
Abstract
BACKGROUND:
CT-derived fractional flow reserve (FFRCT) and diagnostic accuracy rely on good image quality during coronary CT angiography (CCTA).
OBJECTIVE:
To investigate whether heart rate (HR) and coronary artery calcium (CAC) score decrease image quality and diagnostic performance of two advanced CT scanners including 96-row detector dual source CT (DSCT) and 256-row multidetector CT (MDCT).
METHODS:
First, 79 patients who underwent CCTA (42 with DSCT and 37 with MDCT) and invasive coronary angiography (ICA) are enrolled. Next, coronary segments with excellent image quality are evaluated and the percentage is calculated. Then, diagnostic accuracy in detecting significant diameter stenosis is presented with ICA as the reference standard.
RESULTS:
Compared with the DSCT, the percentage of coronary segments with excellent image quality is lower (P = 0.010) while diagnostic accuracy on per-segment level is improved (P = 0.037) using MDCT. CAC score≥400 is the only independent factor influencing the percentage of coronary segments with excellent image quality [odds ratio (OR): DSCT, 3.096 and MDCT, 1.982] and segmental diagnostic accuracy (OR: DSCT, 2.630 and MDCT, 2.336) for both scanners. HR≥70 bpm (OR: 5.506) is the independent factor influencing the percentage of coronary segments with excellent image quality with MDCT.
CONCLULSION:
During CCTA, CAC score≥400 still decreases the proportion of coronary segments with excellent image quality and diagnostic accuracy with advanced CT scanners. HR≥70 bpm is another factor causing image quality decreasing with MDCT.
Introduction
Coronary arterial atherosclerotic disease is the leading cause of death worldwide [1]. An accurate evaluation of the severity of coronary artery lesions is crucial for the determination of treatment strategies [2, 3]. As a noninvasive imaging modality, coronary computed tomographic angiography (CCTA) has been extensively used due to its rapid and accurate evaluation for coronary artery stenosis [2–5]. In recent years, the CT-derived fractional flow reserve (FFRCT) has developed rapidly. Given the FFRCT reliance on accurate coronary and myocardial segmentation for proper image-based modeling, excellent image quality should remain a primary goal during CCTA [6, 7].
Some unfavorable conditions, such as high heart rate (HR), arrhythmias, severe calcification accompanied by artifacts, may limit the use of CCTA [8]. A medium-sharp kernel can be used to reduce the beam-hardening and blooming artifacts caused by coronary artery calcification (CAC) [9]. Also, iterative reconstruction algorithm, dual source technique, whole-heart coverage detector, and motion-correction algorithm are widely applied to improve coronary image quality [10–14]. Third-generation dual source CT (DSCT) scanners offer temporal resolution of 66 milliseconds to overcome the motion artifact caused by higher HR [10, 15–17]. The latest 256-row multidetector CT (256-row MDCT) system with garnet-based detector, 160 mm z-axis coverage and motion correction algorithm can acquire the images of whole heart within a single cardiac cycle with decreasing radiation dose [13, 18–20].
Abovementioned two latest advanced CT scanners have different advantages. Previous studies have explored the image quality and diagnostic accuracy of 256-row MDCT and DSCT respectively [4, 20]. As to the influence of high heart rate on image quality and diagnostic performance, J. Liang et al. [19] found that 256-row MDCT with motion-correction algorithm could achieve diagnostic image quality. J. Eckert et al. [4] reported that DSCT appears valuable as a tool for safely excluding in stent restenosis. However, no studies have compared the impact of heart rate and CAC on image quality diagnostic performance of these two advanced CT systems (the third-generation DSCT and 256-row MDCT) in the assessment of coronary artery stenosis.
Therefore, the purpose of our study was to compare image quality and diagnostic performance of third-generation DSCT and 256-row MDCT in the assessment of CT coronary stenosis using invasive coronary angiography (ICA) as the reference standard and to investigate impact of HR and CAC on the diagnostic accuracy and the percentage of coronary segments with excellent image quality.
Materials and methods
Patients
From March 2018 to May 2019, 90 consecutive patients underwent both CCTA (either the third-generation DSCT or 256-row MDCT) and ICA in our hospital. 11 patients were excluded due to the interval between CCTA examination and ICA longer than 4 weeks. Finally, 79 patients [54 men and 25 women, mean age: (63.6±10.8) years old] were enrolled in this study. This retrospective study was approved by the institutional review board and written informed consent was obtained from all individual participants included in the study.
CCTA protocol
Forty-two patients were examined using the third-generation DSCT scanner (SOMATOM Force, Siemens Healthineers, Forchheim, Germany) and thirty-seven patients using 256-row MDCT scanner (Revolution CT, GE Healthcare, Milwaukee, WI, USA). All patients without contraindication were treated with nitroglycerin 0.5 mg sublingually for coronary vasodilatation after being positioned on the scanner table. No beta-blocker was applied prior to CCTA exams. Non-contrast prospective electrocardiography (ECG)-triggering scan was performed for CAC score. Then, contrast medium (370 mg iodine/ mL, Ultravist, Bayer Schering Pharma, Berlin, Germany) was administrated via a 20-G intravenous catheter, followed by 40 mL saline using a dual-head power injector. The injection duration was determined by scan time plus 8 seconds and the flow rate ranging from 3.0 to 6.0 mL/s was tailored to the body weight, HR and tube voltage [21, 22]. Finally, CCTA scanning at the end of inspiratory breath holding with bolus tracking technique were performed under tube voltage and tube current individually tailored to patient habitus automatically by the scanners respectively.
