
Abstract
Background
Hepatic arterial infusion (HAI) chemotherapy is being explored for treatment of malignant liver tumors. Maintenance of HAI systems is important for effective treatment.
Purpose
To prospectively evaluate the efficacy of dual-phase CT angiography through the port-catheter system for HAI chemotherapy.
Material and Methods
This study enrolled 47 patients receiving HAI chemotherapy for malignant liver tumors who underwent dual-phase CT angiography through the port-catheter system using multislice CT. Using maximum intensity projection images reconstructed from vascular-phase CT imaging, hepatic arterial patency and catheter location were assessed. Using a combination of vascular- and perfusion-phase CT imaging, system dysfunction and clinical problems were evaluated.
Results
Dual-phase CT angiography was conducted 156 times. Stenosis and obstruction of the hepatic artery and catheter dislodgment were observed seven times in four patients and four times in three patients, respectively. Diagnostic accuracy using vascular-phase CT imaging was 100%. In addition, development of collateral blood supply to the liver and extrahepatic perfusion to the stomach were observed three times in three patients and twice in two patients, respectively. Overall, system dysfunction occurred 16 times in 12 patients, and system correction and treatment modification were required 11 times in 10 patients. In assessing system dysfunction and predicting clinical problems, the accuracy of dual-phase CT imaging was 100%.
Conclusion
Dual-phase CT angiography through the port-catheter system is helpful for assessing catheter system dysfunction and predicting clinical problems in HAI chemotherapy.
The liver is one of the most common sites for cancer metas-tases that result in significant morbidity and mortality (1). The efficacy of systemic chemotherapy for metastatic colo-rectal cancer has improved considerably in recent years using combinations of infusional 5-fluorouracil and leucov-orin with oxaliplatin or irinotecan (2,3), and the addition of biological agents such as bevacizumab, a monoclonal antibody targeting vascular endothelial growth factor, and cetuximab, a monoclonal antibody against epidermal growth factor receptor (4,5). Despite this progress in systemic treatments, long-term survival of patients with unresectable liver metastases remains short. Thus, alternative treatment strategies, such as combinations of hepatic arterial infusion (HAI) chemotherapy with systemic cyto-toxic chemotherapy (6–8), and HAI chemotherapy using newer agents (9–11), are being explored for the treatment of liver metastasis. Additionally, recent studies have reported that HAI chemotherapy results in an effective response in patients with advanced hepatocellular carcinoma (12–14). Thus, HAI chemotherapy is a promising treatment strategy for patients with different types of liver malignancies.
For effective HAI treatment, proper maintenance of port-catheter systems is of great importance, as inadequate drug distribution and catheter-related problems may reduce treatment response and increase local toxicity (15–18). For evaluating perfusion patterns of infused drugs, hepatic arterial perfusion scintigraphy and CT angiography through the port-catheter system have proven valuable. To properly evaluate the patency of the hepatic artery and the position of the indwelling catheter, digital subtraction angiography (DSA) through the port-catheter system or conventional angiography via a transfemoral approach is required (19–21). Therefore, both perfusion analysis and angiography are essential components of proper follow-up for HAI systems.
Recently, multislice CT has been developed as a non-invasive imaging modality for evaluation of vascular anatomy (22–26). When the multislice CT technique is applied, CT angiography through the port-catheter system can potentially be used not only for assessing perfusion of infused drugs but also for evaluating the condition of the hepatic artery and indwelling catheter. Based on this concept, using a 64-channel multislice CT, we have designed a dual-phase CT method that involves intra-arterial administration of contrast medium through the port-catheter system. In this technique, vascular images via the port-catheter system are reconstructed from thin-slice CT data in the early enhancement phase, and conventional perfusion images are acquired in the late enhancement phase. The objectives of the present study were to prospectively evaluate the efficacy of dual-phase CT angiography through the port-catheter system and to assess its clinical impact on predicting system correction and treatment modification in patients receiving HAI chemotherapy.
Material and Methods
Eligibility criteria
All patients were required to have unresectable malignant liver tumors, implanted port-catheter systems for HAI chemotherapy, and a performance status of ≤ 2 according to the Eastern Cooperative Oncology Group classification (27). Hematologic and chemistry parameters were required to be within the following limits: white blood cell count ≥ 3000/mm3, serum total bilirubin < 3.0 mg/dL, and serum creatinine ≤ 1.5 mg/dL. Minor extrahepatic disease confirmed by radiological examination or intraoperative findings was not considered an absolute contraindication if the liver was the predominant disease site. All patients provided informed consent prior to commencement of the examination. The study was approved by the ethics committee at our institution.
Catheter implantation procedure and HAI chemotherapy
Before implantation of the port-catheter system, angiography was performed for arterial road-mapping and arterial redistribution. When an aberrant hepatic artery was encountered, hepatic arterial blood flow was redistributed using coils (FPC35 Pt-Max and VortX; Boston Scientific, Natick, MA, USA; Tornado; Cook, Bloomington, IN, USA) to convert multiple hepatic arteries into a single arterial blood supply. If necessary, extrahepatic arterial branches arising from the hepatic artery and parasitic arteries with hepatopetal blood flow were also occluded using coils and/or a mixture of n-butyl cyanoacrylate (Histoacryl; Braun, Melsungen, Germany) and iodized oil (Lipiodol; Laboratorie Guerbet, Roissy, France). A port-catheter system was then implanted during a surgical procedure via the left axillary artery, or with a percutaneous approach via the right femoral artery. A long, tapered side-hole-type catheter composed of a 2.7-F, 20-cm-long distal shaft and a 5-F, 70-cm-long proximal shaft (Anthron P-U catheter; Toray, Tokyo, Japan: W-spiral catheter; Piolax Medical Devices, Yokohama, Japan) was inserted in the hepatic artery using the following methods: the distal shaft of the catheter with a side-hole was placed in the common hepatic artery and the tip of the catheter was fixed in the gastroduodenal artery using coils; the distal shaft was inserted distally into the hepatic artery and its side-hole was positioned proximally (28,29). The proximal end of the catheter was cut and connected to the port (Soph-A-Port; Sophysa, Orsay, France), which was implanted in the subcutaneous space. Chemotherapeutic agents were infused into the hepatic artery through the side-hole of the catheter.
