
Abstract
Background
Magnetic resonance imaging (MRI) BI-RADS® 3 lesions should have a very high probability of being benign. To prove benignity most institutions do follow-up MRI.
Purpose
To evaluate the necessity of initial short-interval follow-up after 6 months as it is suggested for mammographic BI-RADS®3 lesions.
Material and Methods
We analyzed 163 consecutive MRI-BI-RADS® 3 lesions on follow-up MRI: 75 masses (46%), 67 foci (41.1%), and 21 (12.9%) non-mass-like enhancing lesions (NMLE).
Results
During MRI follow-up (mean time, 563 days) 20% of the lesions disappeared, 23% decreased, 52% did not change, and 4.9% showed increase. All increasing lesions were biopsied (5 benign, 2 ductal carcinoma in situ, 1 invasive carcinoma). The rate of malignancy was 1.8%. All malignant lesions (1 mass, 1 focus, 1 NMLE) showed increase at initial follow-up after a mean interval of 190 days.
Conclusion
In this study the malignancy rate of MRI-BI-RADS® 3 lesions corresponded to mammographic BI-RADS® 3 lesions. Initial short-interval MRI should be suggested to identify malignant MRI-BI-RADS® 3 lesions.
Keywords
Introduction
The current Breast Imaging and Reporting Data System (BI-RADS®) of the American College of Radiology helps to describe and categorize breast findings on mammography, on ultrasound, and on magnetic resonance imaging (MRI) (1). Mammographic lesions which are assessed as BI-RADS® 3 are probably benign and should have a <2% risk of malignancy. In these cases initial short-interval follow-up after 6 months, followed by additional examinations is recommended to prove longer-term (2 years or longer) lesion stability. There are many studies which confirm a malignancy rate <2% of mammographic BI-RADS® 3 findings (2–5).
MRI detected BI-RADS® 3 lesions should also have a very high probability of being benign (1). In contrast to mammographic lesions there is no malignancy rate defined for these findings. Short-interval follow-up examinations are probably useful, but a specific recommendation is missing (“most approaches are intuitive”). Up to now only a few studies on MRI BI-RADS® 3 lesions are published. They show a wide range of malignancy rates from 0.7% to 10%, a high variability of lesion types and enhancement characteristics and different follow-up intervals (6–9).
The purpose of this study was to evaluate the rate of malignancy and the time from first MRI to the diagnosis of malignancy for MRI BI-RADS® 3 lesions to determine if initial short-term follow-up is necessary. Furthermore we wanted to analyze the lesion types and contrast enhancement curves of MRI BI-RADS® 3 lesions to assess if lesions characteristics are helpful to predict malignancy.
Material and Methods
Patients and lesions
A retrospective data analysis based on digital patient reports from the radiology information system (RIS) of our Hospital was performed (SDB). All breast MRI examinations which had been performed at our breast center during a 12-month period (n = 666) were evaluated. The inclusion criteria were diagnosis of BI-RADS® 3 on breast MRI and at least one available follow-up MRI at our institution. In 182 cases (27.3%) at least one BI-RADS® 3 finding was found. Sixty-four percent (n = 117) of these patients with 163 BI-RADS® 3 lesions returned for the recommended follow-up breast MRI to our institution. These patients met the inclusion criteria and built the study cohort. As we routinely do, written informed consent regarding the MRI examination as well as the anonymous data evaluation was given by each patient before dynamic contrast-enhanced breast MRI was performed. All women underwent a bilateral two-view mammography and bilateral breast ultrasound examination before breast MRI.
The indications for breast MRI were in 37 cases (31.6%) preoperative local staging of known breast cancer, in 31 cases (26.5%) equivocal findings on mammography and ultrasound, in 12 cases (10.3%) unclear clinical findings without abnormality on mammography and ultrasound (e.g. a palpable lesion), in 21 cases (17.9%) the exclusion of a tumor recurrence after breast-conserving therapy, in six cases (5.1%) high-risk screening for breast cancer, and in 10 cases (8.6%) other indications.