DSCT scanned mainly using prospective ECG-triggering with tube voltage from 70 to 120 kVp. Gantry rotation speed was 0.25 second per rotation and collimation of 96×0.5 mm. Axial images with slice thickness of 0.75 mm and increment of 0.5 mm were reconstructed at best diastolic and best systolic phases (both phases determined by the scanners automatically) using advanced modeled iterative reconstruction (ADMIRE, Siemens Healthcare, Forchheim, Germany) at strength 3 and a medium soft convolution kernel (Bv36).
Prospective ECG triggering scanning with tube voltage from 100 to 120 kVp was applied to 256-row MDCT within one heartbeat. The collimation is 0.625 mm with detector coverage from 120 to 160 mm based on the scout image. Gantry rotation speed was 0.28 second per rotation. Images with section thickness and section interval of 0.625 mm were reconstructed using 50% of the adaptive statistical iterative reconstruction-V (ASIR-V, GE Health-care, United States) algorithm. The cardiac phase with least coronary motion was selected semi-automatically, and snapshot freeze (SSF) motion correction algorithm was applied to further minimize artefacts.
Imaging analysis
CCTA evaluation including CAC quantification, coronary stenosis and image quality was all performed on a commercially available workstation (Syngo Via VA30A, Siemens Healthcare, Forchheim, Germany). Quantification of CAC was approached by Agatston score [23]. Each coronary calcification scored accounting for both the total area and the maximal density of coronary calcification. Agatston score was calculated as the sum of the scores for all individual calcified lesions in all coronary arteries. It was calculated as the sum of the scores (accounting for both the total area and the maximal density) for all individual calcified lesions in all coronary arteries. The 18-segment model of coronary artery tree was used according to the guidelines proposed by the Society of Cardiovascular Computed Tomography [24]. All segments < 1.5 mm in diameter were excluded from evaluation. All CT image assessment was independently assessed by two experienced radiologists (with 3 and 10 years of experience in cardiac CT imaging, respectively) who were blind to ICA results. A four-point Likert scale was used to assess the image qualitatively: 1 = excellent image quality free of artefacts; 2 = good image quality with minor artefacts, but fully evaluable and diagnostic; 3 = adequate image quality with moderate artefacts, but acceptable for diagnosis; 4 = poor/severe artefacts and non-diagnostic image quality [25]. Evaluable segments were assessed independently for the presence or absence of significant coronary arterial lumen stenosis, defined as a diameter narrowing≥50% [26].
Disagreements regarding the image scores and stenosis between two radiologists were resolved in consensus during a joint reading session. The attenuation and image noise of ascending aorta (AA) at the level of orifice of left main (LM) were measured, as well as the attenuation of LM and proximal segment of right coronary artery were taken.
Invasive coronary angiography
ICA images were evaluated to define the presence of a diameter narrowing≥50% by two experienced interventionists (with 6 and 14 years of experience) who were blind to results of CCTA. At least 2 orthogonal views of each coronary artery were analyzed to determine stenosis, and additional views were used whenever necessary. The ICA was used as the reference standard to determine significant stenosis independent of the CCTA results.
Statistical analysis
The normality of data distributions was analyzed using the Kolmogorov–Smirnov test. All numeric data with normal distributions were reported as mean±SD, and an independent sample t test was adopted. Otherwise, medians (25th–75th percentile) were reported, and the Mann-Whitney U test was used. A chi-square test was used to compare the difference of gender distribution between two scanners. The interobserver agreement of image quality scoring and coronary stenosis detection was tested by the Cohen’s kappa. This was interpreted as moderate for 0.40 < kappa < 0.60, good for 0.60 < kappa < 0.80, and excellent for kappa > 0.80. The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of CCTA to detect≥50% diameter stenosis was calculated using the chi-squared test of the contingency table based on a segment analysis. Patient were divided into high HR group (HR≥70 beat per minute, bpm) and low HR group (HR < 70 bpm), as well as no severe CAC group (CAC score < 400) and severe CAC group (CAC score≥400). The impact of HR and CAC score on diagnostic accuracy and image quality was investigated by Chi-square test and multivariate logistic regression. The odds ratio (OR) value could be obtained after the logistic regression analysis. All statistical analyses were performed using SPSS (version 23.0, Chicago, IL). A two-sided P value < 0.05 was considered statistically significant.
