
Abstract
Background
The optimal optic nerve sheath diameter (ONSD) cut-off for identifying increased intracranial pressure (IICP) remains unclear in adult patients.
Purpose
To validate the diagnostic accuracy of ultrasonographic (US) ONSD > 5.0 mm as a cut-off for detecting IICP by computed tomographic (CT) through a meta-analysis.
Material and Methods
A systemic literature review was performed of online databases from January 1990 to September 2017. A bivariate random-effects model was used to estimate pooled sensitivity, specificity, and diagnostic odds ratio (DOR) with 95% confidence intervals (CIs). A summary receiver operating characteristic (SROC) graph was used to provide summary points for sensitivity and specificity. Meta-regression tests were performed to estimate the influence of the study characteristics on DOR. Publication bias was assessed using Deeks' funnel plot asymmetry test.
Results
Six studies with 352 patients were included in the meta-analysis. US ONSD > 5.0 mm revealed pooled sensitivity of 99% (95% CI = 96–100) and specificity of 73% (95% CI = 65–80) for IICP detection. DOR was 178. The area under the SROC curve was 0.981, indicating a good level of accuracy. Meta-regression studies showed no significant associations between DOR and study characteristics such as probe mode (relative DOR [RDOR] = 0.60; P = 0.78), study quality (RDOR = 0.52; P = 0.67), IICP prevalence (RDOR = 0.04; P = 0.17), or pathology at admission (RDOR = 1.30; P = 0.87).
Conclusion
US ONSD > 5.0 mm can be used to rapidly detect IICP in adults in emergency departments and intensive care units. Further meta-analysis based on individual patient-level databases is needed to confirm these results.
Introduction
Early diagnosis and treatment of increased intracranial pressure (IICP) is important for good clinical outcomes in critically ill patients, particularly in emergency departments (EDs) and intensive care units (ICUs). ICP catheters can provide real-time monitoring of pressure status. However, limited technical availability and procedure-related complications are obstacles for their wide use in clinical circumstances (1). The feasibility of using optic nerve sheath diameter (ONSD) by ultrasonography (US) for identifying IICP has been increasingly reported (2,3). The optic nerve is sheathed in meningeal layers, allowing cerebrospinal fluid (CSF) to communicate between the intracranial and subarachnoid spaces within the optic nerve sheath (4,5). US ONSD can be performed at the bedside in 5 min without causing procedural complications or radiation exposure (1). In addition, low intra-observer (k = 0.91) and inter-observer (k = 0.88) variations have been noted within differences of 0.2–0.3 mm in diameter (1,6,7). The utility of US ONSD can be enhanced when diagnostic accuracy is confirmed using specific cut-offs on radiologic reference tests. In daily practice, IICP is widely diagnosed using computed tomography (CT) due to its lower scanning time and better cost-effectiveness in emergent situations compared with magnetic resonance imaging (MRI). One meta-analysis showed that US ONSD had sensitivity of 95.6% and specificity of 92.3% for IICP detection using CT as the reference (8). However, 25% of included studies (3/12) were performed with pediatric patients and without specific cut-offs for IICP detection. In contrast with adults, pediatric populations have shown positive correlations between mean ONSD and age (r = 0.414) (9,10); accordingly, age difference should be considered when determining the diagnostic accuracy of US ONSD. In the present study, we chose 5.0 mm as the cut-off for IICP detected on US. Although a wide range of optimal OSND cut-offs have been reported, > 5.0 mm has been validated most frequently for detecting IICP (11). Therefore, the objective of this study was to summarize current evidence for the diagnostic accuracy of US ONSD > 5.0 mm for detecting IICP on CT through a meta-analysis of studies with adult patients.
