
Abstract
Background
The 256-slice computed tomography (CT) scanners with wider detector coverage and faster gantry rotation speed are now available. The performance of scanners that feature a rotation speed of 270 ms at coronary CT angiography (CCTA) has not been evaluated in patients with a higher heart rate.
Purpose
To evaluate the image quality of 256-slice CT with faster gantry rotation speed in patients undergoing CCTA.
Material and Methods
We enrolled 886 patients; 357(40.3%) underwent study on a 64-slice CT at a rotation speed of 420 ms, the other 529 (59.7%) were examined using a 256-slice CT scanner at 270 ms. Two observers judged the image quality of 2658 imaged coronary arteries on a 4-point scale.
Results
The mean image quality score was significantly higher for the 256 - than the 64-slice CT scans (3.94 ± 0.28 vs. 3.73 ± 0.61; P < 0.01). There was no significant difference in the image quality scores between 64 - and 256-slice scans in patients whose heart rate (HR) was <60 bpm. However, in patients whose HR exceeded 60 bpm these scores were significantly higher for 256-slice CT images (P < 0.01).
Conclusion
CCTA performed on the 256-slice CT scanner yielded significantly better image quality in patients with an HR exceeding 60 bpm.
Keywords
Introduction
Coronary computed tomography angiography (CCTA) facilitates non-invasive, accurate evaluation for the confirmation or exclusion of significant coronary artery stenosis (1–3). Although the gantry rotation time is faster on advanced scanners (4,5), a high heart rate (HR) increases motion artifacts of the coronary arteries and this limits the diagnostic image quality (4). New 256-slice CT scanners with wider detector coverage and a faster gantry rotation speed (270 ms/rotation) are now available. The single-cycle temporal resolution of the 256-slice CT instruments is 135 ms; it is 165–210 ms for 64-slice CT scanners. Klass et al. (6) whose study population included only patients with a stable HR below 65 bpm suggested that CCTA performed on a 256-slice CT scanner yields significantly improved and more stable image quality than 64-slice CT. To our knowledge, the effect of using 256-slice CT for CCTA in patients with a high HR has not been thoroughly assessed.
The purpose of this study was to clarify the effect of the faster gantry rotation speed and wider detector coverage of 256-slice CT scanners on the image quality at CCTA in high HR patients and to compare the results with images acquired on a 64-slice CT scanner.
Material and Methods
This retrospective study was approved by our institutional review board; patient informed consent was waived.
Study population
We reviewed 1014 consecutive series of ECG-gated CCTA studies performed at our institute during the year 2011. A total of 128 patients with inadequate breath-holding during scanning and patients with atrial fibrillation, coronary artery bypass grafting, and aged less than 16 years were excluded. Consequently, 886 patients (591 men, 295 women; mean age, 70.3 ± 10.3 years; age range 32–91 years) were included. All were referred for CCTA for clinical reasons based on guidelines promulgated by the American College of Cardiology (7). Of the 886 patients, 357 (40.3%) underwent scanning on a 64-slice CT scanner (Brilliance 64, Philips Healthcare, Cleveland, OH, USA) between January and May 2011. In June 2011 we replaced that machine with a 256-slice CT scanner (Brilliance iCT, Philips Healthcare, Cleveland, OH, USA) and assessed the other 529 patients (59.7%) seen thereafter on the new scanner.
Patient characteristics.
