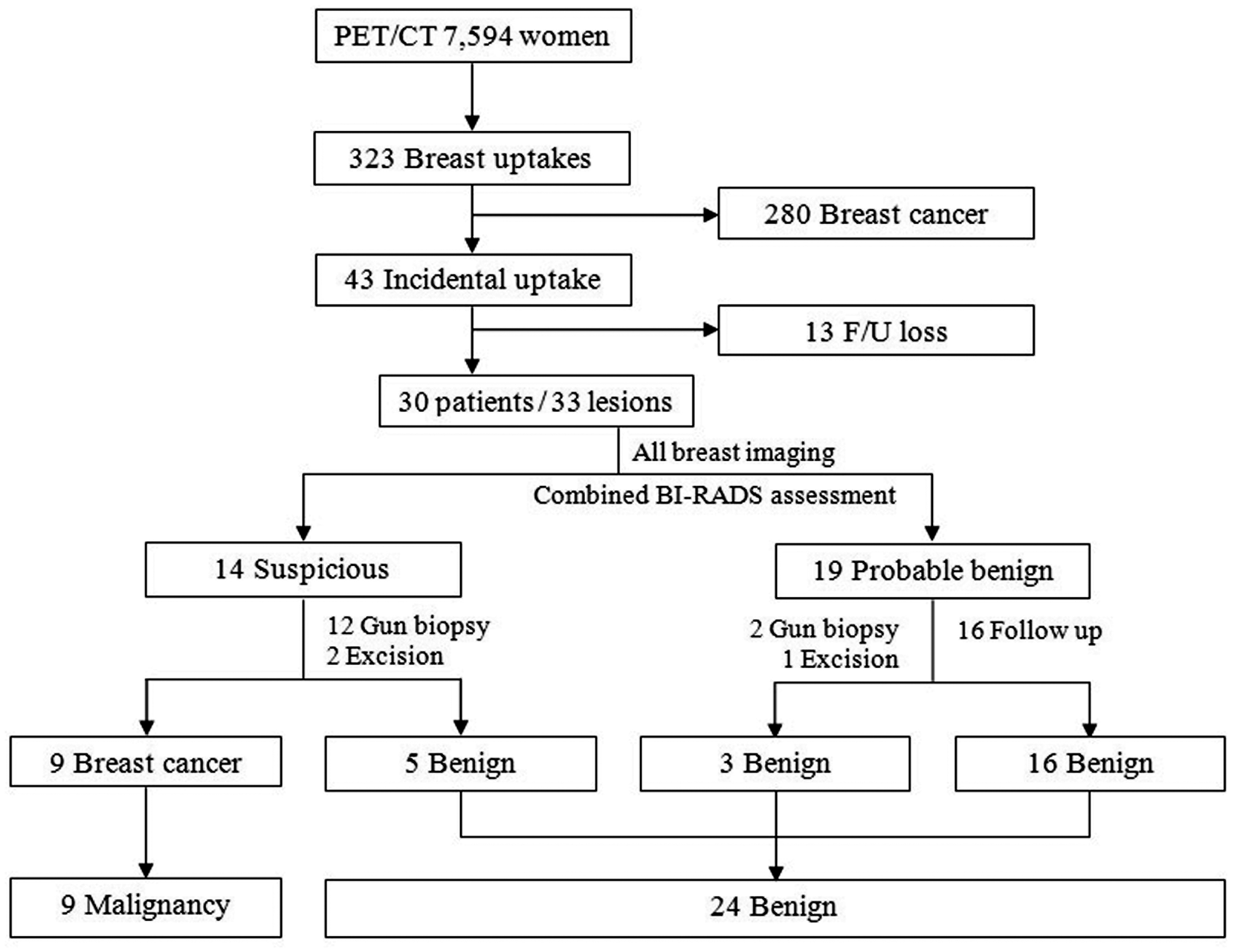
Among 33 incidental hypermetabolic lesions, 17 underwent gun biopsy (n = 14) or excision biopsy (n = 3), confirming nine malignancies and eight benign lesions (Fig. 1). Malignant lesions included invasive ductal carcinoma (n = 5), ductal carcinoma in situ (n = 3), and papillary carcinoma (n = 1). No metastatic lesion was found in the breast. All patients with incidental breast cancer underwent curative surgery, except for two who had unexpected distant metastasis in other areas of the body. Benign lesions included fibrocystic change (n = 3), fibroadenoma (n = 2), fat necrosis (n = 1), sclerosing adenosis (n = 1), and intraductal papilloma (n = 1). All excision biopsies revealed benign results, including fibroadenoma, sclerosing adenosis, and intraductal papilloma. No missed cancer was found in patients with biopsy-proven benign lesions during the follow-up period. The remaining 16 lesions underwent imaging follow-up for at least 2 years; their combined BI-RADS categories were negative (n = 13), benign (n = 2), and probably benign (n = 1). Follow-up modalities included PET/CT (n = 7), mammography only (n = 3), both mammography and sonography (n = 2), sonography only (n = 2), and CT (n = 2). The results of follow-up were negative (n = 15) or benign (n = 1). No missed cancer was found during the follow-up period; thus they were considered assumed benign lesions.