HAI chemotherapy was initiated 2 to 14 days after catheter placement. The following chemotherapeutic agents were used: 5-fluorouracil (1000 mg/m2 weekly as a 5-h infusion) was administered to patients with liver metastases from colorectal and testicular cancer; 5-fluorouracil (330 mg/m2 weekly as a 2-h infusion), mitomycin C (2.7 mg/m2 biweekly as a bolus infusion), and epirubicin (30 mg/m2 every 4 weeks as a bolus infusion) were administered to patients with liver metastases from gastric, breast, and gallbladder cancer; and 5-fluorouracil (1000 mg/m2 weekly as a 5-h infusion) and cisplatin (6.7 mg/m2 weekly as a bolus infusion) were administered to patients with hepatocellular carcinoma and liver metastases from esophageal cancer. Patients received HAI chemotherapy until one of the following occurred: progressive liver disease, extra-hepatic progression that was predominant over the hepatic lesions, catheter dysfunction and/or complications that prevented further treatment, or excessive toxicity. In the event of a complete response, treatment was continued for an additional 3 months.
Dual-phase CT angiography and DSA through the port-catheter system
Patients were followed until the end of HAI chemotherapy. Dual-phase CT angiography and DSA through the port-catheter system were performed within 10 days after implantation of the catheter-port system and every 2 to 3 months thereafter to assess patency of the hepatic artery, position of the catheter, and perfusion pattern in the liver. Imaging was also performed when patients complained of any symptoms related to HAI of the chemotherapeutic agents.
Dual-phase CT angiography was performed using a 64-channel multislice CT scanner (Light Speed VCT; GE Healthcare, Milwaukee, WI, USA). The following CT parameters were used: a pitch of 0.984, a gantry rotation speed of 0.5 s, a detector collimation of 64 × 0.625 mm, 120 kV, auto mA (max 650 mA), a matrix of 512 × 512, and a field of view of 35 cm. A 24-gauge Huber-type needle (Coreless needle; Nipro, Osaka, Japan) was used for access to the implantable port. The contrast medium was diluted with normal saline to contain 100 mg I/mL of iopamidol (Iopamiron; Bayer Schering Pharma, Osaka, Japan), and 25 mL of the solution was injected via the implantable port at a rate of 0.7 mL/s during the following dual-phase CT scanning procedure. CT data acquisition began 6 s after the initiation of injection, and multiple sections encompassing the entire liver were obtained in a craniocaudal direction with an approximately 4-s scan time during a single breath-hold to evaluate configuration of the hepatic artery and vascular flow through the port-catheter system. After allowing breathing for 16 s, CT images were taken in the same range during an additional breath-hold to assess perfusion of the contrast media in the liver. The former and latter CT imaging was defined as the vascular phase and the perfusion phase, respectively. Contiguous axial images were reconstructed with a 5-mm thickness. Additionally, for three-dimensional (3-D) postprocessing, 0.625-mm axial images were obtained from CT data in each phase. In the vascular phase, maximum intensity projection (MIP) reconstructions were created with a 1808 view parallel to the longitudinal axis of the patient. If necessary, a volume-rendering technique was additionally used. In the perfusion phase, reformatted CT images were created in coronal and sagittal directions. The 3-D imaging reconstructions were generated on a commercially available workstation (Advantage Windows 4.3 and AW Sweet 2.0, GE Healthcare).
DSA was performed using manual injection of the contrast medium through the port-catheter system to confirm hepatic arterial patency and the position of the indwelling catheter. Images were acquired within 10 days after dual-phase CT angiography.
Image analysis of dual-phase CT angiography
Dual-phase CT angiography was assessed via a consensus of two experienced radiologists who were unaware of clinical data except for data about the catheter placement method used for each patient.
Initially, in vascular-phase CT images, patency of the hepatic artery and location of the indwelling catheter were evaluated using reconstructed MIP imaging. Volume-rendered imaging, original axial thin-slice CT images, and reformatted coronal and sagittal CT images were additionally used to assist evaluation. Patency of the hepatic artery, ranging between the common hepatic artery and proximal portions of the segmental hepatic artery, was classified into three categories: obstruction, stenosis, and normal patency. Stenosis was defined as narrowing of the vascular lumen exceeding 50%. Catheter dislodgment was assessed based on flow patterns and position of the catheter tip in vascular-phase MIP imaging, which was compared with an angiogram via the port-catheter system obtained just after implantation. Dislodgment was diagnosed as follows: when the splenic artery was seen with normal patency of the hepatic artery and the catheter tip was withdrawn, we judged that the side-hole of the catheter was withdrawn from the hepatic artery into the celiac arterial trunk; when the abdominal aorta was seen and the catheter tip was withdrawn, we judged that the side-hole of the catheter was withdrawn into the aorta; when only either the right or left hepatic artery was observed with no visualization of the proper hepatic artery and the catheter tip was advanced, we judged that the catheter was advanced distally into each lobar hepatic artery. When the catheter tip was considered to be appropriately located while the splenic artery was seen with normal patency of the hepatic artery, we judged that the catheter was not dislodged and that the contrast medium had flowed over the common hepatic artery into the splenic artery due to an excessive injection rate or the influence of the cardiac cycle. When the flow of the contrast medium via the port-catheter system was satisfactorily observed while minor movement of the catheter tip was suspected, it was managed as having no catheter dislodgment. These interpretations were correlated with the findings of DSA through the port-catheter system, and the diagnostic value of stenosis and obstruction of the hepatic artery and catheter dislodgment was assessed.
Subsequently, in the combination vascular- and perfusion-phase CT images, dysfunctions of the port-catheter system were evaluated. Perfusion abnormalities via the port-catheter system were assessed using axial, coronal, and sagittal reformatted perfusion-phase CT images. If intrahepatic perfusion defects and/or extrahepatic perfusion were observed, vascular-phase CT imaging was used to confirm hepatic arterial obstruction, catheter dislodgment, and development of extrahepatic vessels. When intrahepatic perfusion defects were seen on perfusion-phase CT imaging with normal patency of the hepatic artery on vascular-phase MIP imaging, development of collateral blood supply to the liver was suspected. When extrahepatic perfusion reaching the stomach beyond the duodenum was observed on perfusion-phase CT imaging with extension of many vessels into the stomach and duodenum on vascular-phase MIP imaging, system dysfunction potentially caused by gastroduodenal ulcer or gastroduodenitis was presumed. When extrahepatic perfusion was seen only in part of the duodenum on perfusion-phase CT imaging, it was not considered to be system dysfunction, as such perfusion was not necessarily associated with gastroduodenal toxicity (30). These interpretations were correlated with clinical symptoms and imaging findings of DSA through the port-catheter system, additional angiography via the transfemoral route, and endoscopy, all of which were performed to investigate catheter system dysfunction and to resolve any problems.
