
Abstract
Background
Invasive placental disorders are potentially life-threatening. Its diagnosis and evaluation of degree of invasiveness is vital in surgical and treatment planning.
Purpose
To compare the role of various imaging modalities used in current practice for evaluation of invasive placental disorders, and evaluate the validity of certain imaging signs for prediction of invasive placenta.
Material and Methods
Twenty-two patients, which were clinically stratified as a risk group for underlying invasive placental abnormality, underwent Doppler sonography and magnetic resonance imaging (MRI). Abnormal placental invasiveness was assessed using various Doppler sonography and MRI signs described in the existing literature. We systematically evaluated the utility of each of these modalities and signs, and compared the roles played by them separately and in combination. All the cases were correlated with surgical and pathological findings.
Results
Nine patients had surgical and pathological confirmation of placental adhesive disorders, of which eight were predicted correctly by MRI (true positive) while one was misdiagnosed as normal placenta (false negative). All the nine cases were correctly identified by Doppler sonography. MRI was more accurate in predicting bladder invasion, identifying 5/6 cases.
Conclusion
Both MRI and Doppler sonography are useful for detection of invasive placental disorders. However, MRI is a better predictor of bladder invasion.
Introduction
Evolution has not settled on a single, most efficient placental design. While the placenta in most other mammals is less invasive in nature, that in human beings is a highly invasive hemochorial in nature (1). Further, with increased use of uterine surgery for various indications, a previously scarred myometrium is sometimes not able to control the trophoblastic invasion when the placenta becomes morbidly adherent (1,2). An invasive placenta can be potentially life-threatening; hence, optimal management mandates accurate prenatal identification. Ultrasonography aided by color Doppler is the first line modality in evaluation of invasive placenta. However, there has been recent interest in the role of magnetic resonance imaging (MRI) in assessing placenta accreta, especially in cases where diagnosis is equivocal on sonography. The present study aims at reviewing and correlating various sonographic, Doppler, and MRI features in the diagnosis of placenta accreta. We further try to assess the role of above modalities for vesical wall invasion in cases of placenta accreta.
Material and Methods
Subjects
Patients for the present prospective observational study were recruited from patients referred for sonography for evaluation of invasive placenta, mainly due to a previous history of Cesarean deliveries or other uterine surgeries. The study was carried out from September 2011 to June 2013. The study was approved by the institutional review board (IRB) and written informed consent was obtained from all patients. A total of 22 patients were included in this analysis, which were clinically stratified as a risk group for underlying invasive placental abnormality. All these cases were rescreened by a junior radiologist (1 year of experience in obstetric imaging) who charted the imaging features. The same patients were re-examined by a senior radiologist (more than 10 years of experience in obstetric imaging) within 24 h and a diagnosis of invasive placenta was made in 10 of these patients, who were included in the analysis. Two of these patients were in the second trimester, while eight patients were in the third trimester of pregnancy. Those having a contraindication for MRI (such as presence of metallic implants, claustrophobia) or those who were too unstable to perform MRI, were excluded from further analysis.
Imaging
Pelvic sonography was performed on IU-22, Philips Medical Systems (Best, The Netherlands) and Xario, (Toshiba Medical systems, Chiba, Japan) equipment using a 3.5 MHz curved electronic array transducer. Grayscale B-mode sonography was first used to assess the placental tissue localization and shape, followed by an assessment by superimposing color/power Doppler over suspected and potential regions of interest. MRI was performed on a 1.5 T (Magnetom Avento, Siemens Medical System, Erlangen, Germany) superconducting magnet using a 16-channel transmit-receive body coil. A small amount of fluid in the urinary bladder aided the evaluation of the uterine and bladder serosa; therefore, all Doppler ultrasound (US) and MR examinations were obtained with a partially full bladder. Following a localizer scan, sagittal, axial, and coronal half-Fourier acquisition with single-shot turbo spin echo (HASTE) (TR/TE, min/90.0 ms; matrix, 256 × 224; thickness with no gap, 4 mm; echo train length, 94; receiver bandwidth, 62.50 kHz) were acquired during breath-hold. Next, sagittal, coronal, and axial true fast-imaging with steady-state precession (True FISP) (TR/TE, 3.5/1.8 ms; matrix, 256 × 224; signal acquired, 1; thickness with no gap, 5 mm; flip angle, 50°; receiver bandwidth, 125 kHz) were acquired. All studies were done during free breathing without any sedation. The procedure was carefully explained to the mother and it was ascertained that patient was well fed before the procedure. If not, the mother was given 100–200 mL oral glucose to reduce maternal anxiety and fetal motion during the scan. The entire examination time was 20–25 min.
