
Abstract
Background:
A synovial sarcoma arising from the kidney is extremely rare. To date, few data are available on their radiological features.
Purpose:
To identify the computer tomography (CT) imaging findings of primary renal synovial sarcomas (PRSSs).
Material and Methods:
Five cases of PRSS confirmed by histopathological and cytogenetic studies were retrospectively analyzed. All patients had undergone unenhanced and multiphase enhanced CT examinations (one patient underwent CT twice). The CT characteristics, including shape, size, margin, attenuation, and enhancement pattern after intravenous contrast medium injection, were analyzed.
Results:
The study involved two female and three male patients (mean age, 27.4 years; range, 15–43 years). Unenhanced CT showed completely or partly well-defined masses, with heterogeneous (n = 5) or homogeneous (n = 1) patchy low density. On multiphase contrast-enhanced CT, in five of the six CT examinations, the tumors appeared as solid-cystic masses with cyst walls or pseudo-capsules, and demonstrated moderately heterogeneous (n = 5) and/or septate enhancement (n = 2), with a “rapid wash-in and slow wash-out” pattern of enhancement in the solid component. Only one tumor showed a simple cyst appearance and developed an irregular, intratumoral, septate soft density 8 months later. A renal vein and inferior vena cava thrombus was noticed in one patient, while lymphadenopathy was not observed in any patient.
Conclusion:
PRSS should be included in the differential diagnosis when an adolescent or young adult presents with a renal neoplasm appearing as a solid-cystic mass with well-defined borders, a cystic wall or pseudo-capsule, heterogeneous or septate enhancement, a “rapid wash-in and slow wash-out” pattern of enhancement in the solid component, and no sign of lymphadenopathy.
Introduction
Synovial sarcomas are generally deep-seated tumors that most often affect the para-articular regions of the extremities of adolescents and young adults (1,2). They account for about 5–10% of adult soft-tissue sarcomas (1,2). Occasionally, however, synovial sarcomas have been identified in unusual sites such as the thoracic and abdominal wall (3), head and neck region (4), and retroperitoneum (5) as well as in visceral organs such as the lung (6), pleura (7), and prostate (8). Primary renal synovial sarcoma (PRSS) is a rare tumor, which was first described by Faria et al. in 1999 (9). Since its description, fewer than 80 cases of PRSS have been described in the literature, and most of these were case reports (10). Furthermore, only a few studies included a description of the radiologic findings. We, therefore, retrospectively reviewed the computed tomography (CT) findings of five patients with PRSS. To our knowledge, our series is the largest collection of PRSS cases with CT imaging to date.
Material and Methods
Patients
The study protocol was approved by our institutional hospital review board. The records of five consecutive patients with histologically proven PRSS treated in our hospital during 2006–2013 were reviewed. The resection specimens were collected and analyzed at a central pathology laboratory. The definitive diagnosis was based on histological and immunohistochemical evaluations. All medical records, including the history of the disease, imaging studies, and surgical and pathological data, were retrieved for all five patients.
Imaging protocol
CT had been performed at least once in all five patients and twice in one patient (Case 1). CT imaging was performed using two 16-slice spiral CT scanners (Brilliance™ 16, Philips Medical Systems, Best, The Netherlands, n = 4; LightSpeed 16, GE HealthCare, Milwaukee, WI, USA, n = 2). The imaging parameters were as follows: section thickness reconstructions, 5–8 mm; field of view, 23 cm; voltage, 120 kV; current, 200–300 mA; and matrix, 256 × 256. For contrast-enhanced CT, an intravenous bolus dose of 80–100 mL non-ionic iodinated contrast agent (Iopromide; Ultravist; Schering Shanghai, China) was administered at a rate of 2.5–3.0 mL/s to the patients. Contrast-enhanced CT examinations, including arterial-, venous-, and delayed-phase CT, were performed after the initiation of intravenous contrast medium injection, and acquired after a delay of 30–45, 60–90, and 150–200 s, respectively.
