
Abstract
Background
High resolution ultrasonography features have also been described as having a useful supporting role in the diagnosis of subacute granulomatous thyroiditis (ST), and images are generally characterized by heterogeneous hypoechoic areas of the affected tissue with lack of flow on color Doppler US.
Purpose
To determine the sonographic features of subacute granulomatous thyroiditis.
Material and Methods
We reviewed the medical records of patients referred at the Endocrine and Metabolic Unit of our Institution between January 2010 and December 2011.
Results
A total of 7520 patients were evaluated in our department between January 2010 and December 2011. Among them, 22 (0.3%) patients had a diagnosis of ST (19 women and 3 men, 45.4 ± 9.7 year; range, 33–62 years). Ultrasound examination showed bilateral ST in 64% of patients. Thyroid volume was 13.2 ± 7.7 mL, without difference if ST was unilateral (13.2 ± 7.1 mL) or bilateral (13.9 ± 8.3 mL). On grayscale US, heterogeneous diffusely or focally marked hypoechoic areas, like “lava flow”, were found in all the lesions.
Conclusion
Our data confirm the high sensitivity of US in the diagnosis of ST: diffuse hypoechoic and confluent areas with the characteristic features like “lava flow”.
Introduction
Subacute granulomatous thyroiditis (ST) is one of the inflammatory thyroid disease, known as de Quervain’s disease, characterized by a clinical course of cervical pain with symptoms of hyperthyroidism and laboratory data indicating suppressed thyreotropin (TSH) levels, elevated thyroid hormone profile (fT4 and fT3) and elevated C-reactive protein (CRP) (1).
A painful thyroid following an upper respiratory tract infection is often the sign of de Querven’s thyroiditis. Subacute granulomatous thyroiditis is diagnosed clinically even if imaging studies could be helpful (2).
Until the development of ultrasound technology, scintigraphy was the only diagnostic imaging technique supporting the diagnosis of thyroid disease; this procedure is still considered a fundamental step in the management of hyperthyroid patients alone or in association with echography (3,4).
After ultrasound (US) introduction into clinical practice in the late 1960s, thyroid ultrasonography proved to be very effective in the diagnostic approach to thyroid disorders (5–7). In a previous study we showed no difference in the diagnosis of Grave’s disease between ultrasound and scintigraphy, with a slight increase in direct costs adopting this last procedure (8).
This retrospective study was addressed principally to determine the sonographic features of subacute granulomatous thyroiditis; the secondary endpoint was to evaluate the cost-effectiveness of ultrasound versus scintigraphy in the diagnosis of subacute granulomatous thyroiditis.
Material and Methods
We reviewed the medical records of patients referred to the Endocrine and Metabolic Unit of our Institution from January 2010 to December 2011. Searching criteria were the diagnosis of subacute granulomatous thyroiditis and imaging studies (ultrasound and scintigraphy) performed in all the patients. In order to delete inter-observer variability we selected only patients submitted to thyroid US by the same skilled (CC) sonographer.
Ultrasound investigation was performed using an ultrasonographic scanner (LOGIQ 9, GE, Healthcare, Milwaukee, WI, USA) equipped with a 10–14-MHz linear transducer for morphological study and 4.7 MHz for color Doppler evaluation. Scintigraphy (technetium-99 m pertechnetate) was always performed after ultrasound evaluation using a gammacamera equipped with a low-energy high-resolution collimator; the results were classified as compatible with ST (low uptake <3%) or not compatible (normal or high uptake). Diagnosis of ST was made in patients with biochemical and clinical thyrotoxicosis, with at least one of the two instrumental methods suggestive of ST and elevated erythrocyte sedimentation rate or C-reactive protein level.
Serum free thyroxine (fT4) was determined by a commercially available radioimmunoassay (fT4 RIA CT-RADIM, Rome, Italy; range, 8.0–18.0 pg/mL); serum thyroid stimulating hormone (TSH) was measured by a sensitive immunoradiometric assay (TSH IRMA Co Tube second generation; range, 0.2–4.0 mUI/L; BIORAD, Hercules, CA, USA).
