
Abstract
Background
Further development established hand-carried ultrasound (HCU) imagers in daily clinical workflow providing several advantages such as fast bedside availability and prompt diagnosis.
Purpose
To evaluate the diagnostic yield of a latest generation HCU imager compared to chest radiography (CR) for the detection of pleural effusion (PE) in intensive care patients.
Material and Methods
Forty-eight hemithoraces of 24 patients on surgical intensive care units were enrolled in this study. All hemithoraces were evaluated using both HCU and CR. Definite diagnosis of PE was achieved using a high-end ultrasound system as standard of reference. Statistical analysis was performed using 2 × 2 tables and a McNemar test. A P value of <0.05 was considered statistically significant.
Results
PE was present in 35 of 48 hemithoraces (73%). The HCU examination was carried out technically successfully in all hemithoraces. Sensitivity and specificity of HCU for the diagnosis of PE was 91% and 100%, respectively, whereas sensitivity and specificity of CR was 74% and 31%, respectively. The difference between HCU and CR was statistically significant with respect to specificity but not sensitivity (P = 0.008 and P = 0.11, respectively).
Conclusion
Due to its ease of use and its high diagnostic yield HCU systems of the latest generation constitute a helpful technique for the primary assessment of PE.
In patients being treated in intensive care units pleural effusion (PE) is a common complication (1). Usually the diagnosis of pleural effusion is based on physical examination and chest radiography. However, the diagnostic accuracy of physical examination is low, even when performed by experienced operators (2). Furthermore chest radiography may underestimate the amount of pleural effusion, in particular when the image is taken in a sitting or supine position. A minimum of 200 mL of pleural fluid is necessary to detect costophrenic obliteration in posteroanterior radiographs, but up to 500 mL of pleural fluid can be present without detectable costophrenic obliteration in some cases (3). In the supine position more than 500 mL of pleural fluid must be present to be detectable in chest radiographs (4).
Chest ultrasound is a useful and non-invasive tool for the evaluation of PE as shown by prior studies (5). Ultrasound can even reveal very small amounts of pleural fluid, as little as 3–5 mL (6). Additionally thoracentesis can be performed under ultrasound guidance (7, 8). Further advantages of chest ultrasound are low costs, lack of radiation exposure, and user-friendliness.
Further development generated miniaturized ultrasound systems leading to an introduction of hand-carried ultrasound (HCU) imagers in daily clinical workflow. The major advantage of these devices is a fast bedside availability allowing prompt diagnosis and immediate therapeutic measures (9).
In the present study we evaluated the diagnostic yield of a latest generation HCU imager in comparison to chest radiography for the recognition of PE in intensive care patients.
Material and Methods
Patients
On two consecutive days all 24 patients (48 hemithoraces) on a cardiothoracic and general surgical intensive care unit for whom a supine chest radiograph was ordered by the ward physician were additionally examined with both hand-carried and high-end ultrasound. Patients were enrolled in this study irrespective of their underlying disease. There was no exclusion criterion. The study operators (SS, CD, FP) who carried out the ultrasound examination and the reading of the chest radiographs were unaware of the indication for the supine chest radiograph and the patients' underlying disease. The patients' basic demographic data are shown in Table 1. Written informed consent was obtained from all patients and the study was approved by the institutional ethics committee.
Basic demographic characteristics of all enrolled patients including frequency and type of surgery
Chest radiography
Indications for supine chest radiography were clinical signs of cardiac decompensation, clinically suspected pneumonia, PE or atelectasis and the exclusion of a pneumothorax after central vein catheterization in six, five, five, four, and four patients, respectively. All radiographs were acquired on the intensive care units using a mobile X-ray device (Mobilett XP ECO, Siemens Healthcare, Erlangen, Germany). All chest radiographs were evaluated for the presence of PE by the same radiologist (FP), who had specialized in cardiopulmonary imaging for 4 years and who was unaware of the ultrasound results. All chest radiographs were included and each hemithorax was scored separately.
Chest examination with hand-carried ultrasound
The HCU examination was carried out using a latest generation device (VScan, GE Healthcare, Waukesha, WI, USA) with a plane 1.7–3.8 MHz transducer for two-dimensional imaging and a 3.5-inch color LCD-display The probe measures 120 × 33 × 26 mm. The weight of this device is 390 g. The total scan time is approximately 62 min with fully-charged batteries. A picture of the HCU device is shown in Fig. 1. The chest ultrasound examination with the HCU imager was performed within a maximum of 3 h after the acquisition of supine chest radiograph. The operator (SS) was unaware of the results of both chest radiography and high-end ultrasound.

