
Abstract
Background
Computed tomography pulmonary angiography (CTPA) is used most often in routine clinical practice for the assessment of a suspected pulmonary embolism. The diagnostic accuracy relies on sufficient contrast enhancement.
Material and Methods
A total of 2786 CT pulmonary angiographies, acquired on a 64-row CT during deep-inspiration breath-hold, were reviewed. Twenty-four examinations were considered non-diagnostic due to poor contrast enhancement in the pulmonary arteries (PA), although they showed preserved vascular enhancement of the superior vena cava (SVC) and the ascending aorta (AO). Eleven flawed CTPA examinations, including severe breathing artifacts and incorrect triggering were excluded. In 13 of the remaining patients, the examination was repeated during shallow breathing. Vascular contrast enhancement was compared between both scans by measuring the relative enhancement within the SVC, the main PA, and the AO. Image quality was scored by two, clinically experienced radiologists. The values are given as median and [25th;75th] quartile.
Results
There was a significant difference in the CT values for the PA between the repeated scans (P = 0.0002, Wilcoxon test), and with the CTPA in deep-inspiration showing a median enhancement of 97 HU (59–173), compared with 303 HU (239–385) in the CTPA acquired during free breathing. The differences for both the AO (P = 0.54) and the SVC (P = 0.78) were not significant. Scoring for the attenuation quality rose significantly (P = 0.0002) and no severe motion artifacts were detected on either scans.
Conclusion
If there is insufficient pulmonary artery enhancement during CTPA, attenuation of the pulmonary arteries can be improved by acquisition during shallow breathing and is without significant loss of the overall diagnostic image quality.
Introduction
With computed tomography pulmonary angiography (CTPA), a number of technical and patient-related factors contribute to the diagnostic quality of the images obtained (1). Despite technically sound execution with correct bolus triggering, incidentally a pattern of low attenuation values in the pulmonary arteries with very high attenuation in the large veins and the aorta can be seen. It has been shown that an increased contribution to the right atrial flow input of the inferior vena cava compared to that of the superior vena cava can cause interrupted attenuation of pulmonary vessels (2). As CTPA is performed during a single breath-hold, deep inspiration before breath-hold or the Valsalva maneuver has been discussed as the most likely cause (2,3). It has been suggested that image acquisition during quiet breathing may improve the enhancement (4,5). However, it has not yet been analyzed whether there is any benefit from acquisition during quiet breathing or predominantly a reduction in diagnostic quality caused by breathing artifacts. Our study tested acquisition during quiet breathing as an alternative to breath-hold examinations in situations where low attenuation in the main pulmonary artery occurred.
Material and Methods
Study population
For this retrospective study our institutional review board waived the requirement for patient consent. We retrospectively identified 2786 CTPAs in our PACS-System, which were completed at our institution between 2006 and 2011. Twenty-four examinations had to be repeated due to poor enhancement in the pulmonary trunk. These 24 examinations had been rated as “non-diagnostic” by the attending radiologist and had been repeated immediately, including a second administration of contrast agent. From these examinations, we excluded 11 in which the second scan was performed due to technical problems during the initial image acquisition (operator-related, e.g. “too early” or “too late” start of the scan or contrast-medium extravasation). In the remaining 13 cases, as low vascular attenuation was suspected to be breath-related because of preserved enhancement in the superior vena cava and the aorta, the image acquisition was repeated during shallow breathing.
Scan protocol
Acquisition parameters.
