
Abstract
Tuberculosis has still an important impact on public health because it is an important cause of death, particularly in developing countries.
On the other hand recent studies have shown that tuberculosis is again becoming concentrated in big cities of Western Europe, especially among immigrants, drug addicts, poor people, and the homeless, despite progress in reducing national rates of the disease.
Diagnostic imaging is challenging for radiologists because signs of tuberculosis may easily mimic other diseases such as neoplasms or sarcoidosis. Clinical signs and symptoms in affected adults can be non-specific and a high level of pre-test clinical suspicion based on history is fundamental in the diagnostic work-up. Impact of tuberculosis in the world is extremely important considering the high incidence estimated during 2011 that was 8.7 million cases. This article gives a review of imaging patterns of chest tuberculosis as may be detected on conventional radiography and computerized tomography (CT). The main aim is to improve radiologist’s familiarity with the spectrum of imaging features of this disease and facilitate timely diagnosis. Furthermore, we consider the emerging role of alternative methods of imaging, such as magnetic resonance imaging (MRI), that can be helpful and highly accurate for a better definition of some signs of tuberculosis.
Introduction
Tuberculosis is an infectious disease caused by Mycobacterium tuberculosis, a rod-shaped, non-spore-forming, aerobic bacterium, often neutral to Gram’s staining. Pulmonary tuberculosis has been classified into primary and post-primary tuberculosis. Primary tuberculosis occurs in patients not previously exposed to Mycobacterium tuberculosis. Within 2 years after the infection, primary tuberculosis usually results in active disease (1). Post-primary or reactivated tuberculosis occurs in patients who have been previously infected and have developed a certain degree of acquired immunity. Reactivated tuberculosis may result from both endogenous reactivation (more often) and exogenous re-infection (super-infection) (2). The burden of disability and death due to tuberculosis is immense, with an estimated 8.7 million incident cases of tuberculosis in 2011 in the world; among these, about 15% were human immunodeficiency virus (HIV)-positive. There were estimated 170 per 100,000 population rates prevalent cases of tuberculosis in 2011. However, because of insufficient case detection and incomplete notification, reported cases represent only 60% of the total number of new cases. About 60% of cases are in the South-East Asia and Western Pacific regions. The African region has 24% of the world cases, and the highest rates of cases and deaths per capita (3). In the past, primary tuberculosis was considered a childhood disease while post-primary tuberculosis was known as a typical form of adulthood infection. However, despite progress in reducing national rates of the disease in most of the developed countries, it still affects high-risk urban groups such as people who originate from high tuberculosis burden areas of Asia and Africa, homeless people, and people abusing drugs or alcohol. It is therefore important to immediately identify the disease to treat correctly infected patients and prevent it spreading. This is not always an easy task because symptoms of presentation may be subtle and non-specific. Moreover, the radiologic signs of the disease are often misleading. Indeed, tuberculosis may be diagnosed in about 25% of cases initially misinterpreted as lung cancer (4).
Clinical manifestations
The key in diagnosing tuberculosis is a high index of suspicion. Clinical signs and symptoms of pulmonary tuberculosis in adults are often nonspecific, whereas complete absence of symptoms occurs in approximately 5% of adult cases (5). The most frequent respiratory symptom is cough for more than 2 weeks, but also hemoptysis and pleuritic chest pain may be considered classic complaints, while dyspnea may be present in case of extensive lung involvement. Systemic manifestations include low-grade fever, anorexia, fatigue, night sweats, and weight loss that may persist for weeks to months (6). The most common hematologic associated manifestations are high white blood cells count and anemia, both occurring in 10% of patients (7), and raised inflammation indexes. Clinical manifestations of tuberculosis are highly influenced by age and immune status of the infected patient. Diagnosis of tuberculosis in elderly is frequently delayed because classic symptoms rarely occur or may be confused by other chronic diseases. A cryptic presentation with fever of unknown origin, often accompanied by pancytopenia or leukemic reaction, is particularly common (8). The clinical manifestations of tuberculosis in HIV-infected people depend on the severity of their immunosuppression. In people with advanced disease, pulmonary tuberculosis is often accompanied by extra-pulmonary involvement (9).
