
Abstract
Background
Three-vessel coronary artery disease (CAD) comes along with globally reduced myocardial perfusion potentially restricting the demarcation of regional hypoperfusion in stress perfusion cardiac magnetic resonance imaging (MRI).
Purpose
To evaluate whether stress perfusion cardiac MRI is capable of detecting myocardial hypoperfusion in patients with 3-vessel CAD reliably.
Material and Methods
Two hundred and five patients with symptoms of CAD were included. The examination protocol comprised imaging of myocardial perfusion at stress (0.14 mg/kg/min adenosine for 4 min) using a 2D saturation recovery gradient echo sequence after administration of gadobutrol (0.1 mmol/kg body weight). Perfusion sequences were assessed qualitatively by two experienced observers. Coronary angiography served as standard of reference.
Results
Sensitivity and specificity for hemodynamically relevant stenoses in patients with 0-, 1-, 2-, 3-vessel coronary artery disease were 100%/91%, 91%/73%, 90%/71%, 92%/64%; positive/negative predictive value, 67%/100%, 91%/73%, 83%/81%, 93%/58%; diagnostic accuracy, 93%/87%/83%/87%, respectively. The negative predictive value in patients with 3-vessel CAD was lower than in patients with 0- and 2-vessel CAD and the specificity lower than in patients with no CAD whereas the positive predictive value was higher than in patients with no CAD. The other proportions did not differ significantly between the groups.
Conclusion
The diagnostic value of stress perfusion cardiac MRI in patients with 3-vessel CAD is comparable to results in patients with 1- or 2-vessel CAD. In the rare event that stress perfusion images do not depict regional hypoperfusion in patients with severe 3-vessel CAD, myocardial ischemia could be identified by reduced semi-quantitative perfusion parameters.
Keywords
Introduction
Besides various manifestations of arteriosclerosis coronary artery disease (CAD) is the leading cause of death in the industrialized world (1–4). Consequently there is an increasing demand for techniques being capable to detect CAD reliably at an early stage.
In the course of CAD, several phases are passed through beginning with reduced myocardial perfusion at stress and ending up in myocardial infarction (MI) (5–7). Due to the course of CAD described as cascade of ischemia, there is a special interest in techniques assessing myocardial perfusion at stress to reveal first signs of CAD (8).
As success of systematic prevention had been limited (9), the focus is on an early diagnosis seeking to reduce mortality and morbidity (10,11). Most widely spread techniques to assess myocardial perfusion are single photon emission tomography (SPECT) and myocardial stress perfusion magnetic resonance imaging (SPCMR) (8,12–15). The capability of SPCMR to detect CAD was confirmed by a number of studies (16,17). Pharmacologically induced stress by adenosine infusion causes vascular dilation in normal vessels with consequently increased myocardial perfusion and due to the lack of perfusion reserve consequent relative hypoperfusion in myocardium supplied by coronary arteries with stenoses. This can be depicted by reduced and delayed contrast enhancement of the corresponding myocardial segments during the first pass (12,18).
Consequently, the detection of CAD necessitates a significant regional difference of myocardial perfusion (18–21). In the case of progressed CAD, regional differences of myocardial perfusion will be reduced due to globally restricted perfusion and myocardial ischemia might evade detection by SPCMR. For a technique developed to detect CAD at an early stage an impairment of the diagnostic accuracy in patients with progressed disease might be a limitation.
Aim of our study was to assess retrospectively, if SPCMR will identify decreased myocardial perfusion reliably in patients with 3-vessel CAD compared to 1- or 2-vessel CAD.
Material and Methods
Patient group
Patient group composition.
