
Abstract
Background
Non-invasive evaluation of coronary stent patency by coronary computed tomography angiography (cCTA) remains challenging. Multiple studies showed that CT technology but also individual stent design strongly influence the assessability of coronary stents by cCTA.
Purpose
To expand the available data on cCTA characteristics of coronary stents by 24 novel types to help interpreting examinations of patients after stent placement and selecting which stents are suitable for assessment by cCTA.
Material and Methods
Twenty-four novel coronary stents (17 cobalt–chromium, six stainless-steel, one platinum–chromium) were examined in a coronary phantom. Standard cCTA parameters with stent-specific algorithms were used. Image quality was quantified for each stent using established parameters (in-stent attenuation alteration and visible lumen diameter).
Results
Most stents (n = 14) showed lumen visibilities of 45–55%. No severe restriction of lumen visibility (>60%) was found. The majority of stents (n = 13) caused only small intraluminal attenuation deviations and no severe alterations (>20%) were found. When grouped by manufacturing material, no significant differences were found between cobalt–chromium and stainless-steel with identical mean visible diameters (1.52 ± 0.17 mm vs. 1.52 ± 0.13 mm) and comparable attenuation alterations (35.04 ± 16.56 HU vs. 21.25 ± 14.60 HU). The only platinum–chromium stent showed a smaller visible diameter (1.23 mm) and higher attenuation alteration (41.70 HU), but was also deemed to be assessable by cCTA.
Conclusion
All 24 novel evaluated stents are eligible for non-invasive evaluation by cCTA without significant differences between cobalt–chromium and stainless-steel stents. This updated catalogue of CT appearances of current coronary stents may serve as reference when taking care of patients with stents in need of coronary imaging.
Introduction
Percutaneous coronary interventions (PCI) are among the most frequently performed therapeutic procedures in medicine and, in most cases, include the deployment of a coronary stent (1,2). Despite continuous improvements in stent design and medical treatment, in-stent restenosis (ISR) still represents the main complication in these patients (2,3). Therefore, the accurate reassessment of the vessel lumen after stent placement continues to be a relevant task. If ISR is clinically suspected, usually an invasive coronary angiography is performed (4). Although non-invasive alternatives using computed tomography (CT) are desirable, coronary CT angiography (cCTA) continues to be partly impeded by beam-hardening and partial volume artifacts, due to the metallic composition of stents (5). Thereby, the ability to adequately visualize the stent lumen does not only depend on the used CT technology (6–12), but also on the individual stent type, as various stent materials and designs lead to different levels of X-ray attenuation and subsequent artifacts (13–15). These specific influences have been described in a catalogue of the CT appearance of coronary stents, which was first published in 2006 (13) and has been updated twice since (14,15). In the meantime, the stent market has expanded further and new types have become available of which the CT imaging properties have not been investigated yet. Therefore, the purpose of our study was to evaluate the stent lumen visualization in 24 novel coronary artery stent types.
Material and Methods
Evaluated stents and experimental set-up
Twenty-four coronary artery stents of different materials and designs were studied. Manufacturer, material, strut thickness, length, and nominal diameter of the stents are summarized in Suppl. Table 1.
Seventeen stents were made of a cobalt–chromium alloy, six of stainless surgical steel (316L), and one of a platinum–chromium alloy. All investigated stents are balloon-expandable.
Before imaging, each stent was placed into a plastic tube with an inner diameter of 3 mm, simulating a coronary artery. The plastic material had a thickness of 0.3 mm with a CT number comparable to that of a vessel wall (35 HU). The tube was filled with Iohexol (300 mg Iohexol/mL; Accupaque 300; GE Healthcare, Braunschweig, Germany), which was diluted with saline solution to a CT number of 260 HU at 120 kVp, and sealed at both ends. Finally, the tube was placed in a plastic container (36 × 24 cm) filled with vegetable oil to simulate epicardial fat. The density of the oil was calibrated to measure −95 HU at 120 kVp. The phantom was then positioned onto the CT scanner table in the gantry parallel to the z-axis and centered in the isocenter of the scanner.