Imaging findings in primary tuberculosis
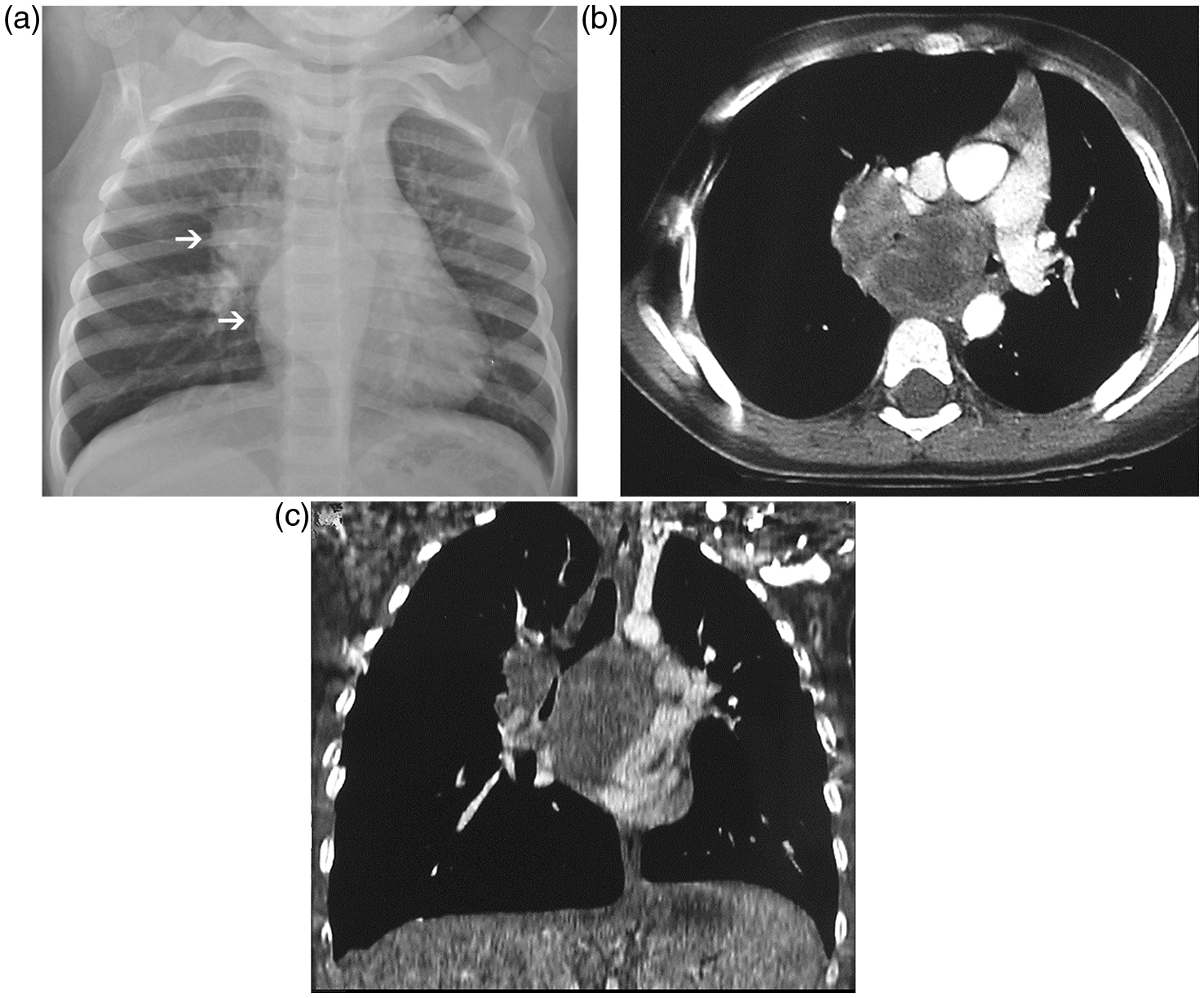
Primary tuberculosis manifests with three main entities: parenchymal disease, lymphadenopathy, and pleural effusion. On chest film, parenchymal disease typically manifests as dense, homogeneous parenchymal consolidation, predominantly located in the middle and lower lobes, especially in adults. Airspace consolidation, related to bronchiolo-alveolar caseous exudate, is usually unilateral and evidenced through radiographs approximately in 70% of children with primary tuberculosis (Fig. 1) (2). At CT studies, the appearance of the parenchymal consolidations in primary tuberculosis is most commonly dense and homogeneous but may also be linear, patchy, nodular, or mass-like (2). In nearly two-thirds of cases, the parenchymal focus resolves without sequelae at conventional radiography; in the remaining cases, the parenchymal focus can calcify, thus initiating the Ghon focus (1). Satellite calcified foci and persistent mass-like opacities, called Tuberculomas, can be found in approximately 9% of patients. Lymph node enlargement is the hallmark of primary tuberculosis in childhood. This condition is encountered in about 95% of children affected by tuberculosis; on the other hand, radiographic evidence of lymph nodes enlargement is far less common in adults (43% of cases) (10,11). Lymphadenopathies are usually unilateral and located in the hilum or para-tracheal regions (Fig. 2a). On computed tomography (CT), which is more sensitive than chest radiography for assessing lymphadenopathy, enlarged nodes typically show central low attenuation, representing caseous necrosis, whereas peripheral rim enhancement represents the vascular rim of the granulomatous inflammatory tissue (12) (Fig. 2b and c). The combination of a Ghon focus and a calcified hilar node is called Ranke Complex and is suggestive of previous tuberculosis infection. Pleural tuberculosis is considered a complication of primary tuberculosis, although in up to 19% of detected cases may occur in association with post-primary disease (13). It is usually unilateral, on the same side as the primary focus, but can also occur in patients without any evidence of parenchymal disease. A bronchopleural fistula must be ruled-out in the diagnosis when an air-fluid level is identified (14). Tuberculous effusions contain high quantity of proteins and often show fibrin strands and septa on thoracic ultrasound imaging (15). Very often septa that have been imaged by ultrasound are not detected by CT. In