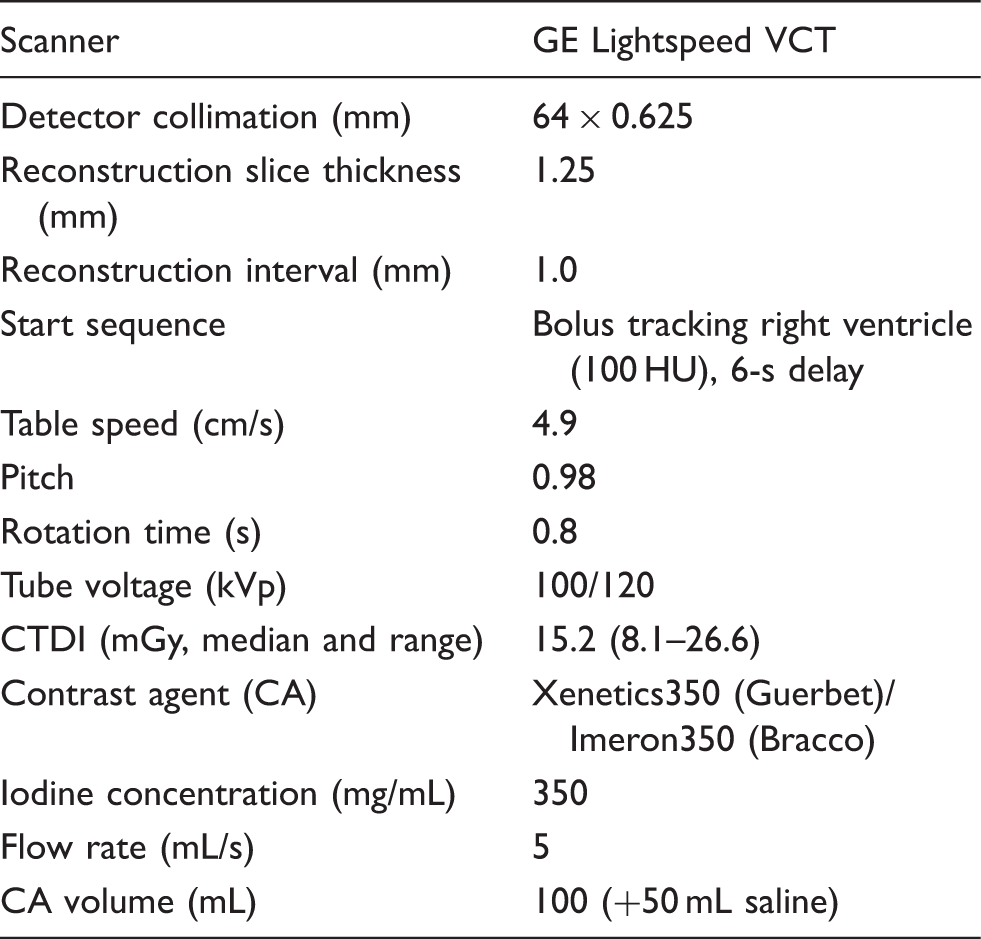
Image evaluation
The examinations were evaluated for image quality and the possible presence of a pulmonary embolus by two, blinded (for both patient data as well as the breathing maneuver) radiologists, each with more than 10 years of clinical experience (HS and CvF). Reconstruction in axial, coronal, and sagittal orientation was used.
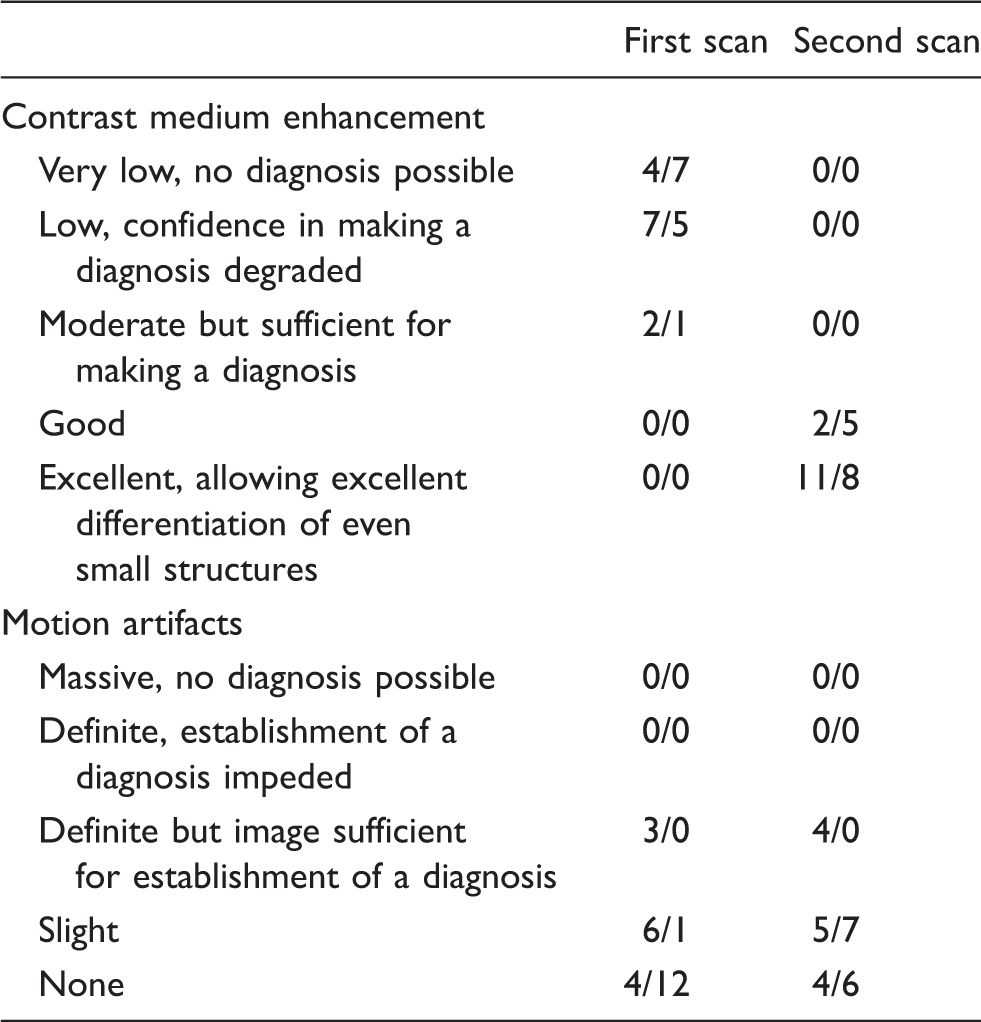
Subjective quality score (adapted from
Mean vascular attenuation was measured in Hounsfield Units (HU) using circular region of interests of at least 1 cm2. Vascular contrast enhancement of the main pulmonary artery, ascending aorta, and superior vena cava was defined as attenuation after contrast medium injection seen during the diagnostic scan, subtracted by the attenuation of the right ventricle on the first scan of the bolus tracking series.
Statistical analysis
Statistical analysis was performed using Prism 5.0 c (GraphPad Software, Inc. La Jolla, CA, USA). The non-parametric Wilcoxon test was applied. Values for P < 0.05 were considered statistically significant. Values are given as the median, 25th;75th quartile, and range.
Results
Study population
The mean patient age for all CTAs in the PACS system, and performed during the observed time frame, was 63 years [50;72 years] (range, 0–97 years). The 13 examinations that were repeated during free breathing, were performed on six female patients and seven male patients with a median age of 42 years [34.8;67.8 years] (range, 25–81 years), which was a significantly lower age than that seen in the general population (P = 0.024). Pulmonary embolism (PE) was detected in five patients on the repeated scans (Fig. 1), whereas only one major embolus in the main pulmonary arteries was detected on the first scan. One of those five patients showed a chronic embolism, two had an acute embolus in one lung segment, and two showed emboli in multiple segments of both lungs.
