
Abstract
Background
Cardiac and liver iron assessment using magnetic resonance imaging (MRI) is non-invasive and used as a preclinical “endpoint” in asymptomatic patients and for serial iron measurements in iron-overloaded patients.
Purpose
To compare iron measurements between hepatic and myocardial T2* and T2 at 1.5T and 3T MRI in normal and iron-overloaded patients.
Material and Methods
The T2 and T2* values from the regions of interest (ROIs) at mid-left ventricle and mid-hepatic slices were evaluated by 1.5T and 3T MRI scans for healthy and iron-overloaded patients.
Results
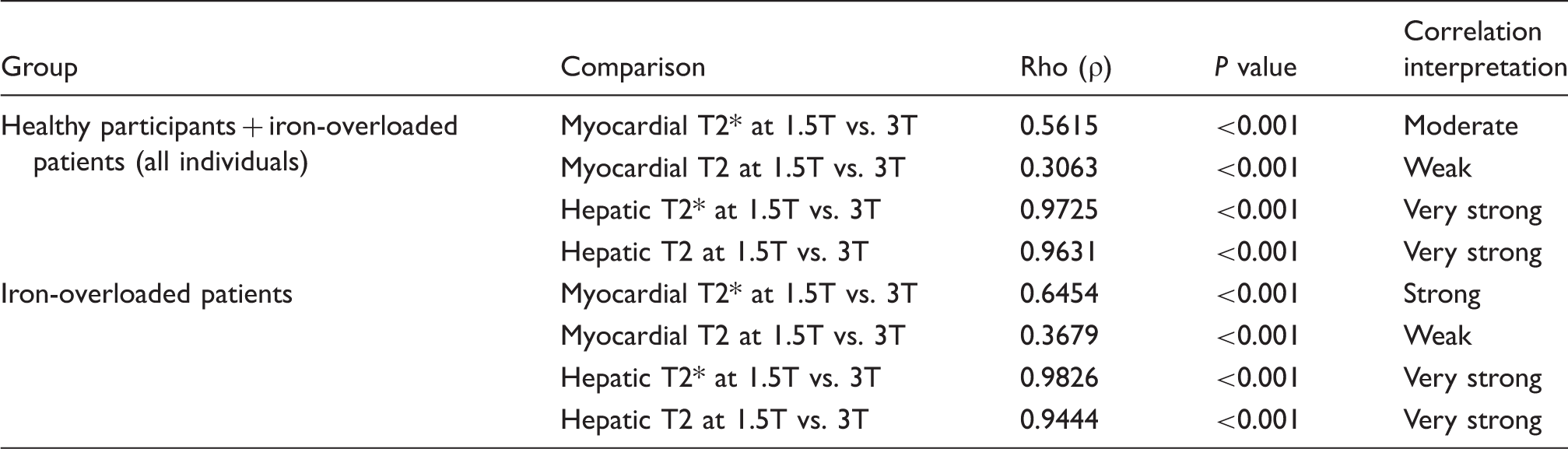
For iron-overloaded patients, the myocardial T2 (1.5T) and myocardial T2 (3T) values were 60.3 ms (range = 56.2–64.8 ms) and 55 ms (range = 51.6–60.1 ms) (ρ = 0.3679) while the myocardial T2* (3T) 20.5 ms (range = 18.4–25.9 ms) was shorter than the myocardial T2* (1.5T) 35.9 ms (range = 31.4–39.5 ms) (ρ = 0.6454). The hepatic T2 at 1.5T and 3T were 19.1 ms (range = 14.8–27.9 ms) and 15.5 ms (14.6–20.4 ms) (ρ = 0.9444) and the hepatic T2* at 1.5T and 3T were 2.7 ms (range = 1.8–5.6 ms) and 1.8 ms (range = 1.1–2.9 ms) (ρ = 0.9826). The line of best fit exhibiting the linearity of the hepatic T2* (1.5T) and hepatic T2* (3T) had a slope of 2 and an intercept of –0.387 ms (R = 0.984).
Conclusion
Our study found myocardial T2 (1.5T) nearly equal to T2 (3T) with myocardial T2* (3T) 1.75 shorter than myocardial T2* (1.5T). The relationship of hepatic T2* (1.5T) and hepatic T2* (3T) was linear with T2* (1.5T) approximately double to T2* (3T) in iron-overloaded patients. This linear relationship between hepatic T2* (1.5T) and hepatic T2 (3T) could be an alternative method for estimating liver iron concentration (LIC) from 3T.