Image of the study hand-carried ultrasound device (VScan, GE Healthcare, Waukesha WI, USA) with kind permission of Mr Bastian Werminghoff (GE Healthcare Germany, Munich, Germany)
Chest examination with high-end ultrasound
Chest examination with the high-end ultrasound system (LOGIQ E9, GE Healthcare, Waukesha, WI, USA) with a curved-array 1–5 MHz transducer was carried out as standard of reference for the assessment of pleural effusion. The operator (CD) was unaware of the findings of both chest radiography and HCU. The chest ultrasonography with the high-end ultrasound system was performed within a maximum of 15 min after the HCU examination.
Technique of ultrasound
In order to standardize and simplify the ultrasound examinations all patients were examined lying in their beds in intensive care units. In particular, none of the patients was moved for the examination with the HCU or high-end ultrasound system. Both hemithoraces were examined without modifications of the patients' breathing frequency. The intercostal spaces were used us ultrasound windows. In all hemithoraces at least two intercostal ultrasound windows were employed to scan the dorsal and lateral aspects of the basal pleural space for the presence of PE. A PE was diagnosed when an anechoic space between the parietal pleura and the highly reflective visceral pleura-lung interface was present (9). An echoic space between the parietal pleura and the highly reflective visceral pleura-lung interface was considered to represent severe complications such as empyema or hemothorax. Neither thoracentesis nor other interventions that could have influenced the amount of pleural effusion were performed between the acquisition of the chest radiograph and the acquisition of the HCU and high-end ultrasound examination.
Statistical analysis
Data were collected using Excel tables (Excel 2007, Microsoft, Redmond, WA, USA). Statistical analysis was performed using PASW 18 (PASW v. 18, IBM SPSS, Inc., Armonk, NY, USA). Agreement between the findings of hand-carried ultrasound or chest radiography and the definite diagnosis generated by high-end ultrasound was assessed from 2 × 2 tables. Comparison of sensitivity and specificity between hand-carried ultrasound and chest radiography was made using the McNemar test. A P value of < 0.05 was considered statistically significant.
Results
Chest ultrasound with the high-end ultrasound system, the standard of reference, depicted PE in 21 of 24 patients (87.5%) and in 35 of 48 hemithoraces (73%). Bilateral PE was found in 14 of 24 patients (58%), whereas unilateral pleural fluid on the right or left side was present in three patients (13%) and four patients (17%), respectively.
HCU was carried out technically successfully in all 24 patients and in all 48 hemithoraces. In the operator's experience the employed HCU system exhibited convenient handling, including: (a) quick availability with a boot time of less than 20 s; (b) comfortable scanning of the hemithoraces of the lying patients with the small plane transducer; (c) clear reading of the images on the 3.5-inch color LCD display; as well as (d) easy storage of patient data and ultrasound images. Mean scanning time of the HCU examination was 1.5 min with a range of 1–3 min. Examination with HCU revealed pleural effusion correctly in 32 out of 35 hemithoraces and showed no false-positive results. Thus, sensitivity and specificity were 91% and 100%, respectively. In the remaining three cases where HCU examination showed false-negative results the amount of PE that was identified by the high-end ultrasound system was estimated to be less than 50 mL. The weight of the three patients with false-negative findings (96, 115, and 122 kg, respectively) was in the upper range of all 24 patients (median weight 86 kg). Positive and negative predictive value for the diagnosis of PE with HCU was 100% and 82%, respectively.
Chest radiography diagnosed PE correctly in 26 of 35 hemithoraces and was false-positive in nine out of 48 hemithoraces. Hence, sensitivity, specificity, positive and negative predictive value for the diagnosis of PE with chest radiography were 74%, 31%, 73%, and 32%, respectively.
Sensitivity of HCU (91%) was superior to sensitivity of chest radiography (74%) but the difference was statistically not significant (P = 0.11). Specificity of HCU (100%) was higher than the specificity of chest radiography (31%) and the difference was statistically significant (P = 0.008).
The results of sensitivity and specificity of HCU and chest radiography are summarized in Table 2.
Sensitivity, specificity, positive and negative predictive value for the diagnosis of pleural effusion using hand-carried ultrasound and chest radiography with high-end ultrasound as standard of reference
Figs. 2 and 3 demonstrate examples of incongruent and congruent findings of HCU and chest radiography in patients with PE.
