
Abstract
Background
Computed tomography (CT) has important roles for lung cancer screening, and therefore radiation dose reduction by using iterative reconstruction technique and scanning methods receive widespread attention.
Purpose
To evaluate the effect of two reconstruction techniques (filtered back projection [FBP] and adaptive iterative dose reduction using three-dimensional processing [AIDR 3D]) and two acquisition techniques (wide-volume scan [WVS] and helical scan as 64-detector-row CT [64HS]) on the lung nodule identifications of using a chest phantom.
Material and Methods
A chest CT phantom including lung nodules was scanned using WVS and 64HS at nine different tube currents (TCs; range, 270–10 mA). All CT datasets were reconstructed with AIDR 3D and FBP. Standard deviation (SD) measurements by region of interest placement and qualitative nodule identifications were statistically compared. 64HS and WVS were evaluated separately, and FBP images acquired with 270 mA was defined as the standard reference.
Results
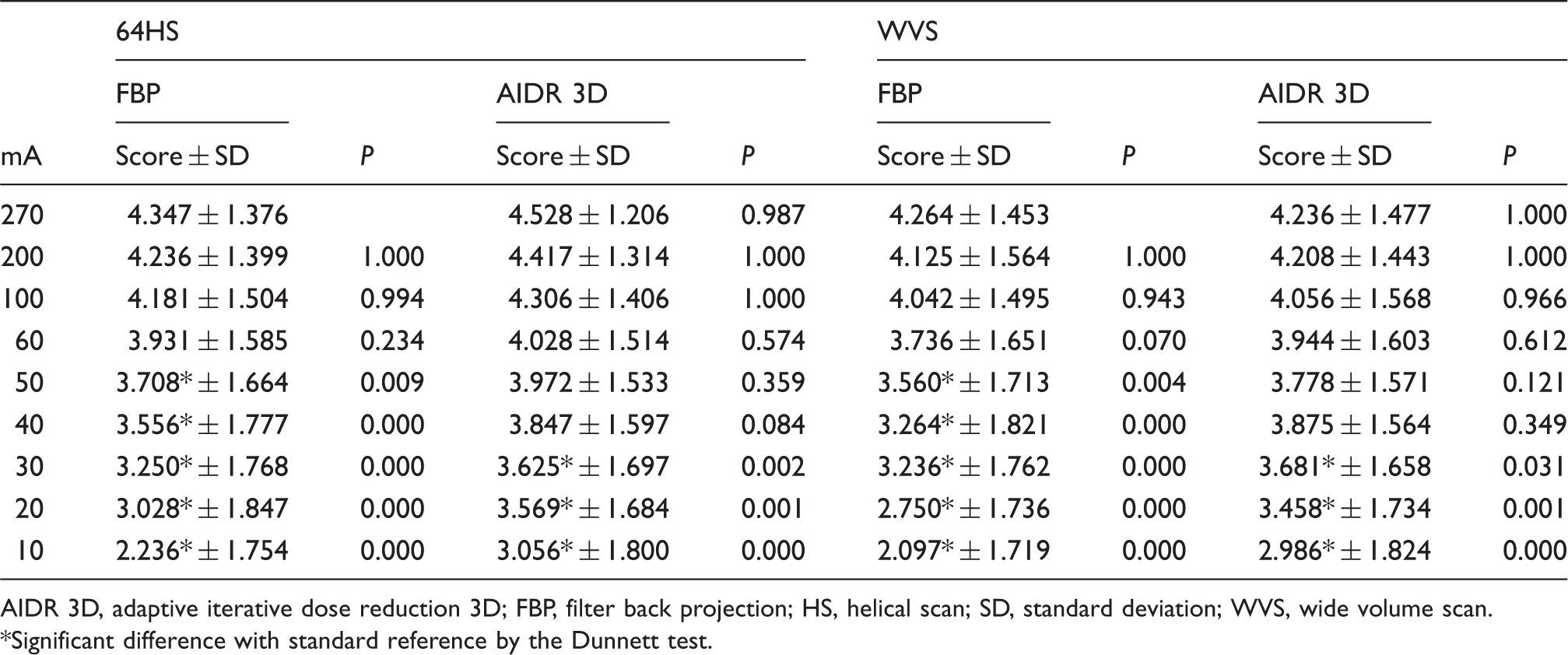
SDs of all datasets with AIDR 3D showed no significant differences (P > 0.05) with standard reference. When comparing nodule identifications, area under the curve on WVS with AIDR 3D with TC <30 mA, on 64HS with AIDR 3D with TC <40 mA, and on reconstructions with FBP and each scan method with TC <60 mA was significantly lower than with standard reference (P < 0.05). With the same TC and reconstruction, SDs and nodule identifications of WVS were not significantly different from 64HS (P > 0.05).