Imaging review
Two experienced radiologists specializing in diagnostic imaging of the abdomen reviewed the CT characteristics of each lesion, including the location, shape, size, margins, and attenuation of the unenhanced and contrast-enhanced lesions. If needed, raw images reconstructed at 5–8-mm section thickness were transferred to an independent workstation, and multiplanar reconstruction or curved planar reconstruction was obtained so as to clearly demonstrate the lesions. In the unenhanced CT images, attenuation was classified as low, moderate, or high with respect to the adjacent tissues. Similarly, on contrast-enhanced CT images, the degree of enhancement was classified as none, mild, moderate, or marked. The pattern of enhancement after intravenous contrast medium injection together with the tumor-spread patterns (including nephric and perinephric changes) was also evaluated. The results of imaging review were followed by final decisions, made by consensus by both reviewers.
Results
Clinical data
The study group included two women and three men, with a mean age of 27.4 years (range, 15–43 years). Four of the five patients were symptomatic, and included lower back pain (n = 3), hematuria (n = 2), and nausea and vomiting (n = 1). Results of routine laboratory tests, including complete blood count, serum glucose, electrolytes, and renal function tests, revealed no significant abnormalities in any of the patients.
CT findings
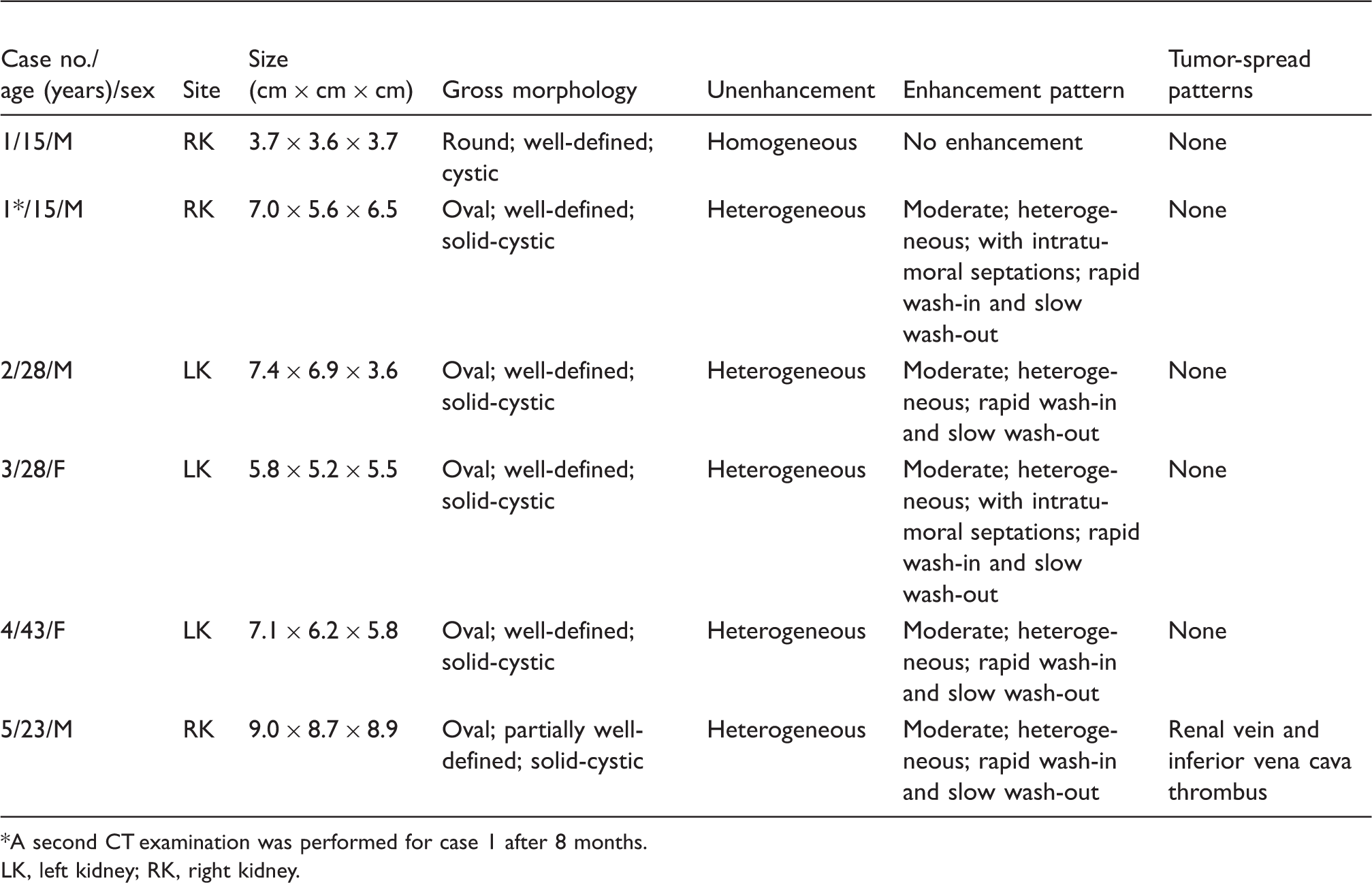