Case analysis
Abnormal invasiveness was assessed using established Doppler sonography criteria, which included the presence of placenta previa, presence of irregular anechoic areas (lacunae), moving echogenicity (turbulence) within those lacunae, Doppler flow within these lacunae with vascular channel distributed throughout placenta, disruption of retroplacental flow, dilated subplacental vascular channels with pulsatile venous flow, and interface vascularity with abnormal blood vessels linking placenta to the bladder with arterial blood flow (3). The cases were marked as negative for invasive placenta only when all the signs were absent on Doppler sonography. Further evaluation by MRI using standardized criteria (4) for detection and characterization of placental invasiveness was done, which included marked placental heterogeneity, dark intraplacental bands, intraplacental hemorrhages, and uterine bulge. Again, the cases were marked negative for placenta accreta only when all the described set of criteria were not present in the patient. Presence of vesical wall invasion by invasive placenta was assessed by bladder hypervascularity of the uterine serosal– bladder wall complex on Doppler sonography and loss of chemical shift artifacts at the bladder–uterine interface on TrueFISP sagittal and coronal MR images. All the cases were correlated with surgical and pathological findings. All cases with uncomplicated placental removal without excessive bleeding after Cesarean delivery were designated as true negative. All true positive, false positive and false negative diagnoses were confirmed by pathologic examination performed in the Department of Pathology of our institute.
Statistical analysis
The sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of various parameters of color Doppler sonography and MRI in the identification of placental abnormalities were calculated. The diagnostic accuracy was calculated using the standard method (5). All analyses were carried out using Open-epi software (Version 2.3 from Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta, GA, USA). Receiver-operating characteristic (ROC) curves were drawn for individual parameters and the areas under the curve were computed and compared using SPSS version 16(SPSS Inc., Chicago, IL, USA). The area under the curve (AUC) was calculated to compare relative diagnostic efficiencies for each parameter.
Results
MRI signs in detecting placental adhesive disorders (22 patients).
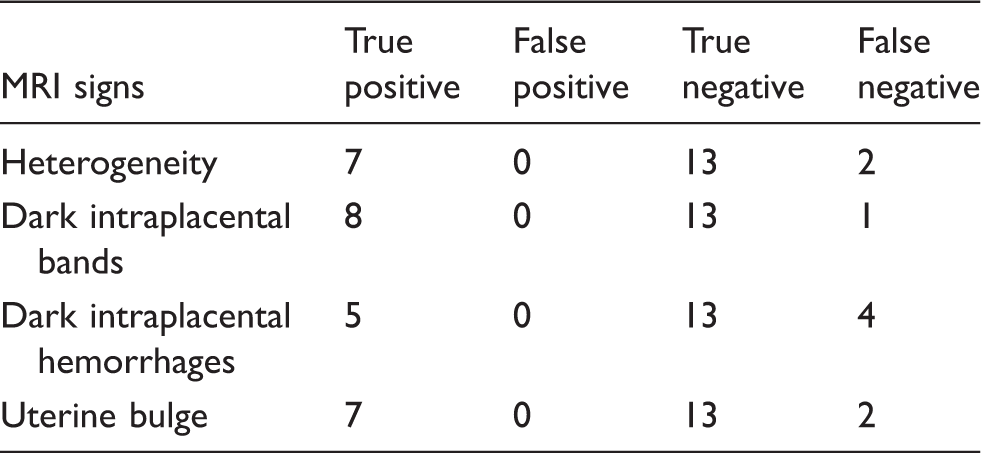
Analysis of MRI signs in placental adhesive disorders (22 patients).

MRI and US in diagnosis of placenta adhesive disorders (22 patients in this study).