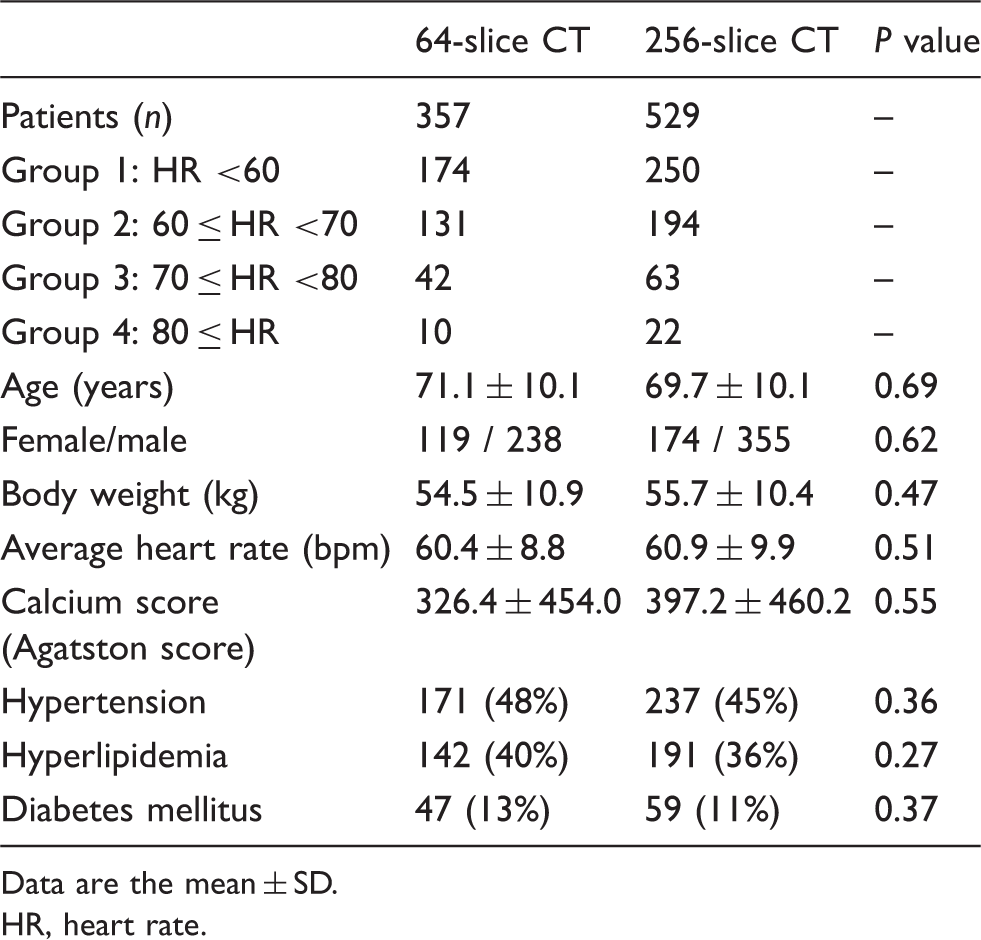
Data are the mean ± SD.
HR, heart rate.
CCTA acquisition
The parameters for 64-slice CT scanning were: detector collimation, 64 × 0.625 mm; tube rotation time, 420 ms; helical pitch (beam pitch), 0.20; tube voltage, 120 kVp; tube current-time product, 800–900 mAs. The calculated volume CT dose index (CTDIvol) was 52.8 mGy. The parameters for 256-slice CT scanning were: detector collimation, 2 × 128 × 0.625 mm with dynamic z-focal spot; tube rotation time, 270 ms; helical pitch (beam pitch), 0.16; tube voltage, 120 kVp; tube current-time product, 800–1000 mAs. The CTDIvol was 51.5 mGy. We did not use the ECG-dependent tube current modulation technique with either protocol.
Imaging and contrast material parameters of helical CCTA at 64- and 256-slice CT.