Introduction
Iron overload syndromes include hereditary and acquired conditions (1,2). The liver has high-capacity mechanisms for clearing iron from the circulation in contrast to heart and endocrine tissues. Without chelation therapy, patients die from endocrine and cardiac complications in the second decade of life (3,4). Close monitoring of the iron balance is crucial for chelation therapy (4–6). In recent years, magnetic resonance imaging (MRI) iron quantification has replaced the traditional liver biopsy for measuring liver iron concentration (LIC) due to its higher sensitivity, reproducibility, and availability (3,4). High liver iron values indicate a prospective risk of cardiac dysfunction while low values do not predict the cardiac iron deposition (3).
The more tissue iron, the shorter the signal half-life, and the shorter T2 and T2* become (7,8). Several published studies have reported a curvilinear relationship between liver iron R2 and R2* and LIC by liver biopsies and also suggested a strong internal consistency between R2 and R2* (3,9,10). Variability among the different MRI scanners and manufacturers is small and studies have found have no significant impact on R2 and R2* (11–14). Wood et al. demonstrated that increasing R2 and R2* or shortening T2 and T2* values reflect cardiac iron deposition in human tissue (4,15,16). The relationship between myocardial T2/T2* and left ventricular function has important implications for clinical management (17,18).
Accurately quantifying liver and myocardial T2* at 3T MRI is still challenging because of substantially decreased T2* values and vulnerable quantitation. A recent report using a multiecho fast gradient-echo sequence (MFGRE) at 3T MRI quantifying LIC from hepatic R2* in transfused patients correlated well with clinical blood test results and biopsy results (6). The objective of this study was to determine hepatic T2* at 1.5T versus 3T and hepatic T2 at 1.5T versus 3T in normal participants and iron-overloaded patients and myocardial T2* at 1.5T VS 3T and myocardial T2 at 1.5T VS 3T in normal participants and iron-overloaded patients.
Material and Methods
Patients and study design
The study enrolled iron-overloaded patients suffering from primary or secondary hemochromatosis. Patients with congenital heart disease or contraindications for MRI were excluded. All participants were prospectively recruited from patients referred for LIC and cardiac siderosis screening or being followed up for these conditions. All participants provided written informed consent before MRI scanning and had successful MRI scans at both 1.5T and at 3T. The 3T MRI scans were obtained within 1 h after finishing the 1.5 T scans. A group of 20 healthy volunteers were scanned to establish normal ranges for hepatic T2 and T2* and myocardial T2 and T2* values in 1.5 T and 3T MRIs. Serum ferritin levels were recorded in the patient group. MRI hepatic T2* values at 1.5 T MRI greater than 6.3 ms were categorized as normal (T2* > 6.3 ms), mild hepatic iron overload (2.8–6.3 ms), moderate hepatic iron overload (1.4 – < 2.8 ms) or severe hepatic iron overload (T2* < 1.4 ms) (19,20). The classification for cardiac iron overload by cardiac T2* measurement at 1.5 T MRI were: normal = >20 ms, mild = 15–20 ms, moderate = 10–14 ms, and severe = <10 ms (21). The study protocol was approved by the Institutional Human Research Ethics Committee of our hospital.
Image acquisition
The study was conducted with two scanners, a 1.5T MRI (Ingenia, Philips Medical Systems, Best, The Netherlands) and a 3T MRI (Achieva XR-series, Phillips Medical Systems). The 3T MRI has no multi-transmitted excitation. Each participant was scanned at the short axis of the mid-left ventricular chamber and a mid-hepatic slice was taken using a 32-channel digital stream (dS) – Torso coil solution for 1.5T MRI scanning and using a 16-channel sense XL – Torso coil for 3T MRI scanning.
T2* sequence acquisition: The mid-left ventricular chamber was scanned in the short axis using a respiratory navigator with ECG synchronizing at the mid-diastolic phases and free breathing single-slice with multi-echoes using the spoiled gradient echoes technique. The imaging parameters for 1.5T were: TR/TE first/delta TE = 18/2.6/2.02 ms, echo times = 8, flip angle (FA) = 20° and the black blood or double inversion recovery (DIR) technique to distinguish myocardium from blood flow, slice thickness = 10 mm, field of view (FOV) = 400 mm, acquisition matrix size = 132 × 256 pixels, and number of signal averages (NSA) = 1. Three-dimensional (3D) volume shimming was used for B0 inhomogeneity compensation. Average scan time was 13 s. The imaging parameters for 3T were: TR/TE/delta TE = 25/0.752/1.523 ms, and acquisition matrix size = 200 × 200 pixels. The NSA of about 6–12 was optimized for the image depending on patient size, patient cooperation, and contrast-to- noise ratio. Average scan time was 2–3 min.