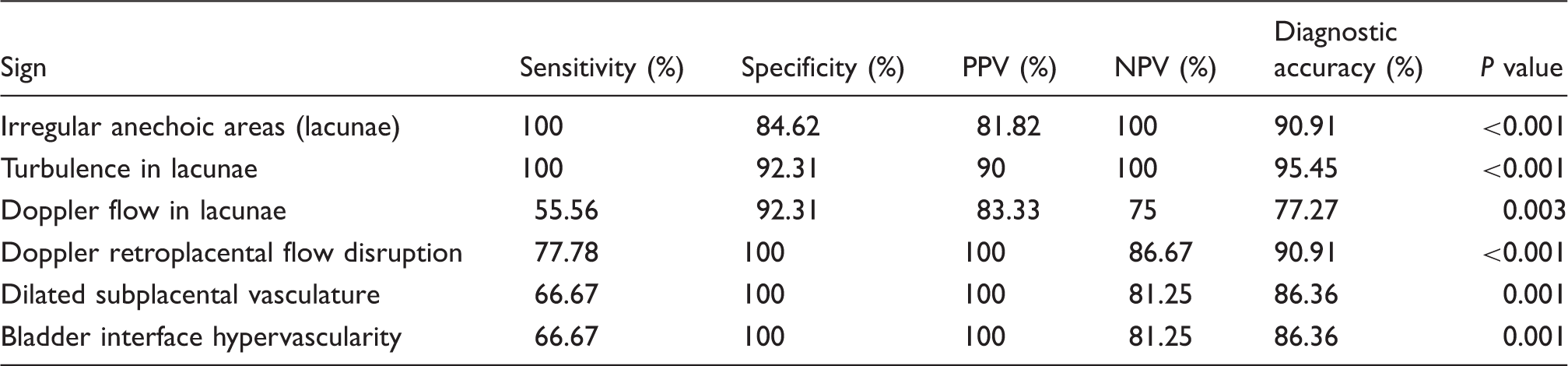
Among the individual sonographic and color Doppler signs mentioned for detection of invasive placenta (Table 4), turbulence in visualized lacunae was the most accurate sign, with a sensitivity of 100% and a specificity of 92% with maximum AUC in ROC analysis (Fig. 1). However, presence of Doppler flow in these lacunae, even on applying power Doppler mode, was less accurate in detecting placental invasion and had a sensitivity of 56% with an overall diagnostic accuracy of 77%. Disruption of subplacental vascularity showed a similar sensitivity of 78%, but was more specific and had a high positive predictive value approaching 100% in this study. Dilated subplacental vessels with pulsatile flow and hypervascularity in the bladder–placenta interface was present in 6/9 cases (67%) but were more specific and identified all 13 true negative cases.
