
Abstract
Background
Depiction of the exact arterial liver anatomy as well as identifying potential extrahepatic non-target vessels is crucial for a successful preparation of radioembolization (RE).
Purpose
To compare the diagnostic impact of dual-energy computed tomography (DECT) to digital subtraction angiography prior to RE.
Material and Methods
DECT was applied in 46 patients with hepatocellular carcinoma (HCC) prior to RE. Eighty kV DE as well as reconstructed 120 kV equivalent DE datasets were evaluated in comparison to correlating digital subtraction angiography (DSA) datasets. Two radiologists evaluated in consensus the delineation of liver arteries and extrahepatic non-target vessels utilizing a 4-point scale (4 = excellent delineation; 1 = non-diagnostic). In addition, the arterial vascularization of liver segment IV was evaluated and classified: signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR; liver arteries to adjacent liver tissue) were obtained via ROI analysis.
Results
Both imaging techniques (DECT, DSA) enabled high-quality assessment of all analyzed liver arteries. Out of the two CT datasets, 80 kVp-DE datasets offered superior delineation of the right gastric artery (3.5 ± 0.7 vs. 2.5 ± 0.5), the vascularization of segment IV (3.9 ± 0.2 vs. 3.3 ± 0.5) as well as potential extrahepatic non-target vessels (3.9 ± 0.1 vs. 3.3 ± 0.5). In accordance to the results of the qualitative analysis, 80 kVp-DE datasets also yielded higher SNR (34.84 vs. 29.31) and CNR (28.29 vs. 21.8) values in comparison to the 120 kVp datasets.
Conclusion
Eighty kVp DECT enables a significantly better assessment of the arteries of the upper abdomen for therapy planning in comparison to correlating 120 kVp datasets. This may allow for identification of potential extrahepatic non-target vessels and assessment of target volume for therapy planning prior to DSA.
Introduction
Radioembolization (RE) is increasingly used in the treatment of hepatic carcinoma and hepatic metastases (1–3). The precise knowledge of the anatomy of the abdominal arteries and determination of the liver volume is crucial for the planning of the therapy process.
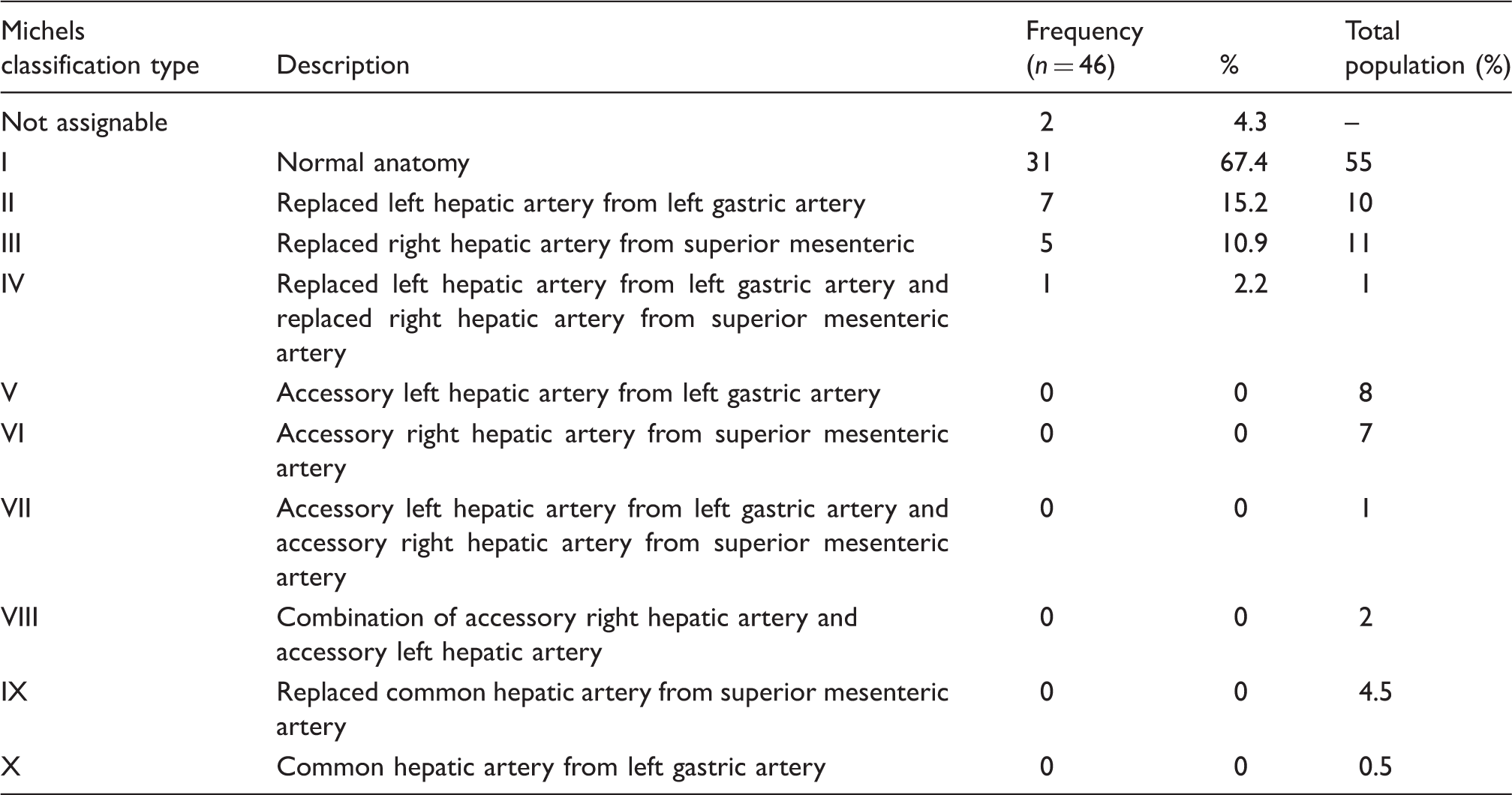
Distribution of classification types according to Michels in the investigated patient population related the total population.
