
Abstract
Background
Knowledge-based iterative model reconstruction (IMR) is known to allow radiation dose reduction while preserving image quality.
Purpose
To investigate the effect of IMR on coronary computed tomography angiography (CCTA) by comparing it with filtered back projection (FBP) and hybrid iterative reconstruction (HIR).
Material and Methods
Forty-five patients (group A) who underwent CCTA with prospective electrocardiogram (ECG) triggering at 80 kVp were included. All images were reconstructed using three algorithms: FBP, HIR, and IMR. The control group comprised 45 patients (group B) who underwent CCTA at 100 kVp; their images were reconstructed with HIR alone. Objective and subjective image quality was assessed by two radiologists.
Results
In group A, the signal-to-noise and contrast-to-noise ratios were significantly higher for images reconstructed with IMR than with HIR or FBP (P < 0.001). IMR was also superior to HIR and FBP in subjective image quality analyses, including image noise, vessel sharpness, beam-hardening artifact, and overall quality (P < 0.001). Moreover, the images reconstructed using IMR in group A had superior image quality with less radiation exposure than those reconstructed using HIR in group B on both objective and subjective analyses (P < 0.001). The mean attenuation values were also significantly higher in group A than in group B (P < 0.001).
Conclusion
Compared with HIR and FBP, IMR provided higher quality images with less radiation exposure in CCTA, using low kilovoltage and prospective ECG triggering.
Keywords
Introduction
Coronary computed tomography angiography (CCTA) is a widely used non-invasive and accurate anatomic imaging modality to assess coronary artery disease (CAD) and cardiac structures in selected patients (1). However, inevitable radiation exposure and its potential carcinogenic risks are major limitations of CCTA (2). To overcome this issue, various computed tomography (CT) protocols and new technologies have been developed, including the prospective electrocardiogram (ECG) triggering mode, tube current and peak kilovoltage (kVp) modulation, and iterative reconstruction algorithms (3–8). In particular, numerous hybrid statistical iterative reconstruction algorithms that allow radiation dose reduction while preserving image quality have been developed (5,9). The recently developed model-based iterative reconstruction (MBIR) or knowledge-based iterative model reconstruction (IMR), which is an advanced CT image reconstruction method, has yielded numerous promising results (10–14). However, indiscriminate application of MBIR or IMR in routine clinical practice remains controversial. Indeed, some argue that IMR may produce several unique artifacts, and its image quality is relatively inferior to that of conventional reconstruction algorithms (15,16).
We hypothesized that the combined use of a low-voltage technique, prospective ECG triggering mode, and IMR could provide diagnostic image quality with significant radiation dose reduction. This study aimed to evaluate the subjective and objective image quality of CCTA acquired using low tube voltage (80 kVp) and prospective ECG triggering, reconstructed with FBP, HIR, and IMR. Furthermore, we compared the image quality of low-tube-voltage (80 kVp) CCTA images reconstructed using IMR with that of conventional-tube-voltage (100 kVp) CCTA images reconstructed using HIR.
Material and Methods
This study was performed at a single tertiary referral institution before and after changing the CCTA scanning protocol. The changes in protocol were as follows: reduction of kVp (100 kVp to 80 kVp) and application of different iterative reconstruction algorithms (HIR to IMR). Our institutional review board approved this prospective/retrospective study. All participants who underwent low-tube-voltage (80 kVp) CCTA provided informed consent for inclusion in the prospective study. The requirement for informed consent was waived for patients whose conventional-tube-voltage (100 kVp) CCTA images were retrospectively reviewed.
Patient selection
Between August 2013 and November 2013, we prospectively included 45 patients (M:F = 28:17; age = 56.2 ± 10.3 years; group A) who underwent low-tube-voltage (80 kVp) CCTA with prospective ECG triggering. Three image sets for each patient were obtained using different algorithms: FBP, HIR, and IMR. The inclusion criteria were as follows: (i) body mass index (BMI) <30 kg/m2; (ii) heart rate ≤65 beats per minute (bpm); and (iii) heart rate difference ≤20 bpm. Patients were excluded if they refused informed consent or had undergone bypass graft surgery, percutaneous coronary angioplasty, or stenting for prior CAD. Patients who had arrhythmia, hemodynamic instability, anticipated risk of iodinated contrast agents such as renal insufficiency or known allergy to iodinated contrast, and contraindications to beta blocking agents, were also excluded.