The CT imaging findings from the five cases are summarized in Table 1. The five patients had a total of five tumors with six CT examinations. On five unenhanced CT, the tumors presented as a heterogeneous soft-tissue mass with multiple, patchy, low-attenuating areas (Figs. 1b, 2a, and 3a). The density of the solid component was slightly higher than that of the normal renal parenchyma (by approximately 5–15 HU). Small punctuate calcifications were noted in two lesions. On the remaining unenhanced CT, the tumor (Case 1, Fig. 1a) showed a homogeneous low density (approximately 20–25 HU). This tumor was initially misdiagnosed as a benign simple cyst and a follow-up was recommended within 12 months. Unfortunately, it developed into a soft-tissue density mass with irregular intratumoral septations as showed in the second CT examination 8 months later (Fig. 1b).
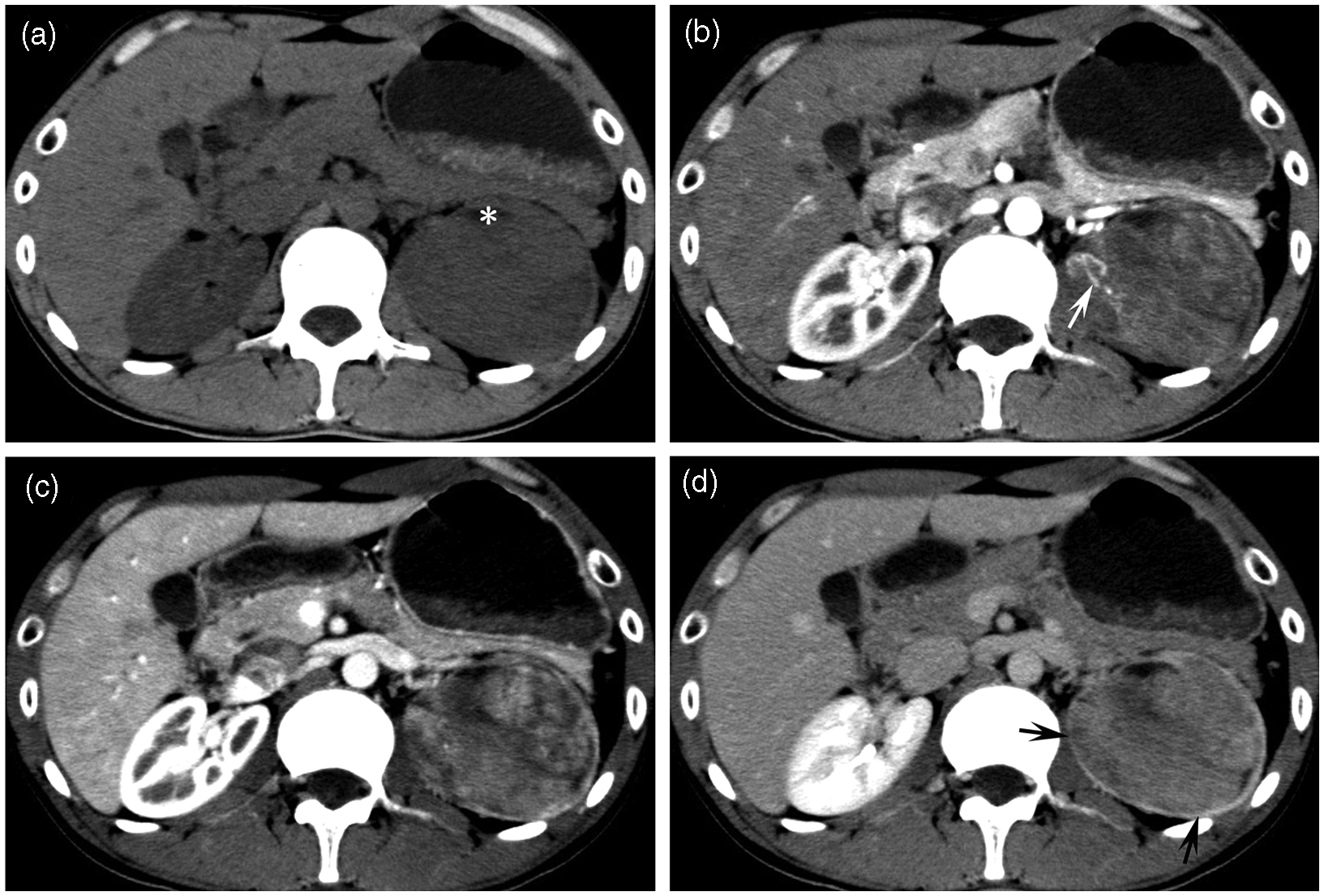
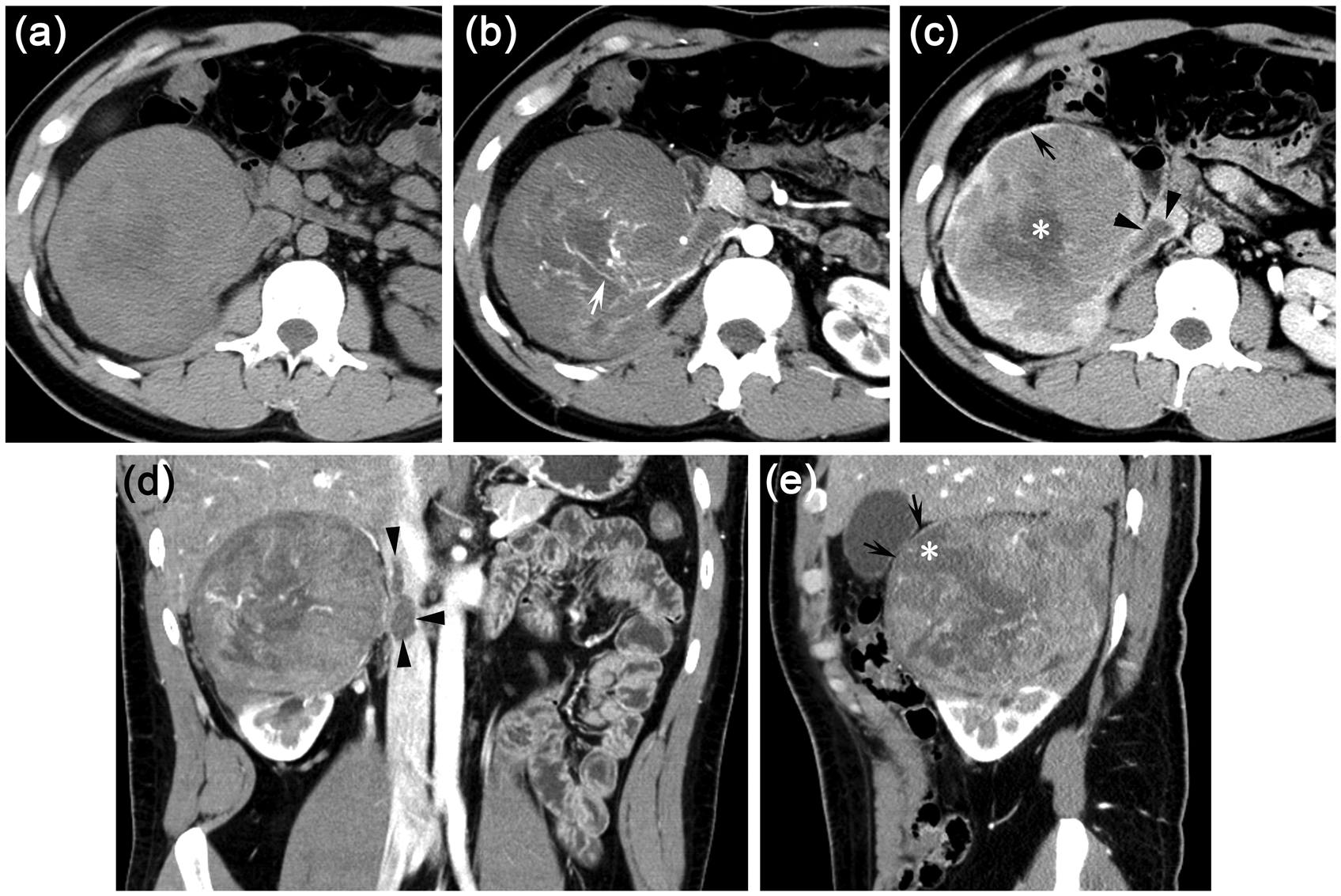
Case 1. A 15-year-old boy with dull pain in the lower back since 1 month. Multiphase CT images (a) showed a non-enhancing, round, cystic lesion measuring 3.7 × 3.6 × 3.7 cm3 (white star) in the right kidney, with homogeneous density and distinct margins. Eight months later, CT images (b, c) revealed multiple patchy low-attenuating areas suggestive of cysts (white star) and irregular intratumoral septates. Soft-tissue component (white arrows) with a “rapid wash-in and slow wash-out” pattern of enhancement. Histological