CT acquisition parameters
CT data were acquired on a 128-row spectral detector CT scanner (IQon, Philips Healthcare, Best, The Netherlands) with a simulated electrocardiogram (ECG) signal at a heart rate of 60 bpm for prospectively ECG-triggered data acquisition. The following routine clinical cardiac scanning parameters were used for all scans without specific optimization (16,17): slice collimation = 128 × 0.625 mm, rotation time = 0.27 s, tube current-time product = 125 mAs, tube potential = 120 kVp and resulting CTDIvol = 11.3 mGy.
The reconstructed field of view was set to 250 mm with a pixel matrix of 512 × 512. From the acquired raw data, images were reconstructed using a slice thickness of 0.67 mm and an increment of 0.35 mm with a (statistical) hybrid iterative reconstruction algorithm (iDose4, Philips Healthcare) using the iteration level 4 and a dedicated cardiac stent convolution kernel (XCD).
All quantitative analyses were performed with a fixed window width of 1500 HU and a window center of 300 HU as previously recommended (8,11,14).
CT data analysis
Axial reformations of all stents were used for evaluation and secondary longitudinal multiplanar reformations (MPRs) were generated for demonstration purposes only. The visible lumen diameter is given as average of the measurements on three representative axial slices in the center of the stent using the electronic caliper tool provided with the scanner’s standard workstation (IntelliSpace Portal, Philips Healthcare).
Attenuation alteration inside the visible stent lumen was evaluated on the same three axial slices using a region of interest measurement as large as possible but excluding the stent strut artifacts. The average attenuation within the stent was compared to the attenuation in the tube outside of the stent. The difference was considered as stent-related attenuation.
The means of the visible stent lumen diameter as well as the in-stent attenuation alteration were calculated and compared grouped by the used manufacturing material.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD) and intra-measurement variability coefficient was calculated for repeated measurements. Mean differences in quantitative imaging parameters (visible stent lumen diameter and in-stent attenuation alteration) were tested using an unpaired student’s t-test for the cobalt–chromium and stainless-steel stents. A two-tailed P value <0.05 was inferred to indicate significance. All statistical analyses were conducted using commercially available software (SPSS, release 23.0; IBM, Armonk, NY, USA).