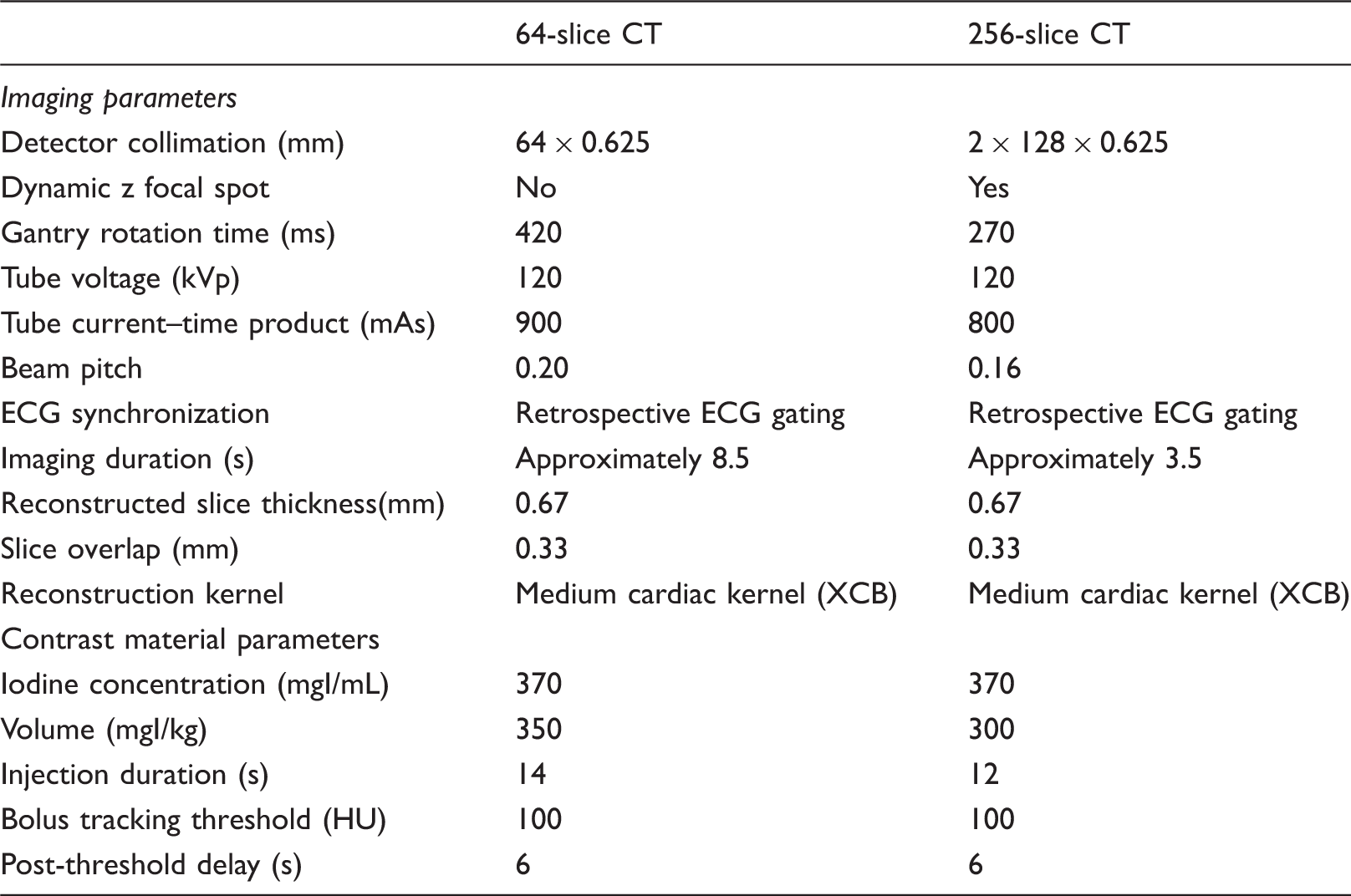
Image analysis
All images were reviewed and interpreted on PACS workstations (EV Insite, PSP Corp., Tokyo, Japan). The available images included axial source images and multiplanar- and curved multiplanar reconstructions. For viewing, images acquired on the two CT systems were intermixed. Two radiologists with 4 and 8 years of experience in CCTA who were blinded to the CT systems used, consensually assessed the images with respect to motion artifacts of the right coronary artery (RCA), the left main to the left anterior coronary artery (LMA-LAD), and the left circumflex coronary artery (LCX). They used a 4-point scale (Fig. 1) where: 4 (excellent) = no motion artifacts, useful diagnostic information; 3 (good) = some motion artifacts, sufficient diagnostic information; 2 (fair) = motion artifacts present, partially limited diagnostic information, and 1 (poor) = too much motion artifacts, no diagnostic information. A total of 2658 coronary arteries were assessed. Image quality scores below 2 (fair) were considered non-diagnostic. We compared the image quality scores of the two CT systems and also compared the scores assigned to patients grouped by their HR.
