
Abstract
Background
The smallest diagnostically appropriate amount of contrast medium should be used in coronary computed tomography angiography (CCTA).
Purpose
To investigate the feasibility of prospectively ECG-triggered high-pitch CCTA using 30 mL of 270 mg I/mL contrast material, 80 kVp, and iterative reconstruction (IR).
Material and Methods
Eighty-two consecutive patients underwent CCTA with a prospectively ECG-triggered high-pitch protocol. Forty-three patients were examined at 100 kVp with filtered back projection after 60 mL of 370 mg I/mL contrast material was administered. Another 39 patients were examined at 80 kVp with IR after 30 mL of 270 mg I/mL contrast material was administered. Subjective and objective image quality was evaluated for each patient. Radiation doses were estimated and compared.
Results
Mean attenuation, noise and signal-to-noise ratio in 80 kVp group were significantly lower than in 100 kVp group (all P < 0.05), while there was no significant difference in contrast-to-noise ratio (CNR), although a trend towards a lower CNR in 80 kVp group was observed (P = 0.099). The subjective image quality between the two groups was not significantly different (P = 0.905). The effective dose and iodine load in 80 kVp group were reduced by 54% and 64%, respectively, when compared with 100 kVp group.
Conclusion
Prospectively ECG-triggered high-pitch CCTA at 80 kVp with 30 mL of 270 mg I/mL contrast material and IR is feasible for patients with BMI less than 25 kg/m2 and reduces radiation dose and iodine load when compared with the standard CCTA protocol.
Introduction
Coronary computed tomography angiography (CCTA) has become a widely used non-invasive imaging technique to assess coronary artery disease (CAD) in clinical practice (1–3). However, the relatively high radiation dose associated with CCTA has raised concerns. Recently, various strategies of radiation dose reduction have been developed, such as prospective electrocardiogram (ECG)-triggering, high-pitch acquisition, low tube voltage, and automated tube potential selection (4,5). Schuhbaeck et al. (6) have reported that radiation dose from CCTA could be reduced to less than 0.1 mSv using prospectively ECG-triggered high-pitch CCTA at 80 kVp in selected patients.
In addition, contrast medium-induced nephropathy (CIN) is associated with a significant risk for permanent renal failure and death (7–9). Recent evidence suggests that the risk of CIN from intravenously administered contrast medium, if any, is probably smaller than traditionally thought (10). Nevertheless, the smallest diagnostically appropriate amount of contrast medium should be used to further minimize the risk (11,12). Even though there is no conclusive evidence that the incidence of CIN is lower in patients injected with isosmolar contrast material (IOCM) when compared with low-osmolar contrast material (LOCM) (13), reducing iodine concentration is one strategy to decrease overall iodine load.
Recently, 270 mg I/mL IOCM has been used in CCTA at 80 kVp and ECG-triggered sequential acquisition for patients with body mass index (BMI) less than 25 kg/m2 to confer a significant reduction in radiation dose and contrast material (14). The estimated mean volume of contrast material per patient was about 57 mL in that study. It has been reported that high-pitch CCTA can be performed with 30 mL of contrast medium without affecting vessel enhancement (15). Accordingly, we hypothesized that a prospectively ECG-triggered high-pitch protocol should be feasible using 30 mL contrast material with a concentration of 270 mg I/mL at 80 kVp. The aim of our study was to investigate the feasibility, image quality, and radiation dose of CCTA acquired using a prospectively ECG-triggered high-pitch protocol with low tube voltage and 30 mL contrast material with a concentration of 270 mg I/mL.