Results
Visible lumen diameters and attenuation alterations of the examined stents.
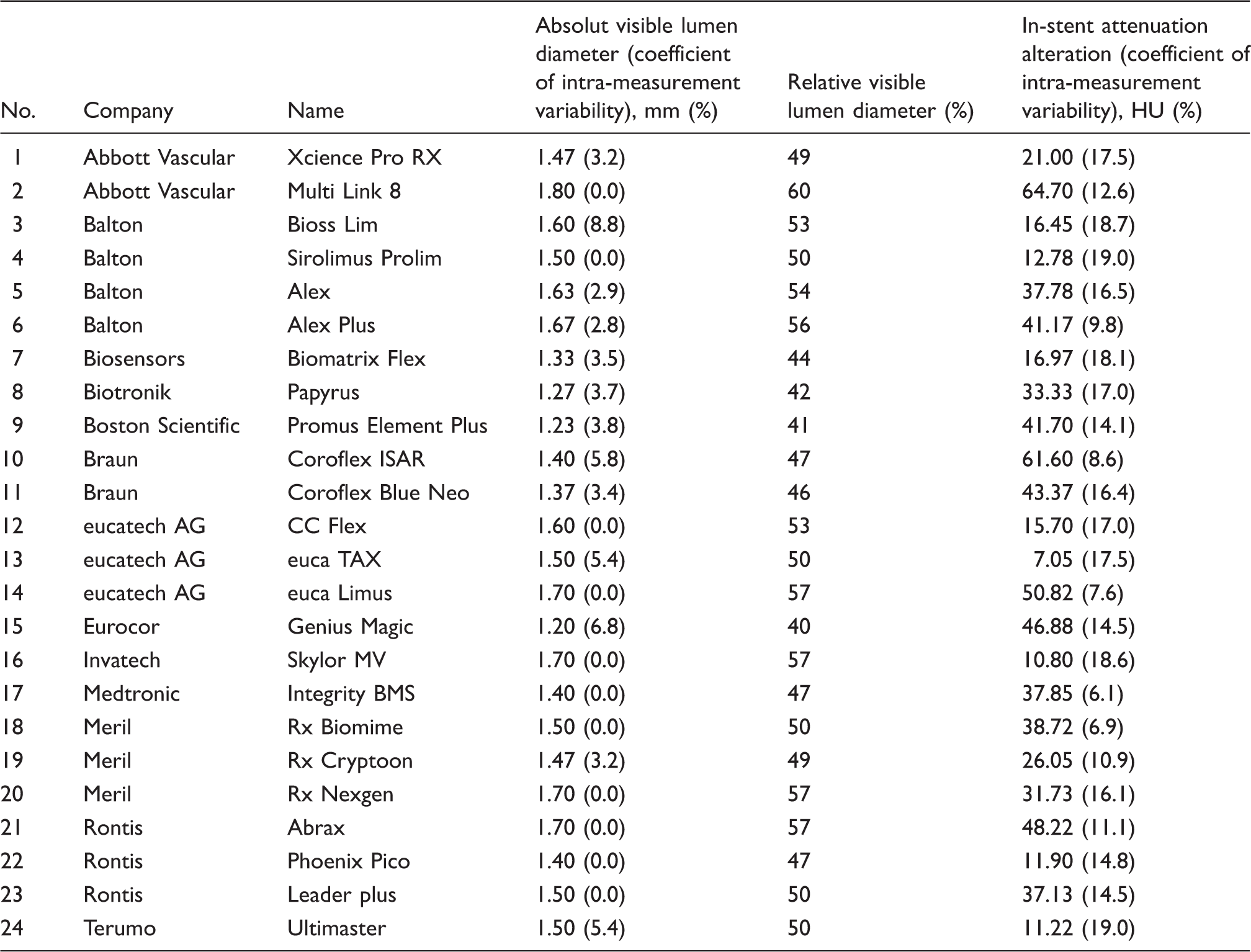
Mean diameters of the visible stent lumen in mm and mean alterations of the in-stent attenuation values in Hounsfield units (HU) of the investigated stents using the described acquisition and reconstruction parameters. The coefficient of the respective intra-measurement variability is given in brackets.
Thirteen stents showed only small deviations of the in-stent lumen attenuation (≥10%), whereas the other 11 stents caused moderate alterations of the measured densities inside of the stent lumen (up to 20%). Again, no severe deviations of in-stent attenuation were observed in the examined set of stents. Intra-measurement variability coefficients for the mean visible stent lumen diameters were low (mean = 2.5%, range = 0.0–8.8%) while they were higher for in-stent attenuation alterations (mean = 14.3%, range = 6.1–19.0%).
For illustration, longitudinal MPRs were created of every stent and then composed to Fig. 1.
Longitudinal through-plane reformations of 24 different coronary stents numbered accordingly to Table 1 (slice thickness 0.67 mm, other acquisition and reconstruction parameters as previously described).
Visible lumen diameters and attenuation alterations grouped by different manufacturing materials.

Mean diameters of the visible stent lumen (in mm) and mean alterations of the in-stent attenuation values (in Hounsfield units [HU]) group by the different manufacturing materials (cobalt–chromium, stainless-steel, and platinum–chromium).
Discussion
In-stent lumen visibility in cCTAs is impaired by stent related artifacts, which depend on the individual characteristics of each stent (material composition, stent strut thickness, stent architecture). In previous studies, the imaging properties were evaluated for a wide range of coronary stents available at that time (13–15). Since then, new stent types have been introduced, of which the imaging properties have not been investigated yet. In our present study we investigated 24 of these novel stent types using current CT acquisition and reconstruction technologies.