In this 41-year-old woman, the first CT angiography scan (a) showed non-diagnostic vessel enhancement and no embolism was found. (b) After repeating the scan during free breathing, multiple segmental embolisms were detected in the right lower lobe (circle). No differences in motion-related artifacts were detected.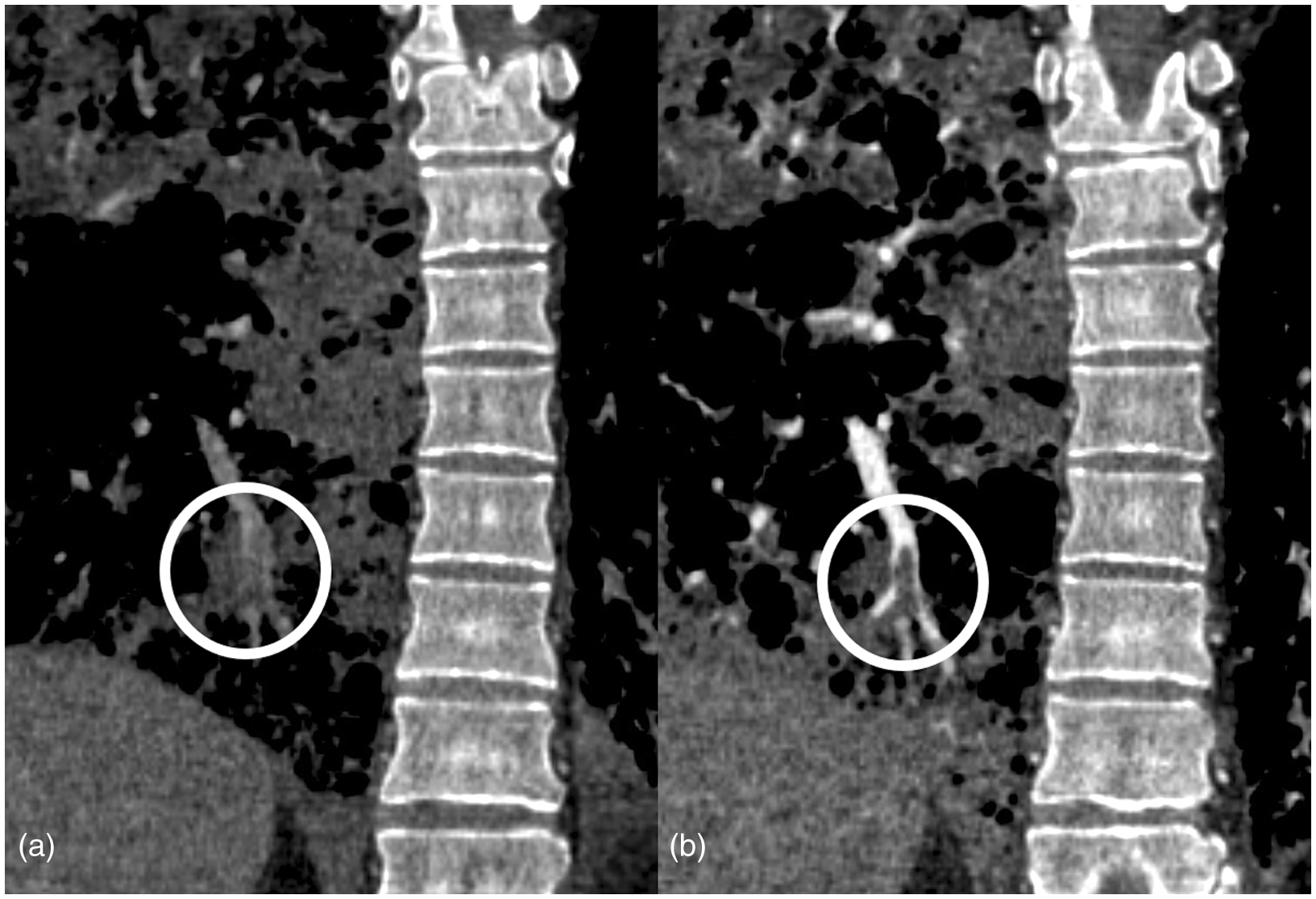
Subjective image quality
Contrast enhancement of the pulmonary vessels in the first exams was graded as “very low, no diagnosis possible” or “low, confidence in making a diagnosis degraded” by both readers. Repeated exams were rated as “good” or “excellent vascular enhancement, allowing excellent differentiation of the subsegmental arteries” by both radiologists, and thus indicating a significant increase in vessel attenuation (P = 0.0002 between the first and the repeated scan for both readers; Table 2).
According to a subjective evaluation, no examination during breath-hold or free breathing revealed motion artifacts that decreased the diagnostic quality (Table 2). In addition, no statistically significant differences were found regarding motion artifacts between the two breathing states for either of the two readers (P = 0.075 for CvF and P = 0.99 for HS).