Material and Methods
Study subjects
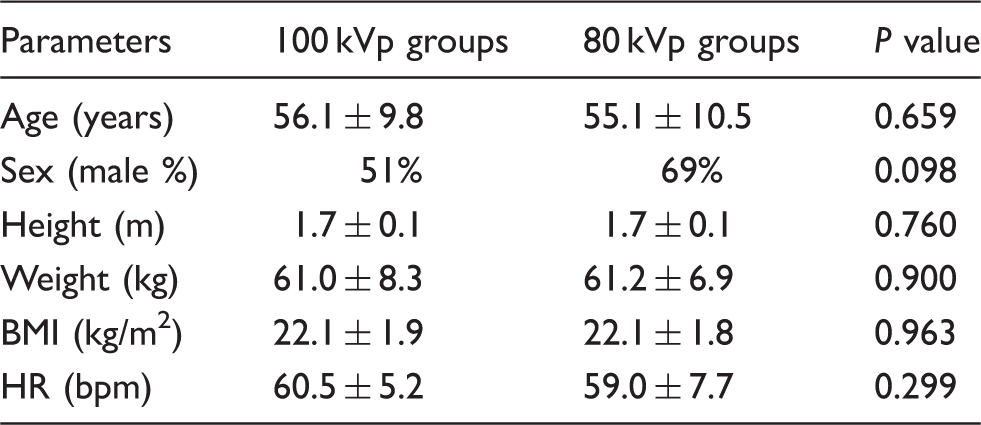
This prospective study was approved by the local ethics board and written informed consent was obtained from all patients. From June to November 2013, a total of 95 patients with BMI ≤ 25 kg/m2 were enrolled in this study. Patients with BMI ≤ 25 kg/m2, heart rate (HR) ≤ 70 beats per minute (bpm), and stable sinus rhythm were included. All patients had been referred to CCTA for evaluation of suspected or known CAD. Patients with an allergy to iodinated contrast agent, cardiac arrhythmia, HR > 70 bpm when performing CCTA scanning, renal insufficiency (GFR < 90 mL/min/1.73m2), pregnancy, coronary artery bypass grafts, and coronary artery stent implantation were excluded. A range of 25–50 mg of metoprolol was (Lopressor) administered orally to patients with HR higher than 70 bpm 1 h prior to their examination when no contraindications were present. Eight patients with HR > 70 bpm were excluded despite oral administration of metoprolol. Five patients with resting HR ≤ 70 bpm that increased to >70 bpm during CCTA were excluded. Finally, 82 consecutive patients (33 women, 49 men; mean age, 56 ± 10 years; age range, 35–84 years) with BMI < 25 kg/m2 and HR < 70 bpm participated in this study. Among the 82 patients, metoprolol was used in 18 patients (7 patients in 100 kVp group and 11 patients in 80 kVp group). The 82 patients were randomly assigned to one of two groups based on their scanning date (i.e. odd numbered days for protocol A and even numbered days for protocol B). Forty-three patients (21 women, 22 men; mean age, 56 ± 10 years; age range, 36–77 years) underwent CCTA with protocol A (100 kVp, 60 mL of 370 mg I/mL iodinated contrast material) and 39 patients (12 women, 27 men; mean age, 55 ± 10 years; age range, 35–84 years) underwent CCTA with protocol B (80 kVp, 30 mL of 270 mg I/mL iodinated contrast material).
CT examination and contrast injection protocol
All examinations were performed on a second-generation dual-source CT system (Definition Flash, Siemens Healthcare, Forchheim, Germany) with stellar detectors, which can reduce electronic noise and improve spatial resolution compared with conventional detector technology (16). Image acquisition was performed in prospectively ECG-triggered high-pitch mode and started at 60% of the R-R interval. The patients were examined at 100 kVp and 80 kVp for groups A and B, respectively. Automatic tube current modulation (CARE Dose 4D; Siemens Healthcare) was used for all CT acquisitions with a quality reference tube current-time product of 370 mAs. Except for tube voltage, the other acquisition parameters were kept constant as follows: tube rotation time, 0.28 s; pitch, 3.4; collimation, 0.6 mm × 64 × 2.