Results
A total of 7520 patients were evaluated for thyroid disease in our department between January 2010 and December 2011. Among them, 22 (0.3%) subjects clearly satisfied the previous criterion for subacute granulomatous thyroiditis (19 women, 3 men; 45.4 ± 9.7 years; range, 33–62 years). All patients presented mild to severe anterior cervical pain swelling and fever. Laboratory findings showed elevated CRP (54.4 ± 12.2 mg/L, nv <5 mg/L), elevated serum fT4 (24.6 ± 3.9 pg/mL) and decreased serum TSH (0.1 ± 0.2 mUI/L).
Scintigraphy showed suppressed radioactive technetium-99 m pertechnetate uptake in all patients.
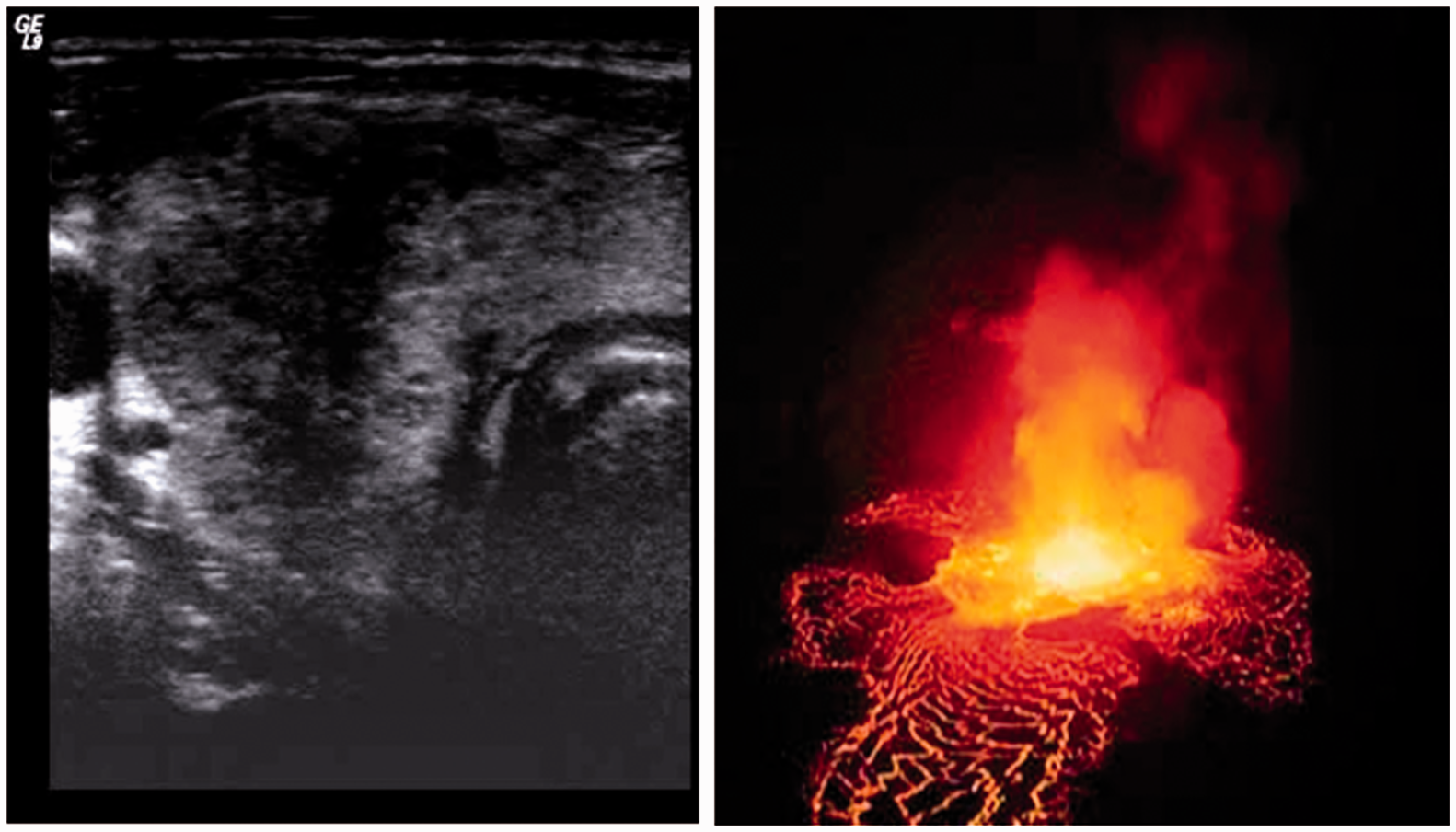
Ultrasound examination showed a prevalence of bilateral ST in 64% of patients. Thyroid volume was 13.2 ± 7.7 mL, without significant difference between unilateral or bilateral involvement (13.2 ± 7.1 mL vs. 13.9 ± 8.3 mL, respectively). On grayscale US, heterogeneous diffusely or focally marked hypoechoic areas, like “lava flow”, were found in all the lesions (Figs. 1–3). No hypervascularity was noted in any of the lesions on color Doppler evaluation.