The imaging parameters of the 1.5T liver scan were: TR/TE first/delta TE = 25/1.071/1.097 ms, echo times = 20, FA = 20°, slice thickness = 10 mm, FOV = 360 mm, acquisition matrix size = 128 × 256 pixels, NSA = 6, and echo train length (ETL) = 8. Average scan time was 14 s for breath-holding and 8 min for free breathing. The imaging parameters of the 3T liver scan were: TR/TE/delta TE = 9.15/0.583/0.679 ms, echo times = 12, ETL = 12, acquisition matrix size = 121 × 132 pixels, and NSA = 6. Average scan time was 2–3 min.
T2 sequence acquisition: The participants were scanned using a black blood single slice with multi echoes in turbo spin echo sequence. The position and geometry parameters were the same as formerly used in the myocardial T2* measurements. The parameters of T2 TSE in 1.5T were TR/TE/delta TE = 2–3 cardiac cycles/3.9/3.9 ms, acquisition matrix size = 152 × 150 pixels, and NSA = 1, and the data were acquired at the end-expiration with expiratory hold. The turbo factor was 12 and the sense factor was 2. Average scan time was 3–4 min. The parameters of T2 TSE in 3T were: TR/TE first/delta TE = 2–3 cardiac cycles/6.7/6.7 ms, echo times = 12, FA = 90°, slice thickness = 10 mm, FOV = 400 mm, acquisition matrix size = 200 × 200 pixels, NSA = 10, and ETL = 12. Average scan time was 5–6 min.
For the liver scans, the parameters of T2 TSE in 1.5T were TR/TE first/delta TE = 1000/3.924/3.924 ms, echo times = 12, FA = 90°, slice thickness = 10 mm, FOV = 400 mm, acquisition matrix size = 200 × 200 pixels, NSA = 2, and ETL = 12. Average scan time was 5–6 min. There were a few different parameters for 3T MRI: TR/TE first/delta TE = 1000/6.238/6.238 ms, and acquisition matrix size = 160 × 160 pixels. Average scan time was 5–7 min.
T2* and T2 measurement method: The gradient echo images were analyzed by MATLAB (The MathWork, Natick, MA, USA) and fit to mono-exponential and offset equations as follows:

The general equation to add a variable offset was

The T2 measurements by Equations 1 and 2 were fit by the same method as above,

Statistical analysis
The statistical analysis was performed using R software 3.3.0 (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables are presented as median and interquartile range (IQR). Patient characteristics were analyzed by Wilcoxon rank-sum for continuous variables after using the Shapiro–Wilk test for determining the normal distributions. Pearson's Chi-squared test was used for gender comparisons. The relationships between T2 and T2* values in 1.5T and 3T were tested by Spearman’s rho analysis. T2 and T2* values were plotted using the MATLAB Statistical Toolbox. P value <0.05 was considered statistically significant
Results
Patient characteristics.
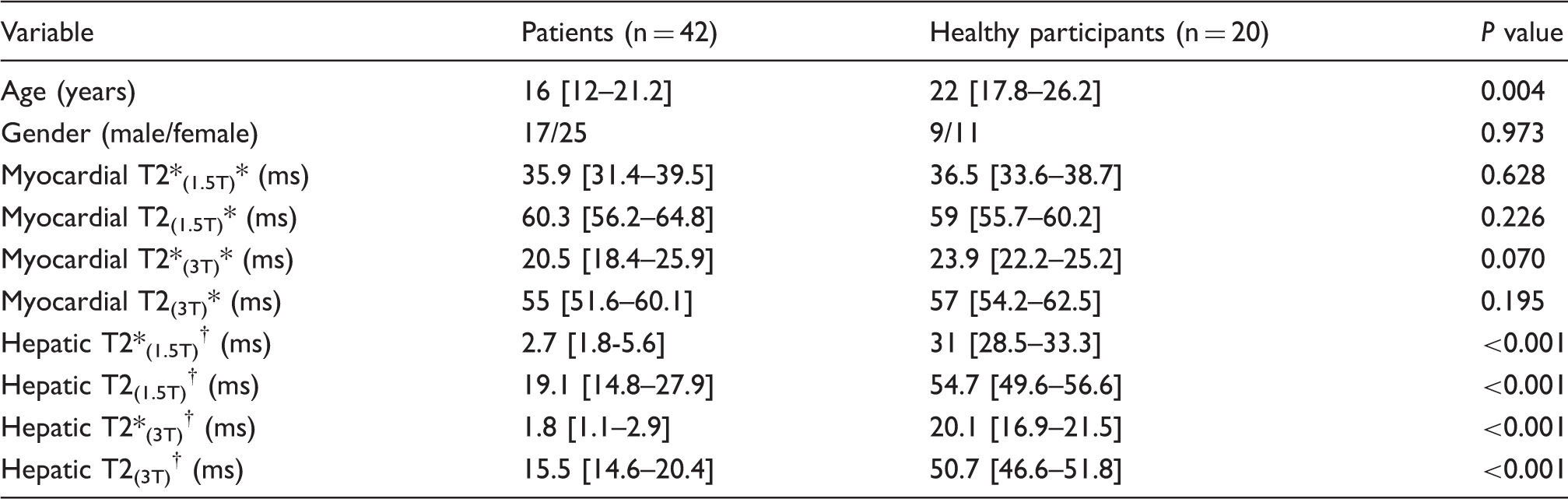
Data are expressed as median [interquartile range].
