
Abstract
Background
After neoadjuvant chemotherapy (NAC), persistent microcalcifications are often observed in spite of a decrease in the primary tumor size.
Purpose
To analyze the changes in microcalcifications after NAC and to evaluate the accuracy of residual microcalcifications in predicting the extent of residual cancer.
Material and Methods
Eighty patients who received NAC and underwent both mammography and magnetic resonance imaging (MRI) before and after the completion of NAC were included. The location of microcalcifications was classified into two types: inside the mass and outside the mass.
Results
The extent of the residual calcifications was larger than the pathologic residual lesion in 14 (74%) of 19 patients with complete response (CR) on MRI, but the discrepancy was <1 cm in eight (42%) patients. The median value of the discrepancy was significantly higher in patients showing CR with outside calcifications compared to CR with inside calcifications (2.0 cm vs. 0.7 cm, P = 0.008). After NAC, the decrease of calcifications was more frequently observed in cancers showing CR on MRI or Miller-Payne grade 5 and the increase of calcifications more frequently occurred in cancers showing progress disease on MRI or Miller-Payne grade 1 (P < 0.001 and P = 0.044).
Conclusion
The change in microcalcifications after NAC was correlated with the tumor response to NAC. The discrepancy was highest in the group showing CR on MRI with outside calcifications. In tumors with inside calcifications, the discrepancy was relatively low within an acceptable range.
Introduction
Neoadjuvant chemotherapy (NAC) has been used to convert inoperable locally advanced breast cancer to an operable status and to downsize tumors in order to allow breast-conserving surgery to take place (1,2). NAC has been shown to reduce micrometastasis and effectively downstage the axillary lymph node (3–7). In addition, NAC allows direct and early observation of the response to treatment, which could lead to a change in the treatment plan in the event of a poor response (8).
The rate of pathologic complete response (pCR) is in the range of 16–20%. Patients who achieve pCR have better disease-free survival and overall survival compared to patients with residual cancer (9–14). A higher rate of pCR (24–51%) has been reported in human epidermal growth factor receptor 2 (HER2)-positive breast cancer with combination therapy comprising taxane and HER2-targeted drugs (15,16).
There are two types of calcification processes in the breast (17). The secretory type is associated with the accumulation of secretions and is likely to be found in benign lesions as well as low-grade or intermediate-grade ductal carcinoma in situ (DCIS). This type of calcification is punctate, round, and amorphous within a cluster (18). The necrotic type of calcification develops in necrotic cellular debris and is frequently found in high-grade DCIS.
After NAC treatment, the number and extent of microcalcifications could remain stable, decrease, or increase according to the tumor response to NAC (19,20). Several studies have compared the extent of microcalcifications after NAC to the extent of the pathologic lesion and found that the extent of microcalcifications tended to overestimate that of the true lesion (21–23).
In clinical practice, it is difficult to determine whether residual cancer cells are present at microcalcification sites, and current treatment guidelines require the excision of microcalcifications seen on MG because they are believed to represent the total tumor burden.
The first aim of this study was to analyze the pattern of changes in microcalcifications after NAC according to the Response Evaluation Criteria In Solid Tumors (RECIST) and Miller-Payne grading system. The second aim was to evaluate the accuracy of residual microcalcifications in predicting the extent of residual cancer after NAC.
Material and Methods
Patients
Institutional ethics committee approval was obtained for this retrospective study and the need for informed consent was waived.
Between January 2012 and December 2014, a total of 204 patients received NAC before surgery. Among them, 84 patients who underwent mammography before and after NAC and demonstrated suspicious microcalcifications within the tumor bed were included in the image analysis. Of these 84 patients, four were excluded due to the poor image quality of the mammography film that was examined at an outside hospital.
Demographics and tumor characteristics of the study patients.

NAC, neoadjuvant chemotherapy; ER, estrogen receptor; PR, progesterone receptor; HER, human epidermal growth factor receptor; HR, hormone receptor (ER or PR); TN, triple negative; SD, standard deviation.
Mammography and MRI technique
Mammography was performed using a dedicated digital mammography unit (LORAD Selenia; Hologic, Bedford, MA, USA) at the time of initial diagnosis and one day before surgery after the completion of NAC. Standard two-view MG examinations were performed and magnification views were acquired if clinically necessary.