examination (d) (hematoxylin and eosin, 40 × and 200 × [lower left corner]) showed that the tumor comprised fusiform, round, or oval cells arranged in solid sheets or fascicles, and gland-like and cyst-like structures composed of cylindrical cuboidal cells (black stars). Case 2. A 28-year-old man with pain in the lower back pain and hematuria since 3 months. Unenhanced CT imaging (a) showed a well-defined and heterogeneous solid mass involving the central portion of the left kidney and a peripheral, patchy, low-attenuating area within the mass (white star). Enhanced multiphase CT images (b–d) revealed twisted and tortuous vessels on arterial-phase images (white arrow), a “rapid wash-in and slow wash-out” pattern of enhancement in the solid component, and a pseudo-capsule formed by compression of the adjacent renal parenchyma (black arrows). Case 5. A 23-year-old man with nausea and vomiting since 10 days. Unenhanced CT imaging (a) showed a partially ill-defined, solid mass involving the right kidney with multiple, intratumoral, patchy areas of low attenuation. Enhanced CT images (b–e) revealed moderately heterogeneous enhancement in the tumor, accompanied by twisted and tortuous vessels on arterial phase images (white arrow), multiple cystic areas (white stars), pseudo-capsule formed by compression of the adjacent renal parenchyma (black arrows), and a renal vein and inferior vena cava thrombus (black arrowheads). CT findings of five cases of primary renal synovial sarcoma. A second CT examination was performed for case 1 after 8 months. LK, left kidney; RK, right kidney.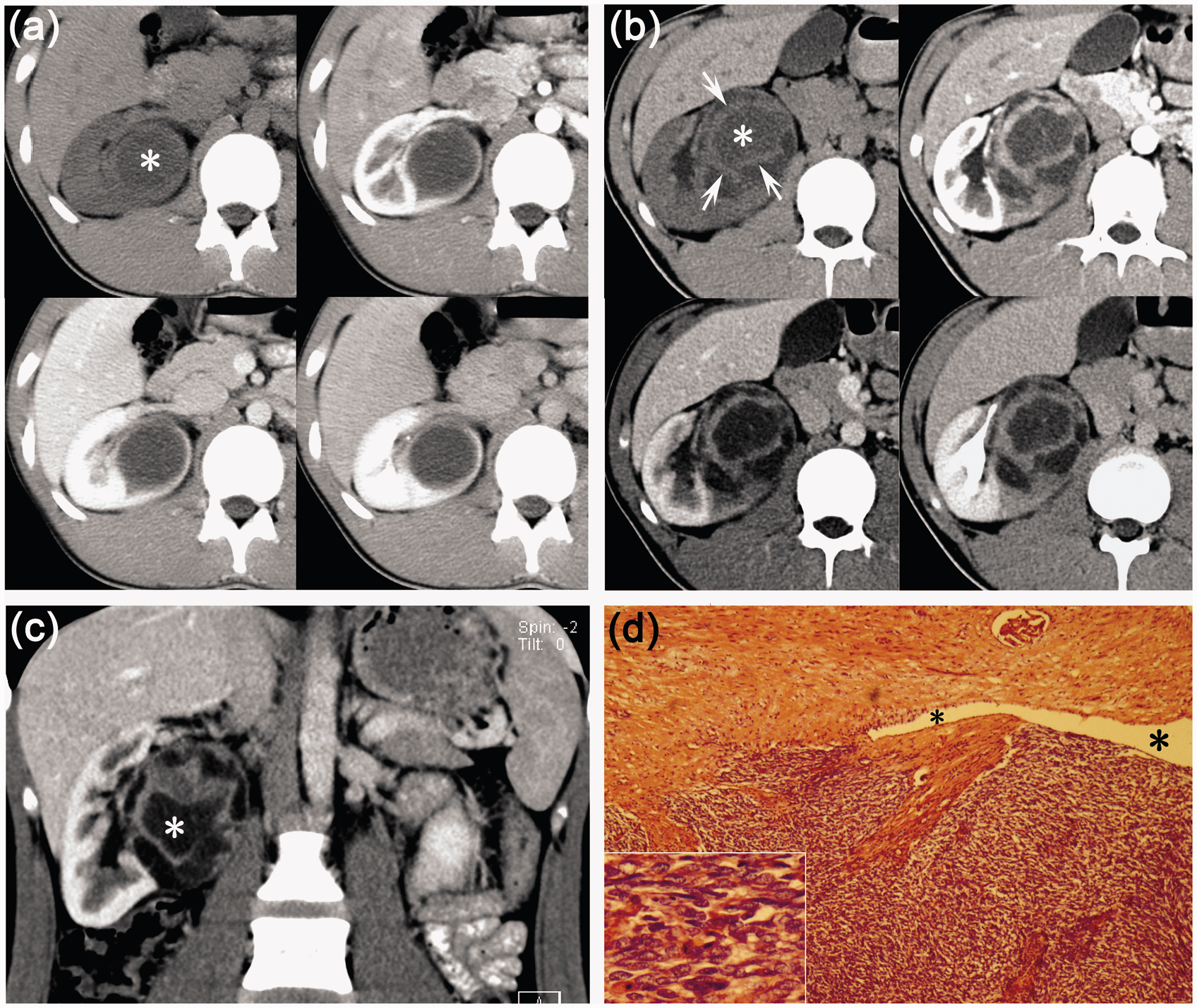