these cases CT usually shows homogeneous fluid in the pleural cavity, but is more panoramic and therefore more sensitive than plain chest radiography and lung ultrasound in diagnosing associated parenchymal diseases. After contrast administration, pleural layers enhance and are revealed as a smooth thickening of the visceral and parietal pleural surfaces separated by a variable amount of fluid (split pleura sign) (13).
Primary tuberculosis in a small child. Antero-posterior chest X-ray demonstrates homogeneous consolidation with air bronchogram in the right middle lung zone. Source: Courtesy of C Defilippi, Pediatric Hospital Regina Margherita, Turin. (a) Posteroanterior chest X-ray shows tuberculosis manifesting primarily as lymphadenopathies with right hilar and sub-carinal masses (white arrows). Same patient as in Fig. 1. Contrast-enhanced axial (b) and coronal (c) CT scan obtained with mediastinal window setting (same patient as Fig. 1) show enlarged confluent right hilar and subcarinal lymph nodes with peripheral rim enhancement and central low attenuation due to caseous necrosis. Source: Courtesy of C Defilippi, Pediatric Hospital Regina Margherita, Turin.
Imaging findings in reactivation tuberculosis
Reactivation tuberculosis tends to involve predominantly the apical and posterior segments of the upper lobes and the superior segments of the lower lobes. These specific locations are explained by relative higher oxygen tension and impaired lymphatic drainage (16). An atypical distribution of the disease involving the anterior segment of the upper lobes or the lower segment of the basal lobes has been reported in approximately 5% of cases of post-primary tuberculosis (17). In most cases, more than one pulmonary segment may be involved, while bilateral disease is encountered in one-third to two-thirds of patients (18). Cavitation, which is the hallmark of this form of pulmonary tuberculosis, may be evident in half of the patients. The cavitation process may be single or multiple and usually creates a lesion surrounded by thick walls with irregular margins, which may be significantly reduced after treatment (Fig. 3a). In a minority of cases, the cavity may contain a small quantity of fluid, usually visualized as an air-fluid level (19). When the amount of fluid content is significantly high, superinfection by other bacteria should be suspected (20). Bronchogenic spreading of the disease occurs when an area of caseous necrosis liquefies and communicates with the bronchial tree. It is identified radiographically