Breast MRI was performed with a 1.5-T system (SignaHDxt; GE Healthcare, Milwaukee, WI, USA) and a dedicated eight-channel breast coil. The standard MRI protocol included an axial Τ2-turbo spin echo sequence (TR = 3616 ms, TE = 98 ms, field of view [FOV] = 300 × 300 mm, slice thickness = 3 mm) and unenhanced and contrast-enhanced axial Vibrant sequences with T1-weighted fat saturation (TR = 5.1 ms, TE = 2.4 ms, flip angle = 10°, matrix = 300 × 300, FOV = 300 mm, slice thickness = 1.5 mm, phase acquisition time = 90 s). Gadobutrol (Gadovist; Bayer Schering Pharma, Berlin, Germany) was injected into an antecubital vein at a dose of 0.1 mmol/kg of body weight and a rate of 3 mL/s, followed by a 20-mL saline flush for all patients. Subsequently, five consecutive contrast-enhanced series were acquired.
Image analysis
Mammography and MR images were retrospectively analyzed by two radiologists with 7 and 11 years of experience in breast imaging in consensus. Both radiologists were blinded to the result of the MRI and pathologic responses when they interpreted the mammography images. On mammography, the shape and distribution of microcalcifications were recorded. The extent of calcifications was measured in centimeters in the greatest dimension on initial mammography and post-NAC mammography. The cases were classified as “decreased,” if either one of extent or number of calcifications had decreased and as “increased,” if either one of extent or number had increased.
On MRI, the residual lesion size after NAC was measured as the longest diameter of the lesion on the maximum intensity projection image and classified into complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD) based on the RECIST 1.1 criteria (24).
For multiple lesions, the longest diameter of each lesion was separately recorded and the sum of the lesions was calculated. Cases in which the residual lesion was measured as <0.2 cm on MRI were termed near-complete responses and were classified as CR by the RECIST criteria.
The location of microcalcifications was classified into two types, inside the mass and outside the mass, based on both initial mammography and MRI findings. If calcifications were located within the mass without an outside component, they were classified as being inside the mass group. If calcifications were located outside the mass or both within and outside the mass, they were classified as being outside the mass group (Fig. 1). The total extent of the microcalcifications was measured on mammography after NAC. The range of discrepancy was calculated as the extent of the microcalcifications on mammography minus the extent of the residual lesion on pathologic examination.
Schematic diagram of the location of calcifications and response to NAC. The assessment of CR and PR was based on MRI. (a) Inside the mass. (b) Outside the mass. CR, complete response; PR, partial response.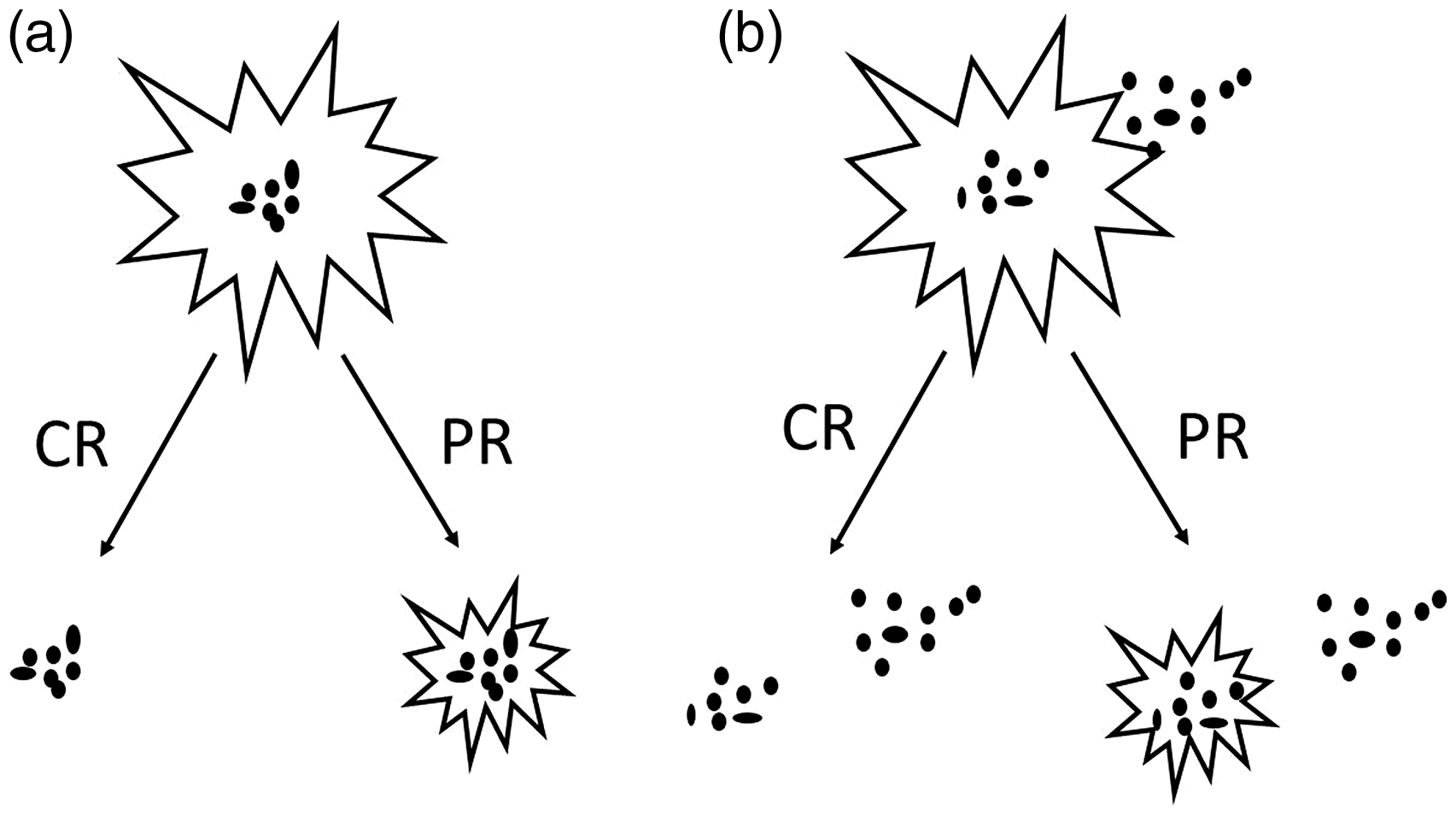
We also acquired the absolute value of the discrepancy in each lesion and compared the median values of the discrepancy according to the tumor response and the location of the microcalcifications.