Material and Methods
Literature search and selection criteria
We searched the electronic databases PubMed, EMBASE, and the Cochrane central database from January 1990 to September 2017 using MeSH terms or keywords as follows (5,8,12): (“optic nerve” [MeSH Terms] OR “papilledema” [MeSH Terms] OR “ONSD” [All fields] OR “ultrasonography” [MeSH Terms] OR “ultrasonography” [All Fields] OR “ultrasound” [All Fields]) AND (“intracranial pressure” [MeSH Terms] OR “intracranial hypertension” [MeSH Terms] OR “brain injuries, traumatic” [MeSH Terms] OR “intracranial hemorrhages” [MeSH Terms] OR “brain edema” [MeSH Terms] OR “cerebral hypertension” [All Fields]). Our inclusion criteria were as follows: (i) studies on adult patients (aged > 18 years) who underwent ONSD measurement on both US and CT; (ii) studies on patients who were suspected of having IICP; (iii) studies with ONSD procedures performed in > 10 cases; (iv) studies in which ONSD > 5.0 mm was used for detecting IICP on CT; (v) studies in which ONSD was measured 3 mm behind the optic globe; and (vi) randomized controlled, prospective, or retrospective case-controlled studies. Exclusion criteria were as follows: (i) studies on pediatric patients or patients who were aged < 18 years; (ii) studies that included significant ocular trauma; (iii) studies that merely compared ONSD according to the presence of IICP; (iv) studies in which authors used an ICP monitoring probe (intraparenchymal and intraventricular ICP catheter) or opening pressure of lumbar puncture (LP) as a reference standard; (v) studies for which there were no extractable data to construct a 2 × 2 table; (vi) studies in which ONSD was measured in patients with idiopathic intracranial hypertension; (vii) review articles or case reports; and (viii) studies that were not written in English (Fig. 1).