Conclusion
In term of SD of lung parenchyma and nodule identification, AIDR 3D can achieve more radiation dose reduction than FBP and there is no significant different between WVS and 64HS.
Introduction
Lung cancer is the largest contributor to cancer mortality worldwide (1,2), and screening with computed tomography (CT) has been frequently investigated (3–6). Therefore, CT has an important role; however, the issue of radiation dose reduction in CT is currently drawing widespread attention. Several techniques are proposed for dose reduction, and recently the iterative reconstruction (IR) technique has been proposed to decrease radiation dose while maintaining image quality. Various IR techniques have been developed (7–12). Adaptive iterative dose reduction using three-dimensional (3D) processing (AIDR 3D) is one of these IR techniques (13–15).
Meanwhile, CT machines have been developed, and in term of scanning techniques there are two representative techniques (16–20), one being helical scanning where the use of thinner detector collimation and a lower beam pitch can produce high image quality compared to that attainable with a thicker detector collimation and/or higher beam pitch (21). The other is wide volume scan (WVS). 320-detector row CT has been applied in clinical settings, and it has gradually been recognized that WVS has superior or equivalent image quality in comparison with helical scanning in several organs (16–20). WVS is different from helical scanning using multiple consecutive axial scans (step-and-shoot scanning), which makes it possible to obtain volumetric scan data for the entire lung with a few rotations. Although WVS might have demerits as cone beam artifacts, step artifacts, and sometimes increased radiation dose due to the expansion of scan ranges, this utility was reported for the lung assessment field and the image quality of WVS was comparable or slightly superior to that of 64-row helical scans (64HS). On the other hand, pulmonary nodule identification assessments under low radiation dose conditions by means of 64HS were performed previously and the detection rate of the 40 mA images were no significant difference with that of 300 mA images (21), however, there have been no reports by means of WVS.
Under these circumstances, it is important to know the limit of decreased radiation doses for different scanning techniques in lung cancer screening. Therefore, we hypothesized that the AIDR 3D technique can achieve further radiation dose reduction on CT examination for pulmonary nodule identification with 320-detector row CT using different scanning techniques, i.e. 64HS and WVS, as compared with the previously applied filtered back-projection (FBP) technique. The purpose of this study was therefore to determine the utility of AIDR 3D for pulmonary nodule identification on dose reduction 320-detector row CT as compared with the previously applied FBP technique and to compare the pulmonary nodule identification between 64HS and WVS in a chest phantom study.
Material and Methods
Phantom specifications
A chest phantom (LSCT001, Kyoto Kagaku, Kyoto, Japan) was used. Details of the chest phantom have been described in the literature (21,22), which can be summarized as consisting of the basic chest structure and simulated pulmonary nodules. The basic structure of the phantom is an anthropomorphic chest with the arms raised. The chest wall and mediastinum consist of a substance radiologically equivalent to water, and the vertebrae and ribs consist of one radiologically equivalent to bone. The lung parenchyma is made up of a composite of Styrofoam and powdered hard urethane foam in a urethane resin adhesive, and has a targeted CT value of −900 HU. Simulated ground-glass nodules (GGNs) and semi-solid nodules measuring 2, 4, 6, 8, 10, 12, and 14 mm in diameter are located at the level of the lung apex, the bifurcation of the trachea, and the lung base in both lungs. The simulated pulmonary GGNs and semi-solid nodules are spheres made of acrylic foam and urethane. The targeted CT values of the simulated GGNs and semi-solid nodules in our study were –800 HU and –630 HU, respectively.