Histopathologic examination
All patients underwent surgery after the completion of NAC. The routinely formalin-fixed, paraffin-embedded tissue blocks were sectioned at a thickness of 4 µm and stained with hematoxylin and eosin. The microcalcification extent was measured in the longest dimension of the residual cancer including both invasive cancer and DCIS. For lesions with diffusely scattered invasive ductal carcinoma (IDC) foci or DCIS, the extent was measured including the total range of all IDC and DCIS lesions.
The estrogen receptor (ER), progesterone receptor (PR), and HER2 statuses were evaluated in core-biopsied specimens before NAC. ER and PR were considered positive only when ≥ 1% of tumor cells showed nuclear staining. HER2 was positive if tumor cells showed 3+by IHC or 2+by IHC with amplification using fluorescence or silver in situ hybridization. Histopathologic tumor regression was semi-quantitatively graded using the Miller-Payne system, a five-point histological grading system that is based on the reduction of tumor cellularity (25). The Miller-Payne system is as follows: grade 1 = no change or some alteration to individual malignant cells but no reduction in overall cellularity; grade 2 = a minor loss of tumor cells but overall cellularity still high, with up to 30% loss; grade 3 = between an estimated 30–90% reduction in tumor cells; grade 4 = a marked disappearance of tumor cells such that only small clusters or widely dispersed individual cells remain, with > 90% loss of tumor cells; and grade 5 = no malignant cells identifiable in sections from the site of the tumor and only vascular fibroelastotic stroma remaining, often containing macrophages, although DCIS may be present. All specimens were reviewed by a pathologist with 16 years of experience.
Statistical analysis
Fisher's exact test was used for the evaluation of calcification changes after NAC according to the RECIST criteria and the Miller-Payne grading system. The Mann–Whitney U-test was used to examine discrepancies between the extent of microcalcifications on mammography and the extent of the residual lesion on pathologic examination.
Analyses were performed using the SPSS 19.0 statistical software package (SPSS IBM, Armonk, NY, USA), and a P value < 0.05 was considered significant.
Results
Shape and distribution of calcifications on pre-treatment mammography.

Values are presented as n (%).
Change in the shape and extent of calcifications after neoadjuvant chemotherapy (NAC).