Angiographic examples of the image quality. (a) Poor image quality (score = 1). There are too many motion artifacts. No diagnostic information. (b) Fair image quality (score = 2). There are motion artifacts. Diagnostic information is somewhat limited. (c) Good image quality (score = 3). There are some motion artifacts. Diagnostic information is sufficient. (d) Excellent image quality (score = 4). There are no motion artifacts and the information is diagnostically useful.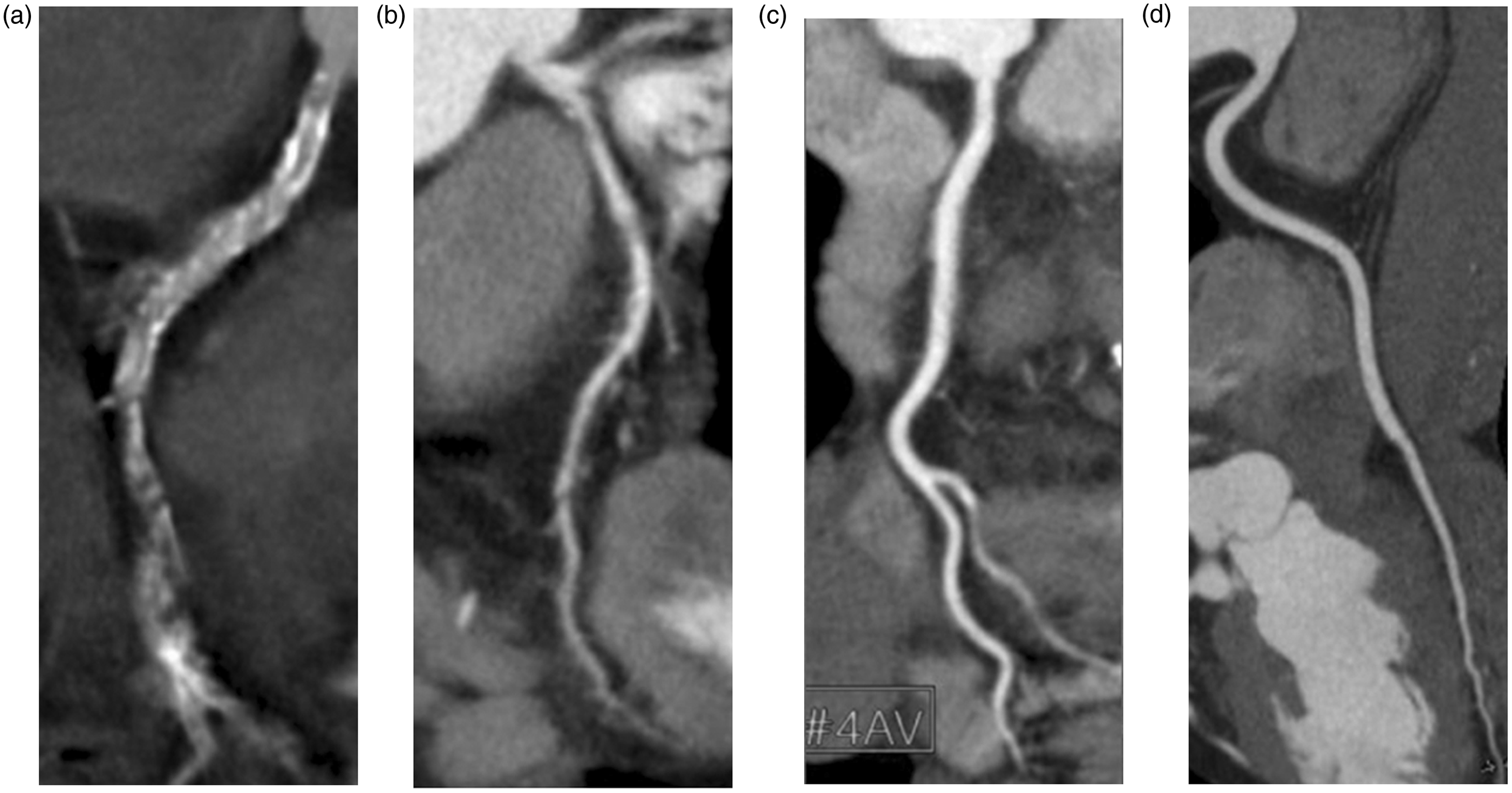
Radiation dose
The machine-generated CTDIvol (mGy) per examination during CCTA imaging was recorded. The method averages the radiation dose over the center slice of a CT examination consisting of multiple parallel slices. The dose length product (DLP) was calculated on the basis of the CTDIvol and data acquisition range. The effective radiation dose to the chest was obtained by using the equation (9): effective radiation dose = DLP × 0.014.