ROC analysis of the document US and color Doppler features to calculate the AUC. Note the maximum AUC was demonstrated in feature combining both the modalities, i.e. dilated subplacental vessels with disruption of retroplacental flow, for detection of invasive placenta. Analysis of USG signs in detecting placenta accreta for 22 patients in this study.
MRI signs in detection of invasive placenta (Tables 1 and 2) showed an overall sensitivity of 89% and specificity of 100%. Among the various signs, presence of dark intraplacental bands was the most accurate sign with highest area under ROC curve (Fig. 2). Marked placental heterogeneity was also reasonably accurate identifying 7/9 cases. Intraplacental hemorrhages were relatively less accurate, detected in five cases.
ROC analysis of the document MRI features to calculate the AUC. Note the maximum AUC was demonstrated for dark intraplacental bands in detection of invasive placenta.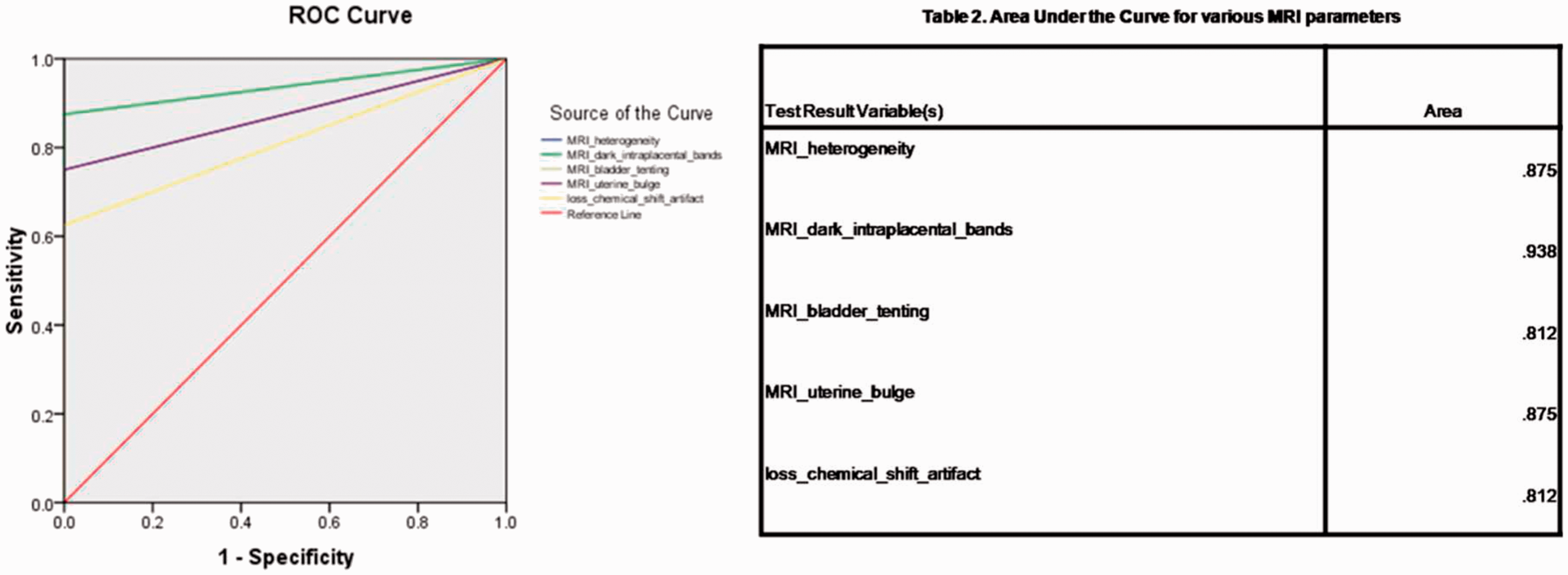
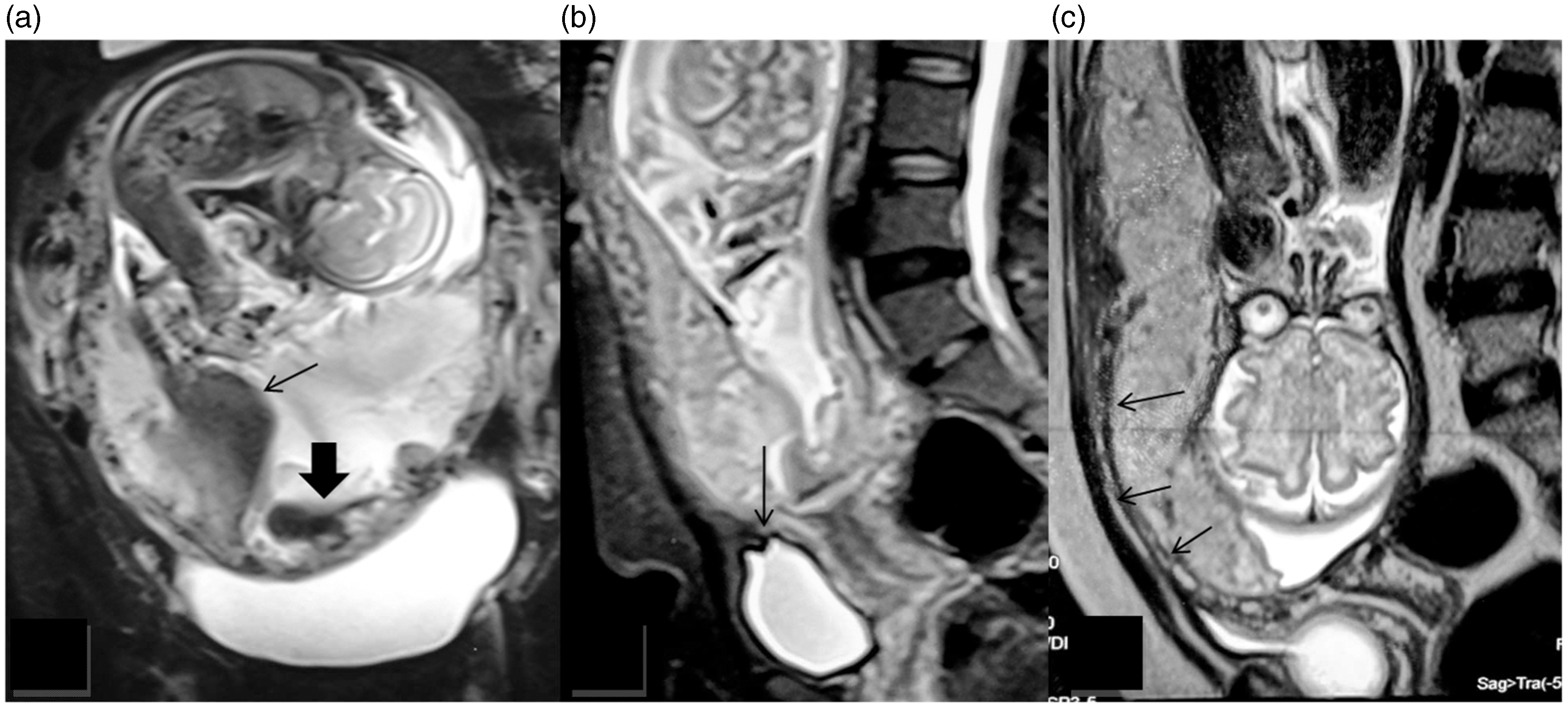
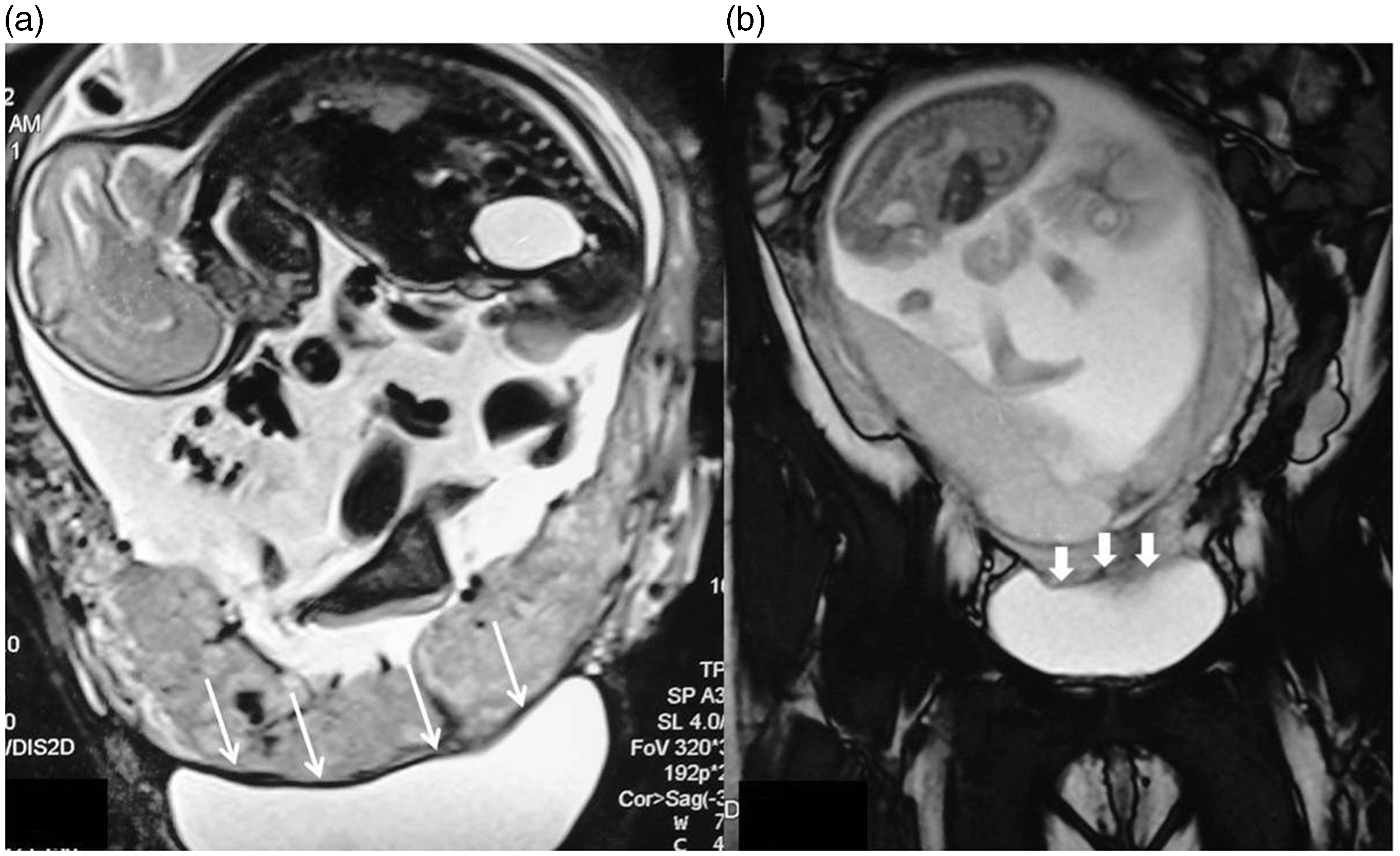