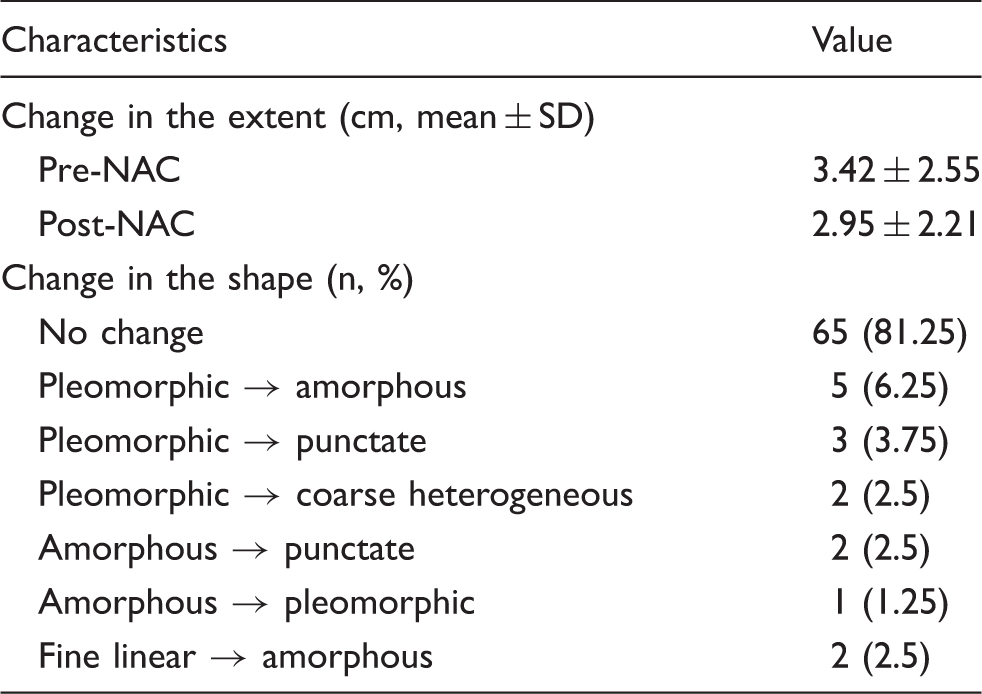
Decrease of microcalcifications was noted in 25 patients, increase in 11 and no interval change in 44 patients. One patient showed the complete disappearance of microcalcifications after NAC. Of 25 patients showing decreased calcifications, pathologic complete remission was found in three patients and the mean extent of calcifications decreased from 3.71 cm to 2.44 cm.
Change in calcifications after NAC according to the RECIST criteria and Miller-Payne grade.
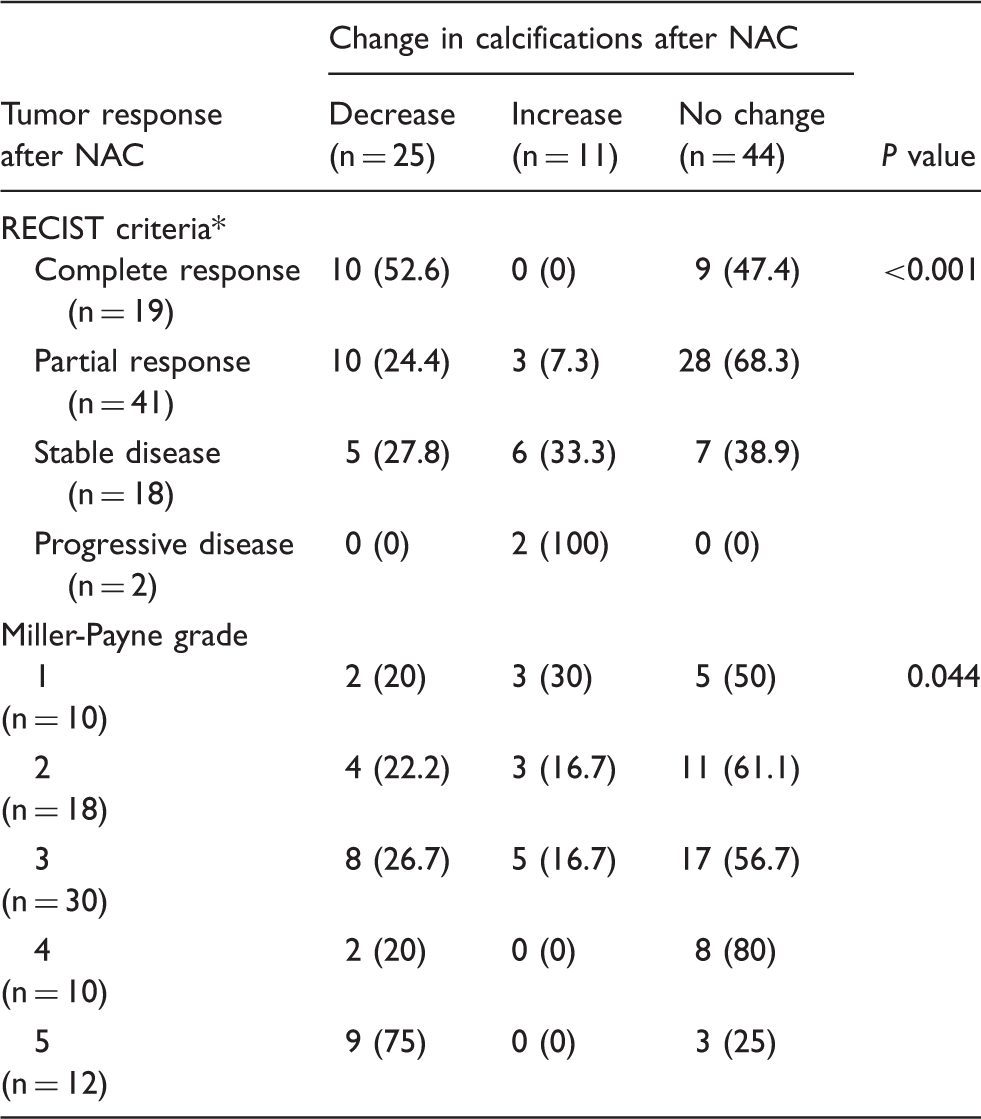
Values are presented as n (%).