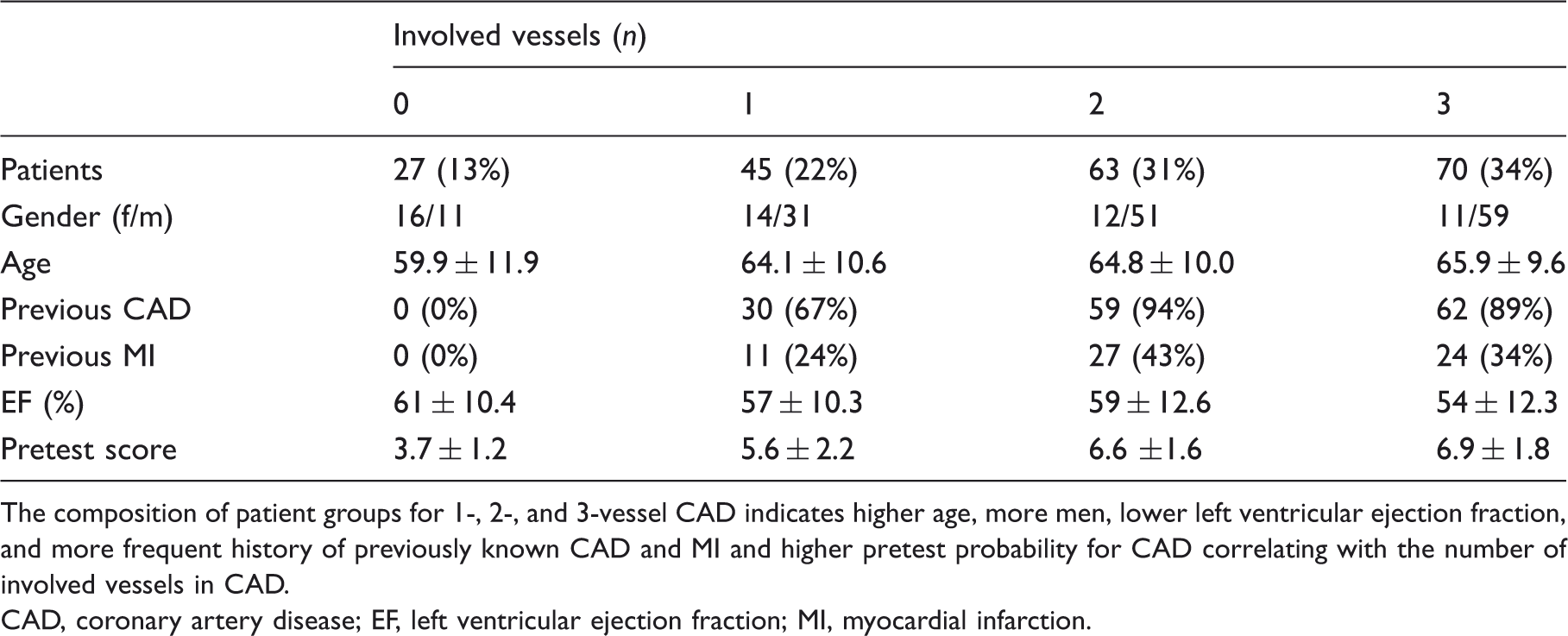
The composition of patient groups for 1-, 2-, and 3-vessel CAD indicates higher age, more men, lower left ventricular ejection fraction, and more frequent history of previously known CAD and MI and higher pretest probability for CAD correlating with the number of involved vessels in CAD.
CAD, coronary artery disease; EF, left ventricular ejection fraction; MI, myocardial infarction.
For the assessment of risk factors for CAD and determination of the pretest probability for stress-induced myocardial ischemia, an 11-point scale was used which included age exceeding 50 years, male gender, previously known CAD, previously known MI, diabetes mellitus, hyperlipidemia, nicotine consumption, hereditary predisposition, arterial hypertension, obesity and pathologic ergometry. Each risk factor was either rated as 1, if present, or as 0, if absent, resulting in a maximum score of 11 points. The mean value of the pretest score was calculated for each group.