Iterative reconstruction (IR) technique
In this study, adaptive iterative dose reduction using AIDR 3D was used as the IR technique. The details regarding AIDR 3D have been described elsewhere (13–15). In brief, in low-dose scanning, the number of X-ray photons becomes relatively small, and the electronic noise on the data acquisition systems becomes dominant, causing degradation of the image quality. AIDR 3D uses a statistical noise model considering both the photon and electronic noise, to eliminate noise due to photon starvation in the projection data.
Scan and reconstruction protocols
The chest phantom was scanned with a 320-detector row CT scanner (Aquilion ONE ™; Toshiba Medical Systems, Otawara, Tochigi, Japan). Conventional 64HS and WVS were performed. The scan parameters of 64HS were 0.83 beam pitch and 0.5 mm × 64 detector configurations. The WVS parameters were 0.5 mm × 320 detector configurations with three gantry rotations. Other parameters were kept constant: 120 kVp and FOV 320 mm. The scan length of 64HS was 375 mm, and that of WVS was 348 mm because of scan overlap.
Tube current was changed at 270, 200, 100, 60, 50, 40, 30, 20, and 10 mA, and dose length products (DLPs) were in the range of 19.2–619.5 mGy·cm. All CT data were reconstructed to 1 mm section thicknesses, and all CT images also underwent a commercially available lung kernel (FC51). The standard strength of AIDR 3D was used. At each tube current, the chest phantom was scanned three times, yielding a total of 54 datasets (2 different scan methods × 9 different tube currents × 3 times). All datasets were reconstructed with FBP and AIDR 3D, yielding a total of 108 datasets. The reconstruction times of each dataset were less than 70 s.
Image analysis
All CT data were analyzed using a semiautomatic image-processing program (ImageJ Version 1.46r, a public-domain Java image processing program available at http://rsb.info.nih.gov/ij/). The standard deviation (SD) of normal lung parenchyma of dose reduction CTs reconstructed with FBP and with AIDR 3D was measured in five slices, i.e. lung apex, tracheal bifurcation level, lung base, the slice between lung apex and tracheal bifurcation level, and the slice between tracheal bifurcation level and lung base. Each slice was kept at all datasets and evaluated individually, and the right and left lungs were graded separately. A circular region of interest (ROI) with a 2 cm2 cross-sectional area was placed at center of each lung field by a chest radiologist (HK).
Next, all CT images were interpreted or analyzed with a picture archiving and communication system (PACS) (ShadeQuest, Yokogawa Electric, Tokyo, Japan) without access to information about the scan parameters and reconstruction. They were randomized and independently reviewed by two chest radiologists (SS and HK) with 8 and 13 years of experience in a lung-window setting (window width, 1600 H; window level, −550 H). To determine the influence of tube currents and reconstruction conditions on identification of pulmonary abnormalities, the probability of the presence of a lesion for each dataset was scored using a 5-point rating scale: 1, absence; 2, probable absence; 3, equivocal; 4, probable presence; and 5, definite presence. GGNs, semi-solid nodules, and normal lung parenchyma were assessed by each reader, and the final probability of the presence of a lesion for each dataset was decided by consensus of the two readers.
Statistical analysis
Standard reference was defined as the dataset acquired with 270 mA reconstructed by FBP, and the datasets of WVS and 64HS were analyzed separately regarding dose reduction assessments.
For the quantitative evaluation, SDs were compared by the Dunnett test. In addition, SDs between 64HS and WVS were compared by means of paired t-test at the same tube current and reconstruction.
Kappa (κ) analysis was used for the evaluation of inter-observer agreement for detection and image quality. Inter-observer agreement was considered to be slight at κ < 0.20, fair at κ = 0.21–0.40, moderate at κ = 0.41–0.60, substantial at κ = 0.61–0.80, and almost perfect at κ = 0.81–1.00 (23).