Based on magnetic resonance imaging.
NAC, neoadjuvant chemotherapy.
Comparison of residual lesion size on histopathology, mammography, and MRI after NAC.
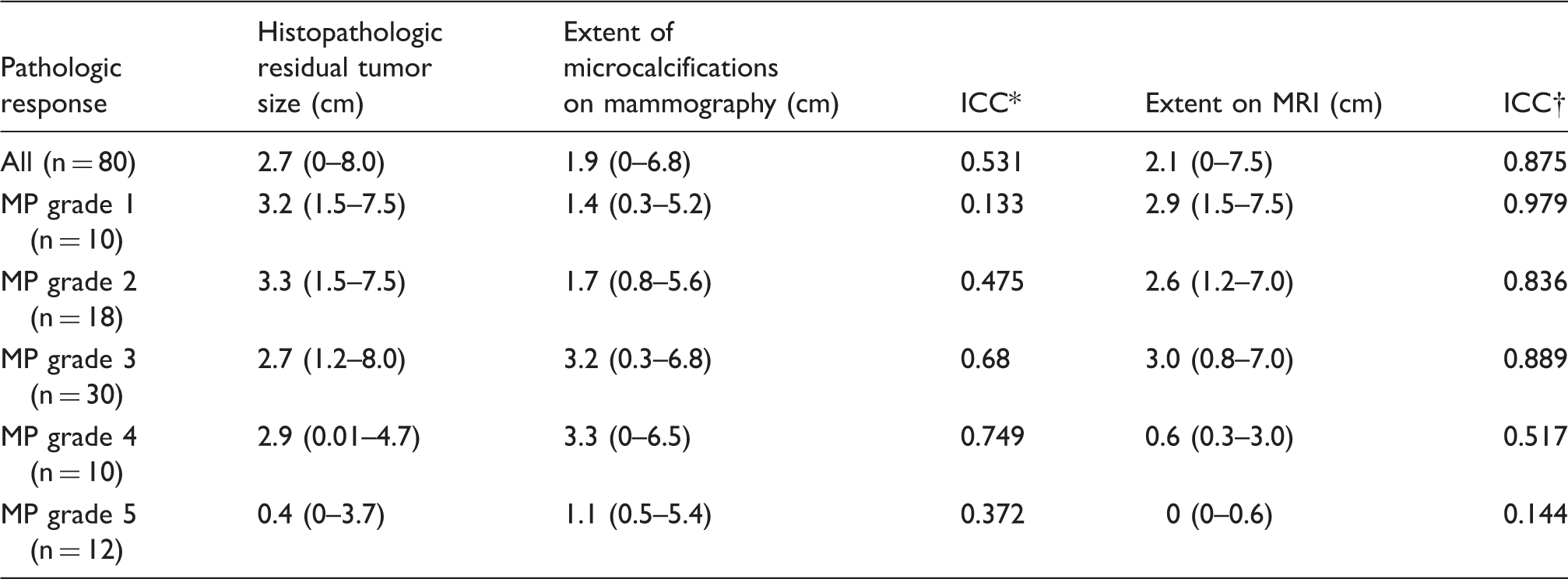
Values are presented as median (range).
ICC between the extent of microcalcifications on mammography and histopathology.
ICC between the extent of enhancing lesion on MRI and histopathology.
MP, Miller-Payne; ICC, intraclass correlation coefficient.
Discrepancy in lesion extent according to the RECIST criteria and the location of calcifications in patients showing CR and PR on MRI.