Myocardial T2* and T2 values were analyzed from 44 MRI studies.
Hepatic T2* and T2 values were analyzed from 35 MRI studies.
Myocardial T2* and T2: The median values of myocardial T2 at 1.5T, myocardial T2 at 3T, myocardial T2* at 1.5T, and myocardial T2* at 3T in patients and healthy participants are shown in Table 1.
The Spearman Rho correlation between myocardial T2 and T2* at 1.5T vs. 3T and hepatic T2 and T2* at 1.5T and 3T in all individuals and in the groups of iron-overloaded patients.
Hepatic T2* and T2: The median values of hepatic T2 at 1.5T, hepatic T2 at 3T, hepatic T2* at 1.5T, and hepatic T2* at 3T in healthy participants and patients are shown in Table 1.
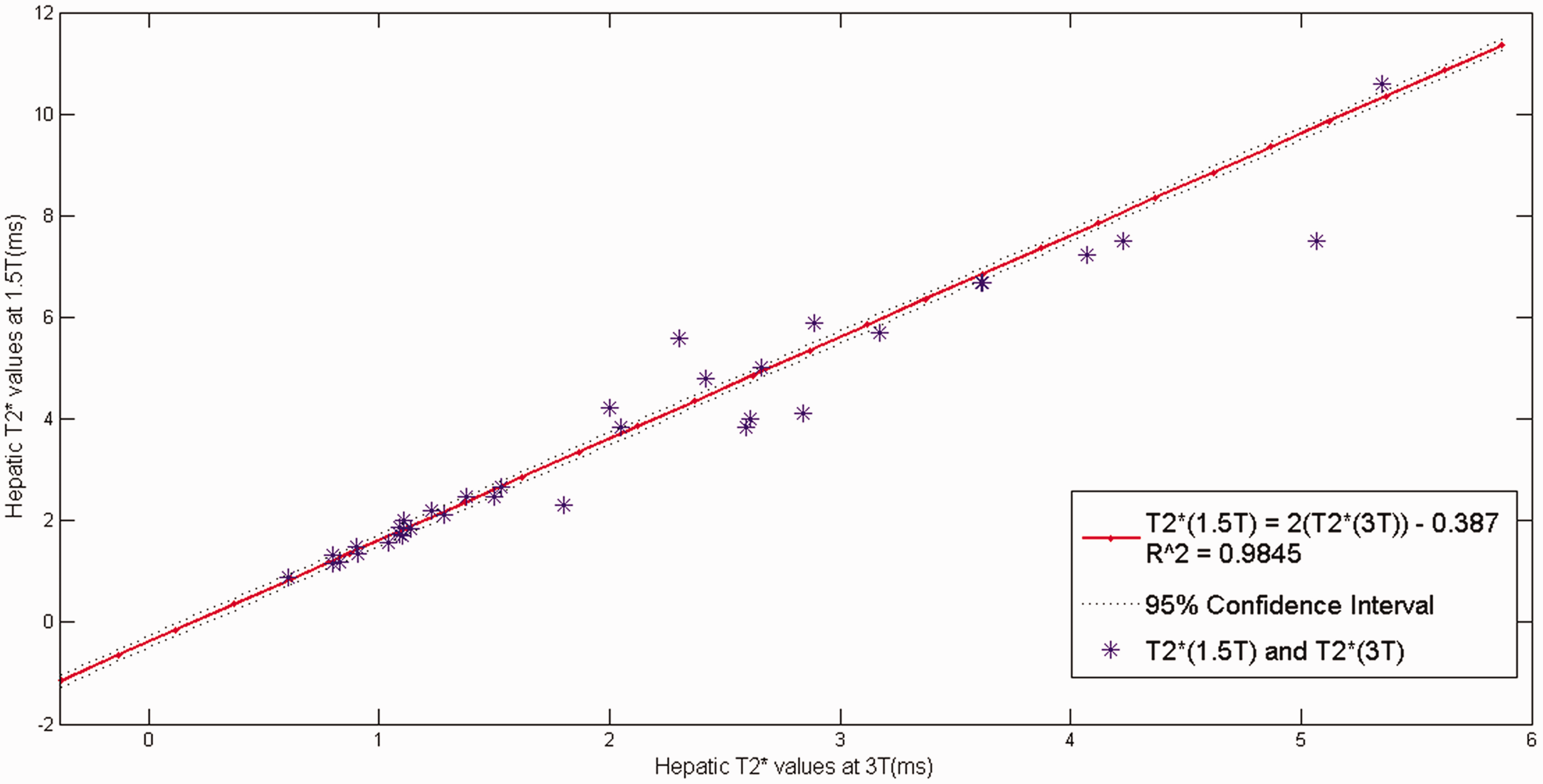
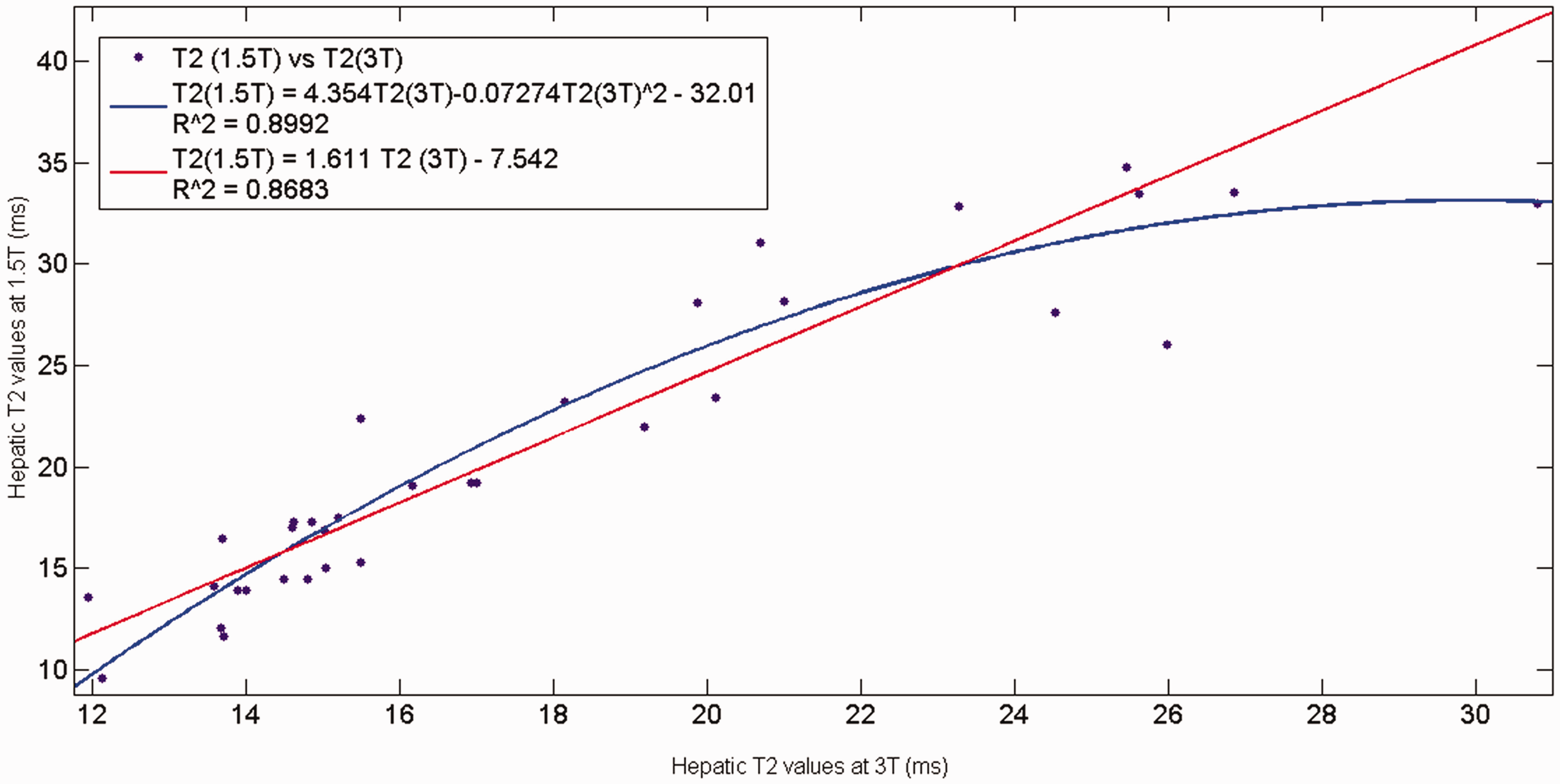
The relationship between hepatic T2 and T2* at 1.5T and 3T: The Spearman-rho analyses of the correlations between hepatic T2* at 1.5T and hepatic T2* at 3T and hepatic T2 at 1.5T and hepatic T2 at 3T in normal participants and iron-overloaded patients are shown in Table 