Flow diagram showing the identification of relevant studies.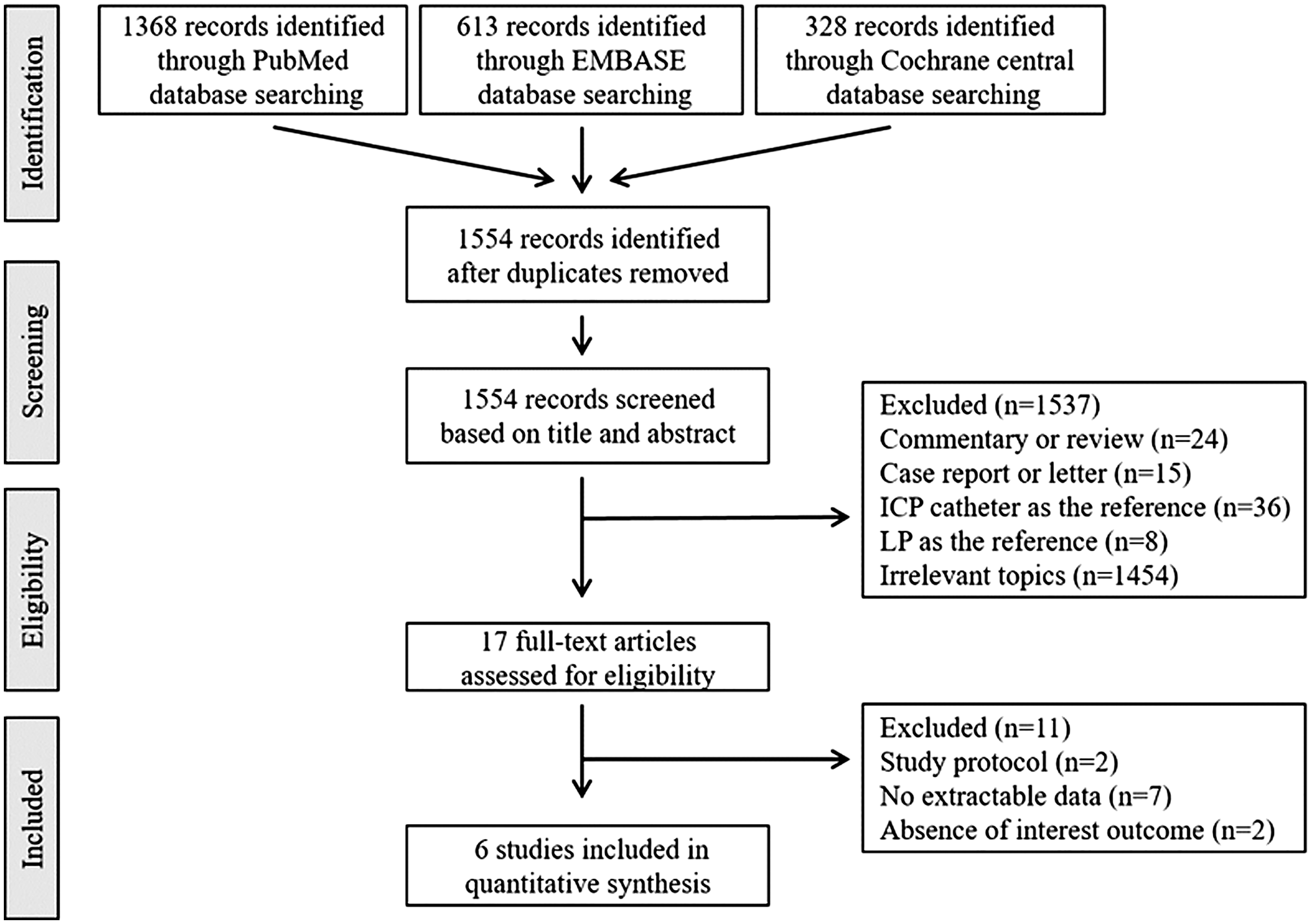
Primary outcomes were sensitivity, specificity, and diagnostic odds ratio (DOR) of ONSD > 5.0 mm for IICP detection in adult patients. We defined IICP as evidence of midline shift, collapsed third ventricle, hydrocephalus, and abnormally compressed cistern on initial CT findings (1,3). We divided IICP prevalence into two groups: low ( < 50%) or high ( ≥ 50%). We categorized US probe frequencies as 7.5 MHz or others (8).
Assessment of methodological quality
We assessed the quality of the included studies using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool, and we evaluated the risk of bias using Review Manager 5 software (8). The QUADAS criteria were as follows: (i) representative spectrum; (ii) acceptable reference standard; (iii) acceptable delay between two radiologic tests; (iv) avoidance of partial verification; (v) avoidance of differential verification; (vi) avoidance of incorporation; (vii) blindness for reference standard results; (viii) blindness for index test results; (ix) presence of relevant clinical information; (x) report of uninterpretable results; and (xi) explanation of withdrawals (Fig. 2) (8). Two authors (JPJ and SK) independently evaluated the eligibility of these studies and extracted data using a uniform standardized form. Disagreements between these two authors were resolved by discussion and consultation with a third author. This study was approved by the Institutional Review Boards of our institution. This meta-analysis was performed according to PRISMA guidelines.