As reflected by the collection of these novel stents, cobalt–chromium has surpassed stainless-steel as the most frequent manufacturing material for coronary stents in the last decade (18). In former studies, stainless-steel stents always represented the largest share of evaluated manufacturing materials (9,13,14,19,20). A comparison of these two most frequent materials in our study gave similar results with respect to the visible lumen diameter as well as stent-related alterations of in-stent attenuation without significant difference between both subgroups. In line with our results, platinum-based stents are known to give rise to stronger artifacts due to the increased density of their manufacturing material (15). The specific imaging properties of the platinum stent tested in our series, however, were still acceptable (Promus Element Plus; Boston Scientific, Marlborough, MA, USA; visible lumen diameter 41%, in-stent attenuation alteration 13%). Among all investigated stents there was no stent with <40% of visible lumen and only five stents with restricted lumen visibility of 40–45%. In the absence of severe lumen narrowing due to blooming artifacts, there was also no stent with extensive artificial alterations of in-stent lumen density. Overall, there was a reasonable mean observed in-stent attenuation alteration of about 10% with a still acceptable maximum deviation of 20%. Therefore, all evaluated stents seemed eligible for non-invasive evaluation by cCTA.
This is a distinct improvement over the beginning of CT-aided coronary stent imaging when not a single evaluated stent showed a lumen visibility of >40% (20). This progress has been made possible by a combination of advances in stent design as well as CT technology. With respect to the stent materials used today, there is hardly any chemical element with higher atomic numbers being utilized. Even with the latest CT scanner technologies, chemicals with high atomic numbers, such as tantalum (atomic number (Z) 73), prevent sufficient lumen visualizations of stents (6). Conversely, the now widespread cobalt–chromium stents consist of chemical elements with only moderate atomic numbers (Z 27 and 24) and additionally allow a considerably thinner manufacturing of the stent struts, which translates into a markedly decreased mean strut thickness in our study of about 80 µm. This is about 40% less than what has been reported for stent designs in the initial CT stent imaging studies (∼115 µm), where artifacts were far more prevalent (20). Moreover, a thinner strut thickness has also been shown to be clinically beneficial as it lowers in-stent restenosis rates (21).
In addition, advances in CT technology have contributed to improved stent visualization. In comparison to the four-slice CT scanner used primarily in 2002 (20), stent imaging capabilities improved in later studies with the use of 16-slice (12) and 64-slice (8) CT scanners, eventually resulting in lumen visibilities comparable to the results of our current study (13).
Our study has several limitations. Due to the in-vitro approach, patient-specific influencing factors (BMI, contrast agent doses, heart function, etc.) were not considered. Additionally, cardiac motion was not simulated in our set-up, therefore possible motion artifacts, as they might occur in patients with higher heart rates or arrhythmia, are not taken into account. Also, the number of novel stainless-steel stents was limited, which therefore potentially restricted the capability to identify subtle statistical differences. However, relevant differences in CT imaging eligibilities between stainless-steel and cobalt–chromium stents seem unlikely based on our results. The intra-measurement variability coefficients for in-stent attenuation alterations were slightly elevated, though still in a clinically acceptable range. The observed variability is to be attributed to spatial variations in the severity of imaging artifacts along the extent of each stent. Conversely, intra-measurement variability coefficients for the mean visible stent lumen diameter were desirably low.
In conclusion, this study expands the catalogue of CT imaging characteristics of coronary stents, originally published in 2006 and updated in 2009 and 2014, by 24 novel, previously unavailable stents. In line with results of other recent studies showing continuously improved CT imaging capabilities of coronary stents, all of these novel stents appear eligible for evaluation by cCTA. This updated catalogue will help to decide which patients with coronary stents are eligible for coronary CT assessment and also prove valuable when interpreting the stented coronary vessel lumen.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.