To compare overall pulmonary nodule identification, each area under the curve (AUC) by means of ROC analysis of datasets was compared with that of standard reference. In addition, AUCs between 64HS and WVS were compared at the same tube current and reconstruction.
Finally, to compare small lesion detection, lesions <10 mm, i.e. 2, 4, 6, and 8 mm in diameter, conspicuity scores of these lesions were compared by the Dunnett test.
A P value of less than 0.05 was considered to indicate a statistically significant difference for all statistical analyses. All statistical analyses were performed with statistical software (Ekuseru-Toukei 2012, Social Survey Research Information Co., Ltd., Tokyo, Japan; and StatMate, ATMS Co., Ltd., Tokyo, Japan).
Results
Representative images are shown in Figs. 1 and 2.
Examples of dose reduction CT images from 64-row helical scans. (a) CT with 270 mA reconstructed with FBP (standard reference). (b) Dose reduction CT (40 mA) reconstructed with FBP. (c) Dose reduction CT (40 mA) reconstructed with AIDR 3D. Standard reference, i.e. CT with 270 mA reconstructed with FBP, (a) shows simulated ground-glass nodules and semi-solid nodules with diameters in the range of 2–14 mm, at 2 mm intervals in both lungs. With dose reduction, image quality of dose reduction CT (40 mA) reconstructed by FBP was decreased (b). However, dose reduction CT images (40 mA) reconstructed by means of AIDR 3D (c) were less influenced by dose reduction in comparison with those reconstructed with FBP. Examples of dose reduction CT images from wide-volume scans. (a) CT with 270 mA reconstructed with FBP (standard reference). (b) Dose reduction CT (30 mA) reconstructed with FBP. (c) Dose reduction CT (30 mA) reconstructed with AIDR 3D. Standard reference, i.e. CT with 270 mA reconstructed with FBP, (a) shows simulated ground-glass nodules and semi-solid nodules with diameters in the range of 2–14 mm, at 2 mm intervals in both lungs. With dose reduction, image quality of dose reduction CT (30 mA) reconstructed by FBP was decreased (b). However, dose reduction CT images (30 mA) reconstructed by means of AIDR 3D (c) were less influenced by dose reduction in comparison with those reconstructed with FBP.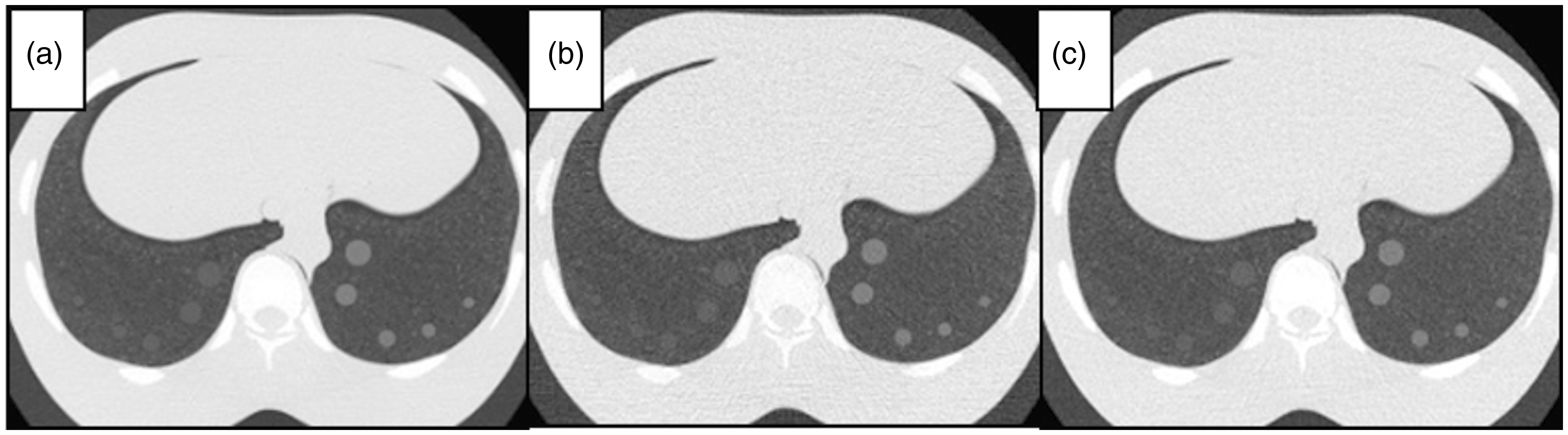

Comparison with SD of lung parenchyma.