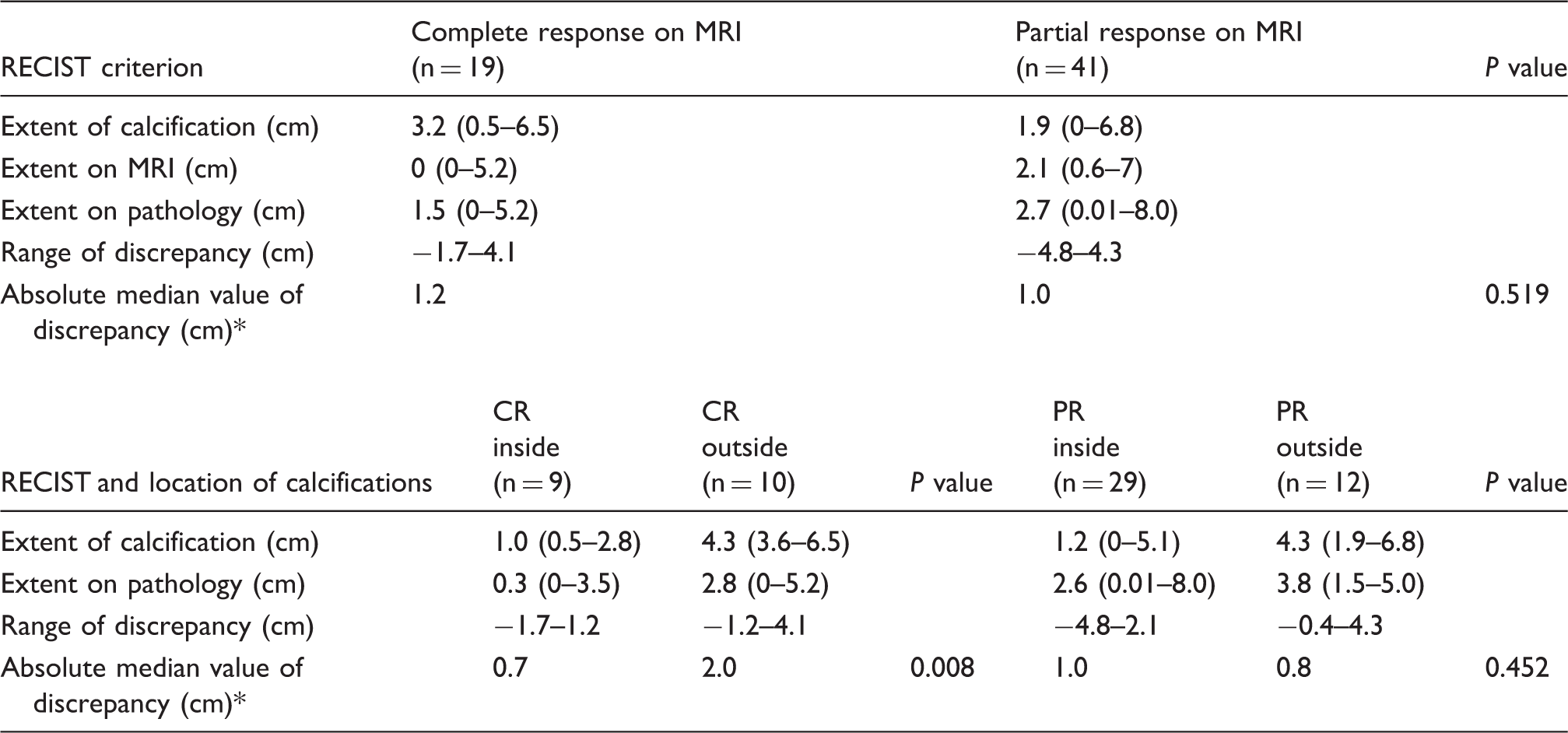
Values are presented as median (range).
Discrepancy between extent of calcification on MG and pathologic extent.
CR, complete response; PR, partial response; MRI, magnetic resonance imaging.
Of 29 patients with PR with inside calcifications, the extent of the calcifications overestimated the true lesion in 11 (38%) patients and underestimated it in 18 (62%). The discrepancy was <1.0 cm in 14 (48%) patients. Of 12 patients showing PR with outside calcifications, the calcifications overestimated the true lesion in 11 (92%) patients and underestimated it in one (8%). The discrepancy was <1.0 cm in four (33%) patients. The median value of the absolute discrepancy was 1.0 cm for PR with inside calcification and 0.8 cm for PR with outside calcification, with no significant difference (P = 0.452).