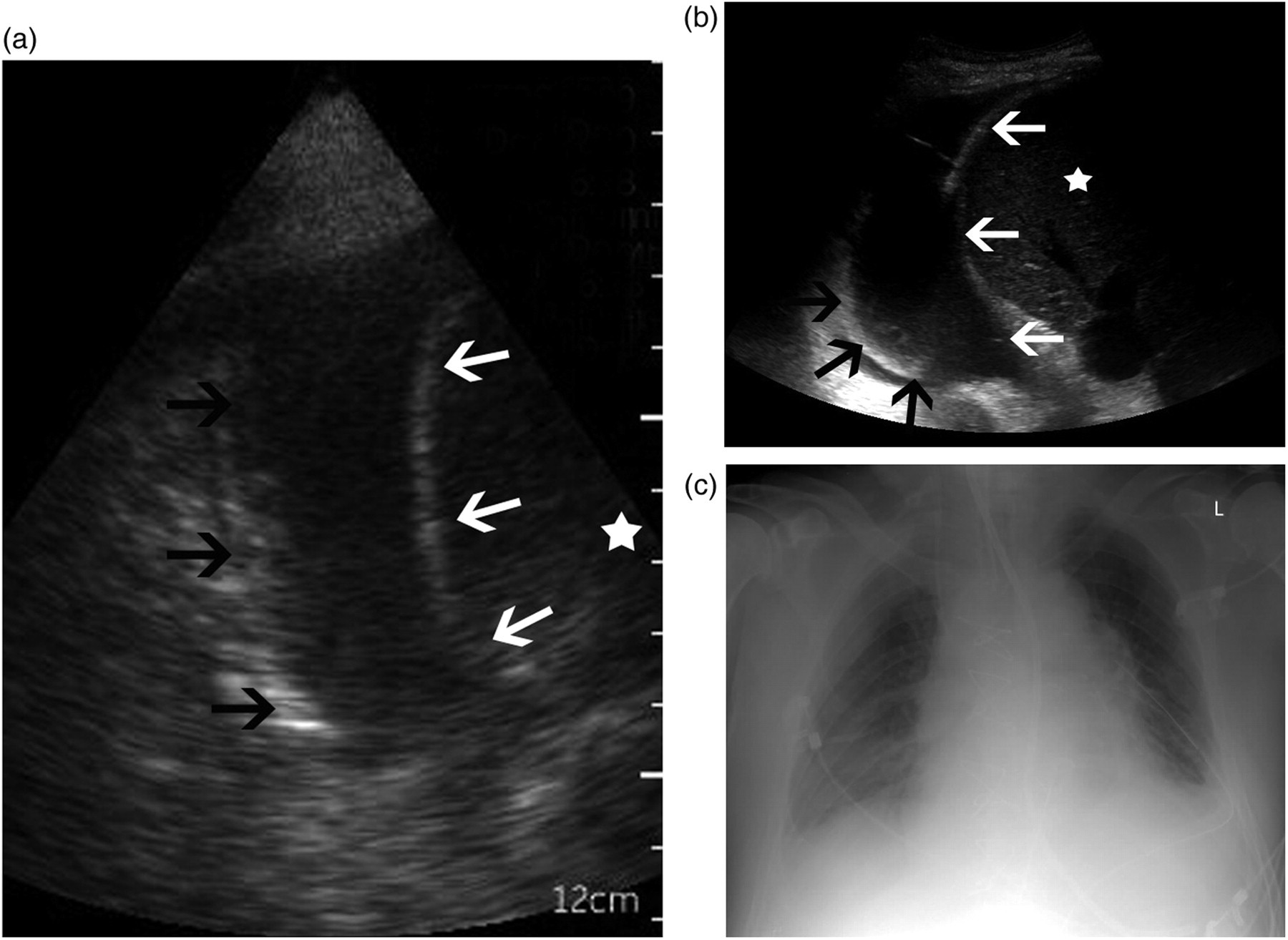
Incongruent findings of hand-carried ultrasound and chest radiograph in an 83-year-old male patient for whom a chest radiograph was carried out for the diagnostic workup of pneumonia 4 days after coronary bypass surgery. High-end ultrasound as well as hand-carried ultrasound depicted a right-sided pleural effusion, whereas chest radiograph was false-negative for the diagnosis of pleural effusion in this patient. (a) Hand-carried ultrasound B-Scan depicts right-sided pleural effusion which is characterized as the anechoic space between the highly reflective visceral pleura (black arrows) and the parietal pleura (white arrows). To note, the higher spatial resolution of the high-end ultrasound (b) compared with the hand-carried ultrasound system (a) is clearly visible (e.g. of the liver parenchyma, marked with a white star). (b) B-Scan with high-end ultrasound system exhibits right-sided pleural effusion which is characterized as the anechoic space between the highly reflective visceral pleura (black arrows) and the parietal pleura (white arrows). To note, the higher spatial resolution of the high-end ultrasound (b) compared with the hand-carried ultrasound system (a) is clearly visible (e.g. of the liver parenchyma, marked with a white star). (c) Supine chest radiograph did not exhibit typical findings of pleural effusion, hence, in this patient absence of pleural effusion was diagnosed
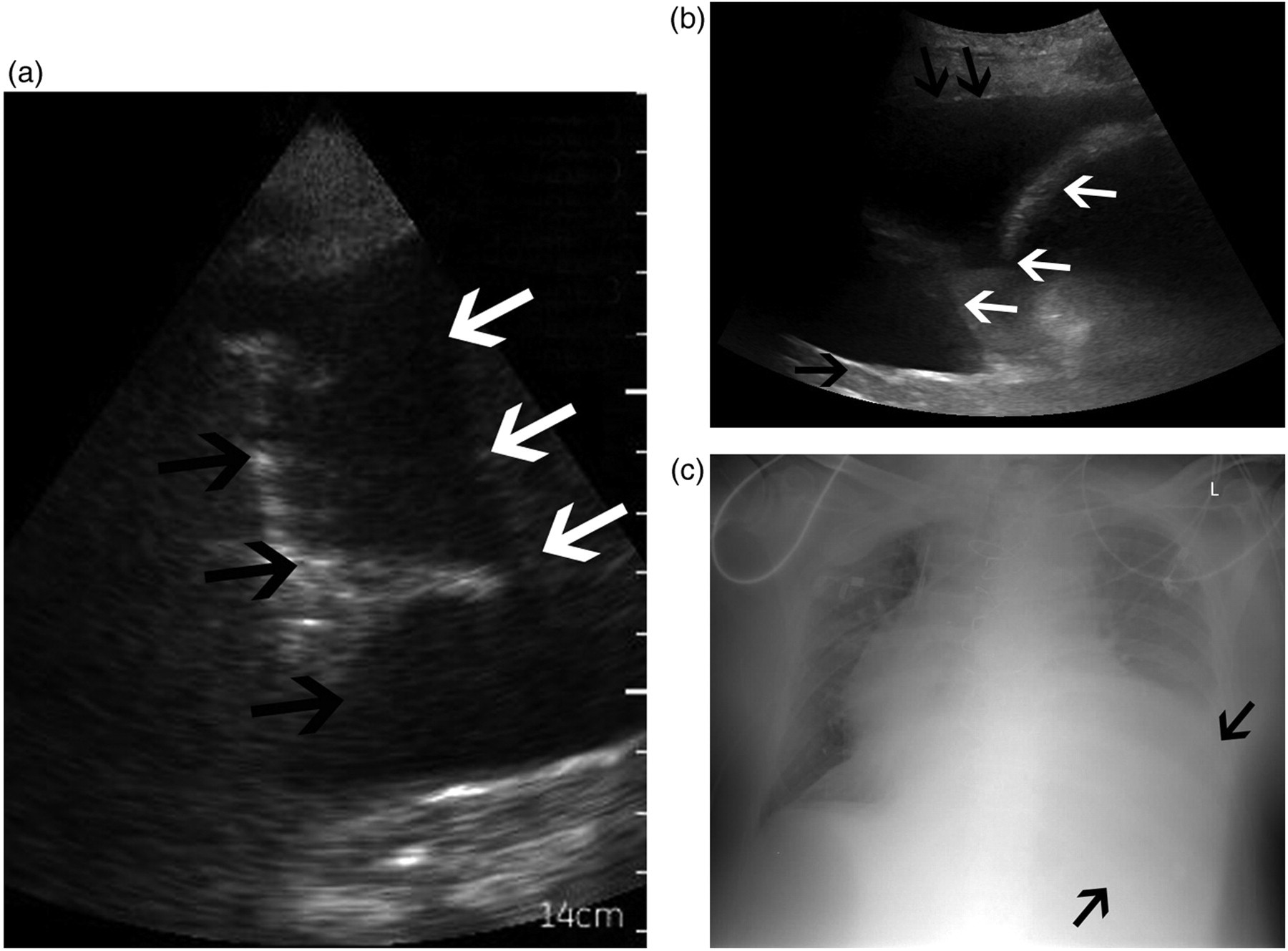
Congruent findings of hand-carried ultrasound and chest radiograph in a 72-year-old male patient 3 days after Whipple's pancreaticoduodenectomy. In this patient a chest radiograph was performed in order to identify the cause for clinically diagnosed cardiac decompensation. Large left-sided pleural effusion was depicted by both the hand-carried and high-end ultrasound system as well as by chest radiography. (a) Hand-carried ultrasound B-Scan demonstrates left-sided pleural effusion which is characterized as the anechoic space between the highly reflective visceral pleura (black arrows) and the parietal pleura (white arrows). (b) High-end ultrasound system B-Scan exhibits left sided pleural effusion which is characterized as the anechoic space between the highly reflective visceral pleura (black arrows) and the parietal pleura (white arrows). (c) Supine chest radiograph displays opacification of the basal left hemithorax (marked with arrows) and presence of pleural effusion to the left was diagnosed