in 20% of post-primary tuberculosis cases as multiple, ill-defined 5–10-mm nodules. These nodules are in a segmental or lobar distribution involving the dependent lung zone, distant from the cavitation process (21). On CT scans, bronchogenic spread can be identified in 95% of patients with post-primary tuberculosis (22). A significant finding on thin-section in CT is the “tree-in-bud” pattern, consisting of 2–4-mm centrilobular nodules and sharply marginated linear branching opacities (23). Tree-in-bud opacities may also be detected in other infections, even if the pattern characterized by a combination of multiple cavitations or nodular opacities in suggestive clinical settings, allows the diagnosis of pulmonary tuberculosis (24) (Fig. 3b). Tuberculoma, defined as a sharply marginated rounded or oval lesion usually measuring in the range of 0.5–4 cm in diameter, is the predominant parenchymal lesion in 3–6% of cases. Tuberculomas are typically solitary lesions, but may be multiple and surrounded by small “satellite” nodules with regular or irregular margins, often containing calcifications (25). Miliary tuberculosis refers to the hematogenous dissemination of tuberculosis. It can occur in both primary and post-primary disease, being somewhat more frequent in reactivation tuberculosis (26). Chest radiography is usually normal at the onset of symptoms, while the typical radiographic findings characterized by diffuse small nodules are seen in 85% of cases during more advanced clinical phases of the disease (Fig. 4a). CT allows accurate early diagnosis when small nodules, typically 1–3 mm in size (Fig. 4b) or macronodules, resulting from fusion of several granulomas, are detected even in asymptomatic patients. Other signs easily detected by high resolution CT (HRCT) are thickening of interlobular septa and fine intralobular networks (27). This latter pattern can be differentiated from the tree-in-bud because the margins of the nodules are well defined and the distribution is uniform, on the contrary the tree-in-bud nodules are poorly defined and have a patchy distribution. The nodules usually resolve within 2–6 months of specific treatment, in most cases without scarring or any calcification (28).