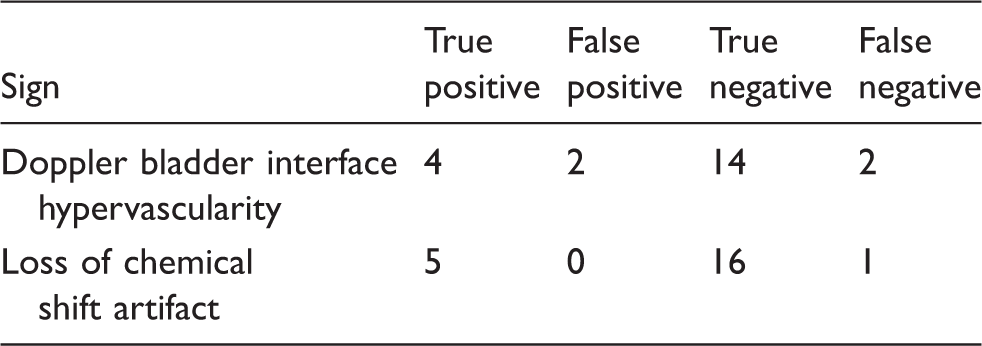
Markers for detecting invasion of the wall of the urinary bladder in cases of placenta percreta included loss of myometrial lining at the bladder interface on sonography, superior tenting of bladder wall, and bladder interface hypervascularity on color Doppler (Fig. 3a–c). Among the various MRI signs of placenta accreta (Fig. 4a–c), loss of chemical shift artifacts (“India-ink line”) at the bladder–myometrial interface, was a sensitive and specific sign for detection of vesical wall invasion, identifying 5/6 cases (Tables 5 and 6; Fig. 5a and b). In one of the six cases, disruption of chemical shift artifact could not be assessed properly and was falsely rendered negative for bladder invasion because bladder was catheterized and inadequately distended. Urinary bladder wall tenting was present in only one of the six cases of placenta percreta while loss of myometrial lining was found to be unreliable as it was noted in many normal pregnancies.