For the selection of control group, we retrospectively identified 505 patients who had undergone conventional-tube-voltage (100 kVp) CCTA with prospective ECG triggering between February 2013 and August 2013. Thirty-two patients were excluded because of high BMI and heart rate. Twenty-six patients with a history of percutaneous coronary angioplasty and two patients who had undergone bypass graft surgery were also excluded. After matching for age, sex, and heart rate, 45 consecutive patients were included in group B (Supplemental materials and Fig. 1).
Flowchart illustrating patient enrollment.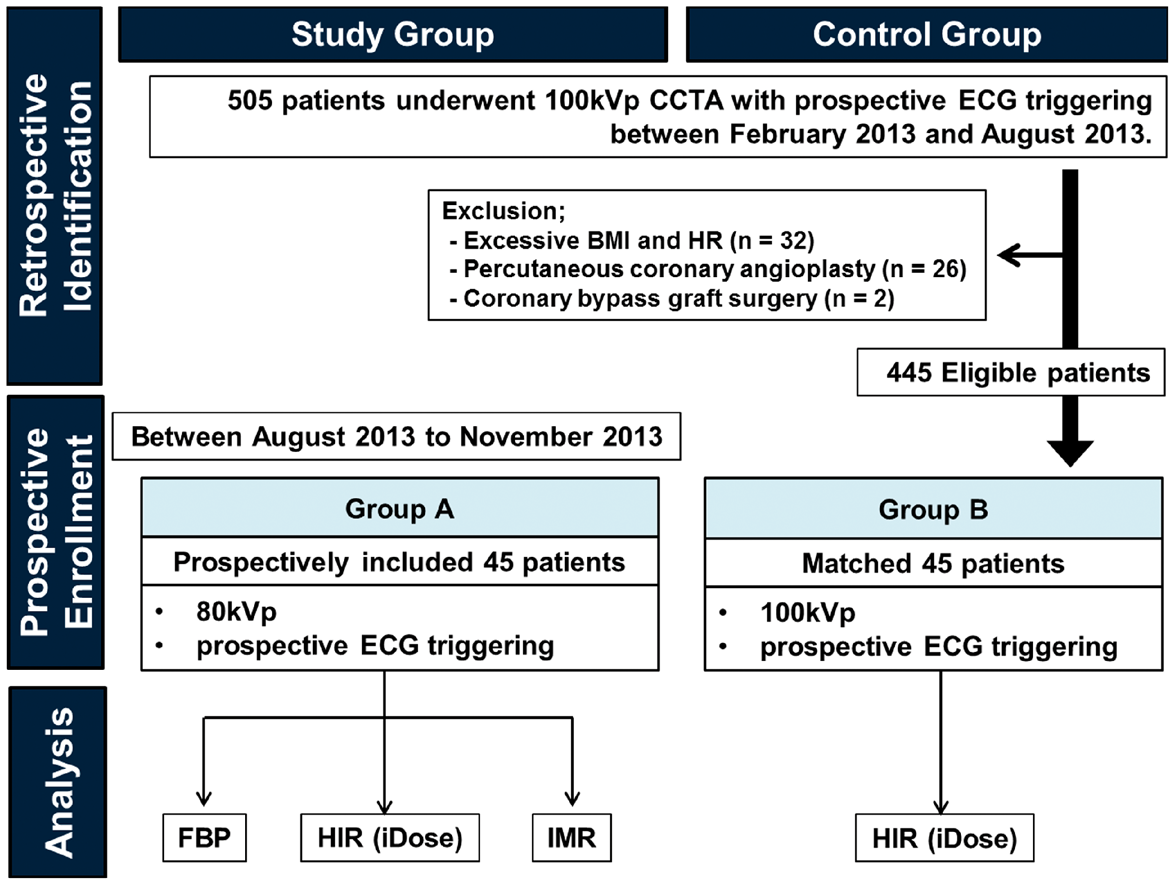
CCTA protocols and data acquisition
The CCTA datasets were acquired using a 256-slice CT machine (Brilliance-iCT; Philips Healthcare, Cleveland, OH, USA) with the following parameters for group A: tube voltage = 80 kVp, tube current–time product = 50–130 effective mAs, collimation = 0.625 mm × 128, tube rotation time = 0.27 s, slice thickness = 0.9 mm, and reconstruction increment = 0.45 mm; and for group B: tube voltage = 100 kVp, tube current–time product = 90–160 effective mAs, collimation = 0.625 mm × 128, tube rotation time = 0.27 s, slice thickness = 0.9 mm, and reconstruction increment = 0.45 mm. The tube current–time product was determined by considering each patient’s body weight and the use of phase tolerance (supplemental materials). Prior to CCTA, patients with a heart rate >65 bpm were administered oral ß-receptor blockers (12.5–25 mg metoprolol succinate; AstraZeneca, Sweden) and every patient received 0.4–0.8 mg of nitroglycerin sublingually. Using the bolus tracking technique (Bolus Pro Ultra; Philips Healthcare), the contrast-enhanced scanning was initiated after 9 s of triggering with a trigger threshold of 110 Hounsfield Units (HU) in the ascending aorta. Approximately 50–70 mL (Iomeron 400, 400 mg iodine/mL; Bracco Imaging SpA, Milan, Italy) of contrast agent was injected through an antecubital vein (injection rate = 4.5–5 mL/s) followed by a 50-mL 1:1 mixed contrast saline chaser (4 mL/s) by