An 18-gauge IV cannula was placed in a superficial vein in the antecubital fossa. In protocol A, contrast enhancement was achieved by injecting 60 mL Iopamiron (Bayer HealthCare Pharmaceuticals, Berlin, Germany, 370 mg I/mL) at 5 mL/s followed by a 40 mL saline flush at 5 mL/s. In protocol B, contrast enhancement was achieved by injecting 30 mL Visipaque, GE Healthcare, Princeton, NJ, USA, 270 mg I/ml at 5 mL/s followed by a 40 mL saline flush at 5 mL/s. The bolus-tracking technique was used with one circular region of interest (ROI) positioned in the root of the ascending aorta (AA). Image acquisition was automatically started 4 s after the signal attenuation in the ROI reached the pre-defined threshold of 100 Hounsfield units (HU).
CT image reconstruction
The enhanced images were reconstructed with 0.75 mm slice thickness and 0.6 mm increment. The images in 100 kVp group were reconstructed with filtered back projection (FBP) algorithm and images in 80 kVp group with sinogram-affirmed iterative reconstruction (SAFIRE, Siemens Healthcare) algorithm. FBP series were reconstructed with the B26f kernel and SAFIRE series with the corresponding I26f kernel. For the SAFIRE algorithm, five presets (strength 1–5) are available for adapting the noise model and controlling image impression and noise reduction. As recommended by the manufacturer, a medium strength level of I3 was used.
Image analysis
Quantitative image quality: All datasets were transferred to a MultiModality Workplace (MMWP, Siemens Healthcare) for evaluation. To evaluate objective image quality under each protocol, one observer measured intravascular attenuation and standard deviation (SD) within circular ROIs on reconstructed 0.75 mm transverse CT images. ROIs were drawn in the ascending aorta at the level of the left main coronary artery (LMA), proximal right coronary artery (RCA), proximal LMA, proximal left anterior descending artery (LAD), and proximal left circumflex artery (LCX). The attenuation of the adjacent perivascular tissue was also measured. ROIs were drawn as large as possible while avoiding calcifications, plaques, and stenos. Image noise was defined as the standard deviation of the CT attenuation value within the ROI placed in the ascending aorta. The signal-noise-ratio (SNR) and contrast-noise-ratio (CNR) were calculated as follows (17–19):
Qualitative image analysis: All datasets were transferred to Syngo.via (Siemens Healthcare) for curved planar reformations (CPR). To evaluate subjective image quality, two experienced cardiovascular radiologists independently reviewed axial CT images and CPRs. Coronary arteries were divided into 15 segments for analysis of CCTA data based on the American Heart Association (20). The image quality of each segment was evaluated on a 4-point scale (Fig. 1) as follows (21): A score of 1 corresponded to a lack of vessel wall definition due to marked motion artifact, poor vessel opacification, prominent structural discontinuity, or high image noise rendering the segment non-diagnostic; a score of 2 corresponded to some motion artifacts or image noise, fair vessel opacification, or minimal structural discontinuity; a score of 3 corresponded to minor motion artifacts or image noise, good vessel opacification, and no structural discontinuity; and a score of 4 corresponded to the absence of motion artifacts or minimal noise, excellent vessel opacification, and no structural discontinuity. Scores 2–4 were considered diagnostic image quality. In addition, the two radiologists independently assessed the presence of coronary artery stenosis ≥50% by reviewing the axial contrast-enhanced CT images and CPRs. In the event of observer disagreement, another reading session was convoked to reach an agreement.