Statistical analysis
In vascular-phase CT imaging, detection of hepatic arterial stenosis and obstruction, as well as catheter dislodgment, was evaluated. With the DSA results used as the standard of reference, the accuracy, sensitivity, specificity, positive predictive value, and negative predictive value were calculated.
The diagnostic value in assessing dysfunction of the port-catheter system was analyzed using combined vascular- and perfusion-phase CT imaging results. Based on the findings of DSA through the port-catheter system, conventional angiography, and endoscopy, as well as clinical symptoms, the accuracy, sensitivity, specificity, positive predictive value, and negative predictive value were calculated. Additionally, the impact of dual-phase CT angiography on predicting clinical problems was evaluated. Clinical problems were defined as cases that actually required system correction and treatment modification. Using cases with actual clinical problems as the reference, the accuracy in predicting clinical problems was calculated.
Results
Between January 2007 and April 2009, 47 patients (age range, 46–81 years; mean age, 63.6 years) at our institution who received HAI chemotherapy using the port-catheter system for malignant liver tumors were entered into this study. Patient characteristics are listed in Table 1. Forty-three patients had liver metastases from the following primary tumors: colorectal cancer (n = 20), gastric cancer (n = 14), esophageal cancer (n = 4), breast cancer (n = 3), gallbladder cancer (n = 1), and testicular cancer (n = 1). Four patients had hepatocellular carcinoma.
Patient characteristics
The distal shaft of a long tapered catheter with a side-hole was placed in the common hepatic artery and the tip of the catheter was fixed in the gastroduodenal artery using coils
The distal shaft of a long tapered catheter was inserted distally into the hepatic artery and its side-hole was positioned proximally
ECOG, Eastern Cooperative Oncology Group; n, number of patients
Dual-phase CT angiography through the port-catheter system was successfully performed during HAI chemotherapy in all 47 patients. Overall, dual-phase CT angiography was conducted 156 times (range, 1–10 times; mean, 3.3 times), with a mean follow-up period of 236 days (range, 57–741 days).
Evaluation of hepatic arterial patency and catheter location using vascular-phase CT imaging
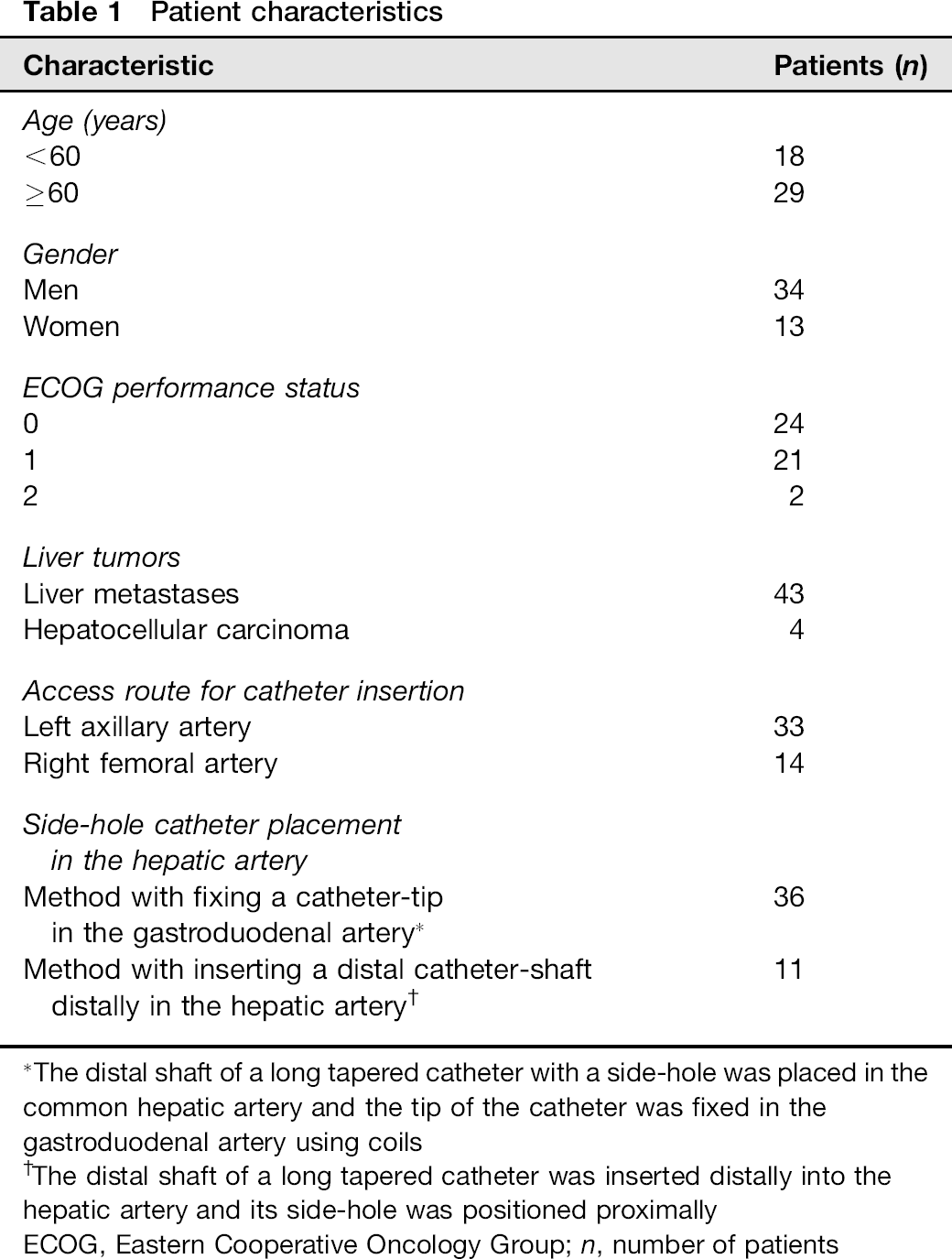
In all 156 CT examinations, hepatic arterial patency was correctly assessed using MIP imaging in the vascular phase; these results were equivalent to those obtained using DSA through the port-catheter system. Obstruction of the proper hepatic artery was identified 5 months after initiation of chemotherapy in one patient, and HAI chemotherapy was subsequently terminated. Stenosis of the hepatic artery was observed six times in three patients as follows: stenosis of the common hepatic artery was seen 8 months after initiation of chemotherapy in one patient, and HAI chemotherapy was discontinued after dissection of the common hepatic artery was observed via reformatted sagittal and coronal CT images (Fig. 1); stenosis of the proper hepatic artery was seen 3 months after initiation of treatment in one patient; and stenosis of both the right and left hepatic arteries was observed at the initial examination and at 3, 6, and 9 months in subsequent exams in one patient, which did not lead to discontinuation of HAI chemotherapy. In the remaining 149 examinations, normal patency was observed in the hepatic artery.