Effect of oral and i.v. beta-blockers on HR
In 349 of the 886 patients (39.4%) the baseline HR was ≥65 bpm and they received oral (n = 251) or i.v. beta blockers (n = 98). Before CCTA the effect of the beta blockers on HR was assessed; the HR before beta blocker administration and also the mean HR during CCTA scanning were recorded. There was no significant difference in the age (P = 0.73) and gender distribution (P = 0.61) of patients treated with oral or i.v. beta blockers.
Statistical analysis
Numerical data were expressed as the mean ± SD. Patient demographics and image quality scores obtained at 64- and 256-slice CT were compared. We also assessed the DLP and the effective radiation dose delivered under the two protocols. Differences in the mean values obtained at 64- and 256-slice CT for normally and non-normally distributed data were determined with the two-tailed independent t-test and the Mann-Whitney U test, respectively. All statistical analyses were with commercially available software (SPSS; SPSS version 15.0, SPSS, Chicago, IL, USA) and P values <0.05 were considered to indicate significant differences.
Results
Image quality analysis
Comparison of the coronary image quality grade at 64- and 256-slice CT.
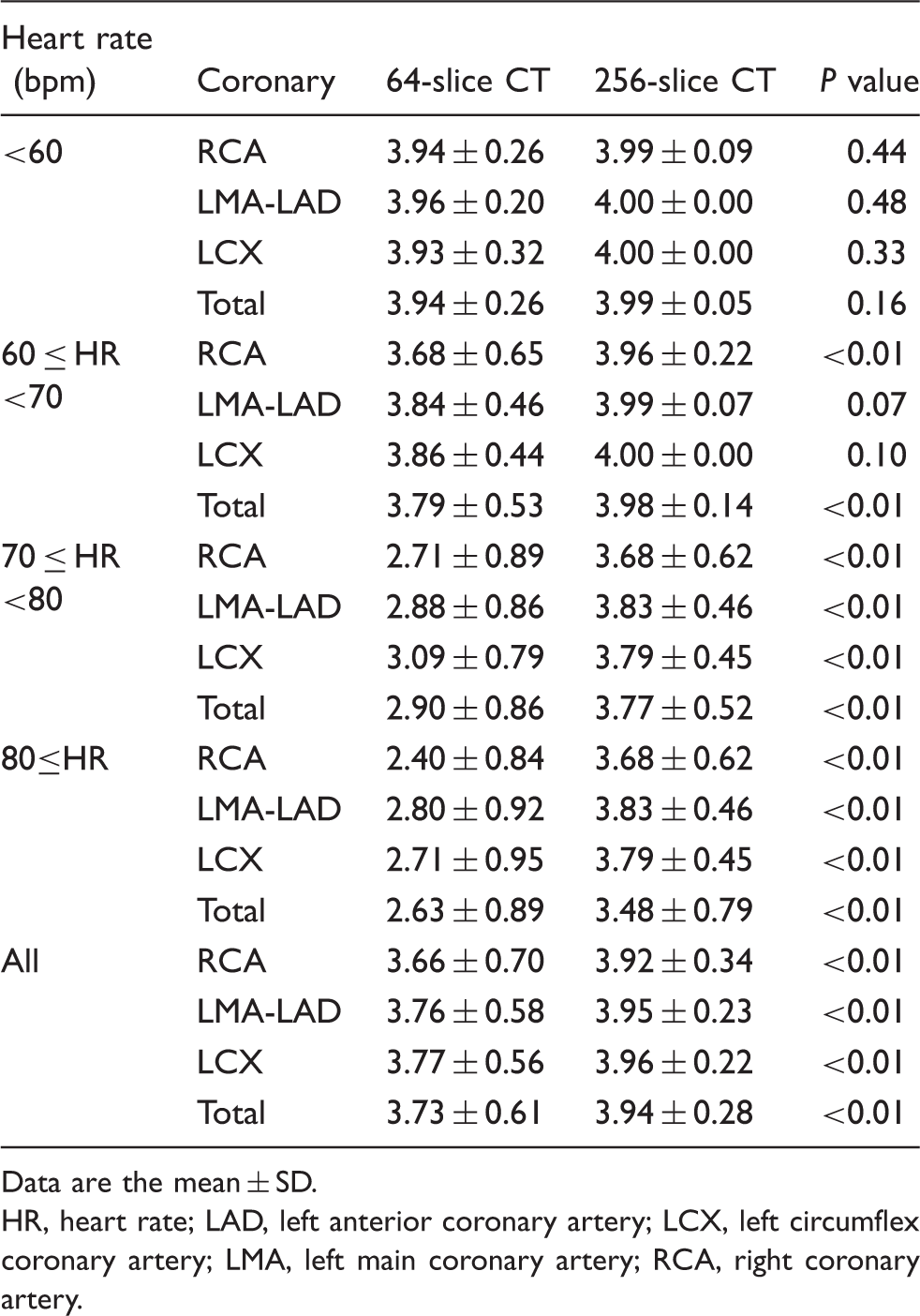
Data are the mean ± SD.
HR, heart rate; LAD, left anterior coronary artery; LCX, left circumflex coronary artery; LMA, left main coronary artery; RCA, right coronary artery.
Number of diagnostic coronary artery images obtained on 64- and 256-slice CT.

Data are the mean ± SD.
HR, heart rate.
Reconstruction cardiac phases on 64- and 256-slice CT.