2. The lines of best fit of hepatic T2* values at 1.5T versus 3T in healthy participants and iron-overloaded patients exhibiting the linearity had a slope of 1.558 and an intercept of +0.3971 ms (R = 0.990) (Fig. 1). The line of best fit of hepatic T2 values at 1.5T versus 3T in healthy participants and iron-overloaded patients had a slope of 1.077 + 1.461 (R = 0.9461) (Fig. 1). In addition, the line of best fit of hepatic T2* values at 1.5T versus 3T in iron-overloaded patients had a slope of 2 and an intercept of (–) 0.387 ms (R = 0.984) (Fig. 2). However, the relationship between hepatic T2 values at 1.5 T versus 3T in iron-overloaded patients had the linear fit curve (R = 0.8683) and the quadratic function (R = 0.8992) (Fig. 3).
Relationship between hepatic T2* and hepatic T2 in healthy participants and iron-overloaded patients. The line of best fit of hepatic T2* values (blue, upper line) at 1.5T and 3T in healthy participants and iron-overloaded patients has a slope of 1.558 + 0.397 (R = 0.990) and the line of best fit of hepatic T2 values (red, lower line) at 1.5T vs. 3T in healthy participants and iron-overloaded patients has a slope of 1.077 + 1.461 (R = 0.9461). Relationship between hepatic T2* values at 1.5T and 3T in iron-overloaded patients. The line of best fit of hepatic T2* values at 1.5T and 3T in iron-overloaded patients has a slope of 2 and an intercept of (–) 0.387 (R = 0.984). Relationship between hepatic T2 values at 1.5T and 3T in iron-overloaded patients. The linear fit curve is shown by the red line (R = 0.8683) and the quadratic function is shown by the blue line (R = 0.8992).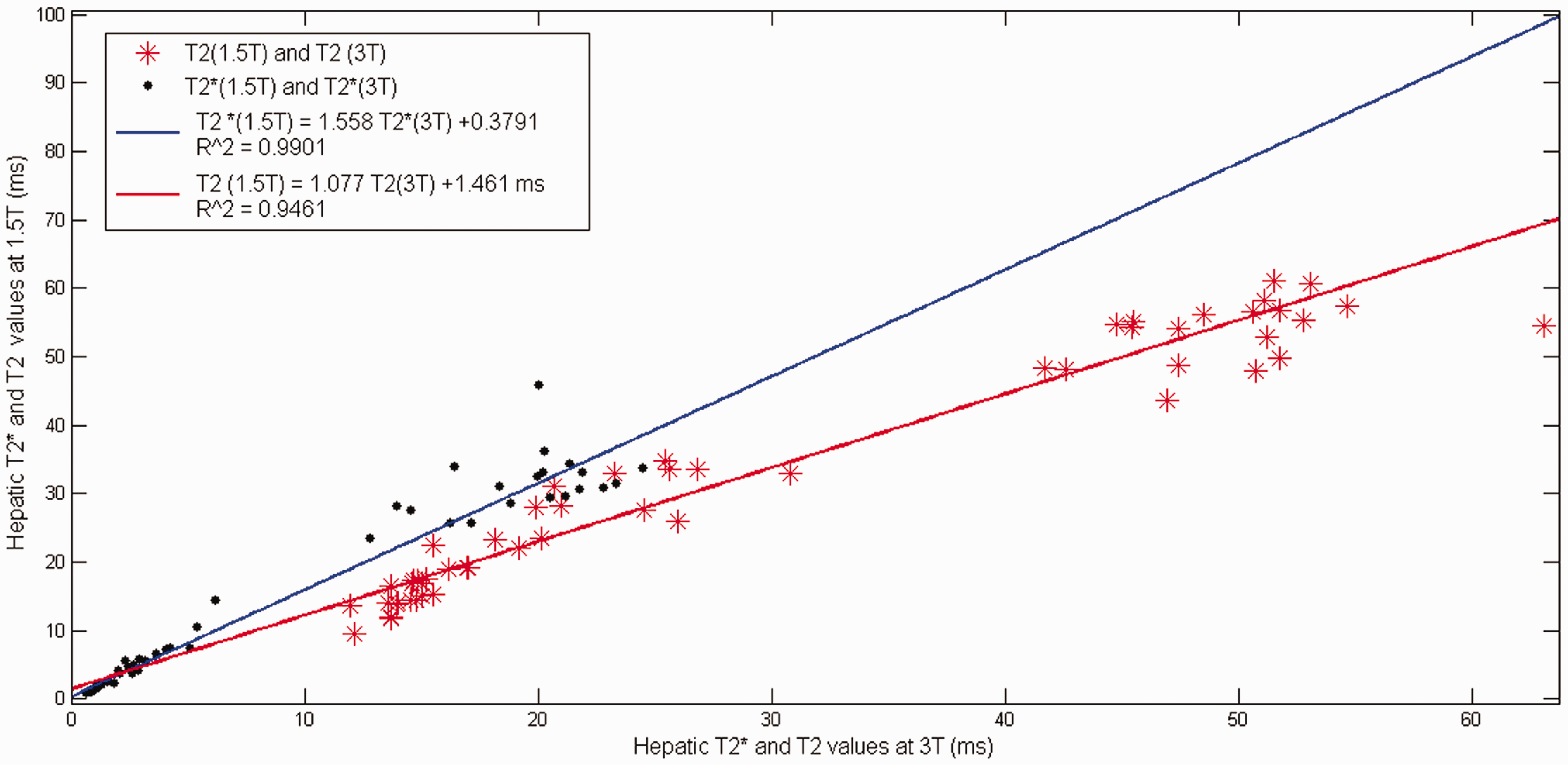
Discussion
Our study aimed to determine the relationship in myocardial and liver T2 and T2* between 1.5T versus 3T in iron-overloaded patients. In this study, the myocardial T2* and T2 at 1.5T and 3T showed no significant differences between normal participants and patients, all values being within a small range (16.7–48.2 ms for myocardial T2* at 1.5 T, 9.3–31.5 ms for myocardial T2* at 3T, 27.4–86.1 ms for myocardial T2 at 1.5T, and 30–75.5 ms for myocardial T2 at 3T), not covering very low T2*/T2 values or high cardiac iron overload. Due to these small differences with the subsequent low R-squared values, it was not possible to establish a reliable assessment relationship between myocardial T2 and T2* at 1.5T versus 3T. However, the myocardial T2 values at 1.5T and 3T in both healthy participants and patients were nearly equal, suggesting that T2 values are independent of the magnetic field because the spin-echo technique is insensitive to magnetic field inhomogeneities (22). Furthermore, the myocardial T2* values at 3T from our study were about 1.75 times shorter than the myocardial T2* values at 1.5T (myocardial T2*(1.5T)/T2*(3T) median ratio = 35.9/20.5). This observation is consistent with a previous study by Guo et al. which found a linear correlation with a slope of 0.61 ± 0.03 (R = 0.95) and zero intercept in the linear fitting curve of 3T of T2* versus 1.5T of T2* in the myocardium (8).