An 81-year-old woman with stenosis and dissection of the common hepatic artery. (a) 
Catheter dislodgment was correctly evaluated using vascular-phase MIP imaging. On four examinations in three patients, catheter dislodgment could be detected using vascular-phase CT imaging as well as DSA through the port-catheter system. In one patient, withdrawal of the side-hole of the catheter from the common hepatic artery to the celiac arterial trunk was observed 9 months after initiation of chemotherapy (Fig. 2), and the catheter was thus replaced. In one patient, withdrawal of the catheter into the celiac arterial trunk was seen 3 and 6 months after initiation of chemotherapy, which required chemotherapy dosage reduction. In another patient, advancement of the side-hole of the catheter from the proper hepatic artery into the right hepatic artery was observed 3 months after initiation of chemotherapy; the left hepatic artery was subsequently embolized using coils to convert the hepatic arterial blood flow into the right hepatic artery. On seven examinations in four patients, while the catheter tip was not withdrawn, the splenic artery was observed with normal patency of the hepatic artery on vascular-phase MIP imaging 3, 6, 9, and 10 months after initiation of chemotherapy in each patient, and thereafter in two of these patients. We judged that the catheter was not dislocated and that these were caused by an overflow of the contrast medium. Subsequently, using DSA through the port-catheter system, it was confirmed that these cases, in which the flow into the splenic artery was not seen on the appropriate control by manual injection, had no catheter dislodgment. On the remaining 145 examinations, appropriate catheter location was confirmed using vascular-phase CT imaging.
A 63-year-old woman with catheter dislodgment. (a) Angiogram via the port-catheter system obtained just after implantation shows a catheter tip inserted distally into the gastroepiploic artery (black arrow), a side-hole of the catheter placed in the common hepatic artery (white arrow), and a distal catheter shaft fixed within the gastroduodenal artery using coils (arrowheads); (b) In a vascular-phase 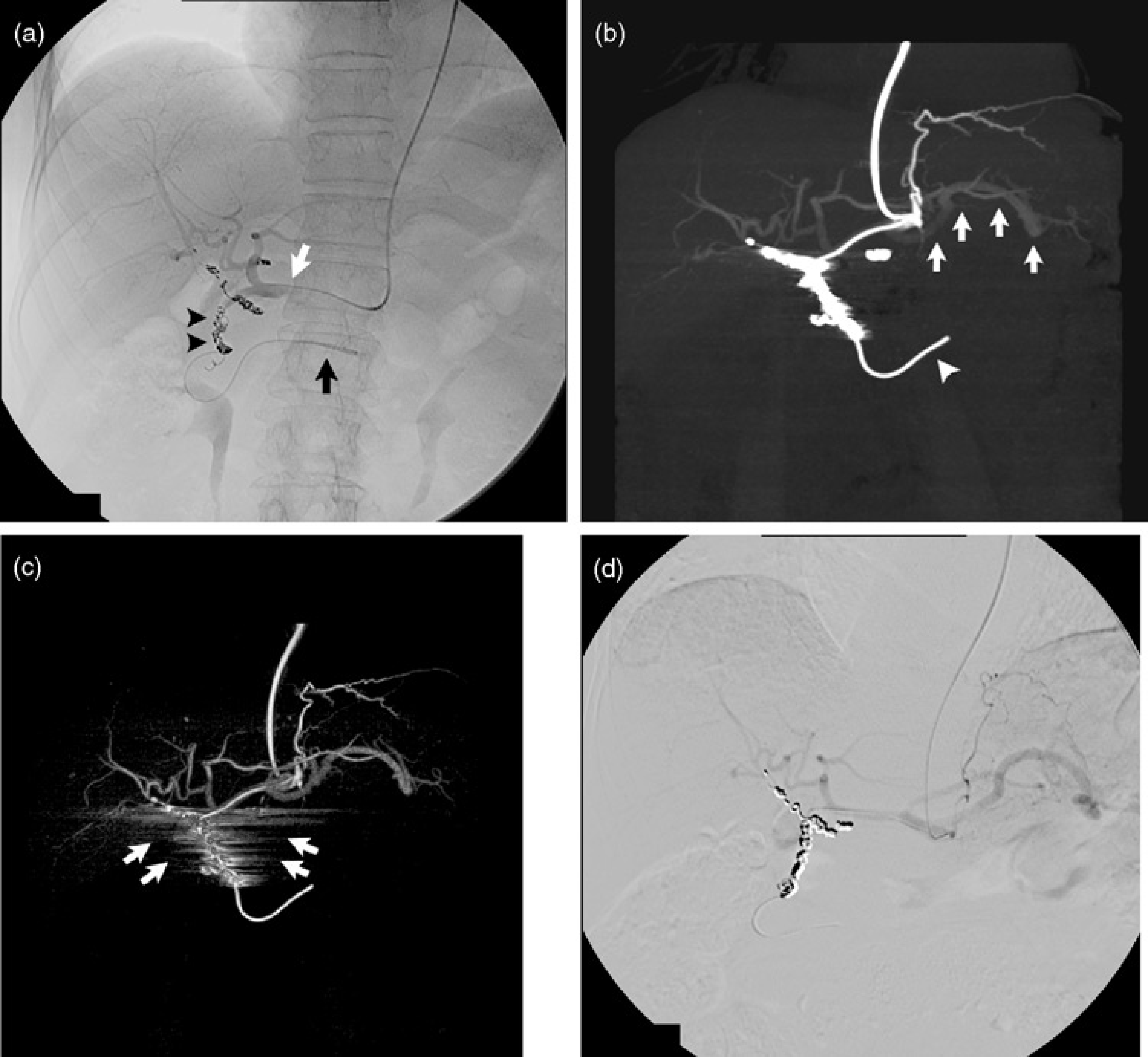
Volume-rendered imaging in the vascular phase was helpful to assess vascular configuration (Figs. 1 and 2). In several cases, however, an imaging artifact was conspicuously revealed around metallic coils in volume-rendering reconstructions (Fig. 2), while less pronounced on MIP processing; this may be a potential disadvantage for evaluating patency of the hepatic artery around coils.