using a dual-head power injector (Stellant; Medrad, Pittsburgh, PA, USA). We reconstructed the raw data from group A at the phase of least cardiac motion within the mid-diastole phase (73–83% of the R-R interval), a 20-cm field of view, 512 × 512 pixel matrix, 0.9-mm slice thickness, and 0.45-mm image increments with FBP, HIR (iDose4; Philips Healthcare), and IMR (IMR; Philips Healthcare) algorithms by using an Xres smooth filter. The iterative reconstruction levels reflecting noise reduction power were level 7 for iDose4 and level L2 for IMR, which were determined based on the consensus of two cardiothoracic radiologists.
Objective evaluation of image quality
For objective analysis, image noise, signal-to-noise ratio (SNR), and contrast-to-noise ratio (CNR) were evaluated. Circular regions of interest (ROIs) were manually drawn on the axial plane and placed over the proximal and distal segments of the coronary arteries, including the right coronary (RCA), left anterior descending (LAD), and left circumflex (LCX) arteries, ascending aorta, and left ventricular (LV) lumen at the mid-ventricular level. Care was taken to place ROIs that were not too small to be affected by pixel variability but not too large to include adjacent structures. The standard deviation (SD) and mean attenuation values of all ROIs were recorded. Measurements were performed three times to minimize measurement bias and the average values were recorded for analyzing the results. Image noise was defined as the SD of each ROI. SNR was calculated as the mean CT attenuation value divided by image noise of the corresponding structures. For the acquisition of CNR, the mean CT attenuation of adjacent perivascular soft tissue of the coronary arteries and LV myocardium were obtained. CNR was calculated using the following formula: CNR = (ROIv – ROIa)/Nv, where ROIv is the mean CT attenuation of the coronary arteries or LV lumen, ROIa is the mean CT attenuation of adjacent perivascular soft tissue or LV myocardium, and Nv is the image noise of the coronary arteries or LV lumen.