Computed tomography (CT) of the liver including CT angiography (alternatively magnetic resonance imaging [MRI] and MR angiography) should be performed prior to RE. In addition, a digital subtraction angiography (DSA) is performed to assess the hepatic arteries as well as the extend of tumor disease. As part of the DSA potential non-target vessels may be occluded with platinum coils.
Dual-energy computed tomography (DECT) is a new diagnostic method enabling tissue differentiation and visualization and quantification of contrast uptake (8–18). The aim of this prospective study was to determine the diagnostic value of DECT for the preparation of RE. Special focus was the delineation of small arterial vessels in using different dual-energy image datasets.
Material and Methods
Between September 2009 and October 2010, 46 patients (22 men, 24 women; mean age, 64 years ± 10 years) were included in this prospective study. A DECT of the upper abdomen as well as a digital subtraction angiography of the hepatic arteries was performed. The study was approved by the Ethics Committee and all patients had given written consent.
CT examinations were acquired by a dual-source multidetector CT (Somatom Definition Dual Source, Siemens Medical Solutions, Forchheim, Germany). In supine position, an injection of a non-ionic contrast medium (1.5 mL per kilogram of body weight, Xenetix 300, Guerbet, Sulzbach, Germany) was performed with Bolus tracking and an injection rate of 4 mL/s. The images were acquired in the arterial and portal venous phases covering the entire abdomen. Test parameters of the tube A/B were as follows: 140/80 kVp and 96/404 mAs. Dose modulation with Care DOSE 4D (Siemens Medical Solutions) was applied.
DSA (TM Philips Allura, Philips Healthcare, Best, The Netherlands and Toshiba Infinix DP-i, Toshiba Medical Systems, Tokyo, Japan) was performed via a transfemoral arterial access. The celiac trunk and the superior mesenteric artery were explored utilizing a macro catheter (5 French Sidewinder-1-Catheter, 5 French Cobra Catheter, Terumo Europe, Leuven, Belgium). After completing overviews of the hepatic arteries a selective angiography of the left and right liver lobe was performed using a microcatheter (Rebar Microcatheter, 0.027 in; EV3, Plymouth, MN, USA) and a contrast power injection (flow, 3 mL/s; volume, 12 mL).
Postprocessing and image reconstruction
The DECT generated three different series of images: 80 kVp, 140 kVp images, and “average images” based on 70% of the 140 kVp and 30% of the 80 kVp information. Image data were transferred for postprocessing to a workstation (MMWP Syngo, Siemens Medical Solutions).