Vascular contrast medium enhancement
Comparing the scans performed during breath-hold and during free breathing, contrast medium enhancement in the main pulmonary artery increased substantially in all patients, from 97 HU [59;173 HU] (29;179 HU) to 303 HU [239;385 HU] (173;488 HU) (P = 0.0002, Fig. 2a). The median enhancement in the ascending aorta (Fig. 2b) was 212 HU [163;273 HU] (130;478 HU) during breath-hold and 239 HU [193;263 HU] (167;337 HU) during free breathing, and thus showing no significant statistical difference (P = 0.54). Furthermore, the contrast medium enhancement in the superior vena cava during breath-hold were 481 HU [213;788 HU] (73;2260) and did not change significantly during free breathing, i.e. 644 HU [298;928 HU] (183;2479) (P = 0.78).
Attenuation (Hounsfield units [HU]) of the main pulmonary artery increased significantly during free breathing versus deep inspiratory breath-holding (a). The contrast-medium enhancement in the ascending aorta (b) and in the superior vena cava (not shown) did not differ between the scans. Wilcoxon signed-rank test (ns P = 0.54, ***P = 0.0002).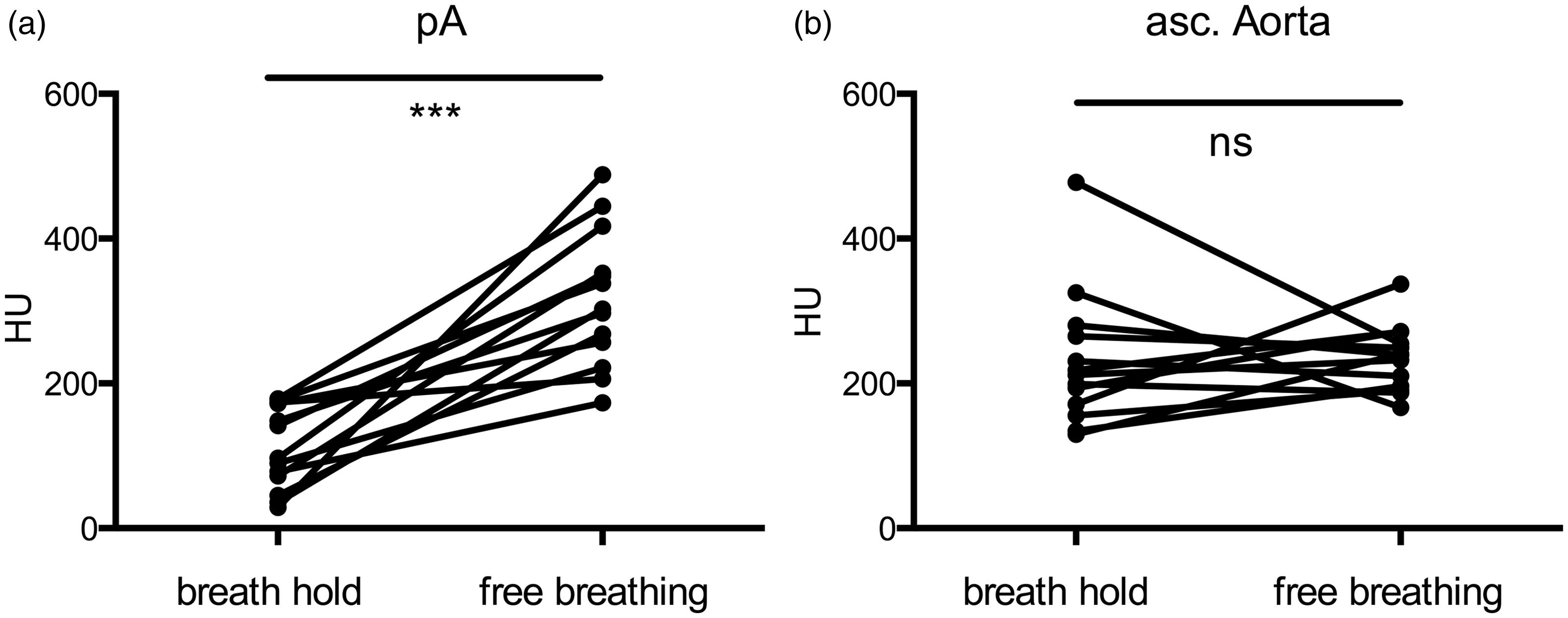
Discussion
This study showed that in patients with low contrast enhancement on breath-hold during inspiration, the pulmonary artery attenuation seen on CTPA increased significantly during free breathing, while the breathing artifacts remained negligible.