Subjective evaluation of image quality
Axial scans, curved multiplanar reformatted images, and cross-sectional images to the long axis of the coronary arteries were prepared for evaluating CAD. Two radiologists with ten years of experience in cardiothoracic imaging independently analyzed the images with a window level of 60 HU and window width of 360 HU. The images were assessed from four aspects into consideration: (i) image noise; (ii) beam-hardening artifact; (iii) vessel sharpness; and (iv) overall image quality. A four-point scale, allocated in accordance with the Society of Cardiovascular Computed Tomography guidelines, was applied. Image noise and beam-hardening artifact were graded as 1 = present and unacceptable, 2 = present and interfering with the depiction of coronary arteries, 3 = present but not interfering with the depiction of coronary arteries, and 4 = minimal or absent. Vessel sharpness was defined as 1 = blurry, 2 = poorer than average, 3 = better than average, and 4 = sharpest. Overall image quality was graded as 1 = unacceptable (inadequate to evaluate coronary stenosis), 2 = fair (sufficient for evaluating coronary stenosis), 3 = good, and 4 = excellent. Motion artifacts were ignored as much as possible. Disagreements between the two observers were resolved by a consensus.
To determine inter-observer agreement, subjective image quality measurements of 20 randomly selected images were obtained by two observers on different days separated by at least two weeks.
CT radiation dose
The CT dose index volume and dose length product (DLP) were recorded. Effective dose was obtained by multiplying DLP with the conversion coefficient (k, 0.014 mSv/mGy ċ cm in the cardiothoracic area).
Statistical analysis
SPSS for Windows (Version 7.5; SPSS Inc., Chicago, IL, USA) was used for statistical analyses. Data were expressed as mean ± SD, numbers, or percentages. Age, sex, average heart rate, BMI, scanning length, radiation dose, qualitative image quality scores, and quantitative image quality parameters such as mean CT attenuation, SNR, and CNR were compared using Student’s t-test and Mann–Whitney U test between groups. For comparing image quality scores and quantitative parameters among the three reconstruction algorithms within group A, paired Student’s t-test and Wilcoxon signed-rank test were used. Kappa analysis was used to compute inter-observer reliability. A P value <0.05 was considered statistically significant.
Results
Patient characteristics and CT radiation dose
Baseline characteristics.
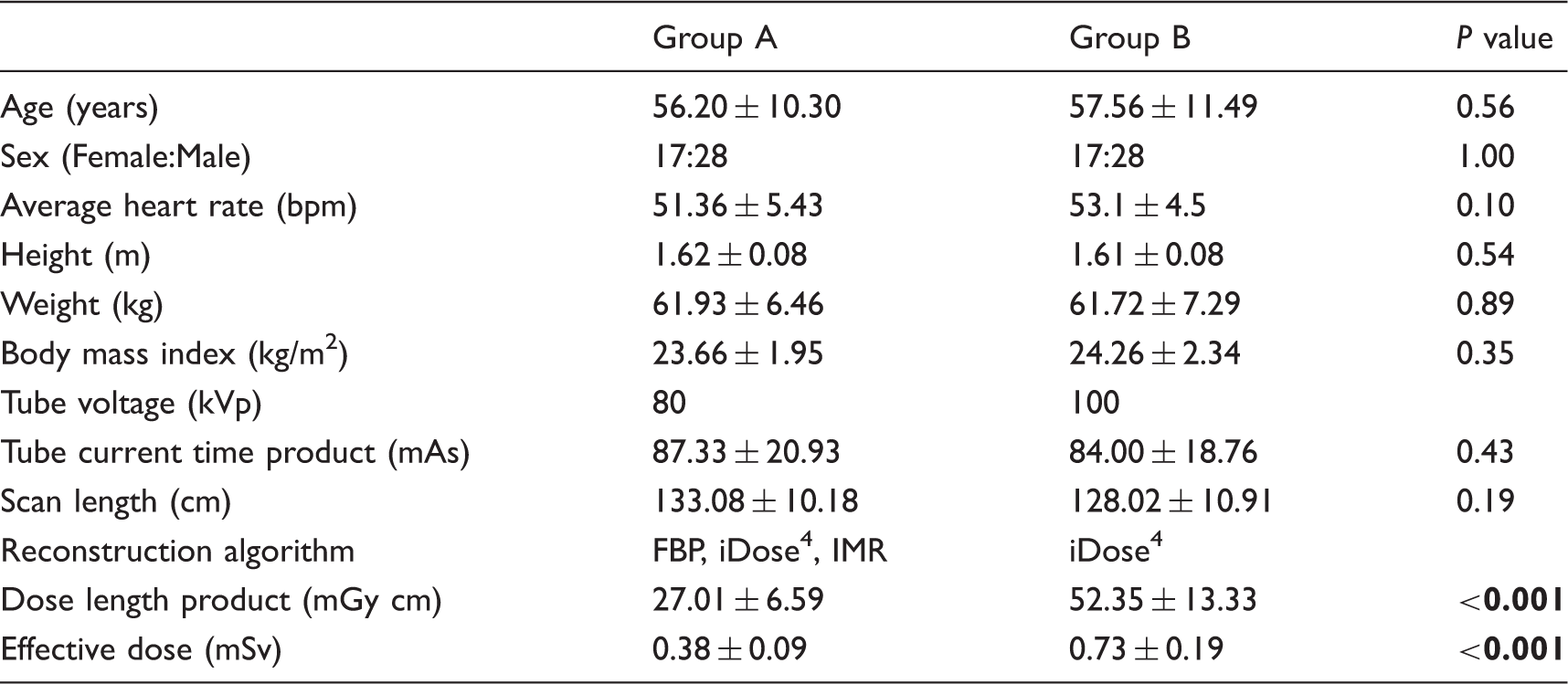
Bold P value <0.05.