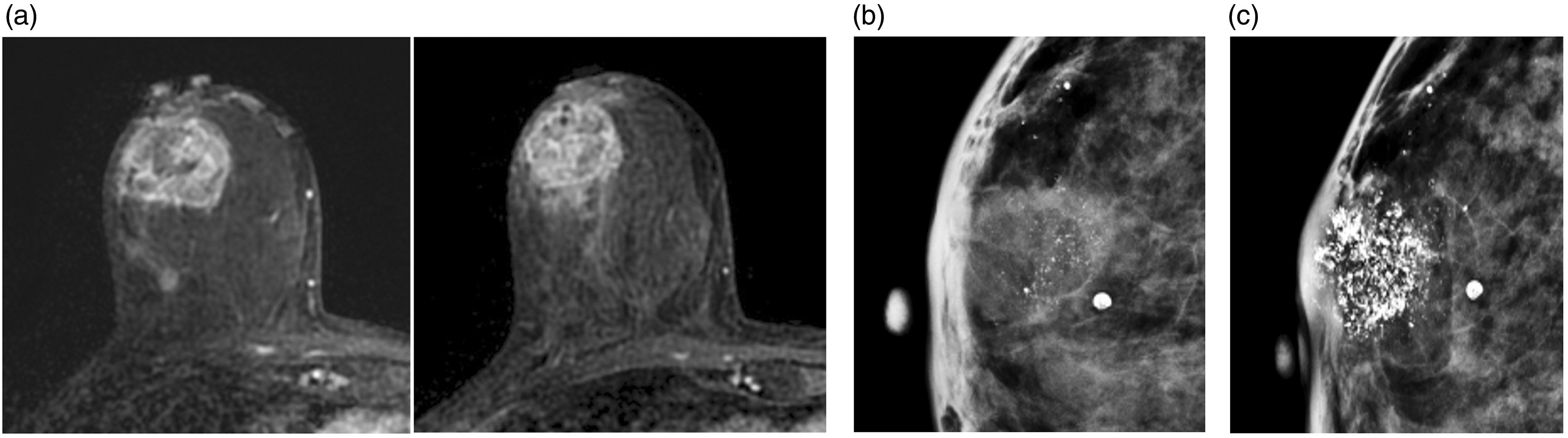
Representative cases are shown in Figs. 2–4.
A 43-year-old woman with known IDC in the right breast. (a) Axial subtraction image shows multifocal enhanced masses with an irregular shape and margin in the right lower inner breast (left). After completion of NAC, axial subtraction image shows 0.3-cm enhanced foci in the tumor bed (arrow in right); this case was classified as a near complete response based on MRI. (b) Initial mammography shows segmentally distributed fine pleomorphic calcifications in the right lower breast. (c) After completion of NAC, the extent and number of calcifications were stable and the extent of the calcifications was measured as 4.3 cm. On pathologic specimens, there were few DCIS foci and the extent was 0.3 cm. A 42-year-old woman with known IDC in the left breast. (a) Axial subtraction image shows an enhanced mass with an irregular shape and margin in the left outer central breast (left). After completion of NAC, the axial subtraction image shows no residual enhanced lesion; this case was classified as a complete response based on MRI (right). (b) Initial mammography shows regionally distributed fine pleomorphic calcifications in the left outer breast. (c) After the completion of NAC, the extent and number of calcifications were stable and the extent of the calcifications was measured as 4.2 cm. On pathologic specimens, there were multiple scattered IDCs and the extent was 3.2 cm. A 52-year-old woman with known IDC in the right breast. (a) Contrast-enhanced axial image shows an oval-shaped mass with heterogeneous enhancement in the right outer central breast (left). After the completion of NAC, the contrast-enhanced axial image shows no interval change in size measuring 2.8 cm. This case was classified as stable disease based on MRI (right). (b) Initial mammography shows grouped fine pleomorphic calcifications within the mass. (c) After the completion of NAC, the number of calcifications was markedly increased. The extent of the calcifications was 2.8 cm, equal to the pathologic extent of the residual lesion.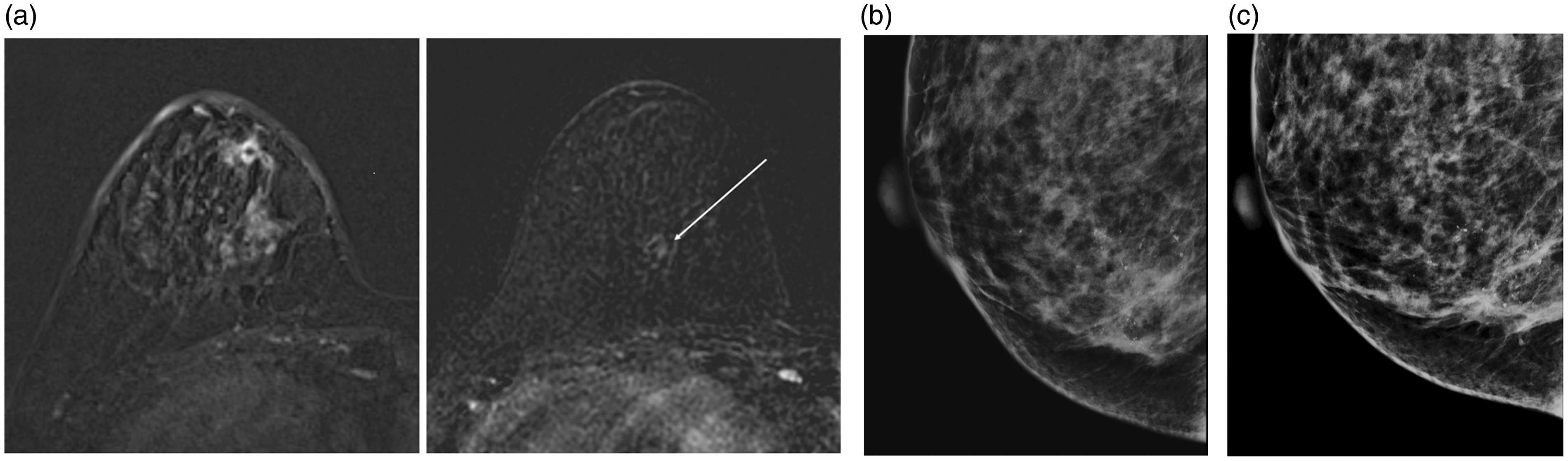

Discussion
Our results revealed that decrease of calcifications was more frequently observed in cancers showing complete response on MRI or Miller-Payne grade 5. In contrast, increase of calcifications more frequently occurred in cancers showing progress disease on MRI or Miller-Payne grade 1. The extent of the residual calcifications was larger than the pathologic residual lesion in 14 (74%) out of 19 patients with CR on MRI, but the discrepancy was < 1 cm in eight (42%) patients. The discrepancy was significantly higher in lesions with CR on MRI and outside calcifications compared to lesions with CR and inside calcifications (2.0 cm vs. 0.7 cm, P = 0.008).