In all patients a follow-up breast MRI after 6 months was recommended. If the BI-RADS® 3 lesion remained at this time stable further follow-up breast MRI examinations were recommended. If the lesion eventually demonstrated stability over a period of at least 18 months no further follow-up was recommended. If a BI-RADS® 3 lesion increased in size or developed more suspicious enhancement kinetics biopsy and histological analysis were performed. The histological reports were taken from the digital pathology system of our hospital.
The study has been approved by the institutional ethics committee (No. 446/2012R).
MRI
Breast MRI was performed at 1.5 Tesla (Achieva, Philips, Best, The Netherlands) with a multi-array double breast coil. After a transverse T2-weighted short-tau inversion recovery sequence (TR, 2933 ms; TE, 50 ms; TI, 160 ms; matrix, 432 × 295; field of view [FOV], 390/390 mm; slice thickness, 3.5 mm), a dynamic contrast-enhanced breast imaging was performed by means of a high-resolution T1-weighted gradient echo sequence (fast field echo [FFE]) in transverse orientation (TR, 8.2 ms; TE, 4.1 ms; flip angle, 20°; matrix 488 × 468; FOV, 420/420 mm; slice thickness, 1.5 mm) with automated intravenous bolus application of 0.16 mmol gadolinium-chelate (Magnevist® 0.5 mmol/mL or Gadovist® 1.0 mmol/mL, Bayer Health Care, Berlin, Germany) per kg body weight. One non-enhanced and seven enhanced series were acquired with an acquisition time of 75 s each. Subtraction images were generated for each contrast-enhanced series by subtraction of the non-enhanced series from the enhanced series. For image analysis a dedicated workstation (ViewForum, Philips, Best, The Netherlands) was used. Enhancement kinetics was evaluated by region-of-interest (ROI) analysis.
Data analysis
All data were entered into a Microsoft Excel spreadsheet and then imported into SAS statistical software JMP 8 for analysis.
For comparing two two-level categorical variables, Pearson T-test was used to test the difference. A P value <0.05 was considered significant.
All lesions which were not further present on follow-up MRI and those which were stable for a minimum period of 1.5 years, and those which were histological benign were defined as benign. All lesions with malignant histology were defined as malignant. The malignancy rate of BI-RADS® 3 lesions was calculated by dividing the number of malignant lesions by all BI-RADS® 3 lesions in which follow-up MRI was available.
The initial and every follow-up breast MRI were evaluated in consensus by two radiologists with 3 years (SDB) and 8 years (KCS-L) experience of breast MRI. The lesion size was measured as the maximum diameter in mm on early subtraction images within 3 min after contrast medium injection. According to BI-RADS® the lesion type (mass, focus, non-mass-like enhancement) and the delayed enhancement kinetics (persistent, plateau, wash-out) of the analyzed BI-RADS® 3 findings were categorized. On follow-up breast MRI the study lesions were assessed as not more present, decreased (in size), stable, or increased (extended size or more suspicious delayed enhancement kinetics).
Results
Patients and lesions
Out of 117 patients (mean age, 51 years; minimum, 33 years; maximum, 76 years) with 163 BI-RADS® 3 lesions, 71 (60.7%) had one unilateral BI-RADS® 3 lesion and 46 patients (39.3%) showed bilateral BI-RADS® 3 lesions, one in each breast.