On contrast-enhanced CT images, all tumors appeared as solid-cystic (n = 5, Figs. 1b, 1c, 2b–d, and 3b–e) or cystic lesions (n = 1, Fig. 1a), with the cystic areas ranging from several millimeters to several centimeters. In five of the six CT examinations, the tumors showed moderately heterogeneous enhancement (n = 5, Figs. 1b, 1c, 2b–d, and 3b–e) and/or septate enhancement (n = 2, Fig. 1b–c); the remaining cystic lesion (Fig. 1a) showed no enhancement. The density values of the solid components in the five masses were 56–77 HU, 65–104 HU, and 62–95 HU on arterial, venous, and delayed phase images, respectively. These solid components demonstrated a “rapid wash-in and slow wash-out” pattern of enhancement (Figs. 1b and 2b–d). Twisted and tortuous blood vessels supplying the lesions were noted on the arterial-phase images of two tumors (Figs. 2b and 3b). The tumors had even or uneven cystic walls (n = 3; Fig. 1a–c) or a pseudo-capsule (n = 3; Figs. 2b, 3c and e) formed by compression of the adjacent renal parenchyma. The border between the tumor and normal kidney was distinct in five lesions (Figs. 1a–c and 2), and partially indistinct, infiltrative, and accompanied with renal vein and inferior vena cava thrombus (Fig. 3c and d) in one lesion. No enlarged retroperitoneal lymph nodes were detected in any of the patients.