Summary of quality assessment of diagnostic accuracy studies and risk of bias in the meta-analysis.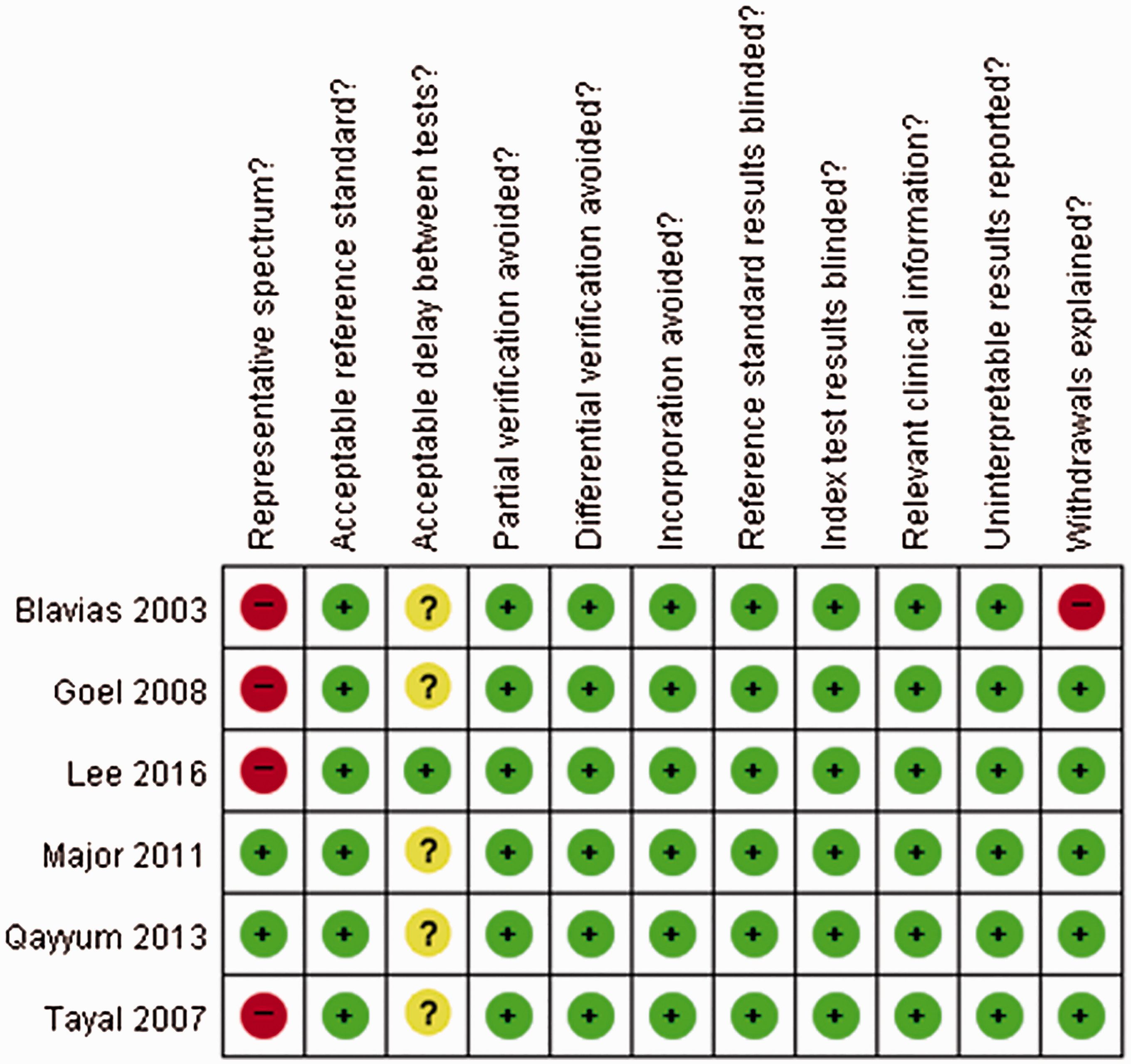
Statistical analysis
For each study, we constructed a 2 × 2 table of true positives (TP), false positives (FP), true negatives (TN), and false negatives (FN). We used a bivariate random-effects model to calculate pooled sensitivity, specificity, positive likelihood ratio (+LR), negative likelihood ratio (−LR), and pooled DOR with 95% confidence intervals (CIs). We performed a threshold analysis to ensure non-heterogeneity of threshold effects (13) and built a forest plot to visually assess heterogeneity. Individual and summary sensitivity and specificity are presented using a summary receiver operating characteristic (SROC) graph. Results are shown as area under the curve (AUC) of SROC (14,15). We evaluated heterogeneity using Cochran's Q test and I2 test (8), and we defined substantial heterogeneity as P < 0.05 and I2 > 50% for the Cochran's Q and I2 tests, respectively. We also conducted meta-regression using restricted maximum-likelihood estimation to estimate the influence of study characteristics on DOR (16). The meta-regression results are presented as relative diagnostic odds ratio (RDOR) with 95% CI. We assessed publication bias with Deeks' funnel plot asymmetry test (17). We performed analyses using Meta-Disc version 1.4 (http://www.hrc.es./investigation/metadis.html) and Stata version 14.0 (Stata Corp LLP, College Station, TX, USA).
Results
Study selection and characteristics
Clinical data of studies included in this meta-analysis.