A 47-year-old woman with diffuse neck swelling. The transverse left thyroid sonogram shows diffuse marked hypoechoic areas with the characteristic feature like “lava flow”. A 50-year-old man with diffuse neck swelling. The transverse right thyroid sonogram shows diffuse marked hypoechoic areas with the characteristic feature like “lava flow”. A 52-year-old woman with diffuse neck swelling. The longitudinal right thyroid sonogram shows diffuse marked hypoechoic areas with the characteristic feature like “lava flow”.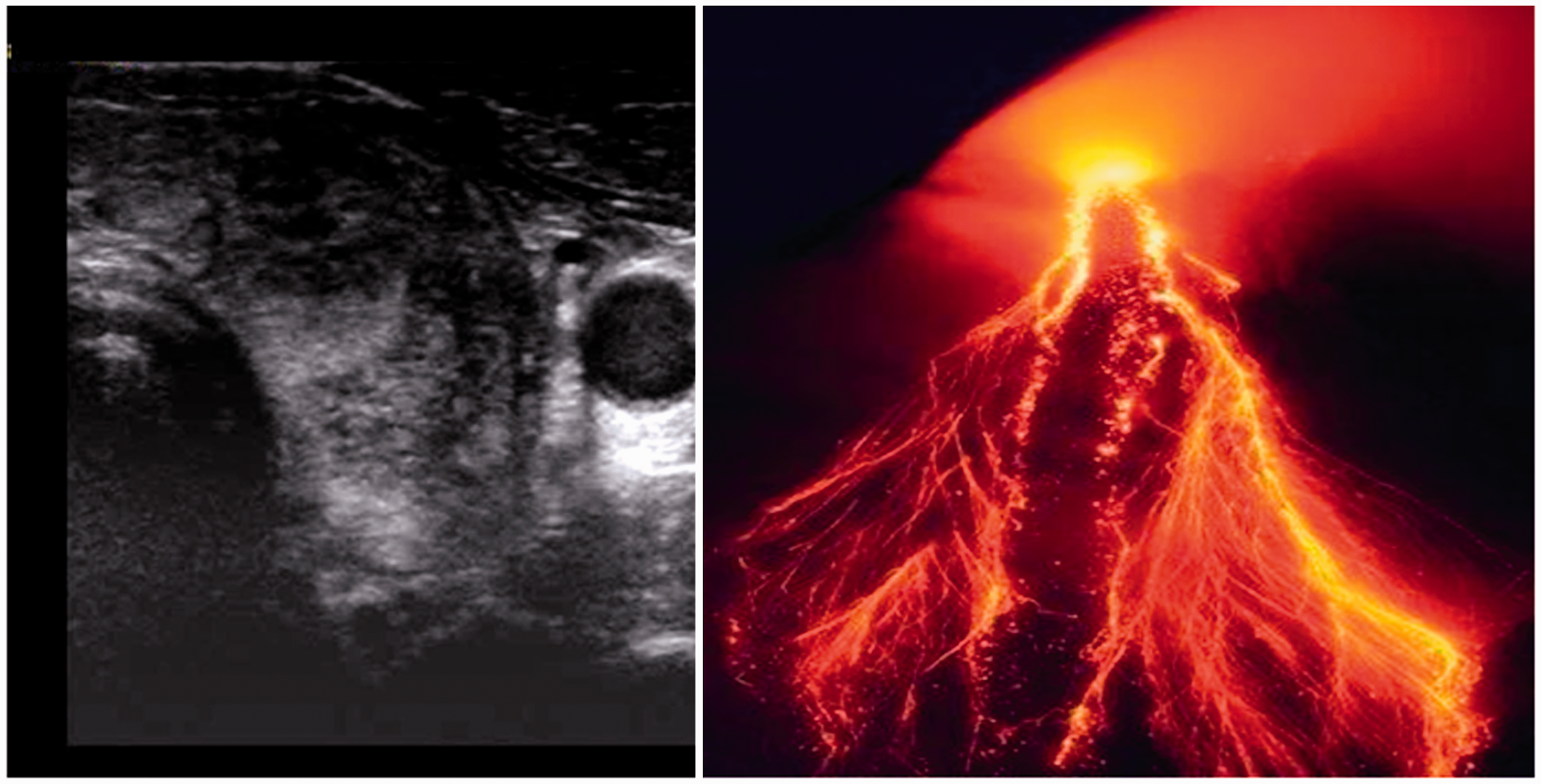

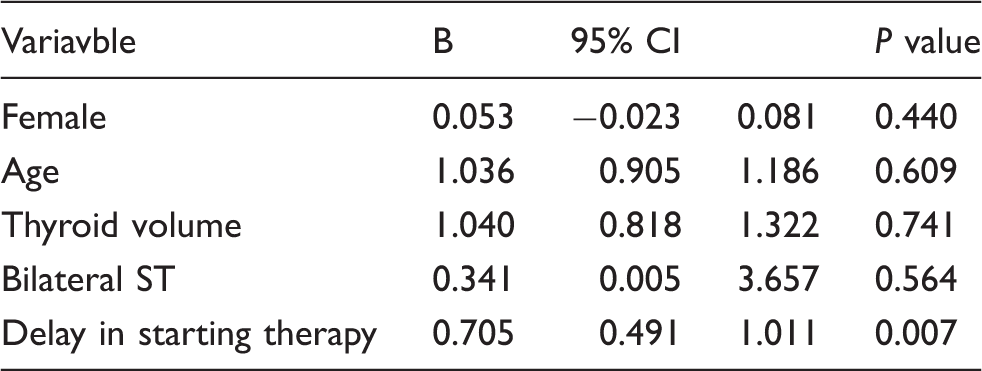
All the patients were treated with prednisone 25 mg daily as initial dose and tapered it by 5 mg every 2 weeks. At 1 year of follow-up, five (22.7%) patients developed permanent hypothyroidism, that required substitutive therapy with levothyroxine; these patients had been diagnosed and treated with a significant delay from the onset of symptoms compared to patients who developed euthyroidism (26 ± 6.5 days vs. 18.3 ± 4.1 days, P = 0.004) (Fig. 4). Multiple regression analysis with euthyroidism restoration at follow-up as dependent variable showed that the delay of starting prednisone treatment was related to hypothyrodism occurrence. Age, gender, thyroid volume, and bilateral subacute thyroiditis were non-significant variables in this model (Table 1).
TSH value at 1 year of follow-up for patient related to the delay in starting corticosteroids therapy (euthyroid [white circles] and hypothyroid [black circles] patients at 1 year of follow-up). Logistic regression analysis of hypothyroidism development predictors in the study population. The delay in starting prednisone treatment resulted in the only significant predictor for the developing of hypothyroidism. Gender, age, thyroid volume, or bilateral subacute thyroiditis did not influence the development of dysthyroidism.