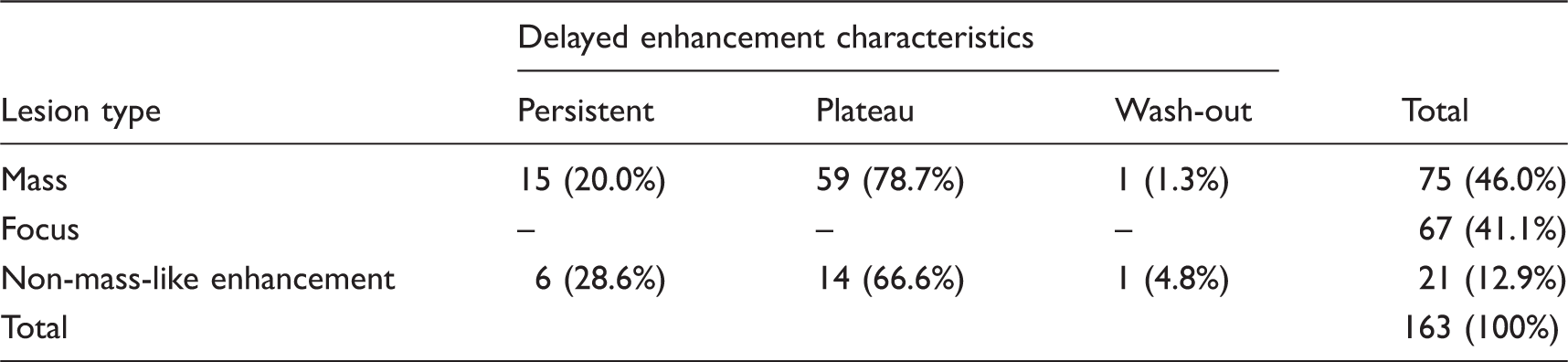
The 163 BI-RADS® 3 lesions were in 46% (n = 75) masses, in 41.1% (n = 67) foci as well as in 12.9% (n = 21) non-mass-like enhancing (NMLE) findings. According to the current BI-RADS® the enhancement kinetics of the foci which are defined as tiny spots <5 mm in diameter were not assessed.
The mean diameter of all lesions was 8 mm (minimum, 2 mm; maximum, 85 mm). The maximum diameter of the 75 masses was on average 7 mm (minimum, 5 mm; maximum, 18 mm). The mean diameter of the 21 NMLE findings was 28 mm (minimum, 9 mm; maximum, 85 mm).
Lesion types and delayed enhancement characteristics of MRI-BI-RADS® 3 lesions (n = 163).
MR follow-up
In most of the BI-RADS® 3 lesions (n = 99, 60.7%) one follow-up breast MRI was performed. In 24.5% (n = 40) of the lesions two follow-up breast MRI examinations, in 8% (n = 13) three follow-up breast MRI examinations, in 5% (n = 8) four follow-up breast MRI examinations, and in 1.8% (n = 3) five follow breast MRI examinations were carried out. This results in a median number of 1.6 follow-up breast MRI examinations per lesion. The mean time of the entire follow-up period was 563 days (range, 34–1566 days; median, 392 days). The first follow-up was performed in the average 314 days after the initial breast MRI (range, 34–1351; median, 226 days).
In 33 cases (20.3%) the former BI-RADS® 3 lesion was not more present on follow-up MRI and in 37 cases (22.7%) the study lesions were assessed as BI-RADS® 2 because of their decrease.
Eighty-five BI-RADS® 3 lesions (52.1%) remained stable. Sixty-two of these stable lesions were classified as benign because of a follow-up time of at least 18 months. The other 23 stable lesions had a follow-up time <18 months because of a certainly benign morphology and an unchanged diameter (e.g. a lymph node, n = 16) or a correlation as benign by an ultrasound after a first follow-up (n = 7).
Eight lesions (4.9%) increased at follow-up and were therefore assessed as BI-RADS® 4 (Fig. 1). In these cases biopsy was performed.
Results of the follow-up breast MRI of 163 BI-RADS® 3 lesions.
The malignancy rate of BI-RADS® 3 lesions
All increased lesions (n = 8) were diagnosed on the first follow-up MRI after a mean time of 236 days. After biopsy histology demonstrated five benign findings (1 fibroadenoma, 2 adenosis, 2 liponecrosis) and three malignant lesions. Two of the malignant findings were ductal carcinoma in situ (1 focus, 1 NMLE). The third malignant lesion was an invasive ductal carcinoma which presented as a mass.
Overall, the malignancy rate of the analyzed MRI-BI-RADS®3 lesions was 1.8% (3/163).
Malignant lesions (n = 3)
A ductal carcinoma in situ (DCIS) was diagnosed in a 43-year-old patient. The indication for breast MRI was high familiar risk of breast cancer. The BI-RADS® 3 lesion was regional NMLE of 32 mm diameter with plateau kinetic curve. On follow-up breast MRI after 132 days the lesion showed no significant change in size but a more suspicious delayed enhancement (wash-out). There was no corresponding finding on mammography and second-look ultrasound. Therefore, an MRI-guided vacuum-assisted breast biopsy was performed.