(a) Transverse transabdominal sonography shows multiple tortuous irregular anechoic spaces within the placenta suggesting placental lacunae (arrows). (b) Doppler evaluation in the above case did not reveal color flow in these spaces probably due to very slow movement of blood, but moving echoes noted even on grayscale suggests presence of turbulent flow (curved arrow). (c) Most cases would however show a typical high velocity turbulent lacunar flow (solid arrow), as seen in another case. (a) A case of placenta accreta showing dark intraplacental bands (arrows), intraplacental hemorrhages (solid arrow), and placental heterogeneity. (b) Another case of placenta accreta showing bladder tenting (arrow). (c) A case of placenta accreta shows lower uterine bulge anteriorly (arrows) with placental heterogeneity. (a) A case showing normal chemical shift artifact (“India-ink line”) at the bladder–myometrium interface (white arrows). This is due to the intravoxel dephasing of fat and water protons (a normal phenomenon). (b) Loss of chemical shift artifact (“India-ink line”) at the bladder–myometrial interface (small arrows) on T2W MRI, seems to be a sensitive and specific sign for detection of vesical wall invasion by invasive placenta. Prediction of bladder invasion in 22 patients in the study. Statistical analysis of various signs in predicting bladder invasion for 22 patients in this study.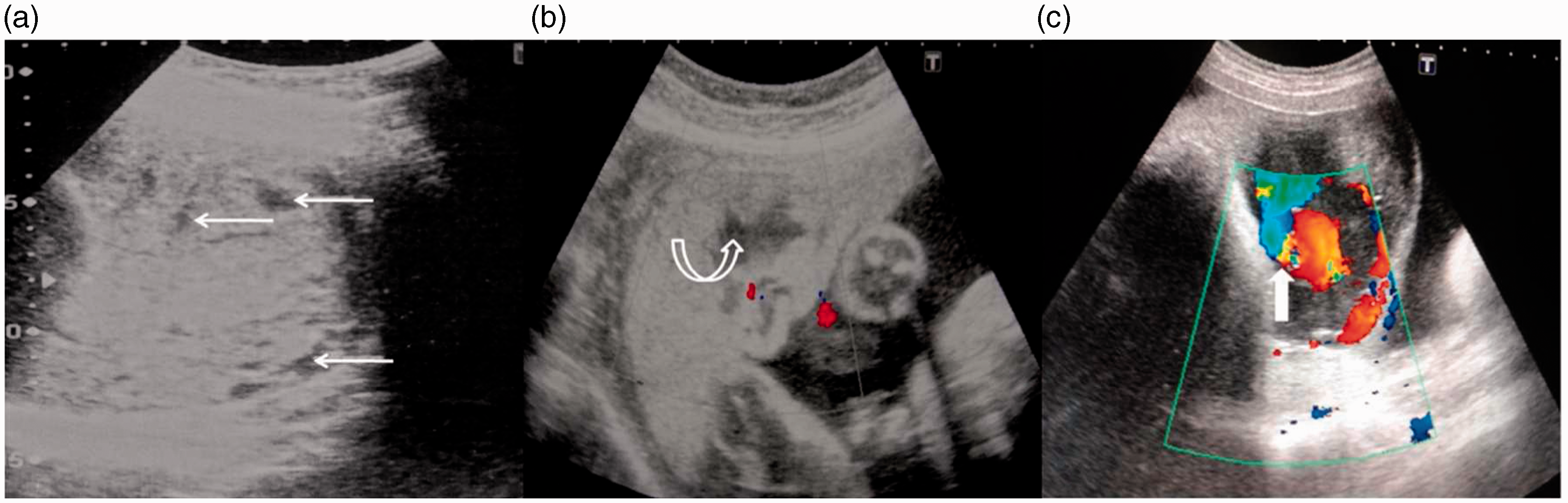

Discussion
Massive obstetric hemorrhage is still the leading cause of pregnancy-related deaths, and placenta previa accreta remains one of the major culprits of pregnancy related bleed (6). Placenta accreta is a potentially life-threatening condition, which includes various abnormalities of placental implantation in which the placenta invades the myometrium. Placenta accreta involves myometrial invasion, placenta increta involves deep myometrial invasion, and placenta percreta invades through the serosal layer of the uterus with potential invasion of adjacent bladder or bowel loops. However, we have used the term “placenta accreta” as a blanket term to describe any amount of abnormal placental invasiveness, as often done in the literature. Accurate identification of extent of invasion helps the surgeons to plan the nature of hysterectomy and thus decreasing blood loss and morbidity.