ED, emergency department; FN, false negative; FP, false positive; ICU, intensive care unit; IICP, increased intracranial pressure; QUADAS, quality assessment of diagnostic accuracy studies; TBI, traumatic brain injury; TN, true negative; TP, true positive; n.c, no comments.
Main analysis
ONSD > 5.0 mm illustrated pooled sensitivity of 99% (95% CI = 96–100) and specificity of 73% (95% CI = 65–80) for detecting IICP demonstrated by CT (Fig. 3a and b). DOR was 178 with a pooled + LR of 4.61 (95% CI = 1.95–10.88) and a pooled –LR of 0.05 (95% CI = 0.02–0.14). All studies had a DOR > 1 without any CIs of 1; accordingly, the positive associations between ONSD cut-off of 5.0 mm and IICP detection were not accounted for by chance alone. Threshold analysis showed a Spearman's correlation coefficient of 0.60 (P = 0.208). Sensitivity results demonstrated homogeneity, but we noted heterogeneity in specificity, which presented non-overlapping CIs.
Forest plot of sensitivity (a) and specificity (b) of optic nerve sheath diameter (cut-off > 5.0 mm) for identifying increased intracranial pressure seen on CT in adults. A pooled sensitivity of 99% (95% CI = 96–100) and specificity of 73% (65–80) were noted. (c) The area under the curve of a SROC graph was 0.981, indicating good accuracy.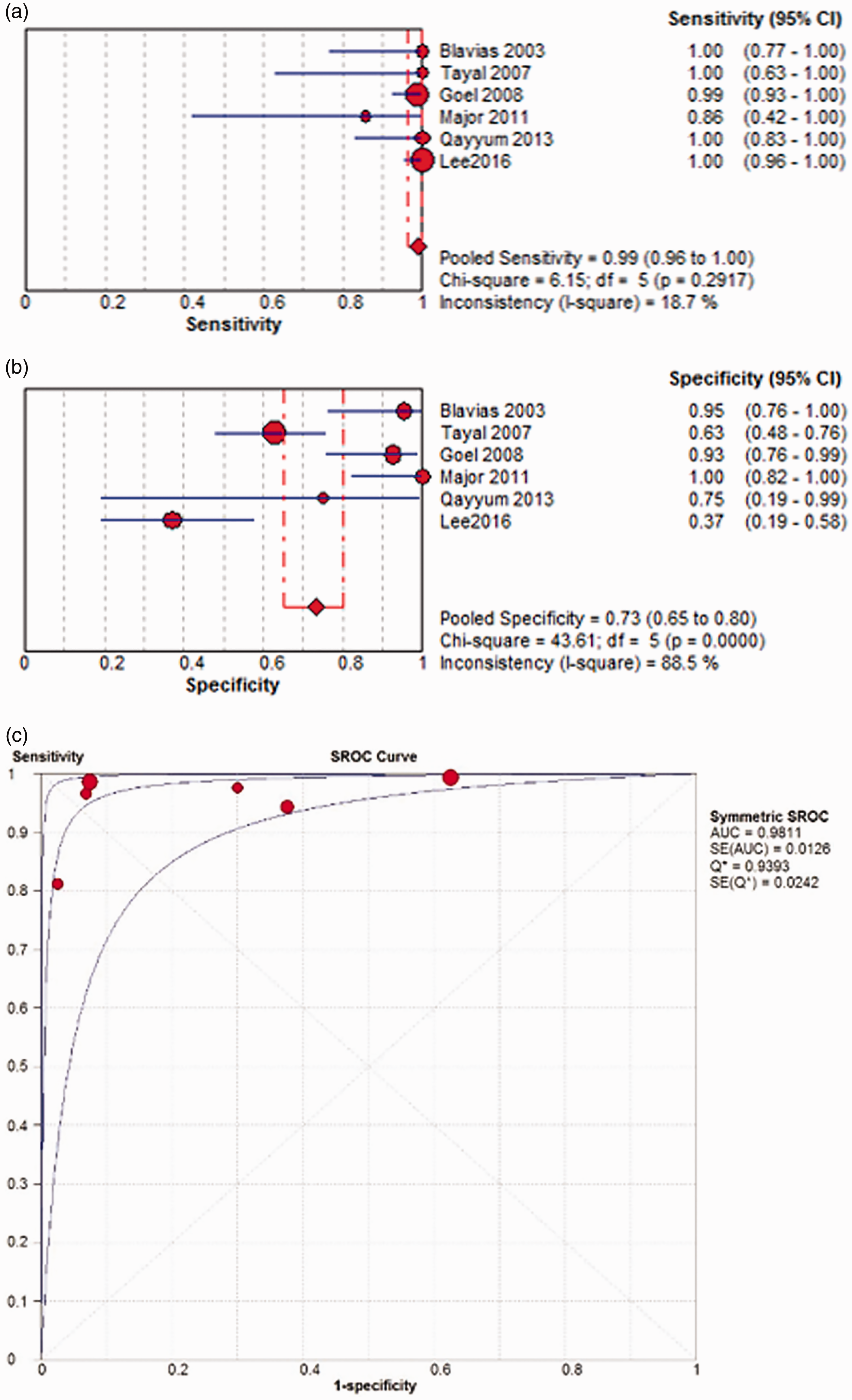