Breast MRI was performed to exclude tumour recurrence after breast conserving therapy in a 62-year-old patient with history of breast cancer (DCIS) 2 years ago. MRI showed multiple foci. Follow-up breast MRI was performed after 177 days and showed an increase in size of one focus from 4 mm to 7 mm. ROI analysis resulted in persistent enhancement. Mammography and second-look ultrasound were inconspicuous, thus MRI-guided vacuum-assisted breast biopsy was performed. The histological diagnosis was DCIS.
A 56-year-old patient presented with a mass lesion, which showed plateau enhancement. Indication for breast MRI was an unclear palpable finding and low diagnostic certainty of ultrasound and mammography due to strong fibrocystic changes and very dense breasts. Follow-up MRI was carried out after 261 days. It showed a more suspicious lesion enhancement (wash-out) and an increased lesion size from 7 mm to 9 mm. The lesion could be identified by second-look ultrasound and an ultrasound-guided biopsy was performed. It revealed an invasive ductal carcinoma (Fig. 2).
From left to right: non-enhanced, enhanced, and subtraction image of the dynamic T1-weighted gradient echo sequence. In the upper row the initial breast MRI examination is displayed, in the lower row the follow-up breast MRI after almost 9 months is pictured. On initial MRI a 7 mm large mass lesion with low initial enhancement and plateau curve in the delayed phase (not displayed) is demonstrated (a–c). The lesion was assessed as probably benign, BI-RADS®3. Follow-up MRI showed an increased lesion size (from 7 mm to 9 mm) and a newly diagnosed wash-out kinetic curve (not displayed). The lesion was assessed as suspicious, BI-RADS® 4 (d–f). After identification on second-look ultrasound and ultrasound-guided large core needle biopsy an invasive ductal carcinoma was diagnosed.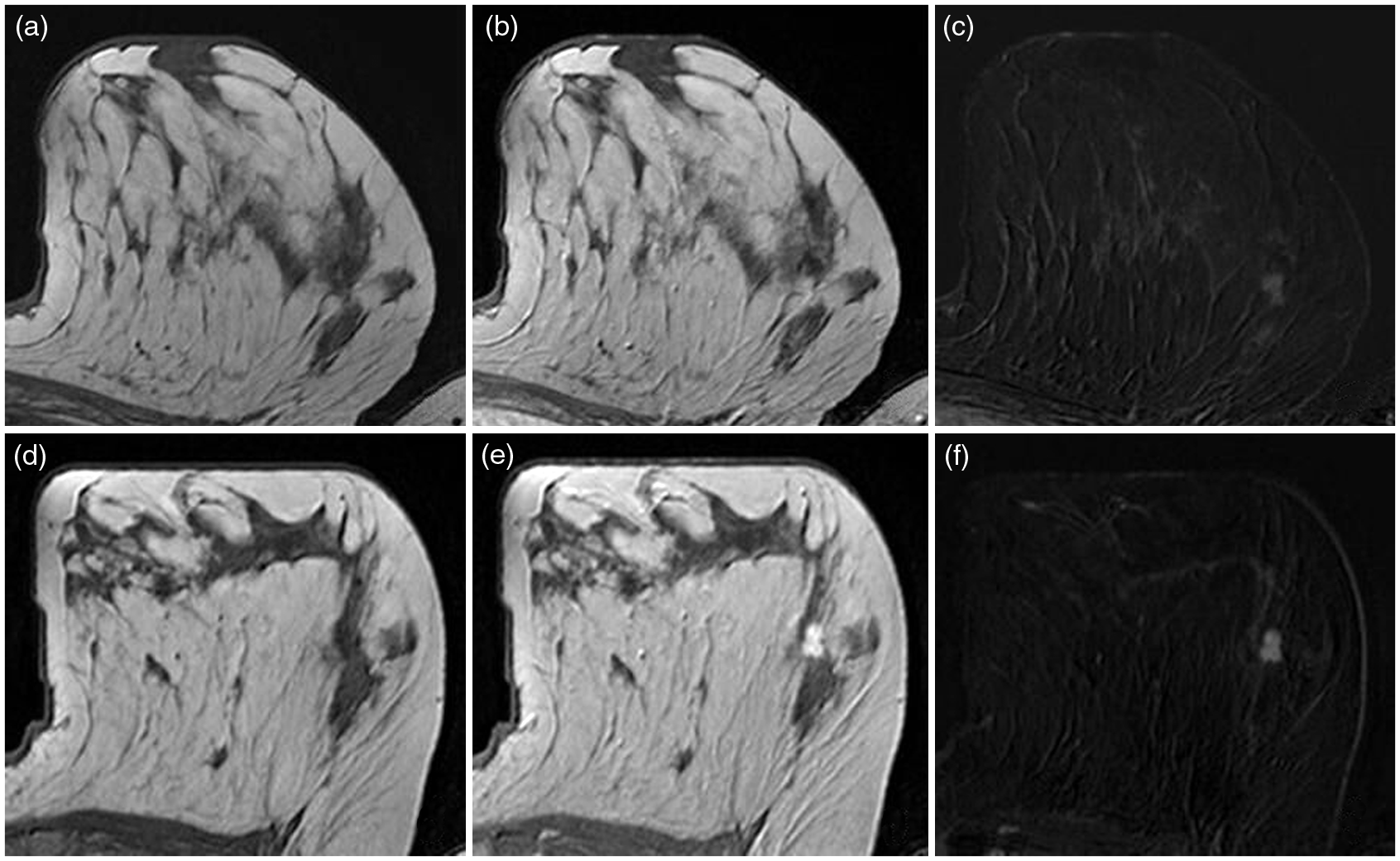
Therefore no correlation was found between the dignity of the lesions and their diameter, kinetic, or type (P > 0.05).
Discussion
In our study 27.3% (182/666) of all breast MRI examinations which were performed during a 12-month period resulted in the diagnosis of at least one BI-RADS® 3 finding. Liberman et al. (6) and Eby et al. (10) report from a comparable number of BI-RADS® 3 lesions (24% and 20%, respectively). However, other authors report from a lower rate of MRI-BI-RADS® 3 lesions (range, 6.3–10.9%) (7,8,11,12). Different patient populations are most likely responsible for these differences. Basically, the number of BI-RADS® 3 lesions is very high, especially against the background of the costs of a short-term follow-up MRI relative to mammography. So the aim should be – into account of a clear definition – to keep the number as low as possible.