Postprimary pattern of tuberculosis in a 55-year-old woman. (a) Axial CT scan of the upper lobes shows an area of cavitation in the right lung, surrounded by thick walls with irregular margins. (b) Axial CT scan at levels of main bronchi shows centrilobular nodules and mucoid impaction of contiguous branching bronchioles producing a tree-in-bud appearance, which reflects the presence of endobronchial spread. Miliary tuberculosis in a young adult. (a) Detail (apex of the right lung) of postero-anterior chest radiograph shows multiple small nodular areas of increased opacity. (b) High-resolution CT scan with lung windowing at the level of carena demonstrates numerous fine, bilateral, unifom-sized, discrete nodules in a random distribution with associated thickening of interlobular septa and fine intralobular networks.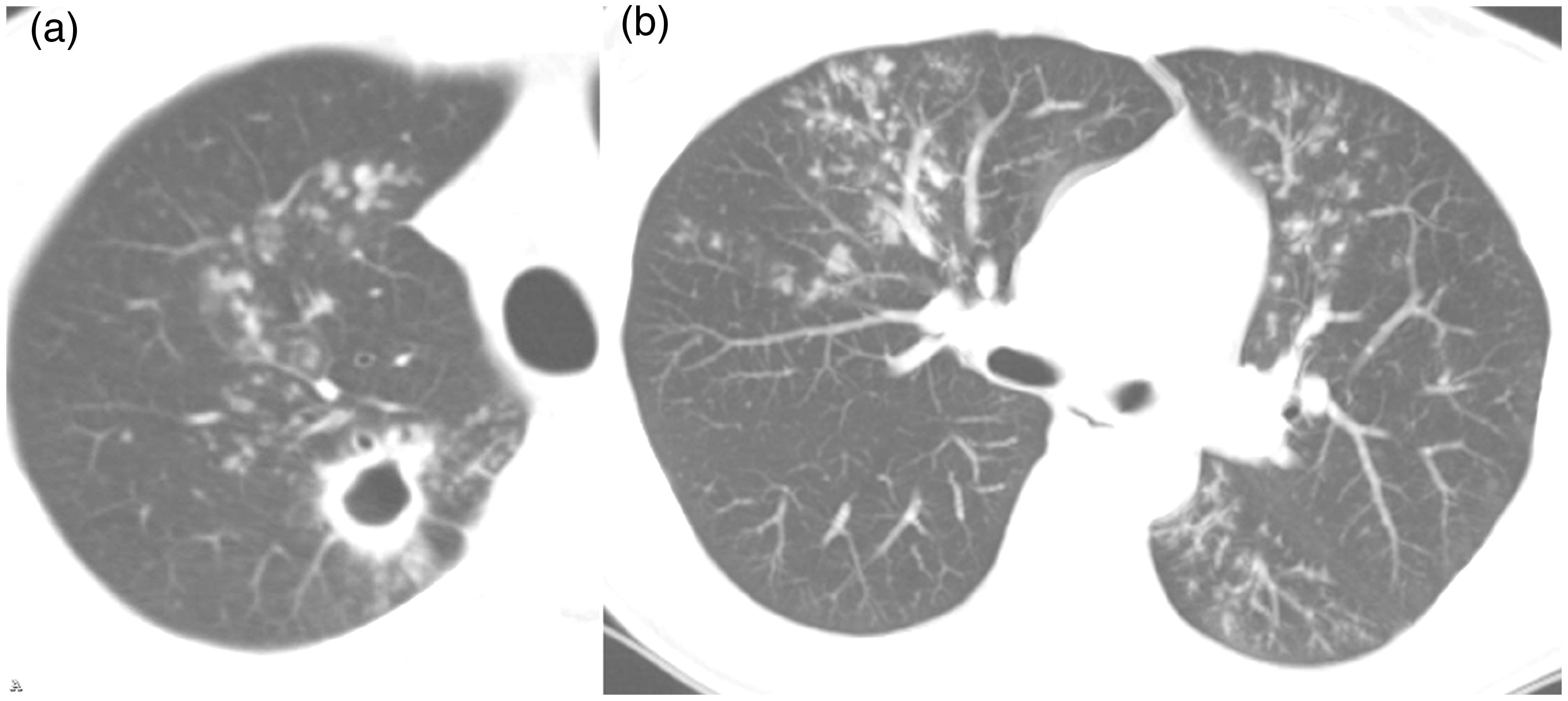

Late complications
Bronchiectasis and residual cavities are sequelae of pulmonary tuberculosis, detected at thin-section CT scans, respectively, in 71–86% and 12–22% of patients with resolved disease. These lesions typically involve the apical or posterior segments of the upper lobes (2). A bronchial dilatation or, more commonly, a residual tuberculous cavity may be colonized by Aspergillus with development of a mycetoma. The typical CT sign consists of an intracavitary mass, usually surrounded by air (the “air crescent sign”) (29) (Fig. 5).
Cavitary tuberculosis associated with aspergilloma in an 83-year-old man. Coronal CT scan shows volume loss of the right upper lobe with dependent soft-tissue aspergilloma within the cavity. Note the air crescent sign (the nodule is separated by a crescent-shaped lucency from the adjacent cavity wall).
Involvement of the tracheobronchial tree is common in the postprimary form and, if not recognized and properly treated, bronchial scar stenosis is a frequent complication that may even lead to obstructive atelectasis, pneumonia and bronchiectasis.
Empyema necessitatis is an uncommon complication of a tuberculous empyema in which the inflammatory mass spontaneously bores into the soft tissues of the thoracic wall, forming a subcutaneous abscess that sometimes opens to the skin (30). The plain chest film shows signs of chronic pleural disease with pleural thickening that may show calcification. CT shows a pleural collection associated with an abscess located at the chest wall level (Fig. 6).
Pleural and chest wall tuberculosis (empyema necessitatis) in a 73-year-old woman. Contrast-enhanced axial CT scan at level of left pulmonary artery using mediastinal window setting shows pleural fluid collection and visceral pleural calcification in right hemithorax, suggesting chronic tuberculous empyema. Lentiform chest wall lesion showing central low attenuation, consistent with focal tuberculous chest wall abscess, is also seen.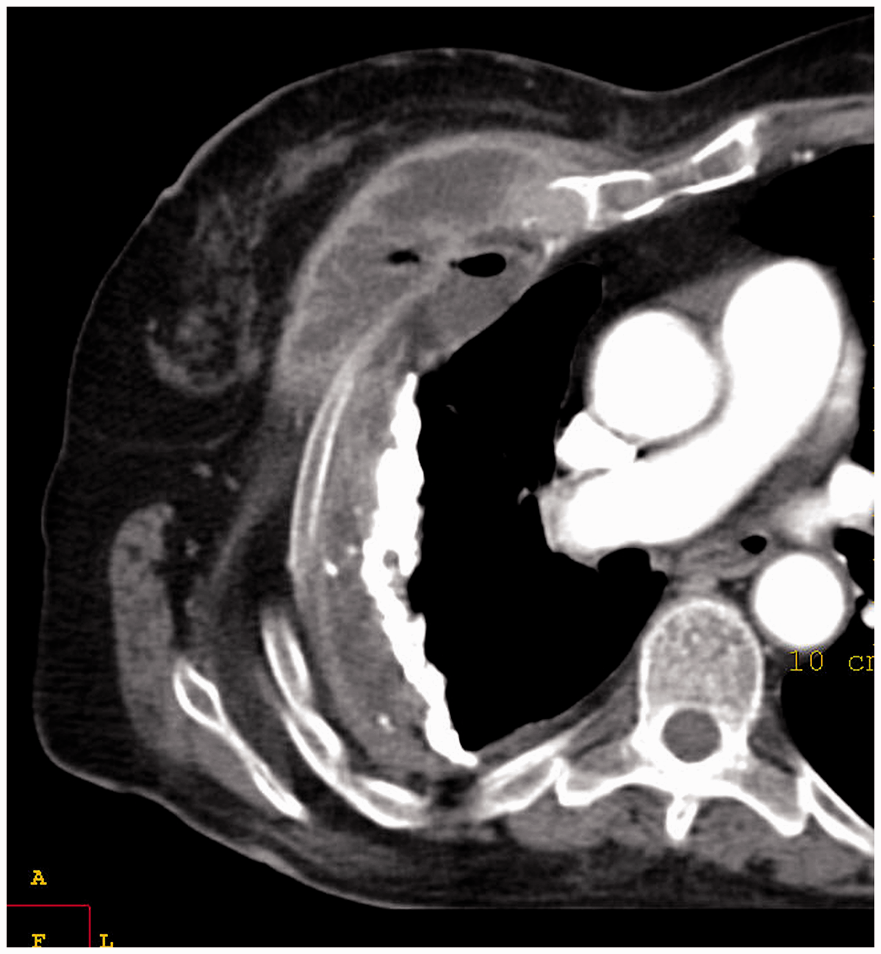