Pathology findings
All resected tumors were round and well-defined, except for one. Histological examination showed that the tumors comprised fusiform, round, or oval cells arranged in solid sheets or fascicles (Fig. 1d). Multiple focal cystic areas lined by epithelial cells with acidophilic cytoplasm and a hobnail morphology were discernible in the tumors (Fig. 1d). Hemangiopericytoma-like areas, focal hemorrhage, and/or necrosis were detected. Immunohistochemical examination revealed that the tumors were positive for Bcl-2 (n = 5), vimentin (n = 5), CD56 (n = 5), CD99 (n = 5), and EMA (n = 4). Stains for S-100, CD10, CD31, CD34, HHF45, HMB45, HMB54, desmin, and WT-1 were negative in each instance where they were applied. The chromosomal translocation t(X; 18) was detected in all five patients.
Follow-up
Four patients had no distant metastasis, while one patient had a lung metastasis at the time of diagnosis. All five patients underwent surgery followed by chemotherapy. Two patients went into remission during the 10–30-month follow-up period after the surgery. The patient who had lung metastasis at the time of diagnosis died of lung and multiple systemic metastases at 10 months after surgery. Another patient died of lung metastases 24 months after surgery. The remaining patient was lost to follow-up.
Discussion
Synovial sarcoma usually occurs in children and young adults and is located adjacent to joints and tendons in the extremities (1,2). Synovial sarcomas originating in the kidney are extremely rare, and account for only an estimated 1–3% of all malignant neoplasms of the kidney (11). Histologically, PRSSs are further categorized into biphasic, monophasic, and poorly differentiated variants, with the monophasic variant occurring more frequently (10). The pathological findings consist of plump spindle cells with minimal cytoplasm, active mitotic figures, and tubular cells with cysts that are lined by hobnail epithelium (12,13). Immunohistochemical studies of PRSSs have consistently showed positivity for Bcl-2, CD99, CD56, vimentin, and EMA (focal positivity), and negativity for desmin, CD34, and S100 protein (9,13,14). Genetic analyses have demonstrated that PRSSs are characterized by the specific translocation t(X; 18) (p11; q11) (15). Identification of this mutation is helpful in confirming the diagnosis and in differentiating PRSS from other renal tumors (9,13).
PRSS can present between 13 and 67 years of age (16,17), and the mean age at presentation has been reported as 35–38.5 years (18). These tumors have a slight male predominance (male-to-female ratio, 1–1.7:1) (10,18). In our study, the ages of the patients were in the range of 15–43 years (mean, 27.4 years), and there was a predilection for men, with a male-to-female ratio of 3:2, which is consistent with previous findings. The clinical presentation of our patients was non-specific, and their symptoms resembled those of other primary tumors of the kidney.