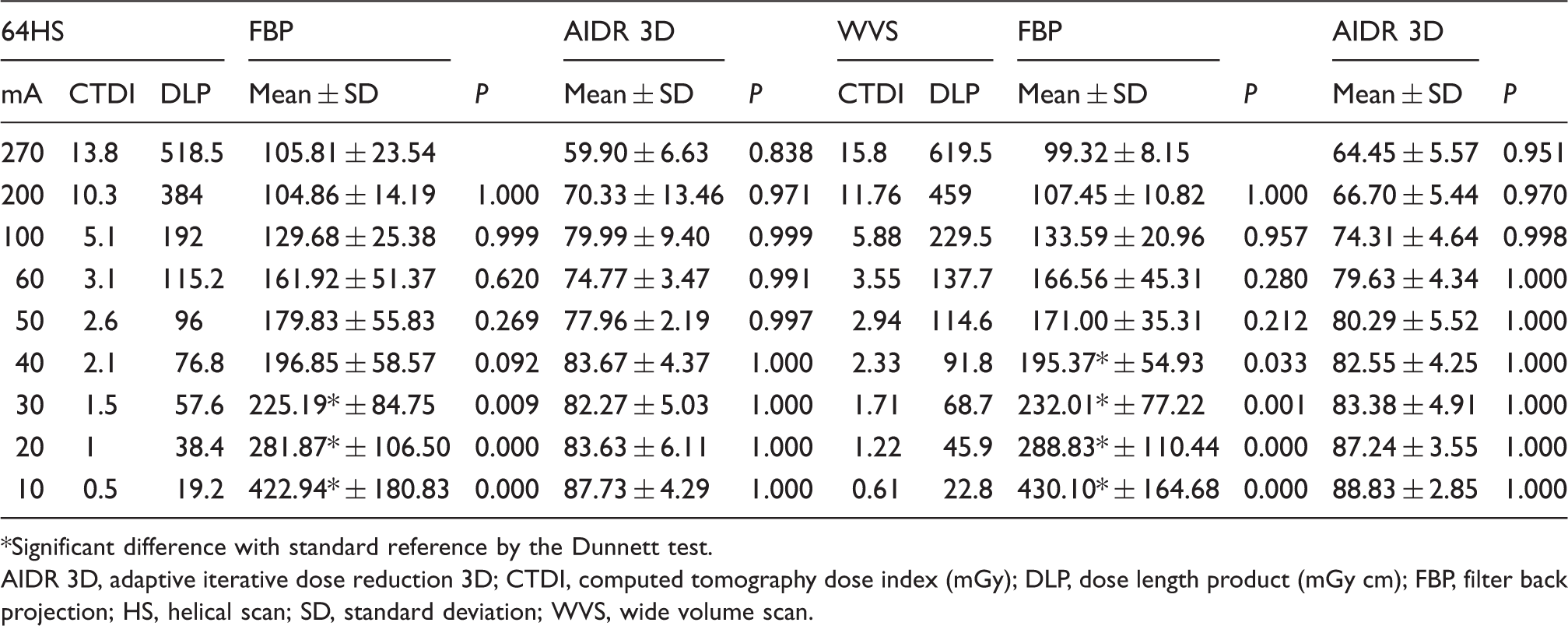
Significant difference with standard reference by the Dunnett test.
AIDR 3D, adaptive iterative dose reduction 3D; CTDI, computed tomography dose index (mGy); DLP, dose length product (mGy cm); FBP, filter back projection; HS, helical scan; SD, standard deviation; WVS, wide volume scan.