FBP, filtered back projection; iDose4, hybrid iterative reconstruction; IMR, iterative model reconstruction.
Objective analysis
The mean CT attenuation values and the CNR and SNR of the aorta, LV lumen, and proximal and distal segments of the coronary arteries obtained using the three reconstruction algorithms in both groups are shown in Supplemental Table 1. The mean CT attenuation values of the aorta and LV cavity were not significantly different among the three reconstruction algorithms. Most of the CT attenuation values of the proximal and distal coronary arteries did not differ significantly either. However, the proximal RCA, LAD, and LCX showed higher CT attenuation values with FBP than with HIR (P = 0.04, P = 0.03, and P = 0.02, respectively). Additionally, the CT attenuation of the proximal LAD and distal LCX were significantly higher on images reconstructed with FBP than with IMR (P = 0.03 and P = 0.02, respectively). All of the CNR and SNR values were significantly higher with IMR than with HIR and FBP (all of P < 0.001). Moreover, the CNR and SNR were significantly higher for images reconstructed using HIR than with FBP (P < 0.001).
The mean CT attenuation values of the aorta, LV lumen, and coronary arteries were significantly higher in group A (80 kVp) than in group B (100 kVp) (P < 0.001). The CNR and SNR of group A reconstructed with IMR were also significantly higher than those of group B reconstructed with HIR (P < 0.001). Intergroup comparisons of the images equally reconstructed with HIR showed that the CNR and SNR were significantly lower for group A than for group B (P < 0.001).
Subjective analysis
Subjective image quality analyses.

Bold P value <0.05.
Values are mean ± standard deviation.
IMR, iterative model reconstruction; HIR, hybrid iterative reconstruction; FBP, filtered back projection.
Inter-observer reliability was good for image noise, beam hardening artifact, and overall image quality (κ = 0.688, κ = 0.691, and κ = 0.655, respectively). A fair degree of agreement on vessel sharpness was observed (κ = 0.502).
Discussion
Our data demonstrated that CCTA images acquired using 80 kVp and reconstructed with IMR (group A) had higher CNR, SNR, and mean CT attenuation values and better subjective image quality than did those acquired using 100 kVp and HIR (group B). The effective radiation dose in group A was approximately half of that in group B (0.38 ± 0.09 mSv versus 0.73 ± 0.19 mSv). We achieved not only substantial radiation dose reduction but also enhancement of image quality, via combination of prospective ECG triggering, low tube voltage technique, and IMR.