MRI
Myocardial perfusion:
SPCMR was performed on a 1.5T system using a multi-channel surface coil (Magnetom Avanto or Magnetom Sonata, Siemens Healthcare, Erlangen, Germany). All sequences were performed with electrocardiography (ECG)-triggered and breath-hold technique. Stress was induced by infusion of 0.14 mg/kg/min adenosine over 4 min. Three minutes after the start of the infusion, a 2D saturation recovery gradient echo sequence in short-axis orientation was acquired to assess myocardial perfusion at stress. Sequence parameters were as follows: TR, 2.2 ms; TE, 1.1 ms; flip angle, 12°; baseline matrix, 192; slice thickness, 8 mm; receiver bandwidth, 650 Hz/pixel; parallel imaging with an acceleration factor of two (GRAPPA; 0.1 mmol/kg bodyweight gadobutrol (Bayer HealthCare, Leverkusen, Germany) were injected at a flow rate of 4 mL/s. During 40 cardiac cycles, three representative short-axis slices were acquired for each heart cycle at a basal, mid-ventricular and apical position. After 10 min perfusion images at rest were acquired using identical sequence parameters.
Myocardial function:
Left ventricular function was assessed using cine steady state free precession (SSFP) sequences in standard angulations (four-chamber view, two-chamber view, and short-axis views including three short-axis views in corresponding slice position to the perfusion sequences).
Myocardial viability:
Ten minutes after resting perfusion, myocardial viability was assessed using segmented inversion recovery gradient echo sequences in standard angulations corresponding to the cine SSFP sequences. Inversion time was optimized individually using an inversion time localizer sequence (TI-Scout, Siemens Healthcare).
The total examination took 45 minutes on average.
Coronary catheter angiography:
All patients of the study population were admitted to invasive coronary angiography to confirm and treat or to rule out hemodynamically relevant coronary artery stenoses. After ventriculography, selective angiography of each coronary artery was performed using digital subtraction technique. Coronary angiography serving as the standard of reference for SPCMR was assessed in consensus by two experienced interventional cardiologists in regard of the presence and extent of coronary artery stenoses. Stenoses exceeding 70% of the vascular diameter were regarded as hemodynamically relevant and treated using angioplasty and if necessary additional stent implantation. Presence of stenoses with at least 70% in right coronary artery (RCA) and left anterior descending (LAD) and left circumflex (LCX) or left main coronary artery, respectively, was classified as 3-vessel CAD.
Image analysis:
Two independent experienced radiologists assessed SPCMR using dedicated software for qualitative and quantitative image analysis (ARGUS®, Siemens Healthcare, Erlangen, Germany). Perfusion, function and viability analysis of the left ventricular myocardium were performed based on the American Heart Association 17-segment model (22).
Myocardial perfusion:
Perfusion images were assessed qualitatively in regard of the presence, localization and extent of myocardial hypoperfusion. Myocardium was classified as hypoperfused, if regional contrast enhancement during the first pass had been delayed and reduced compared to adjacent myocardium on at least five following images. Semi-quantitative perfusion analysis was performed, if qualitative analysis indicated no stress-induced ischemia in spite of an angiographically confirmed coronary artery stenosis. Epicardial and endocardial contours were manually drawn on stress and resting perfusion images using dedicated software (ARGUS®). Peak signal intensity, time to peak, upslope, and area under the curve of the myocardial signal intensity curve were calculated. Semi-quantitative parameters were defined as follows: upslope as mean slope of the signal intensity curve starting with unenhanced myocardium to the maximum signal intensity during the myocardial first pass of the contrast agent; peak signal intensity as the highest signal intensity value of the signal intensity over time curve. The signal over time curve was normalized to the arterial input function. The myocardial perfusion reserve index (MPRI) was calculated as the ratio of the upslope at stress and at rest. Results were compared with the results of patients without stress-induced ischemia in SPCMR and no CAD in coronary angiography as the standard of reference, as myocardial perfusion in these patients is presumably normal.
Image quality was rated on a four-point scale ranging from 1 to 4: 1, poor image quality, myocardial perfusion cannot be assessed sufficiently, significant motion artifacts (breathing, arrhythmia); 2, moderate image quality, myocardial hypoperfusion can be identified although not easily and rapidly, moderate motion artifacts; 3, good image quality, myocardial hypoperfusion with sharp delineation to adjacent myocardium in most parts, no or minimal motion artifacts; and 4, excellent image quality, sharp delineation and high contrast of hypoperfused myocardium to adjacent myocardium enabling easy and rapid identification of myocardial ischemia, no motion artifacts.