Inter-observer agreement of pulmonary nodule detection.
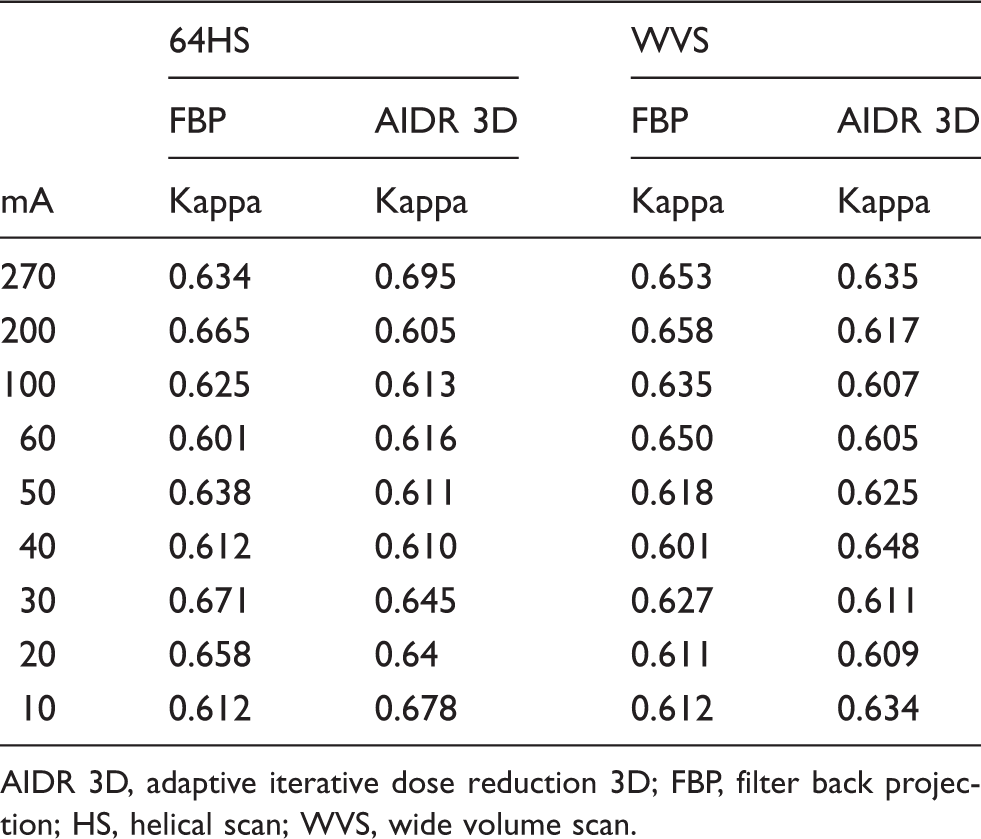
AIDR 3D, adaptive iterative dose reduction 3D; FBP, filter back projection; HS, helical scan; WVS, wide volume scan.
Overall pulmonary nodule identification.