In a recent study, Kuzo et al. suggested that low enhancement in the pulmonary arteries may be due to contrast agent dilution caused by intrathoracic pressure changes occurring during breath-hold (3). Using magnetic resonance flow measurements, it was shown by Kuzo et al. that during deep inspiration the increase of the flow rate was significantly higher in the inferior vena cava compared to that in the superior vena cava. Because contrast agent is usually administered via cubital veins, this results in dilution of the contrast-medium-enhanced blood from the superior vena cava by blood from the lower body. Moreover, following deep inspiration, patients may also undergo a Valsalva maneuver, which consists of expiratory pressure placed against the closed glottis and which has been shown to decrease the pulmonary blood flow (7). Therefore, after dilution during inspiration, vessel enhancement remains low due to the decreased flow rate during breath-hold.
Another study evaluated the ratio of the contribution of the inferior vena cava to the total input blood flow of the right ventricle in patients undergoing CTA. In patients in whom low contrast-medium enhancement in the pulmonary artery was detected, the inferior vena cava contributed approximately 80% to the total flow, whereas in patients with normal enhancement the contribution was approximately 53% (2).
Appropriate patient instruction is, therefore, necessary in order to avoid excessive inspiration and the Valsalva maneuver. Instructing the patient to exhale and hold his/her breath, or image acquisition during breath-hold without any previously instructed breathing maneuver has been previously suggested to improve vessel attenuation (8,9). However, we observed that whenever a patient was not able to follow the instructions he or she was given initially, repeated instructions did not improve the patient’s compliance. This may be due to the patient’s agitated state during an acute situation (Fig. 3). Therefore, at our medical institution repeated breath-hold scans are replaced by repeated scans obtained during quiet breathing.
Following the first CT examination (a) of this 41-year-old male patient in inspirational breath-hold, he was asked to “stop breathing at the end of a normal inspiration” and the scan was then repeated (b). However, this did not improve the contrast enhancement in the main pulmonary artery. Therefore, the scan was performed again during free breathing and resulted in higher enhancement of the pulmonary arteries, which was sufficient for making a diagnosis (c). Automatic bolus triggering was accurately timed in all three scans, as seen in the high contrast enhancement in the superior vena cava and the thoracic aorta.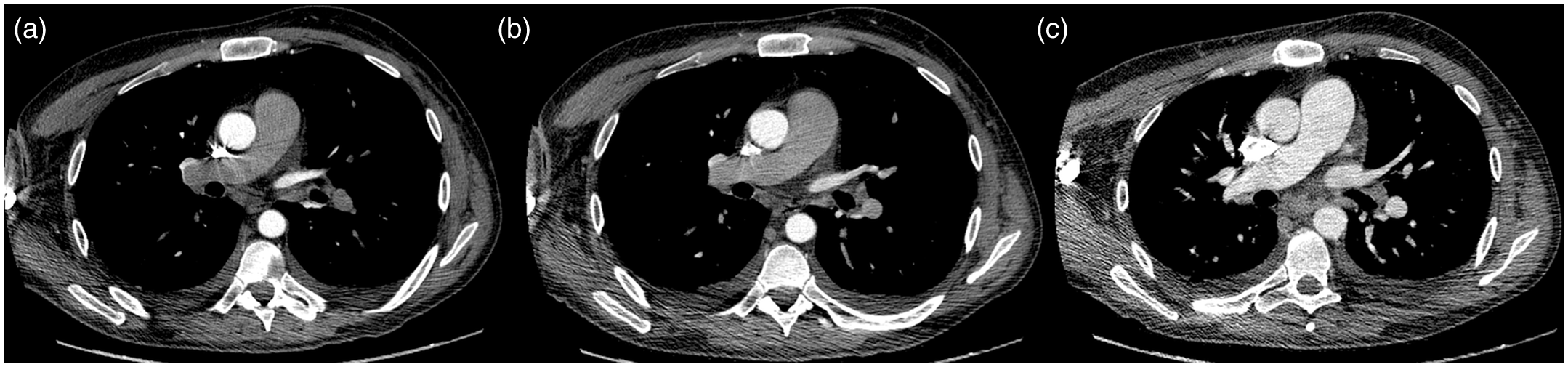
Ley et al. (10), using phase-contrast magnetic resonance imaging, showed that during smooth respiration the standard deviation for velocity measurements in the pulmonary trunk as well as the aorta were the lowest compared to inspiratory or expiratory breath-hold, and thus indicating a more uniform flow. These findings support the use of free breathing in order to achieve homogenous contrast medium enhancement in the pulmonary arteries during CT angiography.