In assessing hepatic arterial patency and catheter location, the accuracy, sensitivity, specificity, positive predictive value, and negative predictive value of vascular-phase CT imaging compared to DSA were all 100%. The diagnostic value of vascular-phase MIP imaging was equivalent to that of DSA through the port-catheter system.
Evaluation of system dysfunction using dual-phase CT imaging
Assessment of catheter system dysfunction using a combination of vascular- and perfusion-phase CT imaging is shown in Table 2. Dysfunction of the port-catheter system, which was accurately identified using dual-phase CT angiography, occurred 16 times in 12 patients.
Assessment of system dysfunction using dual-phase CT angiography
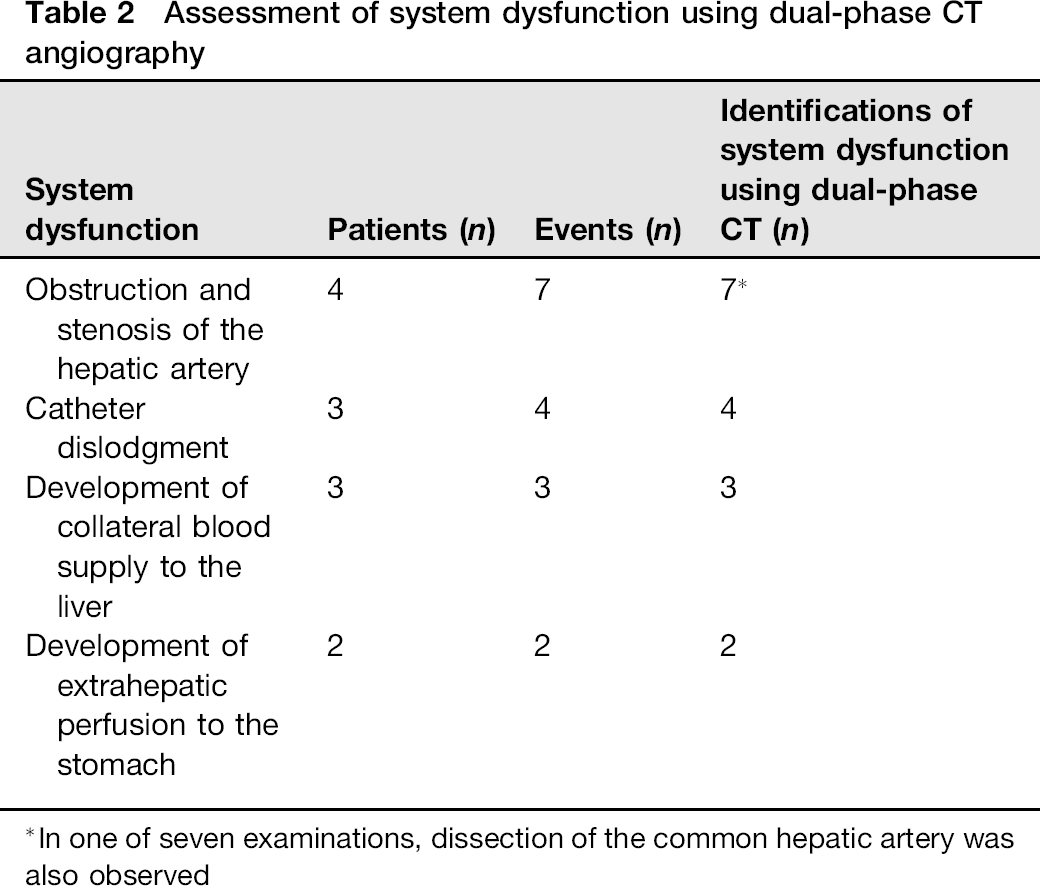
In one of seven examinations, dissection of the common hepatic artery was also observed
Using dual-phase CT angiography, obstruction and stenosis of the hepatic artery was accurately identified seven times in four patients, in one of whom dissection of the common hepatic artery was observed with stenosis of the common hepatic artery (Fig. 1). Catheter dislodgment was also accurately identified four times in three patients (Fig. 2).
In three patients, development of collateral blood supply to the liver, resulting in an intrahepatic perfusion defect in the right subphrenic area, was suspected using perfusion-phase CT imaging 2, 5, and 10 months after initiation of chemotherapy. Subsequently, angiography via the transfemoral approach was performed, and the right inferior phrenic artery was confirmed as a collateral vessel to the liver (Fig. 3). It was then embolized using a mixture of n-butyl cyanoacrylate and iodized oil to correct drug distribution.