The mean age of enrolled patients was 48.4 ± 11.7 years (range, 30–80 years). We divided the patients into two groups according to a cut-off age of 45 years because the incidence of breast cancer in Korean females peaks during their late 40 s (25). Fourteen patients belonged to the younger group (mean age, 38.8 years), including four breast cancers, and 16 patients belonged to the older group (mean age, 56.7 years), including five breast cancers. All three patients with multiple hypermetabolic lesions belonged to the younger group; among them, one had bilateral breast cancer. The malignancy rates were 28.6% in the younger group and 31.3% in the older group, showing no significant difference (P
Twenty-three patients had an underlying non-breast malignancy, and seven patients were identified during cancer screening at a healthcare center. The sites of underlying malignancy were the gastrointestinal tract including the pancreas (n = 10), the head and neck including the thyroid (n = 7), the genital tract including the ovary (n = 4), and other sites including those of unknown origin (n = 3). Seven second primary breast cancers in the underlying malignancy group (30.4%) and two incidental breast cancers in the screening group (28.6%) were identified. The malignancy rates of the two groups were not significantly different (P
Summary of SUVmax and malignancy rate of each group.

N/A, not applicable; SUVmax, maximum standardized uptake value.
SUVmax, BI-RADS assessment, and final results of incidental hypermetabolic lesions.
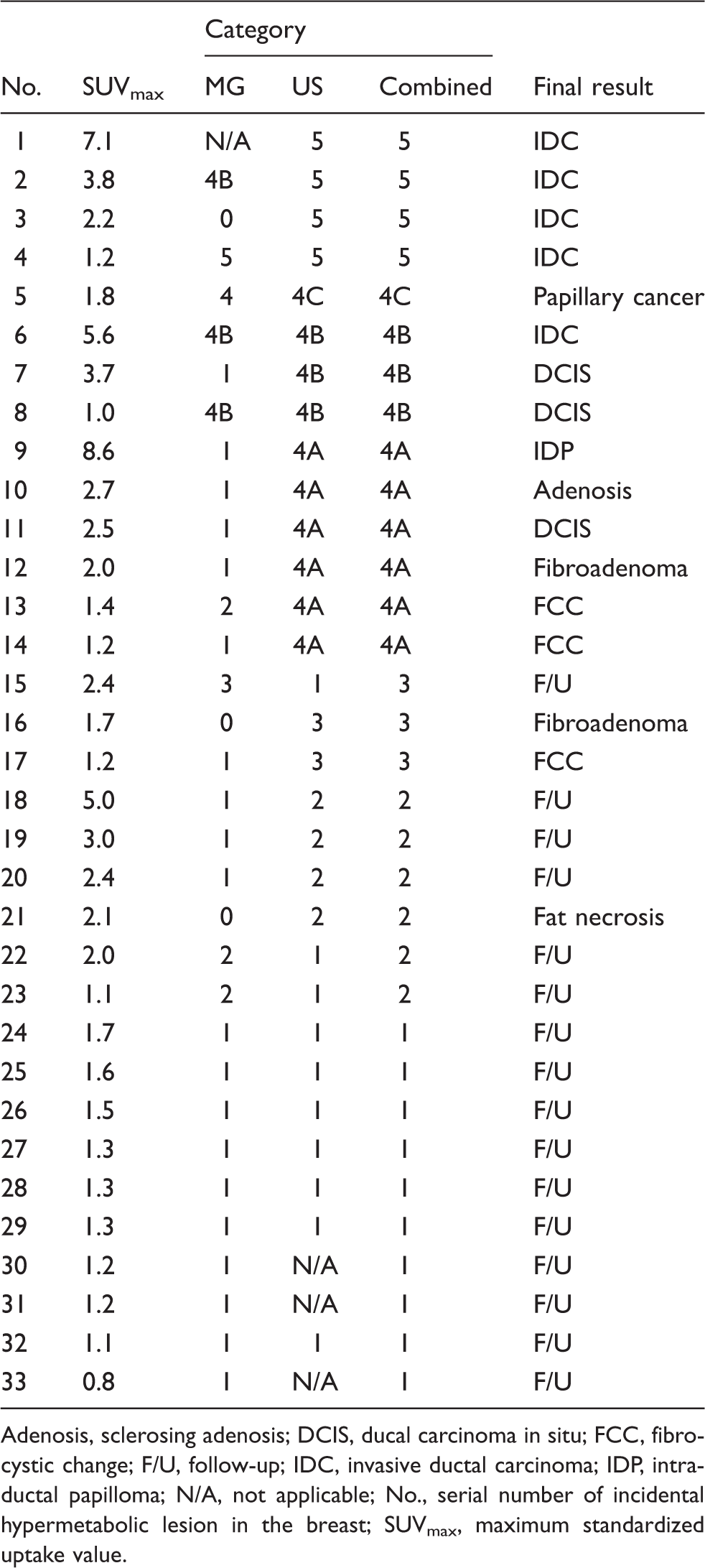
Adenosis, sclerosing adenosis; DCIS, ducal carcinoma in situ; FCC, fibrocystic change; F/U, follow-up; IDC, invasive ductal carcinoma; IDP, intraductal papilloma; N/A, not applicable; No., serial number of incidental hypermetabolic lesion in the breast; SUVmax, maximum standardized uptake value.
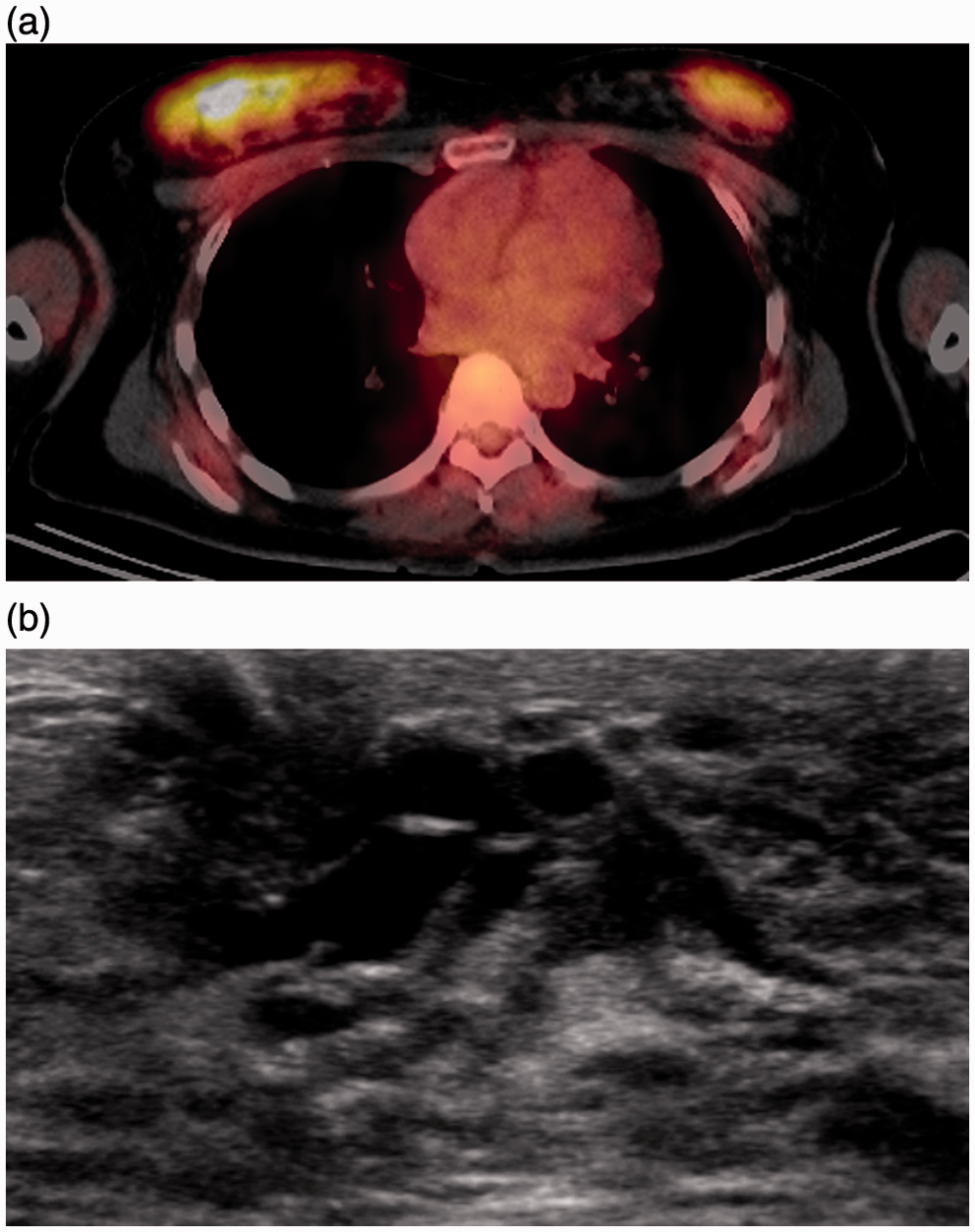
According to combined BI-RADS assessment using findings of mammography and sonography, 14 lesions were assessed as suspicious (category 4 or 5) (Fig. 2), and 19 lesions were assessed as probably benign (category 1–3) (Fig. 3). Histologic diagnosis was performed for all suspicious lesions, revealing nine malignant and five benign lesions. Three of 19 probably benign lesions underwent histologic diagnosis, confirming fibroadenoma, fat necrosis, and fibrocystic change. The other 16 probably benign lesions underwent imaging follow-up for at least 2 years, and no missed cancer was found. Combined BI-RADS assessment showed a sensitivity of 100% and specificity of 79.2%. The positive and negative predictive values were 64.3% and 100%, respectively. Based on combined BI-RADS assessment, the malignancy rate was higher in the suspicious group than in the probably benign group (64.3 vs. 0.0%; P < 0.001) (Table 1). However, the mean SUVmax of the suspicious and probably benign groups were not significantly different (3.15 vs. 1.89; P = 0.156) (Table 1).
A 58-year-old woman with underlying lung cancer. (a) Fusion axial PET/CT image shows a hypermetabolic lesion in the right upper central breast (SUVmax = 1.8). (b) Diagnostic mammography of the right breast reveals a 2-cm lobular indistinct isodense mass in the upper central-inner breast (arrow). (c) Diagnostic breast sonography shows a 1.9-cm irregular indistinct hypoechoic mass (arrowheads), which correlated with the PET/CT and mammography findings. Combined BI-RADS assessment using mammography and sonography was category 4C. A 14-G gun biopsy was performed, confirming papillary carcinoma. A 34-year-old woman with underlying cervical cancer. (a) Fusion axial PET/CT image shows a hypermetabolic lesion in the right-upper and left-upper outer breast (SUVmax = 5.0 and 3.0, respectively). Diagnostic mammography shows negative findings and extremely dense breasts (not shown). (b) Diagnostic sonography reveals no suspicious findings in both breasts but diffuse ductectasia due to breast feeding. Combined BI-RADS assessment using mammography and sonography was category 2. Follow-up PET/CT after 1 year (not shown) reveals no breast uptake. Incidental uptake in both breasts was associated with physiologic changes related to breastfeeding.