Discussion
Subacute granulomatous thyroiditis is a self-limiting thyroid disorder that presents with localized anterior neck pain and often low-grade fever with thyrotoxicosis at least at the beginning of disease (2). The Rochester Epidemiology Project reported an incidence rate of 12.1 cases per 100,000/year, higher in women than in men (19.1 and 4.1 per 100,000/year, respectively) (9,10). Although the cause is most likely a viral infection, ST occurs most commonly (in 80% of cases) in women who are aged 40–50 years (11). The higher incidence in women in the present study (86%) is similar to the findings of previous reports (9–11).
The diagnosis of subacute granulomatous thyroiditis is clinical, but imaging studies may be helpful (2). In hyperthyroid patients, in spite of the wide spread availability of ultrasound, scintigraphy remains the first instrumental procedure in many guidelines (4,12,13). Indeed, a growing number of articles suggests that ultrasound with echo Doppler evaluation could be a good alternative to radiometabolic scan (14–16), as we reported in a previous study in patients affected by Grave’s disease (8).
High resolution ultrasonography features have been also described as useful in supporting the diagnosis of ST: images are generally characterized by heterogeneous hypoechoic areas of affected tissue with lack of flow on color Doppler US (2,17–19).
Our data confirm the high sensitivity of US in the diagnosis of ST, but moreover, underline the specificity of this procedure. In fact all the patients in our study with ST showed diffuse hypoechoic areas in the thyroid gland on ultrasound, resembling “lava flow” (Figs. 1–3). “Lava flow” feature seems to be exclusive of subacute thyroiditis as well as it was not found among the 7520 patients submitted to US not affected by ST.
Our data clearly show that both imaging procedures (scintigraphy and/or ultrasound) are superimposable in term of sensitivity (100%); unfortunately, we have not the data about specificity of scintigraphy in detecting ST, as we do not routinely perform this procedure in all thyreopatic patients. However, if we admit that scintigraphy and ultrasound are equal also in term of specificity, we must underline that ultrasound is less expensive (€31.25 for exam) than scintigraphy (€45.96 for exam). These data suggest that ultrasound evaluation could be a good alternative to radio metabolic scan not only in patients affected by Grave’s disease as previously reported (8), but also in those affected by subacute thyroiditis.
Few reports showed permanent hypothyroidism as a complication of subacute thyroiditis (9,20). During the shorter follow-up of the Olmested County study, only 4% of patients required L-T4 therapy (20). In the present report, with longer follow-up, the incidence of hypothyroidism was higher (22.7%) but in accordance with Fatourechi et al. (9). The authors evidenced a significant higher number of patients who developed hypothyroidism among those treated with corticosteroids than among the not treated ones (25% vs. 10%, respectively), concluding that patients with more severe disease may be more likely to be treated with corticosteroids and thus be more likely to develop hypothyroidism (9). On the contrary, all of our patients were treated with corticosteroids. Multiple regression analysis well evidenced that it was only the delay in starting prednisone treatment to be related to hypothyrodism. In other words, if we want to prevent the developing of hypothyroidism we must treat with corticosteroids patients affected by ST as soon as possible.
Our study has some limitations. The first limitation is the relatively small simple size of patients affected by subacute granulomatous thyroiditis owing to the rarity of this condition. The second limitation is represented by the retrospective nature of the study. Finally, our data do not permit to try any conclusions about specificity of scintigraphy in detecting ST, as we not routinely performed this procedure in all thyreopatic patients.
In conclusion, we suggest that the “heterogeneous” ultrasound features of subacute thyroidithys are specifically identified as “lava flow” images. If images studies are required ultrasound is mandatory for its specificity and sensitivity and more over as less expensive than scintigraphy. To prevent hypothyroidism we suggest to treat patients as soon as possible. Prospective studies are needed to confirm our observation.
Footnotes
Acknowledgements
The authors thank Mr Antonio Guarrera and Mr John Lockwood for their images of volcano lava flows.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.