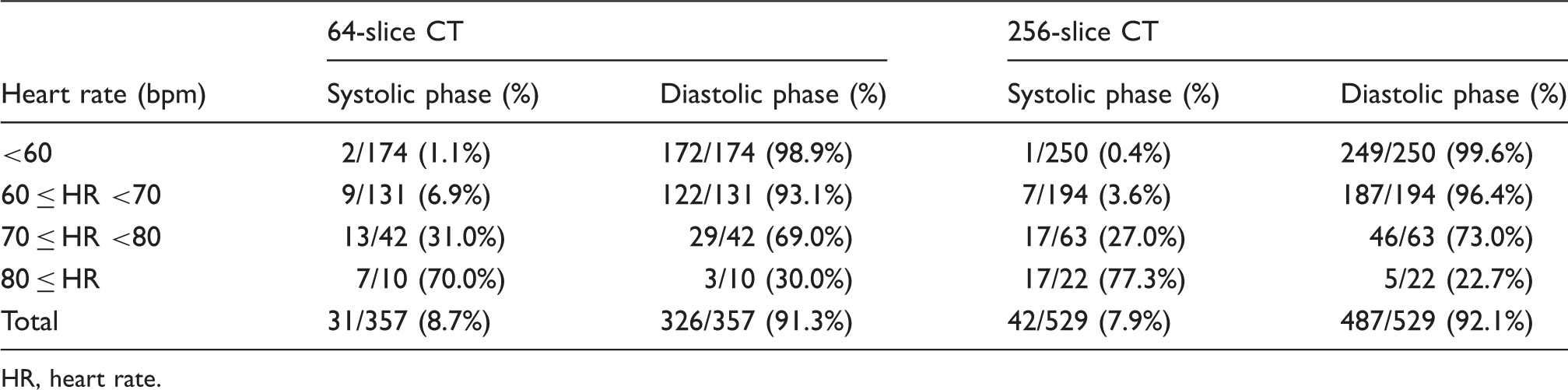
HR, heart rate.
Radiation dose
At 64-slice CCTA, the estimated radiation dose was 14.5 ± 2.6 mSv (range, 11.8–20.6 mSv); it was 15.1 ± 2.9 mSv (range, 12.2–21.0 mSv) at 256-slice CCTA (P = 0.41).
Effect of oral and i.v. beta-blockers on the heart rate
The mean HR reduction obtained with the oral and the i.v. beta-blockers was –19.0 ± 10.1 and –18.8 ± 10.9, respectively (P = 0.53). No major adverse reactions were observed.
Discussion
We demonstrate that in patients with an HR of 60 bpm or higher the 256-slice CT scanner yielded significantly better image quality than the 64-slice scanner. This was primarily attributed to the improved gantry rotation speed (270 ms) of the 256-slice CT scanner and the shorter imaging time required for helical acquisition at wider detector coverage. The increased coverage shortens the acquisition time for the cardiac anatomy and lowers the sensitivity to HR variations.
At CCTA, the 256-slice CT scanner yields a temporal resolution of 135 – 27 ms depending on the patient HR; at 64-slice CT it is 210 – 42 ms. At an HR of 60 bpm or higher, the image quality of 64-slice CT scans deteriorated; this may be explicable by the lower temporal resolution. On the other hand, at 256-slice CCTA the image quality was robust even at higher HR and the temporal resolution was better.
When multi-segment reconstruction algorithms are used, the image quality may suffer due to a broadening of the time sensitivity profile because of inconsistencies of subsequent heart cycles. As the cardiac motion pattern varies with each beat, spatial inconsistencies and blurring occur if data for a single transverse image are sampled from several heartbeats. Segmented reconstruction algorithms assume periodicity of consecutive cardiac cycles, however, data from several subsequent cardiac cycles with slightly different R-R interval lengths are derived from slightly different cardiac phases (10). As this timing shift is averaged out during the reconstruction of each transverse image, blurring within individual images is increased. Theoretically, such spatial inconsistencies impair diagnostic accuracy for stenosis detection and grading. The improved temporal resolution of 256-slice CT can increase the HR range over which single-segment image reconstruction is obtained, thereby avoiding the need for multi-segment reconstruction and excessive image blurring.
Klass et al. (6) who compared the image quality of CCTA performed on 64- and 256-slice CT systems in patients with a stable HR below 65 bpm concluded that CCTA using 256-slice CT yielded significantly better and more stable image quality and attributed this, as we did, primarily to their faster gantry rotation speed. Ours is the first comparative evaluation of 64- and 256-slice CT in patients with a high HR undergoing CCTA. According to Khan et al. (11), at CCTA the image quality was significantly better with 320-row than 64-slice CT. We posit that this is attributable to the reduction in the image acquisition time at 320-row CT because the gantry rotation time was 350 ms for both systems. We suggest that not only the shorter acquisition time but also the faster rotation time improve subjective image quality at CCTA.