Evaluation of image datasets
Image data of the DSA and the DECT acquisitions were compared by two radiologists (with 5 and 10 years of experience) in consensus concerning the following factors:
Delineation of hepatic arterial anatomy based on the Michels classification; Arterial supply of segment IV of the liver: arising from right hepatic artery, left hepatic artery, from right and left hepatic artery, or separately; Delineation of non-target vessels.
DE 80 kVp and 120 kVp equivalent CT image datasets were compared in terms of the following factors:
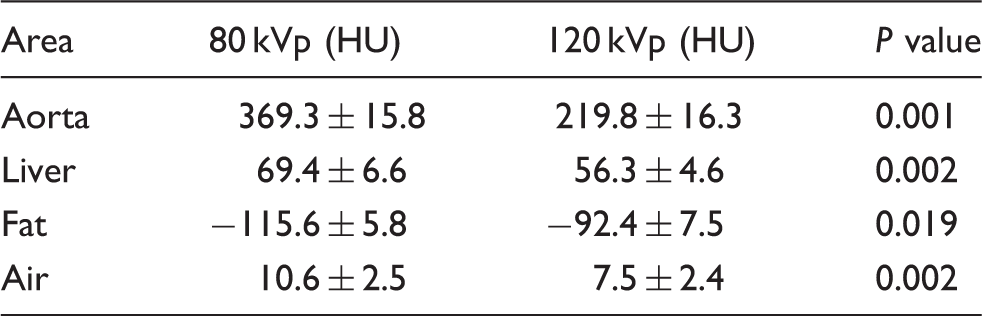
Delineation of the following arteries: common hepatic artery, right hepatic artery, left hepatic artery, gastroduodenal artery, right gastric artery, left gastric artery, artery (s) to segment IV of the liver, accessory arteries. A 4-point scale (1 = not assessable - 4 = well visible) was applied. Overall image quality: CT attenuation values (HU) were determined in four regions: liver tissue; aorta at the level of the celiac trunk; perihepatic fat; air anterior to the patient using region of interests (ROI; 1.0 cm2). Furthermore signal-to-noise ratios (SNR) HU [aorta]/HU [air]) and contrast-to-noise ratios (CNR) (HU [aorta] – HU [liver])/HU [air]) were calculated.
For comparison between the two different DECT datasets and DSA image data, a Wilcoxon signed rank test was applied and tested for statistical significance. All calculations were performed using dedicated software (SPSS, version 21, SPSS Inc., I Chicago, IL, USA). A P value of <0.05 indicated statistical significance.
Results
Hepatic arterial anatomy
Both 80 kVp and 120 kVp equivalent image datasets of DECT allowed for a correct classification assignments by Michels in 44/46 patients (Table 1). In 2/46 patients no classification according to Michels could be made (direct disposal of the hepatic artery from the celiac trunk or direct disposal of the right hepatic artery from the celiac trunk).
Arterial supply of the liver segment 4
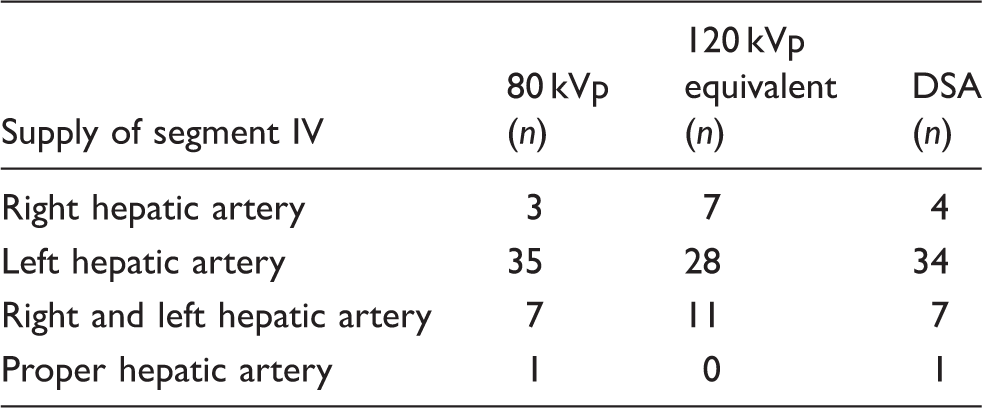
DSA showed a supply of segment 4 via the right hepatic artery (n = 4), the left hepatic artery (n = 34), the right and left hepatic artery (n = 7) and isolated from the proper hepatic artery (n = 1).