Results
Study population
All 79 enrolled patients underwent CCTA and ICA within an interval of 7.3±5.0 days. There was a high prevalence of stenosis of 50% or more on a per-segment level, which was 23.0% (236/1026). There were no differences on age (P = 0.305) or gender distribution (P = 0.786) between two groups. The differences of CAC Score, HR and arterial attenuation between two groups showed no statistical significance. In our study, compared to 256-row MDCT, DSCT group showed lower image noise and higher dose length product. Table 1 demonstrated the detailed information of patient and scan-related characteristics.
Detailed information of patients’ and scanning characteristics between third-generation dual source CT scanner (DSCT) and 256-row multidetector CT scanner (MDCT)
Detailed information of patients’ and scanning characteristics between third-generation dual source CT scanner (DSCT) and 256-row multidetector CT scanner (MDCT)
Numeric data with normal distributions were reported as mean±standard deviation and otherwise medians (25th, 75th percentile) were reported.
A total of 549 coronary segments from 42 patients were assessed using DSCT and 477 segments from 37 patients using 256-row MDCT. Intrareader reproducibility of image quality evaluation and coronary stenosis detection between the two independent readers was excellent for both CT scanners respectively. Detailed image quality score of two CT scanners based on segment analysis were shown in Table 2. Two non-diagnostic segments (Fig. 1) were presented by 256-row MDCT (one patient with HR of 84 bpm, the other patient with CAC score of 2045.7), and none by DSCT. DSCT obtained better image quality on per-segment level than 256-row MDCT significantly (P = 0.033). The percentage of coronary segments with excellent image quality by DSCT was higher than by 256-row MDCT (DSCT 91.7% vs 256-row MDCT 86.7%, P = 0.010).
Detailed image quality score of third-generation dual source CT scanner (DSCT) and 256-row multidetector CT scanner (MDCT) based on per-segment level assessment
Detailed image quality score of third-generation dual source CT scanner (DSCT) and 256-row multidetector CT scanner (MDCT) based on per-segment level assessment
Note: Data are number of segments, and data in parentheses are percentages.
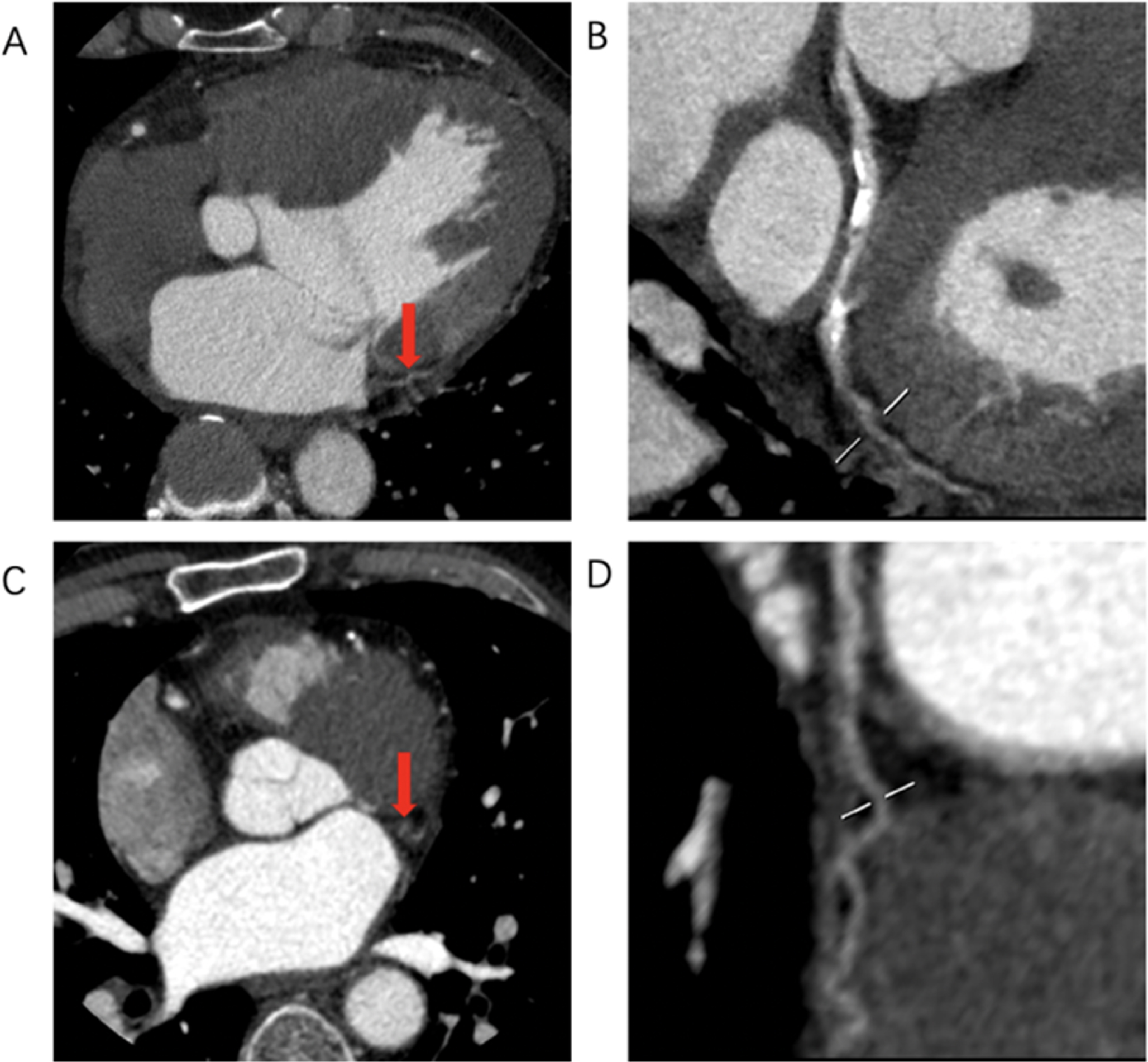
Images of the two non-diagnostic segments from two cases by 256-row multi-detector CT. Figures A and B are axial and curved planar reformatted images of the distal segment of left circumflex artery of one case, C and D are of obtuse marginal branch from another case respectively.