There have been numerous studies showed that the use of IMR with a low tube voltage (80 kVp) for CCTA could reduce radiation exposure while improving image quality (10,12,13,17). Oda et al. reported that IMR could produce acceptable image quality with only 20% of the radiation dose of conventional CCTA (14). In addition, Hue et al. reported that use of the IMR algorithm and 80 kVp subsequently reduced the radiation dose by 66% in animal model (18). This is consistent with our results figuring out the efficacy of IMR and low tube voltage technique. However, we achieved far more radiation dose reduction by either applying prospective ECG triggering mode or reducing tube current, compared with previous reports. Indeed, the average effective dose of group A in our study was 0.38 mSv, which was much lower than a prior study using 80 kVp and retrospective-gated technique (2.4 ± 1.2 mSv) (10) and another study that identically used 80 kVp and prospective ECG triggering mode, but relatively high tube current (0.89 ± 0.09 mSv) (13). We demonstrated that the diagnostic image quality is preserved in submillisievert CCTA by applying prospective ECG triggering technique, low tube voltage and current, and IMR simultaneously.
Owing to a complicated algorithm based on multiple iterations and models, the reconstruction time for IMR is known to be longer than that for FBP or HIR. The actual reconstruction time for IMR in our study was approximately five or six CT images per second. It was relatively longer than that of HIR and FBP, which could reconstruct up to 22–33 CT images per second. Nevertheless, we believe that the reconstruction speed for IMR was clinically acceptable, because it took less than 2 min to reconstruct every single CCTA with IMR in our study. In addition, there have been several concerns about the artificial texture and blotchy appearances in images reconstructed with MBIR or IMR (16,19). However, our data demonstrated that images reconstructed using IMR were superior to those reconstructed using FBP or HIR on both qualitative and quantitative assessment at the 80-kVp setting (Fig. 2). Moreover, CT images acquired at 80 kVp and reconstructed using IMR showed better qualitative and quantitative image properties with less radiation dose than did images acquired at 100 kVp and reconstructed using HIR.