Tuberculosis in immunocompromised hosts
Impairement of the host immunity is a well-known predisposing factor in tuberculosis. Unusual or atypical manifestations are common in immuncompromised patients. For example, diabetic and other immunocompromised patients have a higher prevalence of multiple cavities and frequent non-segmental distribution of the lesions (31). Miliary forms and disseminated disease are also associated with severe immunosuppression (32). Tuberculosis is the first cause of death from opportunistic infections among HIV-infected patients. The radiographic manifestations of HIV-associated to pulmonary tuberculosis depend on the degree of immunosuppression (33). HIV patients with almost preserved cellular immune function show radiographic findings similar to those of non HIV-infected individuals. Patients with a CD4 T-lymphocyte count <200/mm3 have a higher prevalence of mediastinal or hilar lymphadenopathy, frequent nodular or multinodular image pattern with a lower prevalence of cavitations, and often extra-pulmonary involvement as compared with HIV-seropositive patients with a CD4 T-lymphocyte ≥200 mm3 (32).
Emerging role of magnetic resonance imaging (MRI)
Using MRI in the diagnostic management of patients affected by lung tuberculosis is a challenge that may have some advantages but also some disadvantages. Absence of ionizing radiation is obviously a great advantage. However, the small number of signal generating protons, susceptibility artifacts related to the multiple air-tissue interfaces and motion artifacts that require fast imaging or triggering and gating techniques are disadvantages that should always be considered (34). MRI has shown an excellent contrast resolution and appears to be more accurate than non-contrast-enhanced CT in revealing lymph node involvement, pleural abnormalities, and parenchymal caseation (35). Furthermore, signal intensity of lymph nodes may differ depending on the degree of evolution: on T2-weighted fast recovery fast spin-echo (FR FSE T2) FAT SAT sequence slight hyperintensity may indicate flogistic lymphoid hyperplasia, high hyperintensity is suggestive of liquefactive necrosis and central isointensity associated to peripheral hyper-intensity may indicate caseosis (36). Excellent contrast resolution makes MRI superior to CT in assessing pleural involvement in case of subtle or loculated effusions, not seen on CT (37). MRI can therefore be considered as an interesting alternative to CT in subgroups of patients such as children or pregnant women.