In a previous study that analyzed the change in microcalcifications after NAC (20), the number of microcalcifications within a 1-cm2 area decreased in 15% of patients, increased in 7.5%, and was stable in 77.5%. The change in microcalcifications was not related to the tumor response rate in this study. In contrast, the results of the current study showed that the change in microcalcifications was significantly correlated with the RECIST criteria on MRI (P < 0.001) and the pathologic response based on the Miller-Payne grade (P = 0.044). An increase in microcalcifications was more frequently observed in patients with poor response to NAC and decreased in microcalcifications was in patients with better response.
MRI is known to be the most reliable imaging technique for the evaluation of residual cancer after NAC (26–29). Weiss et al. found that MRI was more likely to be correlated with pathologic tumor size than mammography in the calcification-positive group and that mammography overestimated the size of the tumor (21). In the study by Kim et al. (22), the extent of microcalcifications on mammography after NAC showed a lower correlation with the extent of pathologic residual cancer than MRI. They also revealed that the agreement was highest in tumors positive for hormone receptor and HER2. Adrada et al. studied 32 patients with pCR and found that calcifications were associated with DCIS in nine patients and benign lesions in 21 patients, suggesting that the extent of calcifications after NAC is not correlated with the extent of the residual cancer (23).
In clinical practice, the extent of microcalcifications in the SD and PD groups does not receive the attention of radiologists or surgeons because all suspicious calcifications should be excised in these groups. However, in the CR and PR groups, especially where the extent of the calcifications on MG exceeds the extent of enhanced lesions on MRI, it is very difficult to determine the exact extent of the residual lesions. Our study revealed that the discrepancy was relatively low and acceptable in most cases, except in the case of CR with outside calcification. About 78% of cancers with CR with inside calcification, 48% of PR cancers with inside calcification, and 33% of PR cancers with outside calcification showed a minimal discrepancy of <1 cm. In patients showing PR with inside calcification, in particular, the extent of calcification underestimated the true residual lesion in 62%. Therefore, except cancers showing CR and outside calcifications, all calcifications on mammography should be excised regardless of other imaging findings.
The definition of pCR is not standardized and there is controversial issue regarding the inclusion of residual DCIS. Several studies reported that the prognosis of patients with residual DCIS showed no difference in survival compared to patients with no tumor cells, while others reported that patients with residual DCIS had a worse event-free survival than patients with no tumor cells (30–32). We used the Miller-Payne grading system in which pCR was defined as no invasive tumor cells in the breast. For the evaluation of tumor response, RECIST criteria was applied on MRI. NAC can result in a good response of the invasive component with minimal change in the DCIS component due to the lack of angiogenesis. Furthermore, the RECIST criteria have been designed to assess the solid tumor response and their use in the evaluation of DCIS has some limitations. However, most studies have used the RECIST criteria for the evaluation of the breast cancer response after NAC because MRI shows the highest sensitivity not only for invasive cancer but also DCIS.
Our study has several limitations. First, this was a retrospective study from a single center and the number of patients was relatively small. Therefore, a larger study is needed to validate our results. Second, our patients received different chemotherapy regimens and different cycles before surgery. However, we evaluated the correlations between the final tumor response and calcification change without respect to the chemotherapy regimen and duration.
In conclusion, the change in microcalcifications after NAC was correlated with the tumor response to NAC. The discrepancy between the extent of microcalcifications on mammography and the pathologic extent was highest in the group showing CR on MRI with outside calcifications. In tumors with inside calcifications, mammography provided little additional information compared to MRI and the discrepancy was relatively low within an acceptable range.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.