To avoid breathing artifacts degrading the image quality, sufficient scan speed/table feed is mandatory. Using a 64-row multidetector scanner and the protocol described, we were able to obtain acceptable image quality for a diagnostic readout with substantially improved enhancement in the pulmonary artery seen in all of the evaluated cases.
Interestingly, in our study, the median age of the patients with repeated studies was 21 years younger (P = 0.02) than that of the average patient undergoing CTPA scanning for suspected PE. Perhaps due to the greater physical strength of younger patients, a deeper inspiration as well as a following Valsava maneuver may have led to higher intrathoracic pressure changes in this population. Given that younger patients are usually in superior physical shape and can obtain higher intra thoracic pressure changes than older patients, the use of an age-adjusted, free-breathing protocol is recommended if a fast scanner is available. This might help to reduce the number of repeat scans and thus the overall radiation exposure.
In patients with impaired renal function, repeated administration of contrast agent should be carefully considered. Though a recent study, as well as a meta-analysis of previous studies evaluating the incidence of contrast-induced nephropathy, did not detect any difference between groups of patients with or without the application of intravenous contrast agent (11,12), another study of Davenport et al. (13) found an increased risk of contrast-material-induced nephropathy in patients with serum creatinine levels higher than 1.5 mg/dl (13). In this at-risk group of patients a repeated scan with a reduced amount of contrast agent and imaging at 80 kV should, therefore, be considered (14). Alternatively, the second scan may be delayed 24–48 h until the serum creatinine level has been controlled, or scintigraphy may be advisable.
The comparison we made of the enhancement of the initial scan and the repeated scan showed no difference for either CT number in the ascending aorta as well as in the superior vena cava. These data emphasize that the low pulmonary artery enhancement was not caused by incorrect triggering but was due to intrathoracic pressure changes. However, the total iodine load also changed, as on repeated scans additional contrast agent was used. Therefore the enhancement, not the absolute CT values, were used for comparison.
A shortcoming of this study is that no additional testing was performed in order to determine the number of PEs. However, we are confident that the achieved image quality as well as the number of detected embolisms justifies the use of free-breathing protocols when breath-hold examinations are not of diagnostic quality.
Motion artifacts did not increase substantially with quiet breathing. Although both readers came to slightly different grading of the image quality, and reflecting the subjectivity of the quality assessment used, both readers agreed that they saw a considerable improvement in the diagnostic quality in free-breathing examinations. The motion artifacts score also showed no significant difference between the first and second scan, and both readers did not classify any exam as non-diagnostic due to motion artifacts. Therefore, it can be concluded that whenever a 64-row detector system is available, quiet breathing does not lead to significant image quality reduction caused by breathing artifacts. Of note, with the more widespread use of the latest generation of MDCT scanners with 256 row detectors, scanning time can be reduced to an extent that allows free-breathing examinations to be routinely used.
In conclusion, a free-breathing protocol can increase vessel contrast enhancement on a 64-row detector system without significant overall image quality reduction. Such a protocol should be used to improve insufficient contrast enhancement in the pulmonary arteries after other technical errors have been excluded, and it should be considered as a routine protocol for use in young or emotionally agitated patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.