When based on per-segment level analysis, 21.9% (120/549) of the segments scanned by DSCT and 24.2% (115/475) scanned by 256-row MDCT were defined as significant stenosis by IAC. The accuracy, sensitivity, specificity, PPV and NPV of DSCT in detecting significant stenosis was 92.7%, 80.0%, 96.3%, 85.7% and 94.5%, respectively. The corresponding values of 256-row MDCT were 95.8%, 87.07%, 98.6%, 95.9% and 98.2%. When compared with the DSCT, the use of 256-row MDCT was associated with an improvement in accuracy and PPV on per-segment level assessment (p = 0.037 and p = 0.018) respectively. Table 3 summarized the detailed diagnostic performance of DSCT and 256-row MDCT in detecting significant stenosis based on per-segment level. Figure 2 and Fig. 3 illustrated two false-positive cases detected by DSCT and 256-row MDCT, respectively.
Comparison of the diagnostic accuracy of third-generation dual source CT scanner (DSCT group) and 256-row multidetector CT scanner (MDCT) in the detection of significant diameter stenosis (> 50%) for segment-based analysis
NPV: negative predictive value and PPV: positive predictive value.
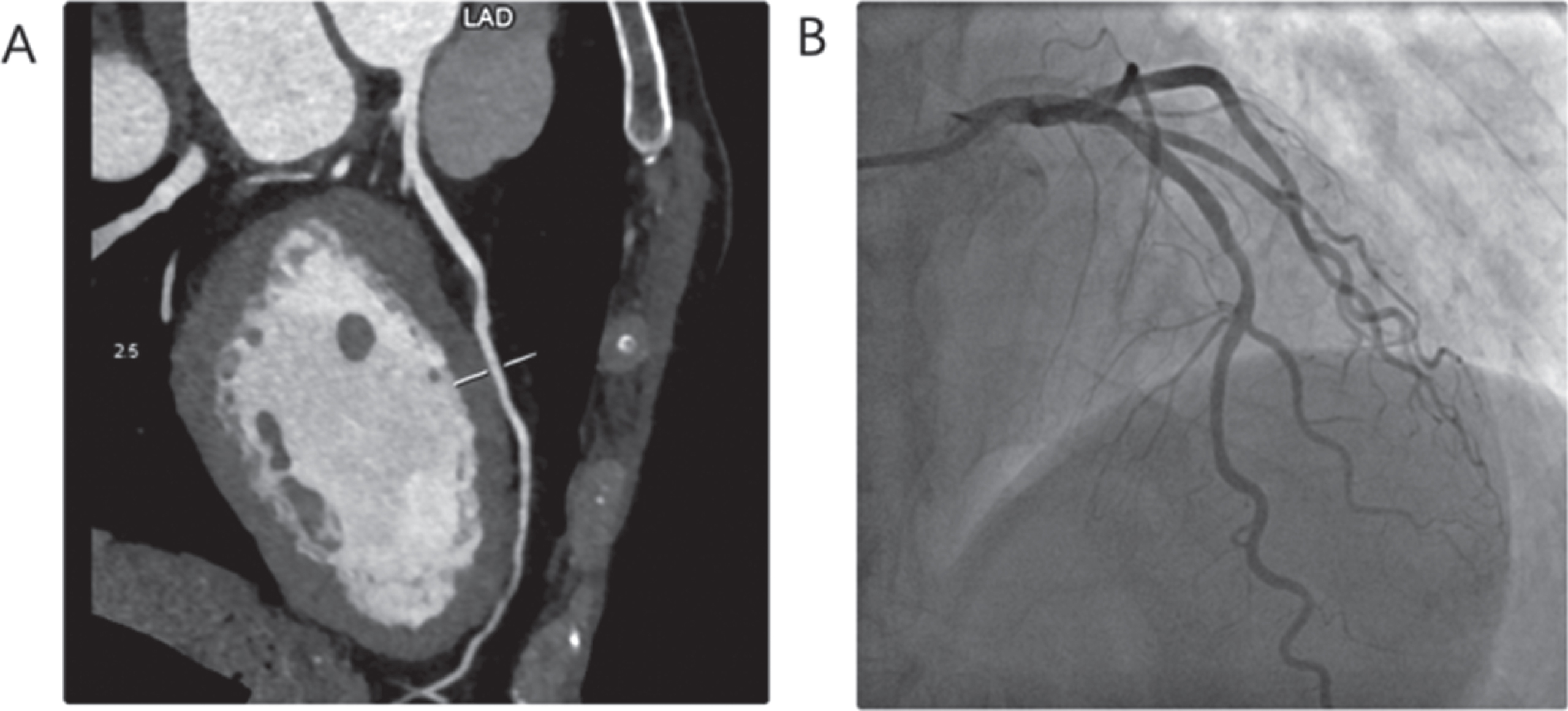
An example of false-positive case by dual source CT in per-patient level. Detection of≥50% diameter stenosis in middle segment of left arterial descending artery (A) using dual source CT and < 50% diameter stenosis by invasive coronary artery (B).