Left ventricular function:
Left ventricular function was assessed qualitatively and quantitatively as well. Each segment was classified qualitatively as normokinetic, hypokinetic, akinetic, or dyskinetic. For quantitative assessment end-diastolic and end-systolic volumes of the left ventricle, stroke volume, and ejection fraction were calculated on short-axis cine SSFP sequences using dedicated software for functional analysis (ARGUS®).
Myocardial viability:
Late gadolinium enhancement images (LGE) were assessed qualitatively by two experienced radiologists in consensus reading for the presence and size of regional hyperenhancement representing MI. Subendocardial or transmural hyperenhancement of vessel-territory distribution visible at 10–20 min after contrast injection was regarded as MI.
Image interpretation:
Results of myocardial perfusion at stress as well as myocardial viability analysis were correlated to determine presence and extent of stress-induced ischemia. Mismatch of perfusion and viability imaging was rated as myocardial ischemia. To confirm a potential mismatch of perfusion and viability imaging, regional hypoperfusion at stress had to be classified larger in regard of its transmural extent or to affect at least one more segment of left ventricular myocardium, otherwise it was categorized as MI without stress-induced ischemia of viable myocardium (23).
Statistical analysis
Continuous measures are presented as mean ± standard deviation if not stated otherwise. Presence and localization of stress-induced ischemia found by MRI was correlated with stenoses found by coronary angiography. SPCMR was rated true positive, if ischemic myocardium had been found in segments supplied by a coronary artery with hemodynamically relevant stenosis, false positive if there had been either no hemodynamically relevant stenosis or the ischemic segments were not localized in the territory supplied by the stenosed artery according to the AHA 17-segment model. If no ischemia had been detected on stress perfusion images in spite of the presence of a hemodynamically relevant coronary artery stenosis on angiograms, SPCMR was categorized as false negative.
According to the angiographical results, patients were divided retrospectively in four groups: 0, no CAD; 1, 1-vessel CAD; 2, 2-vessel CAD; or 3, 3-vessel CAD. Sensitivity, specificity, positive and negative predictive values as well as diagnostic accuracy were calculated for each patient group. Results of patients with 3-vessel CAD were compared to results of patients with no, 1-, and 2-vessel-CAD using chi-square test for comparison of proportions. P values <0.05 were regarded as significant difference (95% confidence interval). For statistical analysis, MedCalc (MedCalc 12, MedCalc Software, Ostend, Belgium) was used.
Results
Patient group composition:
Standard of reference for perfusion analysis was coronary catheter angiography in all patients performed within 10.2 ± 22.0 days to SPCMR. The extent of CAD correlates with age and gender reflected by increasing mean age and proportion of males from group 0 to group 3 (Table 1). Patients with previously known CAD have a tendency to more extended disease, yet, even in group 3, 18 of 70 patients were not previously known to have CAD (Table 1). The pretest probability score correlates with the extent of CAD as expressed in the number of involved vessels and is significantly lower in those patients with no CAD and no stress-induced ischemia in SPCMR (group 0).
Stress-induced myocardial ischemia was observed in 143 of 205 patients (70%). Twenty patients were classified as false positive as in spite of stress-induced ischemia in SPCMR no stenoses exceeding 70% were found by angiography. Yet, 17 patients were found to have intermediate stenoses of 50-69%. In the whole study group, intermediate stenoses were found in 38 patients by angiography, SPCMR indicated stress-induced ischemia in 17 of these patients. In 21 patients with intermediate stenosis, no ischemia was found by SPCMR.
Myocardial perfusion:
Results of the perfusion analysis for each group are given in Table 2 and Fig 1.