A 55-year-old man with typical chest pain underwent CCTA (average heart rate = 50.5 bpm; BMI = 24.19 kg/m2). Total dose length product was 23.5 mGy cm. Curved multiplanar reconstruction images of (a) right coronary artery (RCA) and (b) left anterior descending coronary artery (LAD) reconstructed with FBP, HIR, and IMR are demonstrated. Minimal to mild stenoses are observed in the proximal RCA (black arrow) and proximal LAD (open arrow) with mixed plaques. Image noise and streak artifact are substantially lower for images reconstructed with IMR than with FBP and HIR. The SNR, CNR, image noise, and subjective image quality assessment of the proximal RCA were as follows: 76.07, 82.56, 10.95, and all grade 4 on IMR; 19.46, 21.39, 40.81, and all grade 3 on HIR; and 9.36, 11.37, 108.87, and all grade 3 on FBP.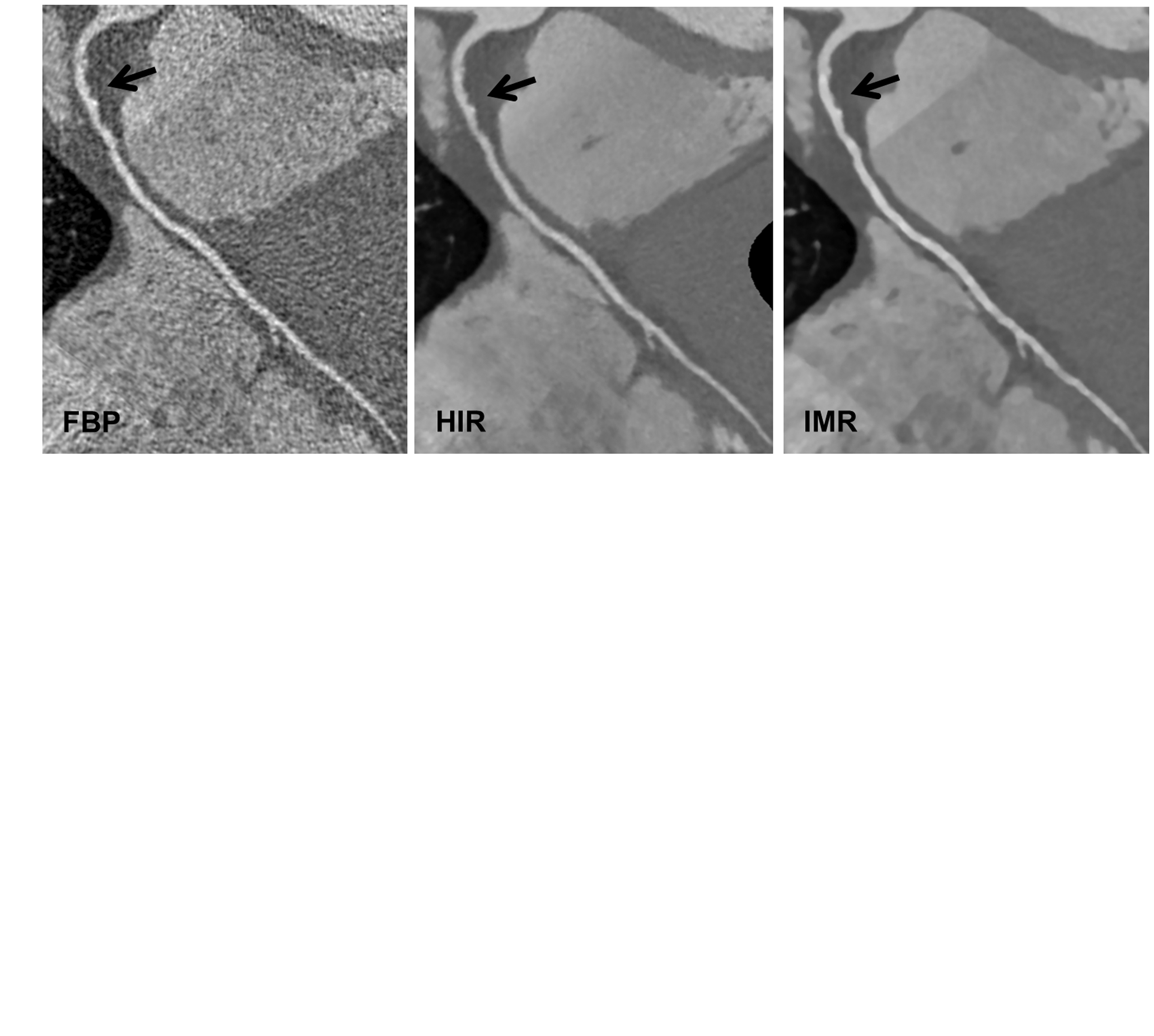
One of the major applications of scanning at a low tube voltage is the reduction of iodinated contrast medium. Previous studies have demonstrated that combined use of IMR with low-tube-voltage technique allowed reduction of dose or concentration of contrast media (10,12,20). The use of iodinated contrast medium for CCTA is also a serious concern since it may contribute to renal impairment. Although we did not deal with reduction of contrast media in the current study, a future study should be performed to evaluate the degree and associations between the amount and concentration of contrast media, radiation exposure and image quality of CCTA. Another major drawback of our study is that we did not evaluate the diagnostic accuracy for detecting coronary stenosis by correlating our data with conventional coronary angiograms. The prevalence of significant coronary artery stenosis was too low (two of total 90 patients) and we lacked reference standard for the majority of lesions. Further studies are necessary to determine the diagnostic performance of coronary stenosis with IMR.
Our study has several other limitations. First, the number of patients was relatively small. Second, our study population was composed of non-obese patients (BMI < 30 kg/m2) with relatively low heart rate (≤65 bpm). Further prospective clinical trials including different patients with diverse characteristics are necessary to validate the efficacy of IMR. Third, we used a single parameter setting in reconstruction using HIR (level 4) and IMR (L2). Fourth, the inter-observer reliability in the subjective analysis was not particularly high, especially for evaluations of vessel sharpness. Fifth, images of group B was reconstructed with only HIR algorithm, which was limited inherently by its retrospective design.
In conclusion, we demonstrated that IMR provides significantly improved image quality with submillisievert radiation exposure in CCTA by using a lower tube voltage (80 kVp) than HIR uses with conventional tube voltage (100 kVp), proposing the feasibility of this method of performing CCTA in clinical practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.