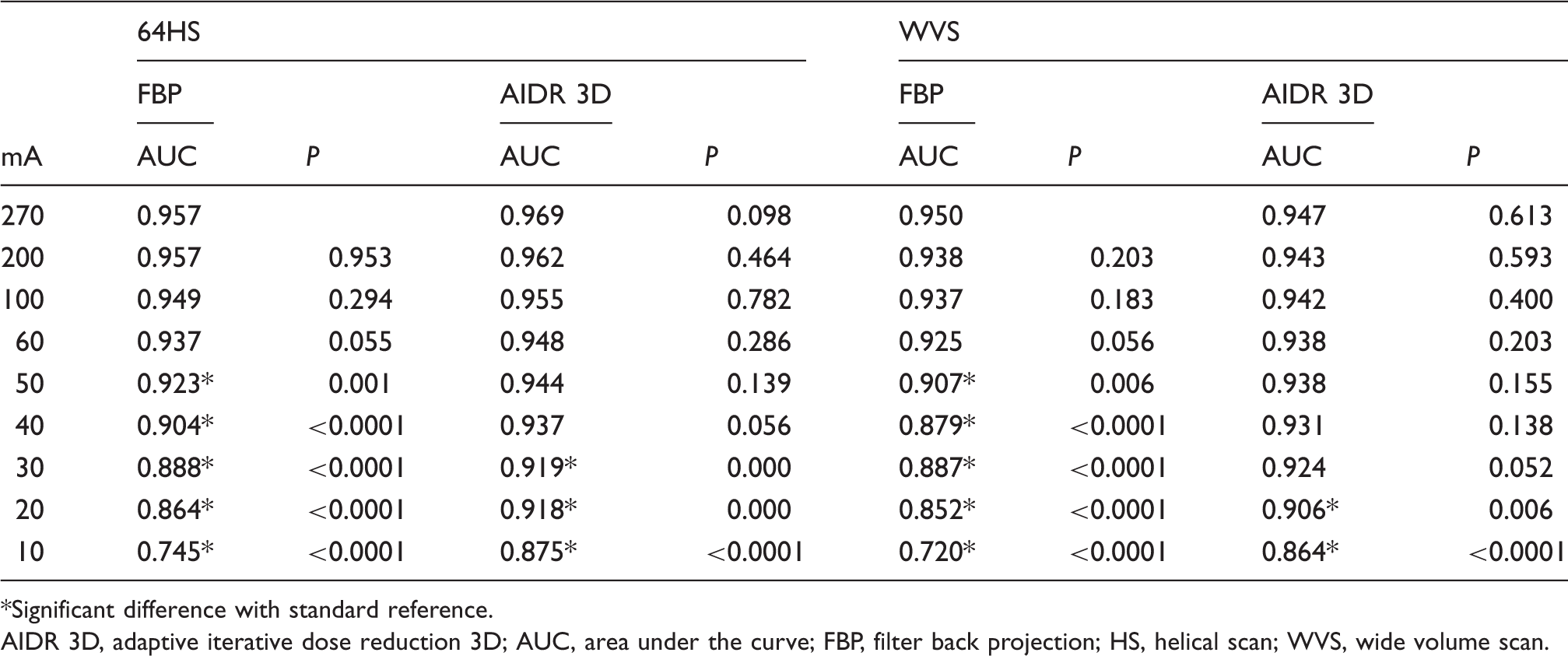
Significant difference with standard reference.
AIDR 3D, adaptive iterative dose reduction 3D; AUC, area under the curve; FBP, filter back projection; HS, helical scan; WVS, wide volume scan.
Conspicuity scores of small pulmonary nodules.
AIDR 3D, adaptive iterative dose reduction 3D; FBP, filter back projection; HS, helical scan; SD, standard deviation; WVS, wide volume scan.
Significant difference with standard reference by the Dunnett test.
Discussion
Our study demonstrated the utilities of AIDR 3D in dose reduction CT, and SDs for the quantitative evaluation were reduced when AIDR 3D was applied to both 64HS and WVS. In addition, regarding pulmonary nodule identification including small nodules, there was no significant difference between standard reference, i.e. 270 mA, and dose reduction CT, i.e. 40 mA and under, therefore dose reduction CT on lung cancer screening is possible when AIDR 3D is applied. Regarding radiation exposure and nodule identification, although 64HS was deemed to be slightly superior to WVS, there were no significant differences. To the best of our knowledge, no reports have been published on the direct comparison of scanning techniques and AIDR 3D for chest dose reduction CT examinations, and our results have the potential of guide of chest dose reduction CT examination.
The issue of radiation dose reduction in CT is currently drawing widespread attention. When the tube current was reduced, image noise was increased and image quality was decreased, because the reduction in tube current leads to a reduction in photons (24). The iterative reconstruction (IR) technique might solve this problem because it can decrease image noise. In fact, comparisons of quantitative SD measurements showed significant superiority of AIDR 3D over FBP in this study. When AIDR 3D was applied, there were no significant differences between SDs on the datasets at 270 mA and at 10 mA. This result suggests that AIDR 3D can suppress background noise regardless of tube current, and, considering the reconstruction times of AIDR 3D, it is proven that AIDR 3D is useful for reconstruction in clinical practice. Therefore, AIDR 3D will have a more important role in the near future. In fact, in an evaluation study of various pulmonary disease cases, image quality of LDCT reconstructed with AIDR 3D was visually equal to that of standard reference (13).