Diagnostic yield of stress perfusion cardiac MRI. Results of stress perfusion cardiac MRI for each patient group indicate reduced specificity and negative predictive value in spite of good diagnostic accuracy in patients with 3-vessel CAD. 1-, 2-, 3-CAD, 1-, 2-, 3-vessel coronary artery disease; DA, diagnostic accuracy; NPV, negative predictive value; PPV, positive predictive value; Sens, sensitivity; Spec, specificity. Diagnostic yield of stress perfusion cardiac MRI. Median image quality, number of ischemic segments of all segments, and number of false positive and negative patients as well as true positive and negative patients for each subgroup (no CAD, 1-, 2-, and 3-vessel CAD). Stress perfusion cardiac MRI provides good overall diagnostic accuracy for 1-, 2-, and 3-vessel CAD, respectively, comparable to published data. However, specificity and negative predictive value in patients with three-vessel coronary artery disease are reduced (NPV, negative predictive value; PPV, positive predictive value).
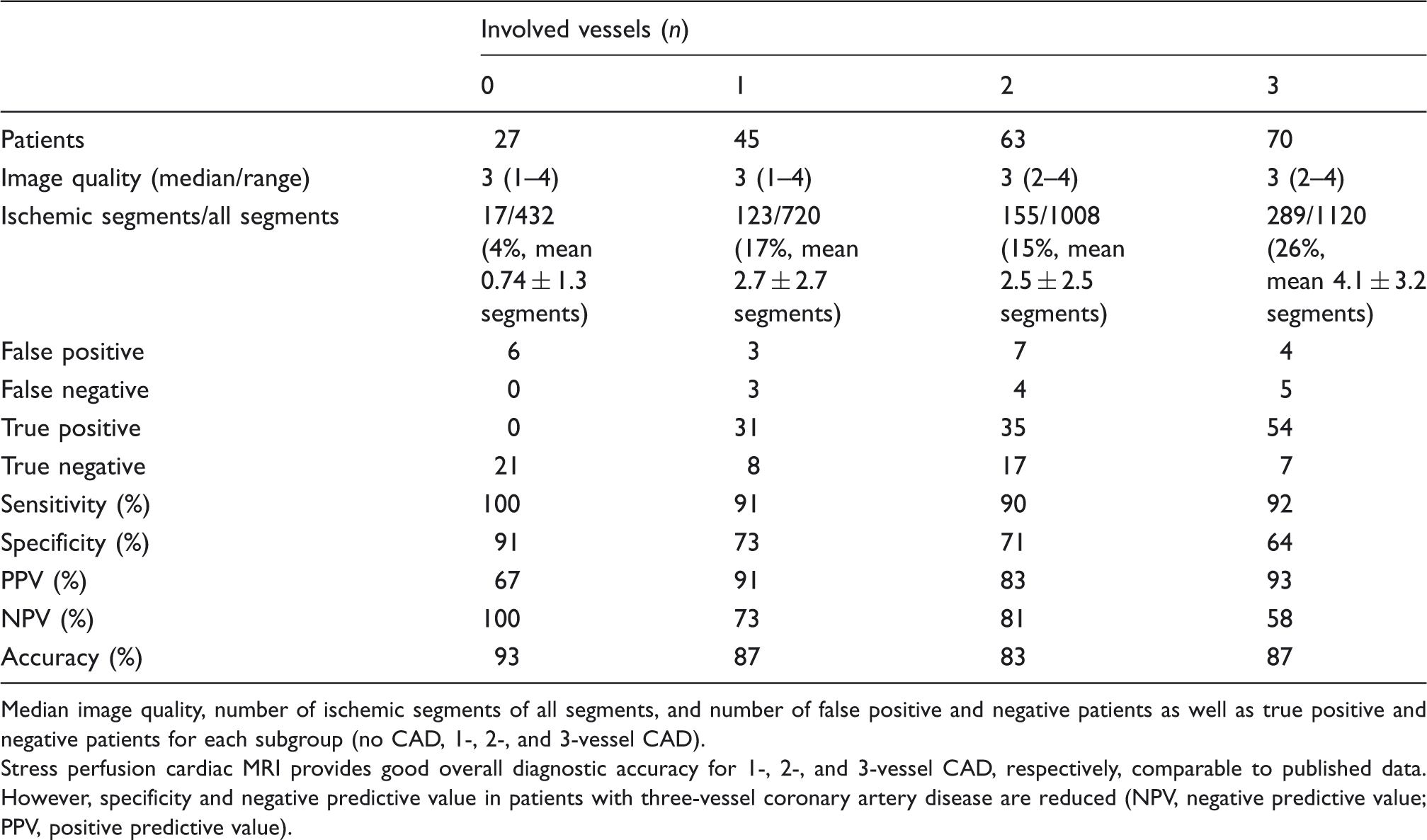
The comparison of the sensitivity and the diagnostic accuracy revealed no significant difference between patients with 3-vessel CAD and patients with no, 1- and 2-vessel CAD (P > 0.05, Figs. 1 and 2). The specificity in patients with 3-vessel CAD was found to be significantly lower compared to patients with no CAD (27%, P < 0.05). The positive predictive value in patients with 3-vessel CAD was found to be significantly higher compared to patients with no CAD (26%, P < 0.05). The negative predictive value in patients with 3-vessel CAD was found to be significantly lower compared to patients with no CAD and 2-vessel CAD (42%/23%, P < 0.05).