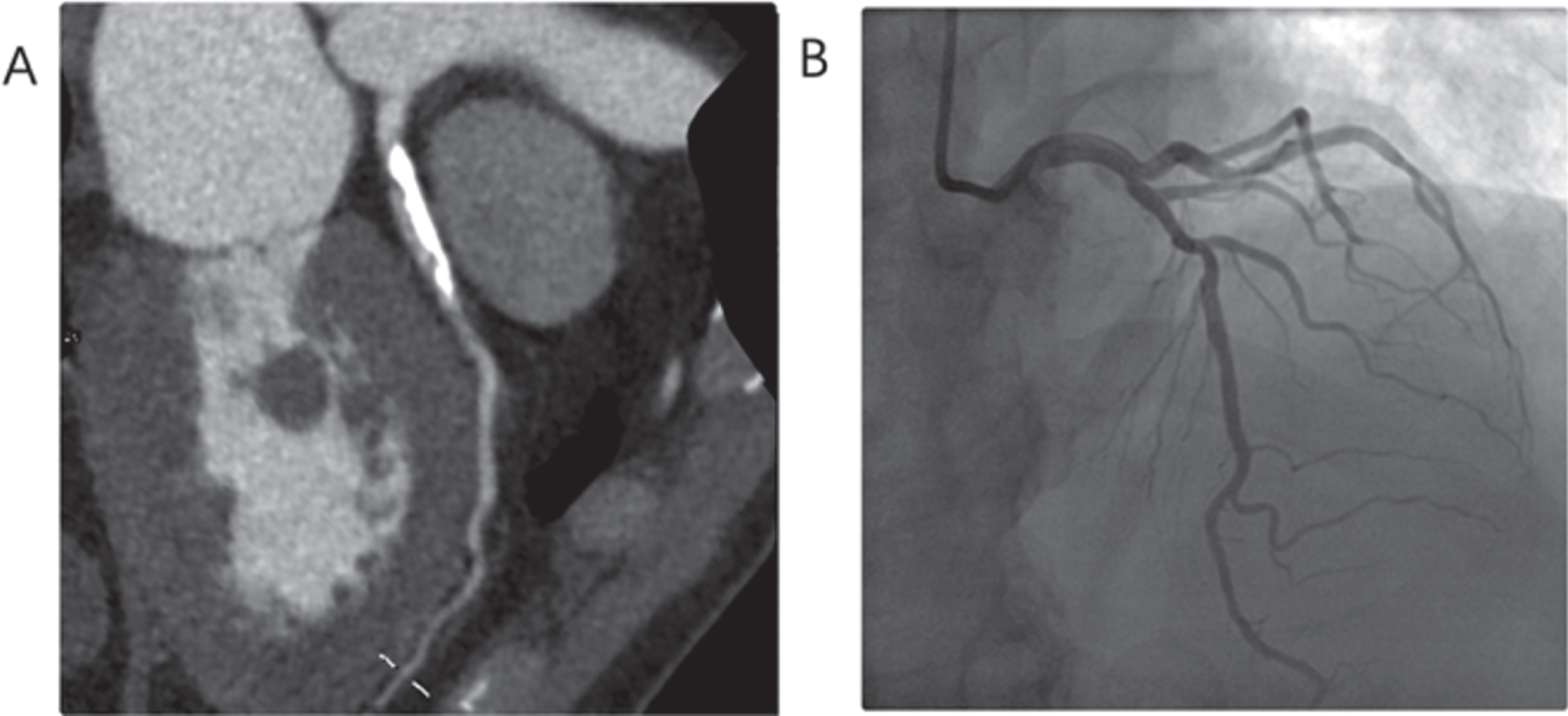
An example of false-positive case by 256-row multi-detector CT in per-patient level. Detection of≥50% diameter stenosis in proximal segment of left arterial descending artery (A) using 256-row MDCT and < 50% diameter stenosis by invasive coronary artery (B).