Curved planar reformations (CPR) from the two groups illustrating the image quality scoring system used in this study. (a) A 100 kVp CCTA study which was given a score of 1 due to marked motion artifact in segment 2. (b) An 80 kVp CCTA study which was given a score of 2 because of mild motion artifact in segment 2. (c) A 100 kVp CCTA study which was given a score of 3 due to mild blurring of contours in segments 2 and 3. (d) An 80 kVp CCTA study which was given a score of 4.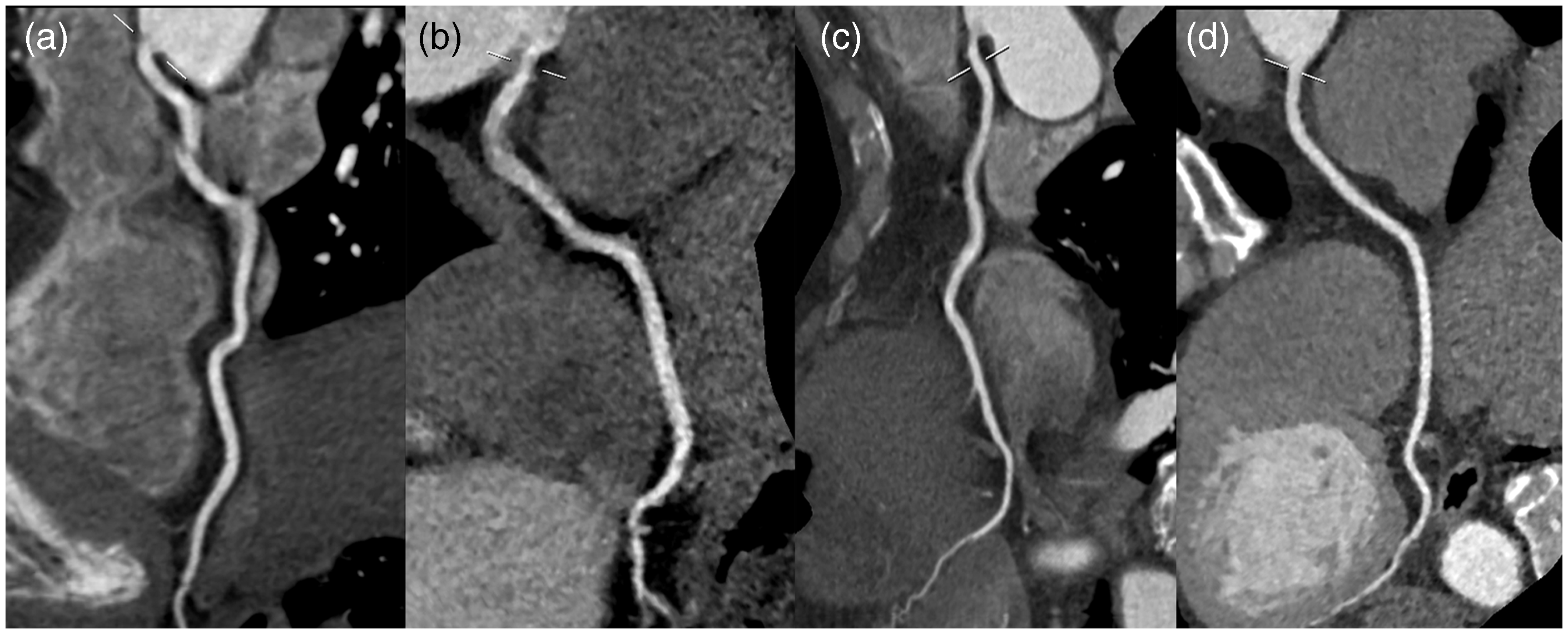
Injection-associated discomfort
The intensity of contrast injection-associated discomfort, defined as warmth, coldness, and pain, was subjectively rated by patients in both protocol groups on a 3-point scale: none; mild; or severe (22).
Radiation dose estimation
To estimate the radiation dose, we recorded volume CT dose index (CTDIvol) and dose length product (DLP) for each patient. The effective dose (ED) was calculated by multiplying DLP by a conversion factor for the chest (0.014 mSv × mGy–1 × cm–1) according to the European Working Group for Guidelines on Quality Criteria in CT (23). Additionally, the size-specific dose estimate (SSDE) was calculated. SSDE is regarded to provide an approximation of the dose absorbed by the individual patient from CT examination (24). SSDE is equal to CTDIvol multiply by size-dependent conversion factors (fsize) (24). In our study, the fsize of each patient was obtained by searching the table provided by AAPM Report 204 after measuring anteroposterior and lateral dimensions from the scout or axial images reconstructed with full field of view (24,25).