We divided the patients into two groups according to the final results. The mean size, based on sonography findings, of the confirmed malignant group was larger than that of the assumed benign group (2.6 ± 1.2 cm vs. 1.1 ± 0.4 cm, respectively; P
Discussion
In the current study, 43 (0.6%) patients had incidental hypermetabolic lesions in the breast on PET/CT. Nine of the 33 lesions (27.3%) were confirmed to be breast cancer. Combined BI-RADS assessment using mammography and sonography demonstrated both sensitivity and negative predictive values of 100%.
The incidence of incidental hypermetabolic lesions in the current study was lower than that of the Western population (0.8–1.1%) but higher than that of the Korean population (0.4%) (16–20). The former reflects the lower incidence of breast cancer in Korea (25), and the latter may be related to subjective visual assessment by the three nuclear medicine physicians. The malignancy rate in the current study was lower than that in other reports (37.5–83.3%) (16–20). This might be due to a higher proportion of excluded patients (23.3 vs. 0–9.0%) who underwent no histologic confirmation or insufficient follow-up.
For evaluation of incidental hypermetabolic lesions, some researchers attempted to differentiate malignancy and benignity using SUVmax. Kang et al. and Chae et al. reported that the SUVmax of malignant lesions were 3.9 and 3.7, respectively, and those of benign lesions were 1.9 and 2.0, respectively; the differences were statistically significant (19,20). In the current study, however, the SUVmax of malignant and benign lesions were 3.1 and 2.2, respectively, showing no significant difference. Similarly, both Kei et al. and Kwak et al. reported that the SUVmax of malignant and benign lesions in the thyroid and bowel were not significantly different (10,11).
The optimal diagnostic cut-off value for differentiation of malignancy and benignity in the current study was 2.15, which is similar to that reported elsewhere (19,20). However, hypermetabolic lesions with an SUVmax lower than the cut-off value were not always benign; 33.3% of incidental breast cancers had a SUVmax lower than the cut-off value. Kang et al. and Chae et al. reported similar results: 44.4% and 34.4% of incidental malignancies, respectively, had an SUVmax lower than the cut-off value (19,20). Thus, the usefulness of SUVmax for discrimination of malignancy and benignity among incidental hypermetabolic lesions is limited.
The SUVmax is relates to lesion size, and could be underestimated in smaller lesions. The mean size of the confirmed malignant group was significantly larger than that of the assumed benign group in the current study. The SUVmax of the confirmed malignant group was higher than that of the assumed benign group, but it was not significantly different. Thus, possible underestimation of the SUVmax of relatively small assumed benign lesions may have been overlooked in the current study.
Some researchers have attempted to differentiate malignancy and benignity using imaging studies. Litmanovich et al. reported that 85.7% of patients with negative chest CT findings were confirmed to have a malignancy; Kang et al. reported that 30.2% and 10.7% of non-suspicious lesions on the CT component of PET/CT and sonography, respectively, were confirmed to be malignant. Chae et al. reported that 5.0% and 12.0% of non-suspicious lesions on sonography and mammography, respectively, were confirmed to be malignant (17,19,20). However, the current study showed that combined BI-RADS assessment using mammography and sonography successfully differentiated malignancy and benignity among the incidental hypermetabolic lesions. Both the sensitivity of the suspicious group and the negative predictive value of the probably benign group were 100%. Thus, based on combined BI-RADS assessment, unnecessary biopsy or further evaluation can be avoided in the probably benign lesions.
Kang et al. denied the role of mammography for the evaluation of incidental hypermetabolic lesions due to the limitations of dense breast (20). However, in the current study, six of nine incidental breast cancers showed positive findings on mammography. The difference in mammographic positivity among the two studies might be related to cancer size (1.7 vs. 2.5 cm).
The current study possessed some limitations. First, relatively small numbers of patients were enrolled compared with recent studies. However, the current study is valuable because it included multiple centers and used combined BI-RADS assessment. Second, not all patients in the probably benign group underwent histologic confirmation. However, no malignancy was detected during the follow-up period, and this limitation is similar to other recent studies.
In conclusion, the initial diagnostic work-up for incidental hypermetabolic lesions in the breast on PET-CT should include both mammography and sonography because combined BI-RADS assessment can differentiate malignancy and benignity. Probably benign lesions according to combined BI-RADS assessment can be followed-up without use of unnecessary biopsies.
Footnotes
Funding
This work was supported in part by the Soonchunhyang University Research Fund.