With the use of DSCT, percentages of coronary segments with excellent image quality were similar between low HR group and high HR group (low HR group 92.2% vs high HR group 90.9%, p = 0.584); with the use of 256-MDCT, low HR group higher than high HR group (low HR group 95.2% vs high HR group 80.4%, p < 0.001). In contrast, with the use of DSCT, percentage of coronary segments with excellent image quality in no severe CAC group was higher than severe CAC group (no severe CAC group 95.2% vs severe CAC group 86.5%, p < 0.001); with the use of 256-MDCT, no severe CAC group and severe CAC group were similar (no severe CAC group 88.7% vs severe CAC group 83.8%, p = 0.118). Taking age, sex, attenuation and image noise of AA, HR group and CAC group into multivariate logistic regression, CAC score≥400 (OR:3.096, 95% CI: 1.651–5.806; P < 0.001) was the independent factor influencing the percentage of coronary segments with excellent image quality by DSCT, while both CAC score≥400 (OR:1.982, 95% CI: 1.140–3.446; P = 0.015) and HR≥70 bpm (OR:5.506, 95% CI: 2.695–11.248; P < 0.001) were the independent factors by 256-MDCT. Figure 4 presents impact of HR and CAC on image quality by using DSCT and 256-row MDCT.
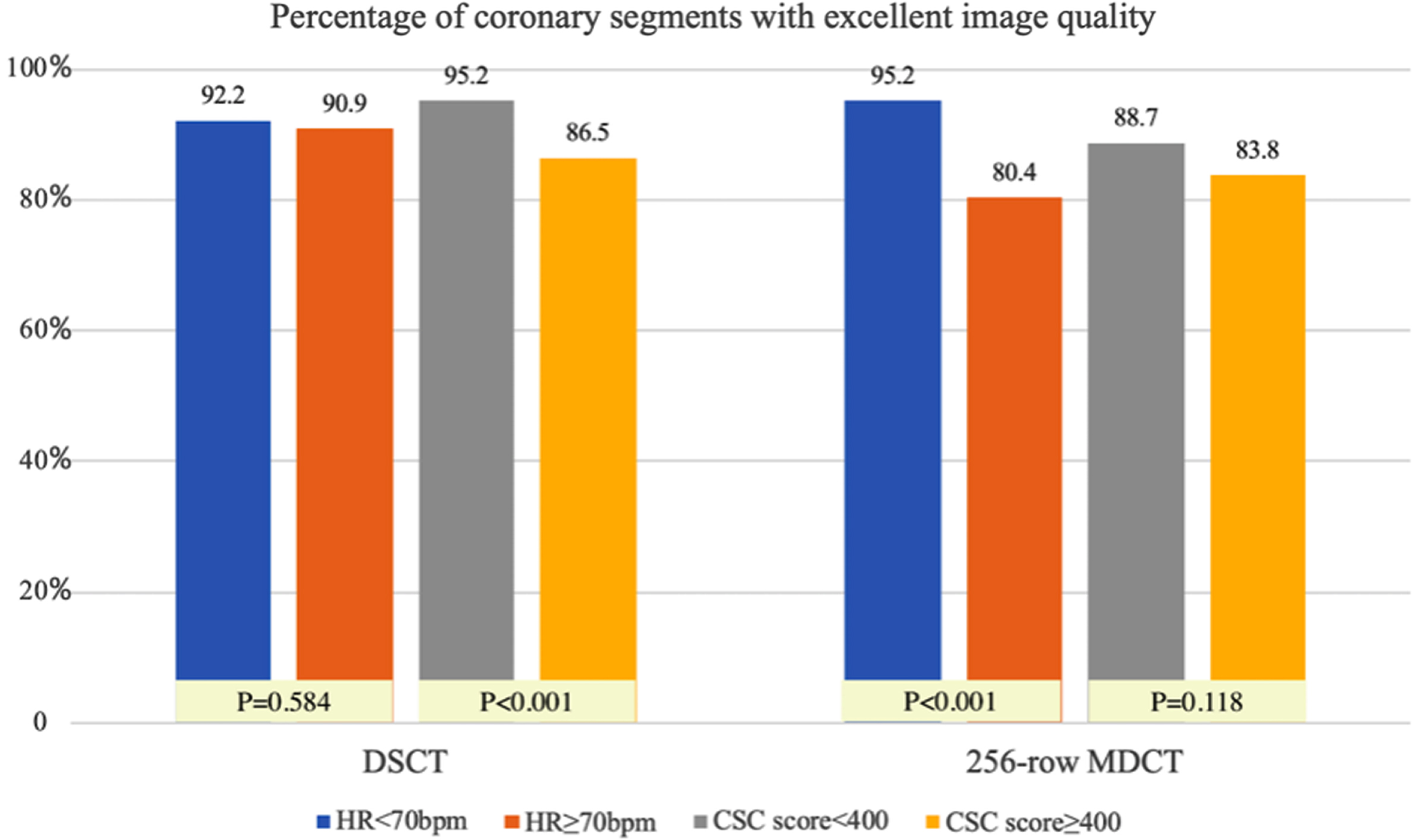
Impact of heart rate (HR) and coronary artery score (CAC) on image quality by using dual source CT (DSCT) and 256-row multi-detector CT (MDCT). Percentages of coronary segments with excellent image quality by DSCT was higher in patients with CAC score < 400 than CAC score≥400. This percentages by MDCT was higher in patients with HR < 70 bpm than HR≥70 bpm.