Statistical analysis
Statistical analyses were performed using the SPSS software version 16.0 (SPSS Inc. Chicago, IL, USA). Quantitative variables were expressed as mean ± SD, while categorical variables were expressed as frequencies or percentages. The Mann-Whitney test was used to compare categorical characteristics. An independent sample t-test was used to compare continuous variables. Kappa analysis was used to assess the inter-observer agreement of the subjective image quality evaluation and for the assessment of coronary artery stenosis. A k value of less than 0.20 indicated poor agreement; a k value of 0.21–0.40, fair agreement; a k value of 0.41–0.60, moderate agreement; a k value of 0.61–0.80, good agreement; and a k value of 0.81–1.00, very good agreement. The frequency of discomfort was compared between the two contrast media groups using Fisher’s exact test. P values < 0.05 were regarded as significant.
Results
Study population
Patient characteristics in the two groups.
Quantitative image quality
Objective image quality evaluation of CCTA in the two groups.

CNR, contrast-to-noise ratio; LAD, left anterior descending artery; LCX, left circumflex artery; LMA, left main coronary artery; RCA, right coronary artery; SNR, signal-to-noise ratio.
Qualitative image analysis
Subjective image quality scores of coronary arteries in the two groups.

LAD, left anterior descending artery; LCX, left circumflex artery; LMA, left main coronary artery; RCA, right coronary artery.
Assessment of coronary stenosis
Among the 1014 segments in two groups, 13 segments in 11 patients (5 segments in 100 kVp group and 8 segments in 80 kVp group) demonstrated stenoses ≥50%. The inter-observer agreement was good for 100 kVp group (k = 0.664, P < 0.001) and 80 kVp group (k = 0.797, P < 0.001). Five patients (one patient in 100 kVp group and 4 patients in 80 kVp group) were referred for invasive coronary angiography (Figs 2 and 3). The comparison of invasive coronary angiography and CCTA showed the promise of CCTA using 80 kVp protocol to accurately diagnose CAD.
Coronary CT angiography and invasive coronary angiography images in a 69-year-old woman in the 100 kVp group. (a, b, c) Curved planar reformations (CPR) of right coronary artery (RCA), left anterior descending artery (LAD), and proximal left circumflex artery (LCX). (d, e) Images of invasive coronary angiography. Low-grade stenoses (<50%) in the proximal RCA, LAD, and LCX are discovered in both CCTA and invasive coronary angiography. CCTA and invasive coronary angiography images in a 65-year-old woman in the 80 kVp group. Panel (a, b, c) Curved planar reformations (CPR) of right coronary artery (RCA), left anterior descending artery (LAD), and proximal left circumflex artery (LCX). (d, e) Images of invasive coronary angiography. Low-grade stenoses (<50%) in the RCA and LCX and a high-grade stenosis (>50%) in the LAD are discovered in both CCTA and invasive coronary angiography.

Injection-associated discomfort
Comparison of the frequency and intensity of contrast-associated discomfort between groups.

Radiation exposure estimation
Radiation dose comparison between the two CCTA groups.
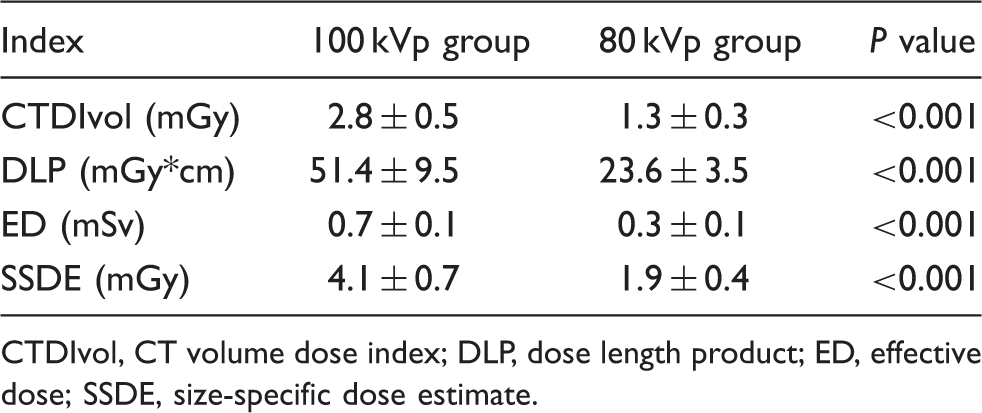
CTDIvol, CT volume dose index; DLP, dose length product; ED, effective dose; SSDE, size-specific dose estimate.