On follow-up 1.8% of our BI-RADS® 3 lesions (n = 163) showed malignancy. Most of the published studies on this subject report from similar malignancy rates of MRI-BI-RADS® 3 lesions. Eby et al. (10) analyzed breast MRI studies of 149 BI-RADS® 3 lesions. Within a 1.5-year follow-up period they could demonstrate a malignancy rate of 0.6%. In another study of this author (7) 236 patients with MRI-BI-RADS® 3 lesions showed a malignancy rate of 0.85%. Weinstein et al. (8) report from a malignancy rate of 0.9% in 106 patients with MRI BI-RADS® 3 lesions. Liberman et al. (6) analyzed a population of high-risk patients and as a result they found a much higher malignancy rate of MRI BI-RADS® 3 lesions (10%). However, in a study of Sandowski and Kelcz (13) 5.1% of lesions that were classified as probably benign on contrast-enhanced MRI were finally malignant. This opposed result is possibly caused by different patient selection criteria. In the cited study the main indication for breast MRI were mammographic findings classified as BI-RADS® 0. Furthermore, less expertise in reading breast MRI studies could have potentially influenced the classification of malignant lesions as BI-RADS® 3. The authors investigated a cohort of all (n = 473) breast MRI examinations which were performed at their institution within 8 years. This means breast MRI was not frequently performed (roughly once per week).
In our study most patients had an elevated breast cancer risk. They presented either with recently or in the past diagnosed breast cancer (n = 58), or with a high familiar risk of breast cancer (n = 6), or with unclear findings on clinical breast examination or on mammography and ultrasound (n = 43). The initially as BI-RADS® 3 assessed malignant lesions in our study (n = 3) occurred in one patient with a high familiar risk of breast cancer and in one patient with history of breast cancer 2 years ago, and at last in one patient with an unclear finding on clinical breast examination. Therefore even if BI-RADS® is an image-related classification, clinical findings and individual patient risk should influence the patient management. For example because of the higher rate of malignancy in case of high-risk patients it should be decided in each particular case if a biopsy or a follow-up should be performed.