Between low HR group and high HR group, the diagnostic accuracy on per-segment level was similar with use of DSCT (low HR group 92.2% versus High HR group 93.5%, P = 0.559) and with use of 256-row MDCT (low HR group 97.1% versus High HR group 94.8%, P = 0.218). Between no severe CAC group and severe CAC group, the diagnostic accuracy on per-segment level was similar with the use of DSCT (no severe CAC group 94.2% versus severe CAC group 90.3%, P = 0.086); while no severe CAC group was higher than severe CAC group with 256-row MDCT (no severe CAC group 97.5% versus severe CAC group 93.0%, P = 0.017). Taking age, sex, attenuation and image noise of AA, HR group, and CAC group into multivariate logistic regression, CAC score≥400 was the independent factor influencing the diagnostic accuracy on per-segment level by DSCT (OR:2.630, 95% CI: 1.468–4.713; P = 0.001) and by 256-MDCT (OR:2.336, 95% CI: 1.059–5.149; P = 0.035). Figure 5 presents impact of HR and CAC on diagnostic accuracy by using DSCT and 256-row MDCT.
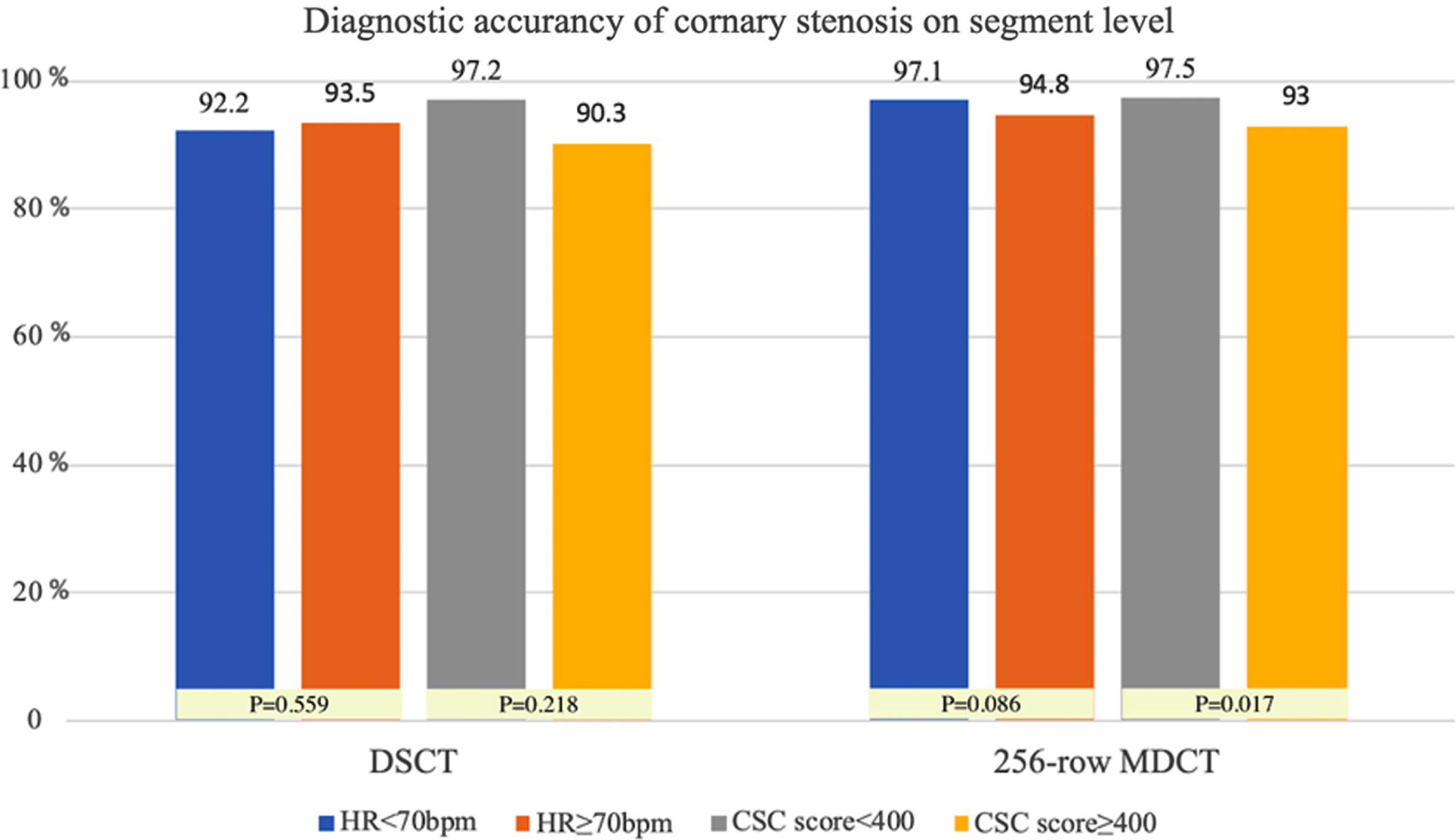
Impact of heart rate (HR) and coronary artery score (CAC) on diagnostic accuracy by using dual source CT (DSCT) and 256-row multi-detector CT (MDCT). Diagnostic accuracy on per-segment level were similar in patients with HR < 70 bpm and HR≥70 bpm by DSCT and MDCT respectively. Diagnostic accuracy by DSCT was higher in patients with CAC score < 400 than CAC score≥400.