At dual-source CT the temporal resolution is 83 ms. Wang et al. (12) compared the image quality at single- and dual-source CT. They reported similar results in patients with a lower HR but in patients with an HR in the range of 70–79 bpm, dual-source CT yielded better image quality, suggesting that faster temporal resolution is a prerequisite for successful CCTA in patients with a high HR.
The higher the HR, the greater is the likelihood of motion artifacts that can considerably diminish the diagnostic accuracy of CCTA scans (13,14). Bamberg et al. (15) evaluated a total of 6253 coronary segments and found that the odds for non-evaluable segments were 1.35 per 10 bpm. According to current guidelines, the ideal HR is below 60 bpm for optimal image quality (16).
Reducing the HR with beta blockers has been recommended in most patients referred for CCTA (16–19). Variability in the HR, which also affects the image quality, was considerably lower in patients treated with beta blockers before CCTA (2.45 bpm ± 1.53 vs. 4.29 bpm ± 2.25) (20). There was no significant difference in the HR reduction after the oral or i.v. delivery of beta blockers and no adverse reactions were elicited in our patients. Maffei et al. (21) reported that the desired effect was obtained much faster with the i.v. than the oral delivery of beta blockers. To avoid prolongation of pre- and post CCTA care we now routinely deliver the beta blocker landiolol hydrochloride i.v. to patients with a high HR who are scheduled for CCTA.
Earlier studies that used 64- and 256-slice CT systems reported that the coronary image quality was equivalent and that the radiation dose could be reduced by 73–77% at prospective compared to helical CCTA (22,23). Thus, in select patients with a regular, low HR, prospective ECG-gated CCTA should be used. However, this technique cannot be applied in patients with an irregular or high HR. Moreover, with prospective gating, cardiac images are acquired during only a small portion of the R-R interval and functional information on cardiac valve and wall motion is not available. Therefore, helical acquisition remains important in patients with an irregular or high HR and when functional information of the heart wall and heart valves must be obtained.
The study population in this retrospective study consisted of 886 patients seen during the period from January to December 2011. During that period we routinely used retrospective ECG-gated scanning to evaluate not only the coronary arteries but also left ventricular function, myocardial ischemia, and the cardiac valves (24–26) and to avoid unexpected motion artifacts. However, we recognize that the radiation exposure was much higher at retrospective than prospective ECG-gated scanning. Hou et al. (23) compared the image quality and radiation dose for CCTA obtained with a prospectively gated and a retrospectively gated technique using a 256-slice CT scanner with a 270-ms gantry rotation speed, the same system we employed in our study. They concluded that a prospectively gated technique was applicable in patients with a stable HR below 75 bpm. With respect to radiation exposure, we should have used a prospectively gated technique in our patients with a stable HR below 75 bpm, and a retrospectively gated technique with ECG-dependent dose modulation in patients whose HR was 75 bpm or higher.
Our study has some limitations. First, we did not consider segment bias in our evaluations. The effect of temporal resolution may be different in each coronary segment even in the same coronary artery. Second, we evaluated the image quality subjectively and did not perform quantitative measurements to assess diagnostic accuracy and the signal-to-noise and the contrast-to-noise ratios. Third, ours is a retrospective study of patients imaged on two different systems. Repeat image acquisition in each patient for prospective studies using both 64- and 256-slice CT systems facilitates patient-specific image quality comparisons but is prohibited by dose-exposure considerations. Fourth, we did not use radiation dose reduction techniques such as prospective ECG-gated scanning and ECG-dependent dose modulation in our CCTA protocol.
In conclusion, ECG-gated CCTA performed on a 256- rather than a 64-slice CT scanner yields significantly better image quality in patients whose HR is 60 bpm or higher. Our findings suggest that 256-slice CCTA is a viable non-invasive option for cardiac imaging in patients with a high HR.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.