Meta-regression for estimated influence of study characteristics on diagnostic odds ratio (DOR).
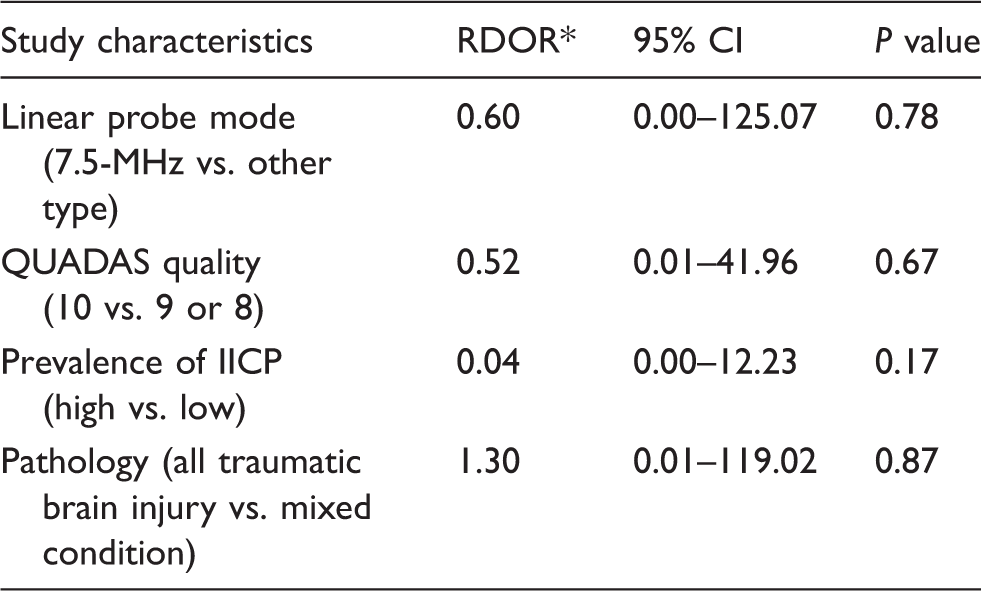
RDOR is < 1 when studies with study characteristics produce a lower DOR.
RDOR, relative diagnostic odds ratio.

Deeks' funnel plot asymmetry test for detecting publication bias in this study; P for the slope coefficient of the regression line is 0.81, indicating no evidence of publication bias (a). Likelihood ratio scatter gram shows functions of mean sensitivity and specificity in the left upper quadrant, suggesting that ultrasonographic optic nerve sheath diameter > 5.0 mm can be useful for confirming increased intracranial pressure when test result is positive or excluding it when result is negative (b).
Discussion
Our study revealed that US ONSD > 5.0 mm had sensitivity of 99%, specificity of 73%, and DOR of 178 for IICP detection demonstrated by CT, suggesting that it is feasible to use ONSD > 5.0 mm for identifying IICP in adult patients.