Radiological differential diagnosis
The differential diagnosis between tuberculosis and some associated pathologic conditions is an emerging problem, as pulmonary tuberculosis may easily reveal aspects that can create diagnostic doubts in the radiologic imaging studies. Differential diagnosis can be particularly challenging when tuberculosis mimicks sarcoidosis, lymphoma, and pulmonary neoplasms (Fig. 7). Changes in epidemiology characteristics of the disease can be one of the causes of difficulties in the differential diagnosis. While in the past primary tuberculosis was mainly a pediatric disease, nowadays it is more common in young adults (age 18–25 years). The differential diagnosis with systemic diseases such as sarcoidosis, Hodgkin’s lymphoma (HL), and some respiratory viral conditions, on occasion may represent a real challenge for the radiologist and the clinician. Indeed morphologic findings of these diseases are characterized by the presence of pathological hilar and mediastinal homogeneous enhancing lymph nodes that can be hardly differentiated from tuberculosis manifestations. On the other hand, lymphadenopathies in tuberculosis show a heterogeneous enhancement with rim-enhancing and central low attenuation that may be considered highly specific (38). However, these findings are not fully pathognomonic and, especially in cases of tuberculosis without parenchymal lesions, lymphonodal biopsy is the only way to reach a reliable diagnosis. If primary tuberculosis is more common among young adults, post-primary tuberculosis is more common among adults. Post-primary tuberculosis findings often determine a further differential diagnostic problem with solid neoplasms, giving isolated opacities on chest radiography or CT scan accompanied by negative sputum.
(a) Coronal CT scan of a central mass with surrounding locoregional lymph nodes suspected to be a pulmonary neoplasm but which was established to be tuberculosis. (b) Axial CT scan showing narrowed apical bronchus and surrounding mediastinal lymph nodes. (c) Axial CT scan showing a pulmonary peripheral tubercular lesion characterized by spiculated margins, in differential diagnosis with peripheral adenocarcinoma.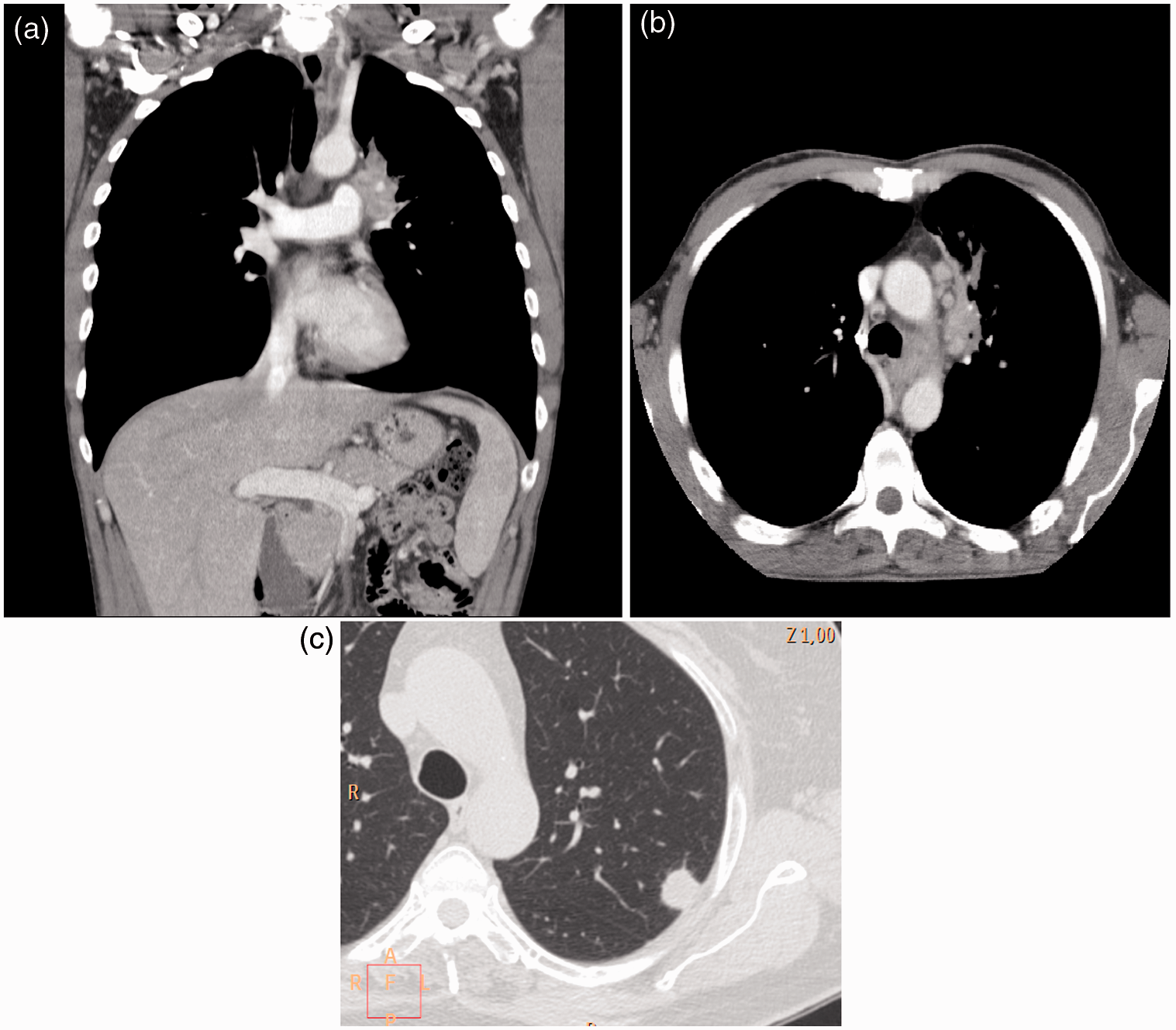
Indeed, the presence of acid fast bacilli in sputum or a positive skin test do not rule out the co-existence of tuberculosis and cancer. CT imaging is helpful for the accurate evaluation of the morphologic and densitometric aspects of the lesion, detection of lymph nodes enlargement, and the possible presence of metastases. Diffuse, central, or lamellar calcifications may be clues to the imaging diagnosis of tuberculosis over malignancy. Positron emission tomography CT (PET-CT) could be another useful tool in case of a challenging differential diagnosis, however, tuberculosis still remains a frequent cause of false-positive diagnoses on PET-CT because tuberculomas may even show hypermetabolic pattern on F18-FDG-PET raising problems of overlapping findings with tumor masses. Surgery or biopsy may occasionally be the only solution to obtain a correct diagnosis (39).