Ultrasound with color Doppler imaging is presently the mainstay of diagnosis of placenta accreta. Few of the early studies labeled the sensitivity and specificity of sonography to be in the range of 93–100% and 79–94%, respectively (7,8). The ultrasonographic findings described in diagnosis of placenta accreta are presence of placenta previa, lacunae, reduced myometrial thickness, and loss of retroplacental clear space (6–8). However, in our experience, loss of retroplacental space is often found in normal pregnancy, and reduced myometrial thickness, also being a subjective parameter, is unreliable in diagnosing placenta accreta. Furthermore, the interface between the placenta and the myometrium is often focally indistinct, making this sign erroneous.
Irregular anechoic areas within the placenta, i.e. lacunae, were the most predictive ultrasonographic sign to detect placenta accreta in our study with a sensitivity of 100% and a positive predictive value of 82%. These lacunae, first described by Finberg and Williams (7), have been the strongest ultrasonographic findings for placenta accreta. Intraplacental lacunae are indistinct anechoic structures of varying size and shape that are found in the placental parenchyma showing turbulent flow, differentiating them from placental lakes (6,7). Power and color Doppler have been suggested to demonstrate turbulence in placental lacunae in previous studies. Twickler et al. reported that all cases of placenta accreta had turbulent flow in placental lacunae (9). However, in our study, Doppler could demonstrate lacunar turbulence in only 56% (5/9) cases. Lacunar turbulence was more reliably detected by moving internal echogenicity on B mode US, exhibiting 100% sensitivity and 90% positive predictive value. This critical observation in our prospective study was in discordance with the previous studies, which suggested the use of color Doppler and power Doppler. We also tried to demonstrate the lacunar flow on double inversion recovery MRI sequence which failed in the first three cases, leading us to discard this approach. In one of our cases with placenta accreta, US demonstrated only one lacuna with moving echogenicity as a sole finding to point towards placenta accreta. MRI was falsely negative in this case. Various studies have demonstrated that color Doppler imaging along with US has a high sensitivity (82–86%) and specificity (92–97%) in the diagnosis of placenta accreta (3,10). Besides demonstration of lacunar flow, other color Doppler features that have been described to detect placenta accreta are interface hypervascularity, with abnormal blood vessels linking the placenta to the bladder with high diastolic arterial blood flow, markedly dilated peripheral subplacental vascular channels with pulsatile venous-type flow over the uterine cervix, and absence of subplacental vascular signals in the areas lacking the peripheral subplacental hypoechoic zone. All these features were assessed in our study and were found reasonably accurate in the evaluation of placenta accreta. Bladder interface hypervascularity and dilated subplacental vasculature were found in 67% (6/9) cases and disruption of retroplacental flow was found in 78% (7/9) cases.
Abnormally increased vascularity at the placenta–bladder interface is assumed to represent abnormal vessels linking bladder and placenta in cases of placenta percreta (3). However, interface hypervascularity had a positive predictive value of only 67% in detecting bladder invasion whereas it was highly predictive in detection of placenta accreta with a positive predictive value of 100%. Hence, increased vascularity at the placenta–bladder interface might represent subplacental hypervascularity in the myometrium overlying the bladder. This was also supported by the fact that in all six patients in whom dilated subplacental vascularity was found, bladder interface hypervascularity was also simultaneously noted whereas both signs were absent in the other three patients with placenta accreta. Moreover, in the study by Chou et al., this sign yielded two false positive results in detecting placenta accreta owing to bladder varices due to neovascularized vessels from previous Cesarean deliveries (3). Furthermore, this finding is subjective and has a high inter-observer bias since no established criteria has been developed to determine cutoff value of Vmax or RI to define hypervascularity. The major pitfall of US in the evaluation of placenta accreta is unreliability in cases where the placenta is posteriorly located. However, in the present work, we could not confirm this limitation as all the cases in this study had anterior walled placenta.