Stress-induced ischemia in a patient with 3-vessel CAD. Stress perfusion cardiac MRI in short-axis orientation basal (a), mid ventricular (b), and apical (c) of a 54-year-old patient with exercise-induced chest pain reveal transmural ischemia of the posterior septum basal, almost circular mid-ventricular and anterior to posterior apical indicating severe 3-vessel CAD which was confirmed by coronary angiography.
Explanations for stress-induced ischemia in group 0 were as follows: one patient had a coronary anomaly resulting in ischemia, in three patients modest stenoses were found but not rated as stenosis exceeding 70% at coronary angiography. These patients had to be rated as false positive according to the group definition for statistical criteria, yet symptoms of myocardial ischemia and stress-induced ischemia depicted by SPCMR correlated. Two patients remained false positive without obvious explanation. For statistical analysis those four patients with an adequate explanation for stress-induced ischemia in SPCMR as described above (one myocardial bridge, three correlating stenoses not exceeding 70% at coronary angiography) are regarded as true positive although not in accordance with the group definition. In consequence, the results as given above arise from the patient group definition and not from limitations of SPCMR.
True negative patients in the subgroups with 1-, 2- and 3-vessel CAD were patients with previously known CAD, which were treated in the past with angioplasty and in part with stents, recurring symptoms but no restenosis exceeding 70% in angiography or stress-induced ischemia in MRI.
All false positive patients had multiple coronary artery stenoses between 60% and 70% but no stenosis exceeding 70% in coronary angiography.
Five patients with 3-vessel CAD were classified as false negative. Two of these patients were found to have stenosis between 70% and 75% in coronary angiography. Three remaining patients were found to have high grade stenoses of about 90% in coronary angiograms. One of these could not be identified to have CAD at all by MRI as there were no signs of MI in LGE CMR. The other two patients could at least be identified to have CAD as MI depicted by LGE CMR indicated the presence of hemodynamically relevant stenoses at least in the past although SPCMR could not identify stress-induced ischemia at present.
To confirm response to adenosine stress, heart rate and blood pressure were monitored in all patients before, during and after adenosine stress. Mean heart rate for the complete patient group was at rest 62 and at stress 79 resulting in an increase of 17 bpm. In those five patients with 3-vessel CAD classified as false negative in SPCMR, mean heart rates were 63 bpm at rest and at 80 bpm during stress, resulting in an increase of 17 bpm at stress. Thus a lack of response to adenosine stress could be ruled out as reason for false negative results.
Semi-quantitative analysis in false negative patients with 3-vessel CAD of the qualitative perfusion analysis did not reveal regional hypoperfusion. False negative patients of the qualitative assessment in group 3 (3-vessel CAD) showed significantly reduced MPRI (1.76 ± 0.53) in comparison to that of 2.87 ± 1.26 in true negative patients (group 0, P < 0.05).
Left ventricular function:
Left ventricular function.