The entire follow-up period of our study was mean 563.5 days, Thereby the first follow-up was performed after a mean time of 314 days. Therewith, the entire follow-up period of our study is longer than the reported follow-up intervals of other authors (240–330 days) (6,7,11). However, all studies show a wide range of follow-up intervals. To prove lesion stability with sufficient certainty a follow-up period of at least 18 to 24 months should be aimed at.
All increasing lesions of our study were diagnosed on short-interval follow-up MRI after a mean time of 236 days. Thereafter no lesion showed increased size or developed more suspicious enhancement kinetics. All malignant lesions (n = 3) were diagnosed after a mean follow-up period of 190 days or 6 months, respectively. Information on this subject in the literature is often missing. Liberman et al. (6) report from a median interval from the initial examination to biopsy of 7 months (range, 3–18 months). Therefore it seems to be advisable to perform the initial follow-up breast MRI of BI-RADS® 3 lesions after a short-term interval of approximately 6 months. This corresponds to the recommended management of mammographic BI-RADS® 3 lesions. The usefulness of further follow-up MRI examinations in case of short-term stable BI-RADS® 3 lesions could not been proven by our data. Further studies are probably necessary to shed light on this issue.
The BI-RADS® 3 lesions of our study which presented as NMLE had a larger diameter (mean, 28 mm) as compared with the masses (mean, 7 mm). However the diameter of MRI BI-RADS®3 lesions was not related to the rate of malignancy. The three malignant lesions had a diameter of 4 mm, 7 mm, and 32 mm, respectively. As far as we know, there is no study which describes the relation of size with malignancy in case of MRI-BI-RADS® 3 lesions.
All three carcinomas of our study showed different lesion types on breast MRI (1 mass, 1 focus, 1 NMLE). Therefore we cannot see any relation between lesion type and malignancy in BI-RADS® 3 lesions. Similar results are found in the literature (7,8), for example Eby et al. (7) described the two diagnosed malignant lesions in their study population of probably benign lesions as one heterogonous NMLE and one 5 mm focus.
The vast majority of lesions in our study demonstrated plateau enhancement kinetics on first MRI, which correlates to the results of Liberman (6). Other studies showed more BI-RADS® 3 lesions with a persistent enhancement (7,8). In all studies lesions with wash-out kinetics were rarely assessed as BI-RADS® 3. Two of our diagnosed carcinomas showed also plateau enhancement on baseline breast MRI but changed to wash-out kinetics on follow-up MRI. The third carcinoma was initially a focus (no assessment of enhancement kinetics) and showed a persistent enhancement on follow-up MRI.
There are limitations of this study; the first is its retrospective design. However, all breast MRI studies were newly assessed by consensus reading, but the diagnosis of BI-RADS® 3 on first MRI did not change in any case. A second limitation of our study is the small study size and relatively low patient compliance to follow-up MRI. Only 64% (n = 117) of the patients with MRI-BI-RADS® 3 lesions returned to the recommended follow-up and could be analyzed. Therefore, a selection bias cannot be excluded. However, the patient compliance rate is comparable to the results of other authors. For instance in two studies of Eby et al. the recommended MRI follow-up of BI-RADS® 3 lesions could be performed in 62% and 63% of the cases, respectively (7,10). In the study of Liberman et al. (6) the patient compliance to follow-up breast MRI was 79%. This is possibly caused by patient selection. In their study only high-risk women who usually come regularly for breast MRI were analyzed. Altogether, we suppose that these limitations do not fundamentally affect the study results.
In conclusion, MRI BI-RADS® 3 occur in approximately one-fourth of all breast MRI examinations. The malignancy rate of those lesions is <2% and herewith comparable to the malignancy rate of mammographic BI-RADS® 3 lesions. All carcinomas of our patient cohort were diagnosed on short-interval breast MRI follow-up within 6 months. Hence, an initial short-interval follow-up according to mammographic BI-RADS® 3 lesions seems to be advisable. Neither the lesion type (mass, focus, NMLE) nor the enhancements kinetics helps to predict malignancy in these lesions. However, if a BI-RADS® 3 lesion increases in size or if it develops a more suspicious enhancement kinetics biopsy should be recommended.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.