This study demonstrated that both DSCT and 256-row MDCT could obtain high diagnostic accuracy in assessing coronary artery stenosis. CAC score≥400 was the only independent factor influencing the percentage of coronary segments with excellent image quality with DSCT, while both CAC score≥400 and HR≥70 bpm were the independent factors with MDCT. CAC score≥400 was also the independent factor influencing the diagnostic accuracy on per-segment level with DSCT and with 256-MDCT.
The third-generation DSCT is equipped with two sets of tubes and detectors, which allows for a higher spatial resolution and temporal resolution [15]. Besides, its iterative reconstruction and true stack technique can also improve image quality [15, 27]. In our study, all segments obtained from DSCT are interpretable. With the increasing number of detector rows and application of SSF technique, 256-row MDCT could also obtain good image quality [10]. However, our study results indicated that 256-row MDCT still have some non-diagnostic segments, which is consistent with previous study [12, 20]. The excellent image quality is critical for further analysis, such as CT-derived coronary fraction flow reserve and coronary plaque quantitative analysis [28, 29]. Our study demonstrated that the DSCT produced higher percentage of images with excellent image quality, which is favorable for further analysis.
Our results showed both CT scanners could obtain high diagnostic accuracy, which was in accordance with previous studies [19, 30]. Overall, the diagnostic accuracy of 256-row MDCT was slightly higher than that of DSCT in our study, and the differences showed statistical significance when based on segment-level analysis. Meanwhile, our study also demonstrated that the 256-row MDCT had a higher PPV value at segment-level, which was the main contributor to the higher diagnostic accuracy. The higher PPV value may give the credit to the wider detector of 256-MDCT. All axial images obtained by 256-row MDCT can be completed in one cardiac cycle with free breathing without slice overlap. In contrast, the data acquisition by DSCT is achieved in several cardiac cycles, and it produces artifacts caused by slice overlaps especially in patients with arrhythmia and/or poor breath holding, which may go against the PPV. Although the 256-row MDCT has less temporal resolution when compared with DSCT, the impact of this disadvantage on image quality did not affect the sensitivity and specificity in detecting a 50% diameter stenosis.
DSCT could obtain good diagnostic performance regardless of HR [8], which is also confirmed in our study by that diagnostic accuracy is similar in patients with HR < 70bpm and with≥70 bpm. Due to the high temporal resolution of DSCT, the image quality of high HR group remains the same as that of lower HR group. Previous studies present that diagnostic accuracy of CCTA using 256-row MDCT in patients with high heart rate improves significantly by SSF technique [18, 31]. In our study, we also demonstrate that diagnostic accuracy with HR≥70 bpm is not inferior in patients than with HR < 70 bpm by using of 256-row MDCT with SSF technique, which was consistent with the finding of Jiang’s study [20]. However, our study demonstrated that the image quality of HR≥70 bpm is inferior to that of HR < 70 bpm by 256-row MDCT.
CAC score has significant influence on diagnostic image quality and diagnostic accuracy [8, 33]. Diagnostic image quality significantly decreases in third generation of DSCT by prospective ECG-gating in patients with CAC score≥2,000 [8]. In our study, diagnostic accuracy and image quality on per-segment level by using DSCT also have a tendency of decreasing in patients with CAC score≥400. Similarly, 256-row MDCT also has a decreasing diagnostic accuracy in patient with severe CAC.
There are some limitations of this study needed to be acknowledged. Firstly, this is a single-center study with a small sample size. Further studies with larger sample size or among multi-center are needed to validate the present results. Secondly, we did not explore the influence of heart rate rhythm on diagnostic accuracy due to limited cases. Thirdly, we did not keep the radiation dose at a similar level which would influence the image quality.
In conclusion, both DSCT and 256-row MDCT could obtain high diagnostic accuracy in assessing coronary artery stenosis. The diagnostic accuracy of DSCT and 256-row MDCT is mainly influenced by CAC. Image quality of DSCT decrease with CAC score increases but image quality of 256-row MDCT decreases with HR increases.
Ethical statement
This retrospective study was approved by the institutional review board (the first affiliate hospital of Nanjing medical university) and written informed consent was obtained from all individual participants included in the study.
Footnotes
Acknowledgments
This work was done in department of radiology, the first affiliated hospital of Nanjing medical university. This research was partly supported by the National Natural Science Foundation of China under grants (81701651 and 81601464). The study was also supported by being blinded for review, which have no influence on the outcome of this research.