Discussion
The present study shows that modern HCU imagers provide a very convenient, fast, and reliable technique for the diagnosis of PE in patients in intensive care units. In comparison to the standard of reference high-end ultrasound, HCU revealed no false-positive result and was false-negative in only three out of 35 hemithoraces leading to a sensitivity and specificity of 91% and 100%, respectively. To note, the three patients with false-negative results were overweight which is associated with reduced image quality of HCU and, the operator with the high-end ultrasound system estimated the amount of pleural fluid to less than 50 mL (which is usually not of clinical significance). In addition, in our study population the diagnostic yield of HCU was superior to chest radiography.
In the present survey all ultrasound examinations were performed in the supine position and, in particular, the patients were not moved, e.g. into an upright position. This proceeding was chosen to enable convenient and fast ultrasonographic examination of the patients using HCU imagers and to prove that HCU reliably depicts PE in patients lying in this supine position.
Diverse HCU imagers have been tested in prior studies, e.g. the Acuson P10 (Siemens Healthcare, Erlangen, Germany) and the OptiGo, (Philips Medical Systems, Andover, CA, USA) (9), but to the best of our knowledge these are the first data on the diagnostic value of a latest generation HCU device for the assessment of pleural effusion in patients in intensive care units being examined lying in the supine position.
Former evaluated HCU imagers already showed promising results for the diagnosis of PE, but these imagers have not made their way into daily clinical workflow yet. Instead, chest radiography remains the standard non-invasive diagnostic tool for the diagnosis of PE, probably related to the fact, that chest radiography is helpful to assess cardiopulmonary complications beyond PE like pneumonia, pulmonary atelectasis, and cardiac decompensation.