A 61-year-old man with development of collateral blood supply to the liver, (a) A reformatted coronal perfusion-phase CT image shows an intrahepatic perfusion defect in the right subphrenic area (arrows); (b) Angiogram of the right inferior phrenic artery shows collateral blood supply to the liver tumor (arrows)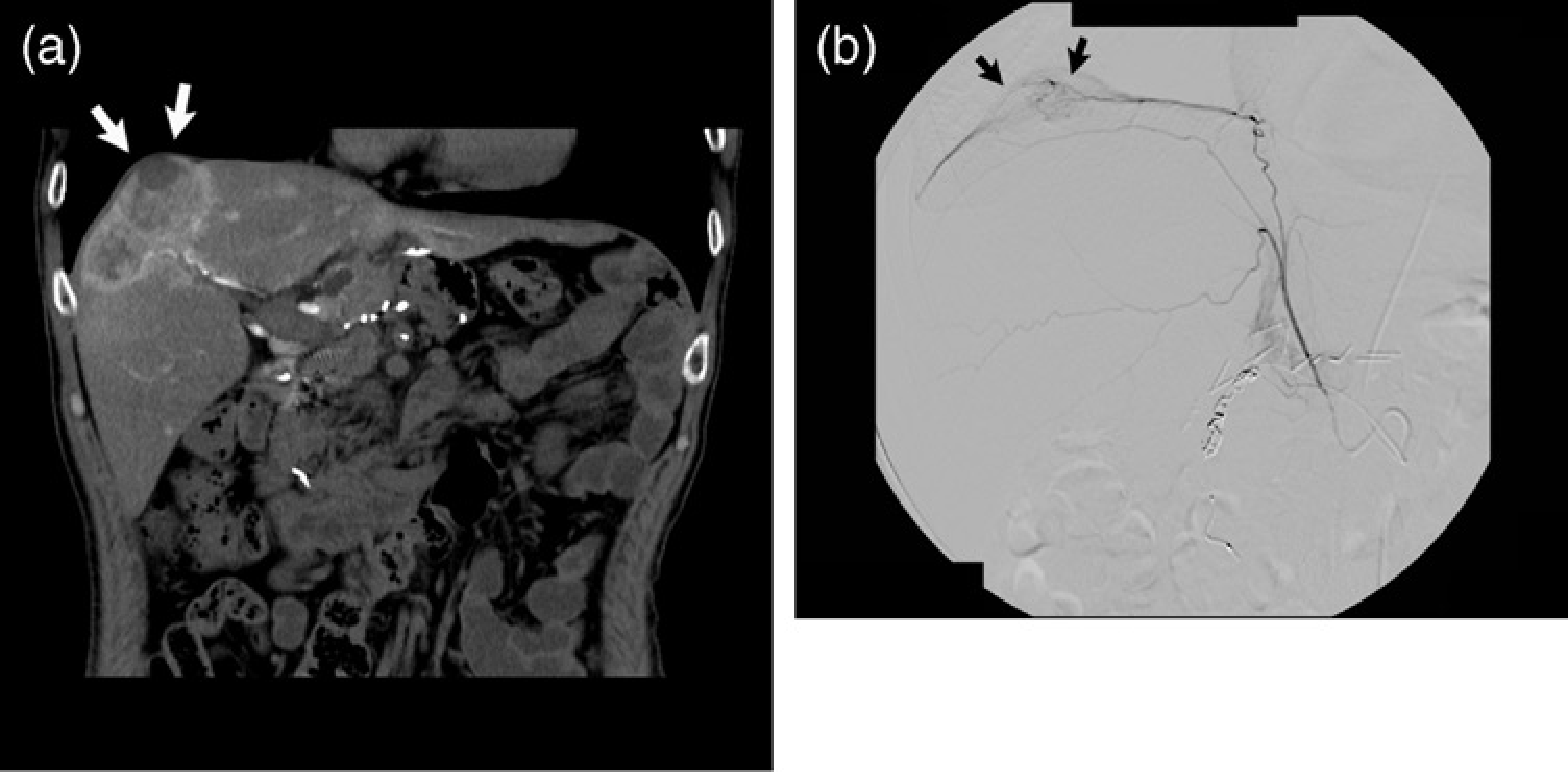
In two patients, a wide range of extrahepatic perfusion was observed not only in the duodenum but also in the antrum of the stomach on perfusion-phase CT imaging 6 and 12 months after initiation of chemotherapy. Development of many gastroduodenal arterial branches was also observed on vascular-phase MIP imaging (Fig. 4). We judged these to be system dysfunction potentially associated with gastric toxicity. Based on this finding, gastric endoscopy was performed and gastric ulcers and acute gastritis were diagnosed. One of these patients complained of epigastric discomfort during HAI, and angiography was subsequently performed showing the development of collaterals to the stomach, which were then embolized using coils. In another patient who complained of anorexia, dosage reduction of chemotherapeutic drugs was required. In the other 14 patients, on 46 examinations, extrahepatic perfusion was observed in part of the duodenum and the pancreatic head. These were judged as cases without system dysfunction, and unresolved gastric toxicity was not observed during treatment.