Arterial supply of segment IV. Comparison between the 80 kVp, 120 kVp equivalent, and DSA image data (DSA = reference).
Delineation of non-target vessels
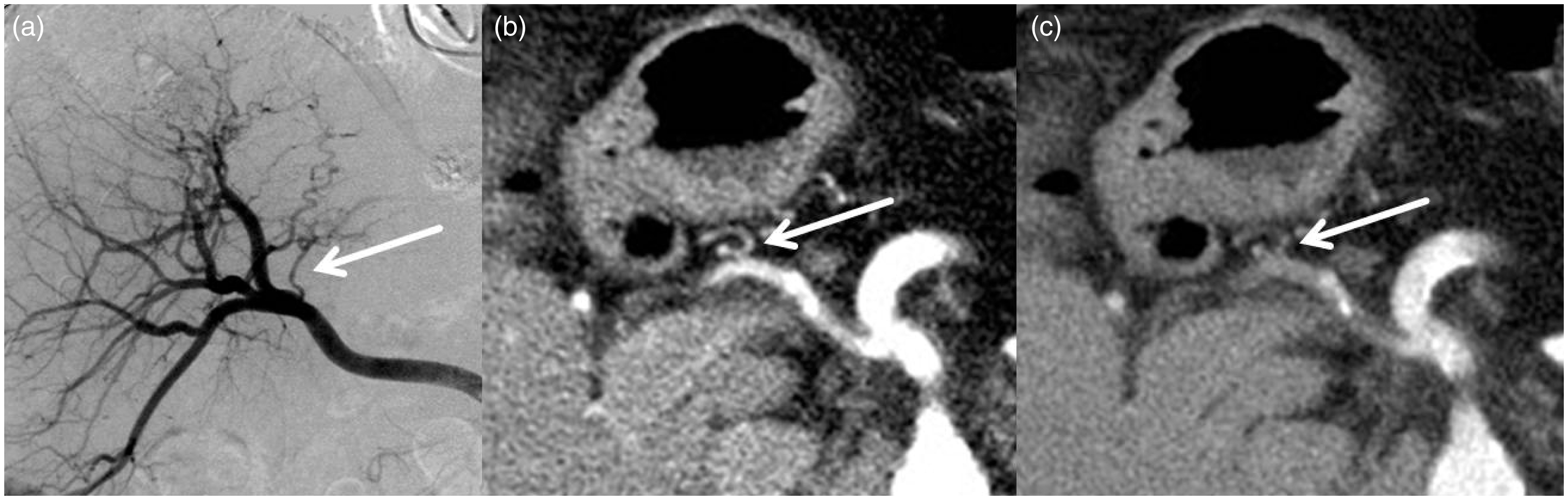
In eight patients accessory arterial non-target vessels were detected by DSA (6 pancreatic arteries, 2 gastric arteries). By means of 80 kVp image data, this could be confirmed in all cases. However, a pancreatic branch could not be detected in one patient based on 120 kVp image data.