When inter-observer agreement for identification of pulmonary nodules was compared, all inter-observer agreements were substantial (0.61 < κ < 0.80). This suggests that tube currents and reconstruction methods should be considered to have less influence on the inter-observer variance for nodule identification. Therefore, the result was more dependent on the tube current and reconstruction methods than on inter-observer variances.
At the assessment of nodule identification, a decrease of about 10–15% of radiation dose becomes possible when applying AIDR 3D. This is of extreme value in screening, at least in comparison with conventional reconstructions such as FBP. AIDR 3D successfully remove the effect of electrical noise from the projection data, and image noise with the lower tube current becomes relatively stable. AIDR 3D should be used aggressively on dose reduction CT screening. In addition, there are several possibilities for optimizations to be investigated by applied AIDR 3D. The reasons for this are as follows: first, although the standard strength was used in this study, this AIDR 3D technique had various types of strength – strong, standard, mild, and weak. Second, because the de-noising filter and the reconstruction kernel (e.g. lung kernel and standard kernel) might also influence the results (25,26), there might be more appropriate reconstruction conditions. Third, AIDR 3D can be used together with the automatic exposure control (AEC) system. However, there might be limitations to evaluations even if they are reconstructed with AIDR 3D in the assessment of ground-glass nodules (GGNs). GGNs were easily influenced by dose reduction in a phantom study (27), and in clinical practice there have been reports on the limitations of GGNs even if they are reconstructed with AIDR 3D (13). In clinical practice, knowledge of this limitation is important.
In this study, two different scanning techniques were used: 64HS and WVS. Regarding radiation exposure and nodule identification, although 64HS was deemed to be slightly superior to WVS, there were no significant differences. Considering these results and the scanning technique independent of the CT machine, the choice of scanning method showed little impact in this phantom study, and 64HS was deemed to be sufficient for lung cancer screening. To ensure that the entire target area is imaged, overlap must be acquired between the volume scans, resulting in the delivery of more radiation to the patient, in particular with WVS. Meanwhile, 0.83 beam pitch was used on the 64HS scan. These are the reasons that 64HS was deemed to be slightly superior to WVS. In contrast, the utilities of WVS were reported in comparison with 64HS (16,18), and the fact remains that WVS has an advantage in the chest field because WVS is not easily influenced by motion artifact from the heart, and WVS with ECG gating is recommended to be performed (18). Knowledge of the features of scanning techniques is important in lung cancer screening, and further clinical studies are needed.
Our study has several limitations. First, we adopted a commercially available chest CT phantom. Therefore, no motion artifacts resulting from breathing or heart motion were observed. In addition, these nodules were perfectly round and their frequency was quite different from that observed in screening or in clinical practice. Moreover, the positions of these nodules had not changed. We would have to say that this phantom study is different from clinical practice; however, this result provides a different direction for dose reduction. Second, only two different reconstructions and two different scanning methods were evaluated. Comparison with other scanning methods and other IR techniques including other strength levels of AIDR 3D might be necessary. Third, although nodule identification was assessed, other findings were not evaluated. The evaluations should be investigated in the future.
In conclusion, in term of SD of lung parenchyma and nodule identification, AIDR 3D can achieve more radiation dose reduction than FBP and there is no significant different between WVS and 64HS.
Footnotes
Acknowledgements
The authors thank Noriyuki Negi, Tohru Murakami, (Division of Radiology, Kobe University Hospital), and Maya Okuno, (Toshiba Medical Systems Corporation) for their contribution to this work.
Declaration of conflicting interests
YO, SM, and KS received research grants from Toshiba Medical Systems. HI and NS are employees of Toshiba Medical Systems.
Funding
This work was supported by Toshiba Medical Systems Corporation.