A 63-year-old man with extrahepatic perfusion in the stomach resulting in gastric ulcer. (a) A perfusion-phase CT image shows extrahepatic perfusion in the gastric antrum (arrows) beyond the duodenum (arrowhead); (b) A vascular-phase 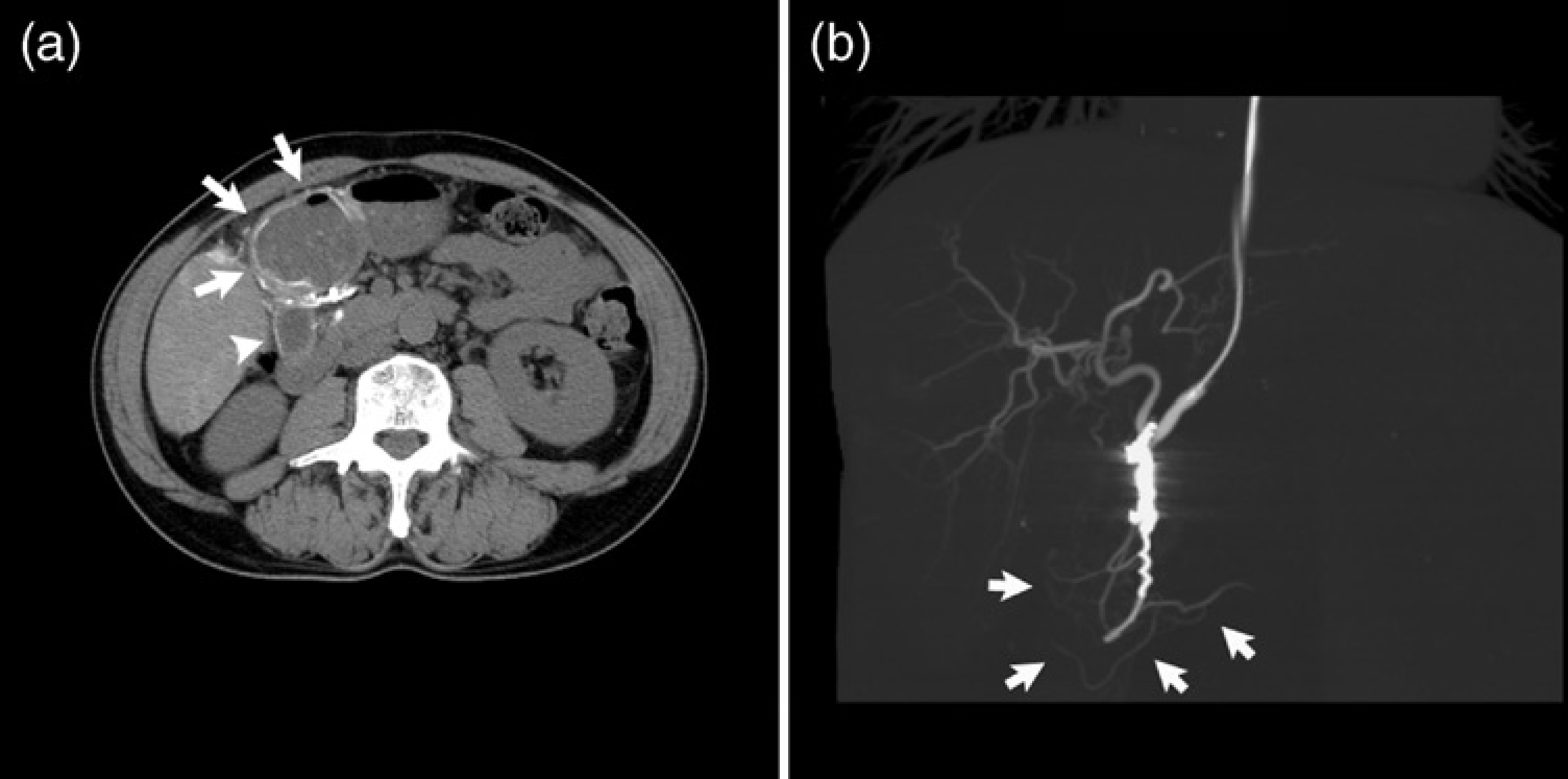
In assessing system dysfunction, the accuracy, sensitivity, specificity, positive predictive value, and negative predictive value of dual-phase CT angiography were all 100%.
Prediction of clinical problems using dual-phase CT angiography
Clinical problems related to dysfunction of the port-catheter system are presented in Table 3. In 10 patients with system dysfunction, actual management was required for system correction and treatment modification. Clinical problems were correctly identified 11 times in these patients using dual-phase CT angiography, and adjustment of the catheter system and treatment modification was performed. In the other 145 exams in which the port-catheter system was deemed to be functioning correctly, no adjustments were required during HAI chemotherapy. Thus, clinical problems were accurately identified and assessed using dual-phase CT angiography in all cases; the accuracy in predicting clinical problems was 100%.
Prediction of clinical problems using dual-phase CT angiography
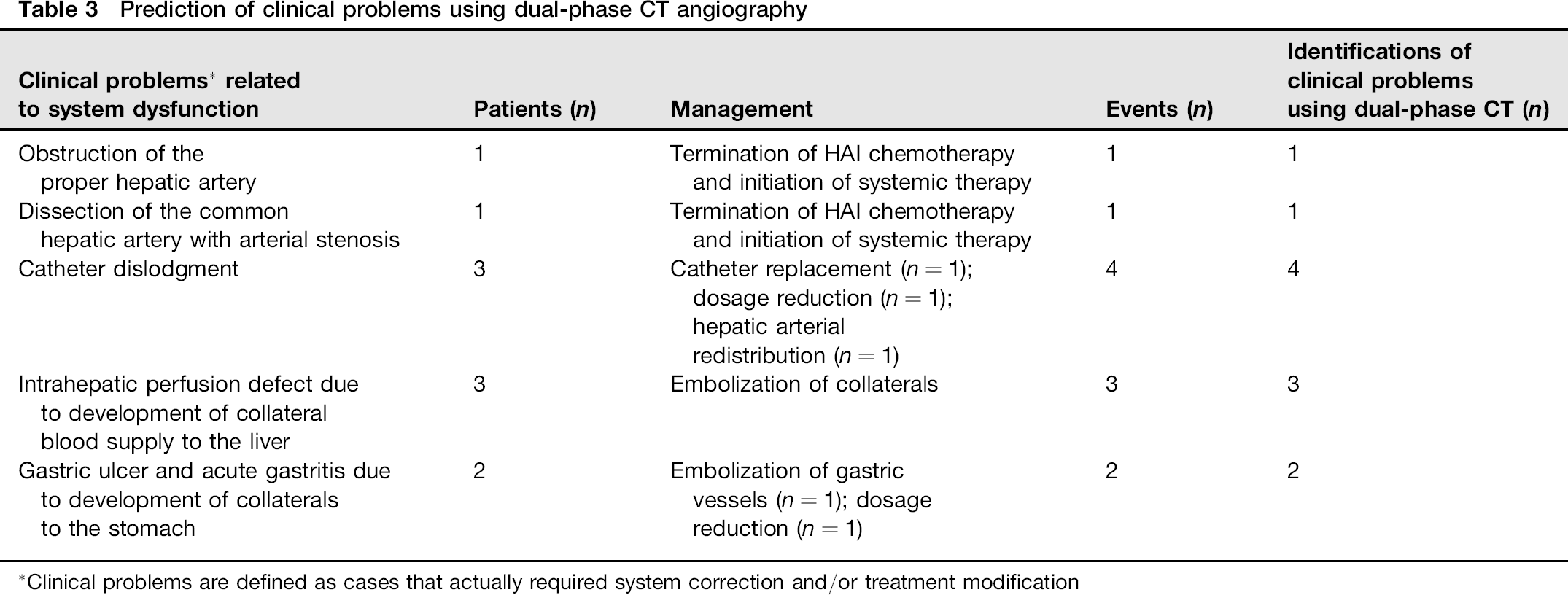
Clinical problems are defined as cases that actually required system correction and/or treatment modification
Discussion
The present results demonstrate that dual-phase CT angio-graphy through the port-catheter system is useful for follow-up after administration of HAI chemotherapy via the port-catheter system. This type of angiography can be used not only to assess drug distribution, but also to evaluate hepatic arterial patency and catheter location instead of DSA through the port-catheter system.