Response to treatment and “imaging healing” concept
Complete recovery of parenchymal abnormalities usually require from 6 months to 2 years on radiographs and up to 15 months on CT scans (28). Lymphadenopathies may persist for several years after treatment. However, absence of improvement of radiological findings after 3 months of chemotherapy in adults, suggest infection by drug-resistant organisms or a superimposed process (40). Imaging findings of multi-drug resistant tuberculosis do not basically differ from those of drug-sensitive tuberculosis, although the mode of acquisition of drug-resistance seems to influence the aspect of the radiologic pattern in multi-drug resistant tuberculosis. Patients, who show resistance without having been previously submitted to anti-tuberculosis chemotherapy or having performed a therapy cycle of less than 1 month, are considered to have primary drug resistance and usually present with a non-cavitary consolidation, pleural effusion, and a primary tuberculosis pattern. On the other hand, patients who acquire multi-drug resistant tuberculosis after a wrong chemotherapy treatment lasting more than 1 month often show cavitation, consolidation, and a reactivation pattern of the disease (40). Differentiation between active and inactive tuberculosis based on radiologic findings is reliable only when the temporal evolution of the disease is considered. According to the American Tuberculosis Association, it is required a detailed observation during the time course of at least 6 months to judge the stability. Other criteria derive from densitometric and morphological features of the lesion. CT patterns suggesting active disease are parenchymal consolidations, areas of ground-glass attenuation, endobronchial spread (centrilobular branching linear opacities, the tree-in-bud sign), miliary pattern, and cavitations.
Conclusions
Although a slow reduction in the incidence of tuberculosis has been reported in developed countries, tuberculosis is still a major challenge on the list of the most serious infectious diseases in the world, even in the 21st century. Chest radiography is the mainstay in the radiological evaluation of suspected or proven pulmonary tuberculosis. CT is useful in the clarification of certain misleading findings and may also be helpful in the determination of disease activity. Nowadays, the radiological presentation of tuberculosis is changing, with fading of the classical distinction between primary and post-primary disease. The traditional imaging concept of primary and reactivation tuberculosis has recently been challenged on the basis of DNA fingerprints, and radiologic features depend on the level of host immunity rather than the elapsed time after the infection. Radiologists must be aware also that new forms of the diseases may present and should be prepared for their prompt recognition, thus helping to avoid a delayed treatment, which is associated with high rates of mortality.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.