Quantitative evaluation of the delineation of arterial vessels
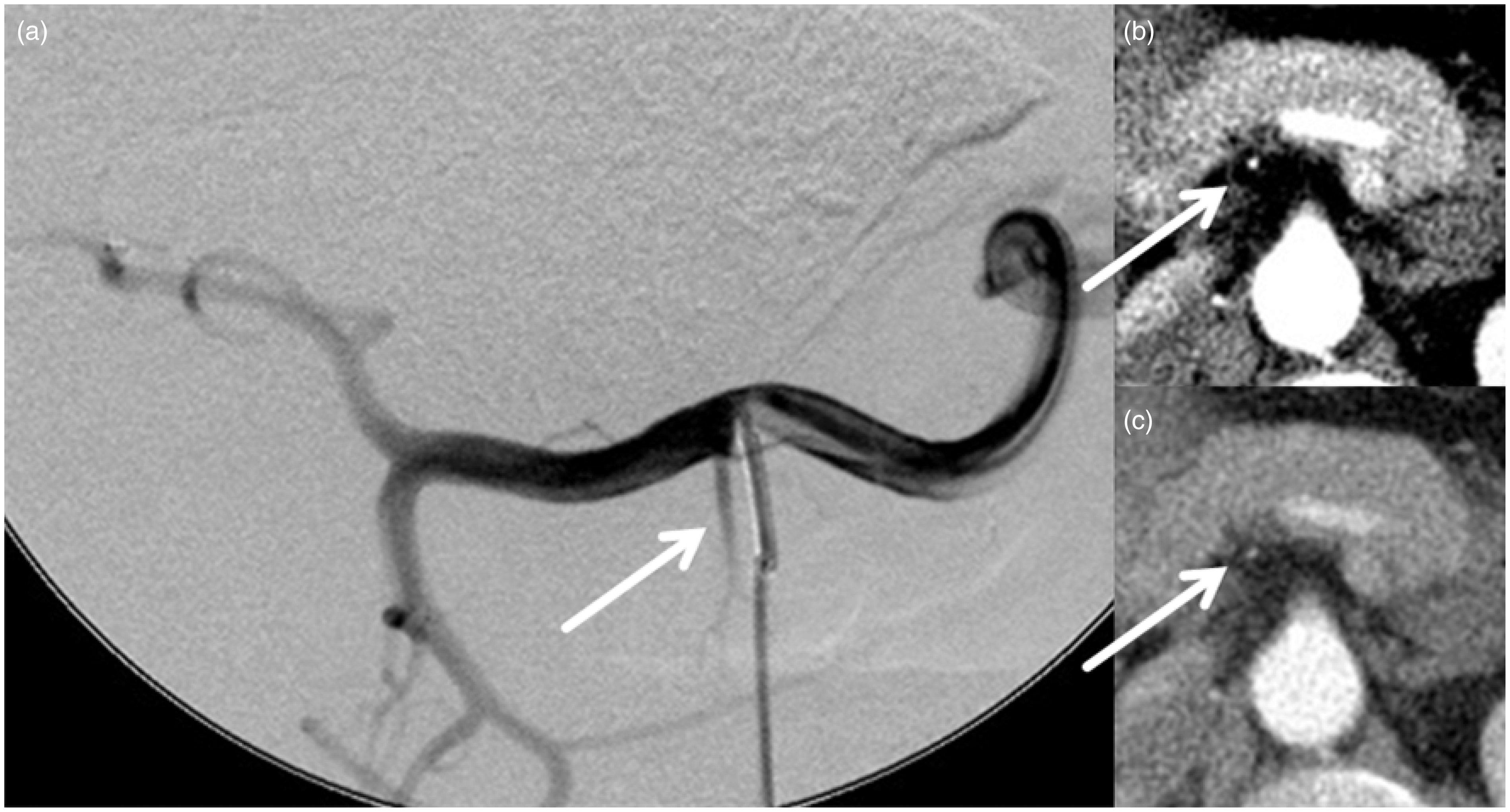
Mean values of 80 kVp imaging (3.9 ± 0.2) was higher than average values of 120 kVp images (3.6 ± 0.6) without statistical significance (P = 0.092). The delineation of the common hepatic artery, the right hepatic artery, the left gastric artery, and the gastroduodenal artery was excellent with both kVp values: the maximum value of 4.0 was reached based on either 80 kVp and 120 kVp data. The depiction of the left hepatic artery was identical for both CT values (3.9 ± 0.6). However, the right gastric artery, the segment 4 arteries and accessory arteries were significantly better delineated on the 80 kVp images (Figs 1–3). The values for the delineation of all arteries are displayed in Table 3.
Imaging of the segment 4 artery (arrow) with DSA (a), 80 kVp (b), and 120 kVp equivalent (c) DECT image data. Clearly better contrast and delineation using 80 kVp image data (DECT parameter: reconstructed slice thickness 3 mm, kernel D30, window settings C:50/W:350, axial). Imaging of an accessory pancreatic artery (arrow) with DSA (a), 80 kVp (b), and 120 kVp equivalent (c) DECT image data. Clearly better contrast and delineation using 80 kVp image data (DECT parameter: reconstructed slice thickness 3 mm, kernel D30, window settings C:50/W:350, axial). Imaging of the right gastric artery (arrow) with DSA (a), 80 kVp (b), and 120 kVp equivalent (c) DECT image data. Better contrast and delineation using 80 kVp image data (DECT parameter: reconstructed slice thickness 3 mm, kernel D30, window settings C:50/W:350, axial). Evaluability of the arterial vessels with 80 kVp and 120 kVp equivalent image data (DSA = reference) (1 = not assessable to 4 = very easy to assess).