Discussion
Our results show that CCTA with low concentration, low volume contrast medium, and low radiation dose on a second generation dual-source CT system constitutes a feasible protocol, which resulted in a 54% radiation dose reduction and a 64% decrease in iodine load compared with a 100 kVp standard protocol, without compromising image quality of CCTA.
Isosmolar, low concentration Iodixanol with a concentration of 270 mg I/mL has the potential to decrease iodine load and has recently been implemented in CT angiography (14,26). However, lower attenuation would result as a consequence of the lower concentration of contrast material, which may in turn lead to degradation of image quality and decreased diagnostic accuracy. Lowering tube voltage effectively increases attenuation of the iodinated contrast agent, which offers an opportunity to reduce the iodine load. A study by Waaijer et al. showed a 43% increase in attenuation per milligram of iodine when the tube voltage was decreased from 120 to 90 kVp (27). In addition, the shortened acquisition time in high-pitch mode corresponds to a shortened temporal window of vascular enhancement required. The recent study by Zheng et al demonstrated the feasibility of CCTA performed with 80 kVp and low-concentration (270 mg I/mL) contrast material in patients with BMI less than 25 kg/m2 (13). However, the mean volume of contrast material they used was about 57 mL, double the amount administered in our study (30 mL). We were able to achieve an even further reduction by implementing high-pitch mode into our acquisition protocol, while Zheng et al. used a sequential protocol. The patients in 80 kVp group suffered from less contrast-associated discomfort compared with 100 kVp group. Thus, our proposed CCTA protocol appears to be promising for selected patients in the clinical setting.
Although high pitch and low tube voltage methods are beneficial to patients in regards to radiation dose and contrast material reduction, the noise caused by the application of these technologies may impair diagnostic interpretability. SAFIRE, a noise-modeling algorithm supported by raw data, was used in 80 kVp group to counter the increased noise and improve image quality in our study. SAFIRE iteratively estimates the local noise content in each image pixel and removes it from the current image dataset (28,29). In our study, the noise in 80 kVp group reconstructed with SAFIRE was even lower than in 100 kVp group reconstructed with FBP. However, the SNR in 80 kVp group was significantly lower than in 100 kVp group due to the substantially lower CT attenuation. To the best of our knowledge, there is no consensus on the optimal values of SNR for acceptable objective quality. In regard to CNR and subjective image quality, no significant differences were observed between the two study groups.
There are a few limitations to our study. First, the sample size was relatively small. Consequently, the subgroups were too small to investigate the impact of BMI and heart rate on image quality. On the same note, patients that experienced specific forms of contrast-associated discomfort were too few to draw any significant conclusions. Further study on a large population should be conducted to examine these aspects. Second, because of the lower SNR in 80 kVp group, 80 kVp protocol may only be applicable to patients with BMI less than 25 kg/m2. Third, the diagnostic accuracy of our presented CCTA protocol should be further assessed with invasive coronary angiography as reference standard. Last, our randomized method is suboptimal.
In conclusion, this study shows that prospectively ECG-triggered, high-pitch CCTA at 80 kVp with 30 mL of 270 mg I/mL contrast material is feasible for patients with BMI less than 25 kg/m2 and allows substantial reduction in radiation dose and contrast material load without substantially impairing image quality.
Footnotes
Conflict of interest
UJS is a consultant for and/or receives research support from Bayer, Bracco, GE Healthcare, Medrad, and Siemens. The other authors have no conflict of interest to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.