Imaging features aid pretreatment diagnosis when a renal tumor is suspected. According to previous reports (19–21), PRSS is frequently seen as a large, well-circumscribed, heterogeneously enhancing, soft-tissue-attenuation mass that may extend into the renal pelvis or the perinephric region. A large number of PRSSs present as a predominantly cystic mass with enhancing septa and solid components, and always have a cyst wall (21–23). The cystic components noted on CT images have been confirmed to be consistent with entrapped dilated renal tubular and in lined with hobnail tubular epithelium at pathological examination (23). In the present series, the PRSS lesions characteristically presented as a completely or partly well-defined, soft-tissue-attenuation mass with many or few cystic changes and a cystic wall or pseudo-capsule. Contrast-enhanced CT revealed moderately heterogeneous enhancement in most lesions (5/6), with two tumors demonstrating intratumoral septations. The above imaging findings are consistent with those of previous reports (19–21).
To our knowledge, the multiphase CT imaging findings of PRSS have not been previously reported. In the present series, the solid component of the tumors showed a “rapid wash-in and slow wash-out” pattern of enhancement during multiphase imaging, which is an unusual manifestation in most common renal tumors. Twisted and tortuous blood vessels supplying the tumors were also noted in two lesions on arterial-phase images. This pattern of dynamic enhancement is thought to correlate with known pathological descriptions: plump spindle cells with high cellular density, hemangiopericytoma-like lesion with thin-walled branching vessels and decreased tumor stroma.
Calcification is a common finding in synovial sarcomas at para-articular sites and can be seen in 30% of lesions (24). However, it is usually not a dominant feature of PRSSs (9,13). In the present series, small punctuate calcifications were observed in only two lesions.
PRSSs often metastasize via the blood and rarely via the lymphatic system (10). Extension into the inferior vena cava thrombus has been reported in three cases in previous studies (25,26), and none of these patients had lymphadenopathy (10). In the present series, a renal vein and inferior vena cava thrombus was noticed in one of the five patients, and no lymphadenopathy was observed in any of the patients, which is consistent with previous reports.
From previously published data, renal synovial sarcomas are believed to have aggressive clinical courses and poor outcomes (10). The median disease-free survival of PRSS patients has been reported to be 33.0 months, and patients who develop metastatic disease have a very poor prognosis, with a median survival of only 6 months (10).
Most PRSSs are preoperatively misdiagnosed as renal cell carcinomas (RCCs) or sarcomas. Cystic changes are also commonly identified in RCCs. However, the cystic regions often located centrally and result in an irregular, peripheral solid component with a “rapid wash-in and wash-out” pattern of dynamic enhancement (20,27). In addition, an RCC with extensive necrosis is the most aggressive form among all malignant renal tumors and may result in metastatic disease or death in up to 40% of cases (28). PRSSs of large size and with a large solid component should be differentiated from other renal sarcomas. It is relatively difficult to differentiate PRSSs from other renal sarcomas without special components such as fat, calcifications, and ossification on the basis of imaging characteristics alone. However, other renal sarcomas most likely demonstrate some common features, including relatively great size, lobulated contour, irregular or indistinct edges, heterogeneous attenuation, and enhancement with central necrotic areas (11).
In conclusion, although rare, PRSSs have some relatively characteristic CT imaging features. This entity should be included in the differential diagnosis when an adolescent or young adult presents with a renal neoplasm appearing as a solid-cystic mass with well-defined borders, a cystic wall or pseudo-capsule, heterogeneous or septate enhancement, a “rapid wash-in and slow wash-out” pattern of enhancement in the solid component, and absence of regional lymphadenopathy.
Footnotes
Funding
This work was supported with funding from the National Nature Science Foundation of China (NSFC) (81071207 and 81271622).