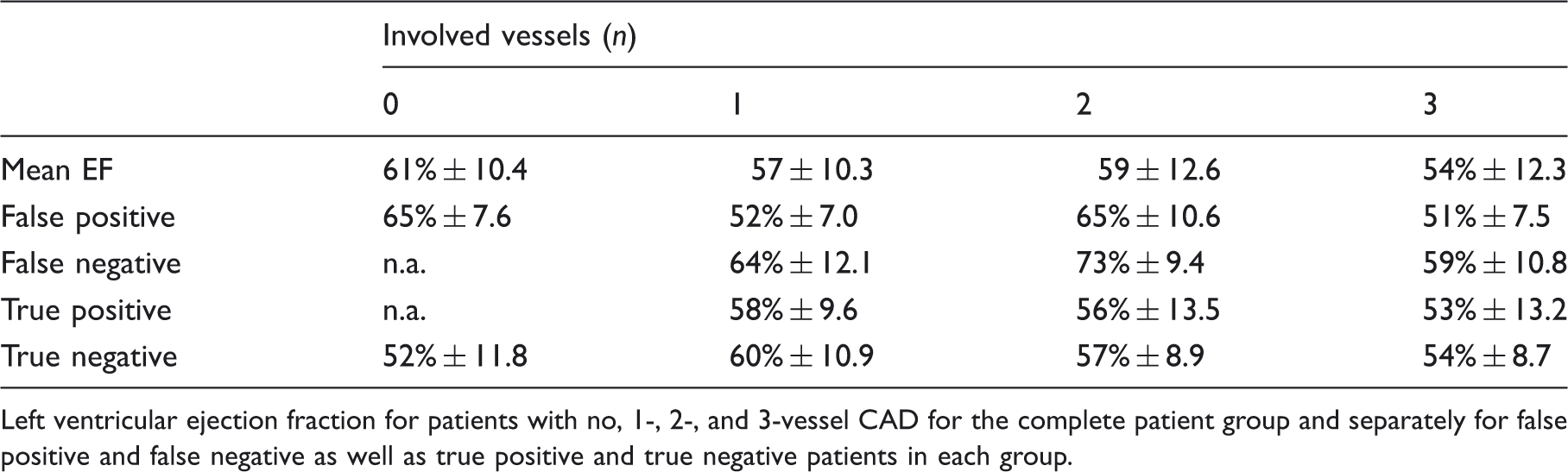
Left ventricular ejection fraction for patients with no, 1-, 2-, and 3-vessel CAD for the complete patient group and separately for false positive and false negative as well as true positive and true negative patients in each group.
Myocardial viability:
Chronic MI was found by late gadolinium enhancement (LGE) cardiac MRI in a considerable percentage of patients in all subgroups with CAD, in which no MI was previously known. The number of patients with chronic MI depicted by LGE images and the number of patients with previously known MI for each group were as follows: group 0, 0/0; group 1, 17 (38%) / 11 (24%); group 2, 31 (49%) / 27 (43%); group 3, 45 (64%) / 24 (34%).
Discussion
In spite of good overall diagnostic accuracy of SPCMR, the diagnostic yield might be restricted in patients with progressed CAD due to global myocardial hypoperfusion. Therefore, our study evaluated, whether patients with 3-vessel CAD could evade detection by SPCMR. Our results suggest that in most patients with 3-vessel CAD, regional hypoperfusion could be detected by SPCMR (Figs. 1 and 2). This correlates with results of recent multicenter studies in which the diagnostic yield of SPCMR in patients with multivessel CAD was not restricted (24,25). However, there are cases with 3-vessel CAD, which were not detected by SPCMR. These are rare and statistically not significant. Yet the possibility has to be considered in patients with intermediate to high pretest probability for CAD and no regional hypoperfusion depicted by SPCMR.