In patients undergoing HAI chemotherapy for malignant liver tumors, dysfunction of the port-catheter system occasionally occurs, resulting in treatment failure. Therefore, it is important to promptly identify and resolve these problems. To evaluate sites of perfusion abnormalities during HAI chemotherapy, CT angiography through the port-catheter system is appropriate (20,21). This is achieved with intra-arterial administration of contrast medium through the indwelling catheter and image acquisition at a single phase in which the hepatic parenchyma is sufficiently enhanced to evaluate intrahepatic perfusion. However, this conventional CT angiography is unsuitable for demonstrating the configuration of the hepatic artery due to poor contrast between vessels and enhanced hepatic parenchyma. In general, DSA through the port-catheter system has to be performed to assess hepatic arterial patency and catheter location.
Sone et al. first reported that obstruction and stenosis of the hepatic artery were observed using MIP processing obtained from multislice CT angiography through the port-catheter system (22). However, with this method, a 5-min waiting period is required after the first scan of conventional CT angiography to eliminate contrast materials in the hepatic parenchyma. In addition, visualization of the hepatic artery may be decreased due to the residual enhancement in the hepatic parenchyma.
In the dual-phase CT angiography through the port-catheter system used in the present study, vascular-phase CT imaging is performed 6 s after initiation of injection, followed by perfusion-phase CT imaging at a 16-s delay after scanning the vascular phase. Thus, a long waiting period is not required. On vascular-phase CT imaging, the hepatic artery was clearly revealed using MIP processing, with good contrast between the hepatic artery and the less enhanced hepatic parenchyma. In the present study, obstruction and stenosis of the hepatic artery were accurately evaluated using vascular-phase MIP imaging with results equivalent to those obtained using DSA through the port-catheter system. These results indicate that vascular-phase CT imaging can be utilized to assess hepatic arterial patency instead of DSA through the port-catheter system. Moreover, in the present study, catheter dislodgment was correctly identified on vascular-phase MIP imaging using findings with an inflow to the splenic artery or aorta and dislocation of the catheter tip. Although the contrast medium flowed over the common hepatic artery into the splenic artery in several cases with no catheter dislocation, this could be distinguished from catheter dislodgment based on the position of the catheter tip. As a result, the location of the side-holed catheter was accurately assessed in all cases using vascular-phase MIP imaging. We consider vascular-phase CT imaging to be a reliable method for assessing catheter dislodgment, similar to DSA through the port-catheter system.
Volumetric 3-D rendering is a useful technique for demonstrating vascular configuration. In the present study, however, an imaging artifact was remarkably observed around metallic coils in volume-rendered imaging in several cases, while it was less so on MIP imaging. This artifact may become a potential drawback in evaluating patency of the hepatic artery around coils, as metallic coils are frequently used for catheter placement. Therefore, we consider that MIP processing is suitable for assessing patency of the hepatic artery in patients with port-catheter systems.
In perfusion-phase CT imaging, which is the same procedure that is performed for conventional single-phase CT angiography, sites of intra- and extrahepatic perfusion abnormalities can be clearly identified. In the present study, perfusion defects in the liver due to development of collateral blood supply and extrahepatic perfusion in the stomach resulting in gastric toxicity could be identified using perfusion-phase CT imaging. Using a combination of vascular- and perfusion-phase CT imaging, an accurate rate (100%) of assessment of port-catheter system dysfunction was obtained. Based on these findings, clinical problems were resolved using appropriate management via the HAI system and treatment. In predicting clinical problems requiring system correction and treatment modification, the accuracy was 100% using dual-phase CT angiography. These results indicate that dual-phase CT angiography is greatly advantageous for administering safe and effective HAI chemotherapy.
Several recent studies have reported that 3-D reconstruction from multislice CT data with intravenous administration of contrast medium is useful for preoperative evaluation of hepatic arterial anatomy (23–26). Using this technique, hepatic arterial patency can potentially be assessed. However, in intravenous enhanced CT angiography, many arterial branches of abdominal organs overlap the hepatic artery, which may hide abnormalities of the hepatic artery. In addition, since the side-hole of the implanted catheter is not visible and blood flow through the port-catheter system is not depicted using this technique, the position of the side-hole of the catheter cannot be evaluated. Therefore, we consider vascular-phase CT imaging through the port-catheter system to be superior to intravenous CT angiography in assessing the condition of the hepatic artery and the indwelling catheter.
The present study has some limitations. First, in vascular-phase MIP imaging, overflow of the contrast medium may cause false-positive judgment of catheter dislodgment in cases with minor movement of the catheter that does not influence the drug distribution, although no such cases were observed in the present study. Therefore, when the splenic artery is observed with normal patency of the hepatic artery on vascular-phase MIP imaging, the position of the catheter tip should be carefully assessed. Second, an intrahepatic perfusion pattern on perfusion-phase CT angiography may differ from the actual drug distribution, since the injection rate using CT angiography is higher than that used during continuous drug infusion. In the present study, abnormal perfusion patterns on perfusion-phase CT imaging were well correlated with actual clinical problems. However, when a problem that cannot be explained by CT angiography findings is observed, addition of hepatic arterial perfusion scintigraphy should be considered. Third, in the present study, the occurrence of dysfunction of the port-catheter system was small. A larger number of these events would be necessary to verify the present results.
In conclusion, this study demonstrated that dual-phase CT angiography through the port-catheter system is a reliable method for assessing dysfunction of the port-catheter system and predicting system correction and treatment modification in patients receiving HAI chemotherapy. With regard to identification of stenosis and obstruction of the hepatic artery and catheter dislodgment, vascular-phase CT angiography can be utilized instead of DSA through the port-catheter system. We believe that dual-phase CT angiography is a helpful follow-up examination in the management of port-catheter systems.