There have been many studies evaluating the role of MRI in the diagnosis of placenta accreta with reported sensitivities ranging from 38% by Lam et al. to 88% by Warshak et al. (11,12). Dwyer et al. found no statistical difference in the sensitivity or specificity between US and MRI in diagnosing placenta accreta (13). MRI features that have been described to detect placenta accreta are increased placental thickness, exophytic uterine masses, abnormal uterine bulging, intraplacental hemorrhage, dark intraplacental bands, intraplacental flow voids, indistinct bladder wall margin, tenting of bladder, thinning of myometrium seen beneath placenta, marked heterogeneity of placental signal intensity, and indistinct placenta–myometrial interface (4,6,14,15). Of these parameters, we found placental heterogeneity, uterine bulge, dark intraplacental bands, and intraplacental hemorrhages to be the most useful (Fig. 5a–c).
Abnormal uterine bulging had a high sensitivity in our study with only 2/9 cases having normal uterine contour. Bulging has been thought to be due to an abnormally tense myometrium created by the placental invasion or by the frequently thickened and hemorrhagic placenta in these cases (4). Thickness >5 cm was noted in 3/9 cases whereas intraplacental hemorrhages were noted in five cases. All but one of the patients with placenta accreta were found to have dark intraplacental bands on T2W images which is thought to represent abnormal bands of fibrous tissue (4,6). The heterogeneous signal in abnormally invasive placenta could be due to the products of intraplacental hemorrhage and sonographically visible lacunae and was seen in seven cases. It should be noted that the heterogeneity in placenta accreta is distributed throughout the placenta unlike large subchorionic hematoma which may also cause marked placental heterogeneity.
One thing that has not been addressed properly in previous studies is bladder invasion. The importance of diagnosing bladder wall invasion is highlighted from a case in this study in which the bladder could not be evaluated properly due to the presence of an empty bladder with a Foley’s catheter in situ. Surgery had a fatal outcome due to torrential bleed owing to the presence of unanticipated bladder wall invasion by placenta percreta. Since this painful experience, we learned to assess the bladder wall with a full bladder. In cases of bladder wall invasion, hysterectomy is modified by using wide margins of surgical excision to avoid traversing the highly vascular placenta. One important feature in the ultrasonographic diagnosis of placenta accreta invasion is the irregularity and hypervascularity of the uterine serosal–bladder wall complex. No surrogate MRI feature of this sign has been described in the literature. We noticed that in cases of placenta percreta with bladder invasion, loss of chemical shift artifact was noted at the bladder–uterine interface (16). The chemical shift artifact or India ink artifact is seen at the interface of fluid-filled organs or visceral structures with surrounding abdominal fat in GRE sequences such as TrueFISP. This artifact is already being utilized in recognizing fat containing tumors in the brain with CSF interface, in detection of adrenal adenomas, renal angiomyolipomas, and to detect lipomatous metaplasia in patients having myocardial infarction (17,18). Recently, loss of this artifact has been suggested to predict renal capsule invasion by renal cell carcinomas and resectability in mediastinal tumors (5,18). Our study revealed that loss of chemical shift artifact at bladder-myometrial interface predicted bladder invasion in 5/6 cases. This sign could not be optimally evaluated due to collapsed catheterized bladder in the single case in which bladder invasion was missed.
A major limitation of this study was the small sample size; however, for evaluation of this relatively rare entity, a large multi-institutional study would be needed for a prospective study to hold a statistical significance. Another limitation was that the interpretation of imaging features in MRI was made without blinding of the radiologists to the findings of US and color Doppler. The strength of our study was its prospective nature and thus elimination of biases which accompanies in analysis of retrospectively evaluated cohort.
In conclusion, this study shows that both MRI and Doppler sonography are useful for detection of placenta accreta. However, MRI is a better predictor of bladder invasion, thus justifying the use of this expensive investigation in its evaluation.
Footnotes
Acknowledgement
The authors wish to thank Prof. M S Pandey (Professor and Head, Department of English, Faculty of Arts, BHU) for his selfless effort in carefully scrutinizing this manuscript. The authors would also like to acknowledge their team of MR technicians led by Mrs Raichel Luyees for their role in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.