The hepatic T2* value has high sensitivity to detect iron overload and is directly proportional to iron concentration (4). However, the first TE and delta TE need to be adjusted for a liver scan, particularly at 3T in very high iron-content patients (hepatic T2* < 3 ms) (4). A few studies have reported a strongly significant linear relationship between R2* and T2* values at 1.5T and at 3T in transfused patients (23–25). The hepatic T2* at 1.5T plotted against the corresponding hepatic T2* at 3T for normal participants and iron-overloaded patients shows a linear relationship having a slope of 1.558 and an intercept of +0.3971 ms (Fig. 1). The expression of this relationship can be expressed as

Equation 4 shows that our study had approximately 1.558 times greater hepatic T2* at 1.5T than hepatic T2* at 3T in both normal and iron-overloaded patients. Particularly for the iron-overloaded patients, the relationship of hepatic T2* between 1.5T and 3T had a linear correlation with a slope of 2 and intercept of (–) 0.387 (Fig. 2) and can be expressed as

Equation 5 shows hepatic T2* at 1.5T having a slope twice that of T2* at 3T and a small intercept (–0.387) for the 95% confidence interval. Our findings are consistent with those of a previous report of Storey et al. in which the line of best fit to the R2* at 3T and 1.5T data had a slope of 2.00 ± 0.06 and an intercept of (−) 11 ms (25). Therefore, we can say that the hepatic T2* at 3T is approximately twice the hepatic T2* at 1.5T in iron-overloaded patients (3,7,24,25).
Determining the relationship of T2 between 1.5T and 3T is a complicated analysis due to confounding factors even in the normal hepatic T2 at 1.5T and 3T. A previous report by de Bazelaire et al. found that the T2 relaxation times at 3T were 8% shorter than at 1.5T in normal liver parenchyma (26). The mean value of hepatic T2 at 3T of the normal participants in our study was about 92% lower than 1.5T (hepatic T2(3T) = 49.63 ms/hepatic T2(1.5T) = 53.74 ms), which is consistent with the study by de Bazelaire et al. For the hepatic T2 values at 1.5T and 3T in normal participants and iron-overloaded patients, all measurement points were found to fit well in a linear curve (Fig. 1). However, the relationship of hepatic T2 at 1.5T and 3T in iron-overloaded patients was not strong enough for linearity regarding to low R-squared values (Fig. 3). We suggest not using the conversion between T2 at 1.5T and T2 at 3T due to low R-squared values and unreliable prediction. Nevertheless, because of less variation and independence of the magnetic field strength of T2, the T2 value could be an alternative for use at high and ultra-high-field strengths due to its lower susceptibility and less B0 and B1 inhomogeneities (3,4,9). The T2 values are different from the T2* values which are dependent on the field strength and require adjustment to decrease TE and delta TE; therefore, the T2* is a drawback to an ultra-high-field strength MRI. However, the technical improvement when scanning the heart using T2 spin echo sequence still involves challenges due to motion artifacts and lower signal-to-noise ratio.
We attempted to determine if there were any cross-correlations between hepatic T2* at 1.5T and T2 at 3T in iron-overloaded patients. All measurements of hepatic T2* at 1.5T and hepatic T2 at 3T values in iron-overloaded patients were plotted (Fig. 4) giving the linear correlation with a slope of 0.8058 and the intercept (–9.76) and R = 0.9687 which can be expressed as
Cross-correlation of the heaptic T2* values at 1.5T and T2 values at 3T in the iron-overloaded patients.

The hepatic T2* value at 1.5T is used for accurate estimates of the LIC, as suggested in the report of Wood et al. (9). Our study found a linear relationship between hepatic T2* at 1.5T and hepatic T2 at 3T. For clinical use, it could be very advantageous for hospitals or situations not having an available 1.5T machine to be able to get an accurate assessment based on hepatic T2* at 1.5T. We can convert the T2 value at the 3T to the T2* of 1.5T from Equation 6 and then eventually estimate the LIC. It is also useful for very high iron-overloaded patients in which the hepatic T2* value is not accurate for LIC estimation (3,24).
There are a few limitations of this study. The median ages of the healthy participants and patients were significantly different because the normal volunteers included only participants aged >15 years with good cooperation in the scanner and the patient group included children and adults. Our study also had only a small number of severe cardiac iron-overloaded patients, leading to our being unable to establish a reliable relationship between myocardial T2 and T2*. We suggest further studies with large populations or multicenter collaborations which will be able to obtain a larger sample of severe cardiac iron-overloaded patients.
In conclusion, this study confirms the possibility of a relationship between myocardial and hepatic T2 and T2* at 1.5T and 3T. The relationship of hepatic T2*(1.5T) showed linearity to hepatic T2*(3T) with T2*(1.5T) approximately double to T2*(3T) in iron-overloaded patients. The relationship of hepatic T2 at 1.5T and 3T was not strong enough for linearity. The linear relationship between hepatic T2*(1.5T) and hepatic T2(3T) could be an alternative to accurately estimating LIC from 3T. The preliminary results found myocardial T2 was nearly equal at 1.5T and 3T and myocardial T2* at 3T was 1.75 times shorter than 1.5T.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for this research from the Faculty of Medicine, Prince of Songkla University.