There were several patients our study group who had no myocardial ischemia in spite of stenoses of 70–75%. Collateralization might be the reason for the lack of stress-induced ischemia, so there is an explanation for negative SPCMR in these patients. In three patients with high-grade stenoses (90%) and 3-vessel CAD SPCMR did not reveal regional hypoperfusion. The reason cannot be certainly identified, yet collateralization seems to be improbable, as patients had obvious symptoms of exercise-induced myocardial ischemia and the stenoses found in coronary angiography were severe and multiple. In these patients, negative SPCMR might be caused by the lack of relative regional hypoperfusion at stress due to globally restricted myocardial perfusion. Semi-quantitative analysis of myocardial perfusion did not indicate regional hypoperfusion as well but generally reduced myocardial perfusion reserve indices in all segments. In the case of normal myocardial perfusion a three- to five-fold increase of myocardial blood flow could be expected which was also confirmed for quantitative analysis using SPCMR in healthy volunteers (18,26). The assumption of globally impaired myocardial perfusion is supported by the fact, that the MPRI was significantly reduced at 1.76 ± 0.53 in false negative patients with 3-vessel CAD compared to 2.87 ± 1.26 (P < 0.05) in patients without CAD in our study group (18,19,23).
Yet, most patients with 3-vessel CAD could be identified by qualitative assessment of SPCMR reliably comparable to results of other studies (14,24,25,27). One reason might be that myocardial perfusion remains in spite of multiple stenoses inhomogeneous due to a different degree of stenosis and collateralization (15).
Myocardial perfusion could also be impaired by low left ventricular ejection fraction reducing differences in regional myocardial perfusion. Yet, in our study group no correlation of low left ventricular ejection fraction and false positive results of SPCMR could be found.
Throughout our study population there are patients with moderate stenoses of approximately 70% and negative SPCMR, rated as false negatives, as well as slightly below 70% and positive SPCMR, rated as false positives. However this might not be a restriction of SPCMR but of coronary artery angiography as standard of reference. Coronary angiography assesses the extent of stenosis as percentage of the luminal diameter (28). Yet the correlation of stenosis of the vascular diameter and its hemodynamical effect is not as strict as the cut-off value of 70% suggests as the extent of collateralization and the length and number of stenoses is not considered (29). In false positive patients, also peripheral branch stenoses evading identification by coronary angiography should be taken into consideration, especially in patients with multivessel CAD. These patients might be an indicator of methological restrictions of coronary angiography as standard of reference, as in fact they have myocardial perfusion disorders indicated by SPCMR.
Clinical symptoms, results of SPCMR, and coronary angiography should be carefully correlated in any patient individually when considering myocardial revascularization, as the mere percentage of luminal stenosis reflects its hemodynamically relevance at least in parts of the moderate stenoses only insufficiently (27).
There were several limitations of our study: first, 151 patients were known to have CAD and 62 to have chronic MI, which might cause a bias. Due to clinical symptoms and in many patients also a history of CAD observers might interpret regions with reduced signal intensities on SPCMR more likely as ischemia as well as moderate coronary artery stenoses on angiograms as hemodynamically relevant.
Second, the effect of coronary artery stenoses was not regularly measured by flow wire, to assess its impact on myocardial perfusion and to conclude on its hemodynamic relevance.
Third, the composition of group 0 is inhomogeneous, as it includes patients with coronary artery plaques not classified as manifest CAD in coronary angiography and one patient with stenosis resulting in ischemia due to a myocardial muscle bridge contributing to false positive findings in SPCMR.
Fourth, the number of negative results of SPCMR of group 3 is low as expected. However, this reduces the power of statistical results.
Fifth, the number for each subgroup is limited restricting the statistical power of the results, especially taking in account that negative SPCMR in spite of progressed CAD is a rare phenomenon. Moreover, a significant part of the study group has also MI which results on one hand in a bias in favor of myocardial ischemia and on the other hand influences results of SPCMR as perfusion is restricted in scar tissue but not necessarily associated with stress-induced ischemia in viable myocardium.
In conclusion, the diagnostic value of SPCMR for the detection of stress-induced myocardial ischemia in patients with 3-vessel CAD is not restricted and comparable to patients with 1- and 2-vessel CAD. In rare cases of progressed 3-vessel CAD, there is no obvious circumscribed hypoperfusion visible in a qualitative analysis of the myocardial perfusion possibly due to globally impaired perfusion. Yet, semi-quantitative analysis of the myocardial perfusion allows for identification of these patients due to reduced perfusion parameters compared to patients with no CAD.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.