Overall image quality
CT attenuation values (HU): comparison between 80 kVp and 120 kVp equivalent image data.
Objective image quality: signal-to-noise (SNR) and contrast-to-noise (CNR) ratios. Comparison between 80 kVp and 120 kVp equivalent image data.

Discussion
Interventional therapy for the treatment of unresectable liver malignancies, particularly hepatocellular carcinoma, is increasingly applied (1,19–22). Also other tumor entities including advanced cholangiocellular carcinoma and liver metastases of colon or breast cancer represent an indication of local tumor treatment. This is particularly true when hepatic tumor progression is observed under systemic chemotherapy. In addition to the trans-arterial chemoembolization (TACE), bland embolization or RE has been established as a therapy option in patients with diffuse hepatic tumor burden (23,24).
Essential for a technically successful and low-risk RE is a very precise knowledge of the individual anatomy of the hepatic arteries. Furthermore, non-target vessels arising from the arterial hepatic tree and feeding other organs need to be identified. The injection of microspheres loaded with yttrium in extrahepatic organs such as the stomach, bowel or pancreas can cause serious complications including ulceration and organ necrosis (25). Furthermore, the arterial supply of liver segment IV is crucial.
Since the initial treatment depends on the tumor burden fed by the right or left hepatic artery, the assignment of segment IV is essential for the calculation of the target volume in order to avoid an over- or under-dosing of radiotherapy.
In this trial we could demonstrate the acquired dual energy 80 kVp images to provide more detailed information prior to RE compared to the 120 kVp equivalent image data. Most useful was the significantly improved vascular opacification at the 80 kV image data. These findings are in accordance with a study by Pinho et al. They could show the 70 kVp image data of the DECT to provide significantly higher vascular contrast with respect to the aortoiliacal arteries compared with monoenergetic 120 kVp own image data (26). With our study we demonstrated that for small-caliber arteries in particular better image data can be evaluated with the low dose datasets.
Iezzi et al. also showed improved arterial enhancement of the pelvic and lower extremity arteries using the 80 kVp image data (27). However, compared to the 120 kVp image data, they found no difference in diagnostic accuracy. In our studied patients group, however, the 80 kVp image data had a decisive influence on the diagnostic accuracy. Non-target vessels were better detected and the arterial blood supply of the liver prior to RE could be depicted more accurately with better classification of the segment IV arteries.
Thus, the hepatic and non-target arteries may already be better identified prior to the routine digital subtraction angiography before RE. This may have implications for the intra-arterial catheter position, which is chosen for the injection of the microspheres. In addition, non-target arteries can be identified more specifically and embolized if necessary.
The significant benefits of DECT were previously demonstrated in numerous studies (8–18). Advantages were evident in the qualitative and quantitative assessment of tumor and organ perfusions, tissue characterization, or the improved plaque detection and characterization. The secondary generation of virtual precontrast image data from the contra-enhanced raw data allows a significant reduction of radiation exposure to the patient.
DECT should be the method of choice in the evaluation of patients before RE. MR angiography has a lower accuracy to evaluate small arteries in the abdomen (7). Another application for DECT could be treatment monitoring after RE. Advantages result in the virtual precontrast image data generation and improved quantification of contrast uptake and vascularization of particular discordant or pseudoprogressive hepatic tumor after RE (8,13).
This study is not without some limitations. The 80 kVp DECT image data were not compared with monoenergetic additionally produced 120 kVp image data. However, the secondary reconstructed 120 kVp equivalent CT images have a proven comparable image quality (15,28,29). Best imaging test to detect the perfusion of segment 4 would be a separate MAA scan of the left and right hepatic artery or a core beam CT in angiography with separate contrast injections.
In conclusion, DECT leads to a significant improvement in the diagnostic evaluation of patients for RE. This could lead to a minimization of the patient load, a timely start of treatment and reduced cost through savings on additional pretherapeutic investigations.