Considering the advantages of the HCU system employed in this study, including (a) ease and quickness of use, (b) quick bedside availability, (c) lack of radiation exposure, (d) low costs, and (e) high diagnostic yield for the diagnosis of PE in patients lying in the supine position we recommend to primarily examine patients by HCU if PE is, for example, clinically a likely diagnosis. If HCU depicts significant amounts of pleural fluid prompt pleural drainage can be initiated. If consequently clinical symptoms disappear, no further investigations such as chest radiography are necessary. In patients in whom HCU was negative further investigation (e.g. by high-end ultrasound or chest radiography) is indicated, in particular when complications like pneumonia, pulmonary atelectasis, or cardiac decompensation are assumed (10, 11). In symptomatic patients with negative ultrasound and negative chest radiography, computed tomography of the thorax should be considered (5, 12, 13).
There are some limitations of the present study. Only 24 patients and 48 hemithoraces were enrolled and examined with HCU, high-end ultrasound, and chest radiography by only one operator, respectively. Ultrasound is an operator-dependent modality and different operators might obtain different results. Nevertheless, in our study, a statistically significant difference of the specificity of HCU and chest radiography was determined. Computed tomography of the thorax is considered the “gold standard” for the diagnosis of PE (14). In the present study high-end ultrasound was chosen as standard of reference for the diagnosis of pleural effusion, because this approach is free of radiation exposure to the patients (15, 16) and, in a recently published survey Xirouchaki et al. showed that high-end ultrasound and computed tomography of the thorax reveal highly concordant results for the diagnosis of PE (17), revealing high-end ultrasound as a eligible standard of reference for the diagnosis of PE.
In conclusion, due to its ease of use and its high diagnostic yield HCU systems of the latest generation constitute a helpful technique for the primary assessment of PE in patients in intensive care units.