ONSD defines the dural sheath diameter surrounding the optic nerve and the CSF. The CSF within the optic nerve sheath communicates with the intracranial subarachnoid space, and a linear correlation between subarachnoid pressure within the optic nerve sheath and ICP has been observed (18). The optimal ONSD cut-off for detecting IICP remains undetermined; with ICP monitoring > 20 mmHg as a reference, various optimal cut-offs points have been suggested. Geeraerts et al. (19) reported that ONSD of 5.86 mm had a sensitivity of 95% and a specificity of 79% for IICP diagnosis, and in cases of ONSD < 5.8 mm, the negative predictive value was 100%. Soldatos et al. (20) showed that ONSD of 5.7 mm in ONSD was optimal for IICP detection by intra-parenchymal catheter, with a sensitivity of 74.1% and a specificity of 100%. With ONSD > 5.0 mm as a reference value for detecting IICP, a sensitivity of 88% and a specificity of 93% were noted (21). Although ICP catheter is the gold standard for pressure assessment, procedure-related complications (hemorrhage and infection) and contraindications (coagulopathy and thrombocytopenia) are major concerns (22); in addition, the procedure is not widely available because it is only performed by neurosurgeons. Therefore, comparison between US ONSD and other non-invasive tests such as CT or MRI is more practical in daily practice. Considering test time and cost-effectiveness in emergency situations, CT might be more appropriate for comparative studies to determine the diagnostic accuracy of US ONSD.
Kazdal et al. (23) reported that the midline shift seen on CT correlated well with ONSD (Spearman's rank correlation coefficient = 0.761; P < 0.0005). However, four patients did not have papilledema despite a significant midline shift of over 5 mm. Aside from midline shift, various conditions such as compressed cistern, collapsed ventricle, and acute hydrocephalus also indicate IICP (1). Ohle et al. (8) reported a pooled sensitivity of 95.6%, specificity of 92.3%, + LR of 12.5, and –LR of 0.05 in US ONSD for IICP detection with CT as the reference. Their results suggested that US ONSD has a high sensitivity for excluding IICP in low-risk groups and a high specificity for diagnosing it in high-risk groups (8). Nevertheless, there are concerns about their interpretation; first, they included studies for meta-analysis regardless of patients' age, and Shofty et al. (9) reported a positive correlation between age and mean ONSD in the control population aged < 18 years. Mean ONSD in different age groups was as follows: 3.1 mm in 0–3 years; 3.41 mm in 3–6 years; 3.55 mm in 6–12 years; and 3.56 mm in 12–18 years, but ONSD in adults did not correlate with age or gender (10). Characteristics of CT findings are also different between pediatric and adult patients, particularly in traumatic brain injury (TBI). Sarkar et al. (24) reported that adult TBI patients have significantly more subdural hematoma, subarachnoid hemorrhage, and compressed basal cisterns than pediatric patients. Thus, age should be considered when analyzing the feasibility of US ONSD for IICP detection with CT as the reference. Second, the US ONSD cut-off for detecting IICP was unclear. In daily practice, the utility of US ONSD remains questionable because most studies have provided merely ONSD differences according to IICP presence. Unrecognized IICP delays prompt management, which can result in cerebral swelling and herniation (25). Accordingly, physicians favor high sensitivity to high specificity because of the risk of excluding the diagnosis with negative test results in clinical circumstances (26). Our meta-analysis showed pooled sensitivity of 99% without significant heterogeneity; in addition, +LR was 4.61, indicating that IICP probability could increase when test results are positive. Our results thus suggest US ONSD > 5.0 mm as a useful screening or serial monitoring cut-off for detecting IICP in ED and ICU settings. Nevertheless, we did observe pooled sensitivity of 73% with significant heterogeneity, although the time delay between US and CT and different clinical characteristics might have been the cause of this heterogeneity. In most studies, US and CT were performed simultaneously, although Lee et al. (1) included patients who underwent US and CT within 1 h. There is no definite time window for checking US ONSD before or after CT scanning; however, longer time intervals might have contributed to the relatively low sensitivity of 37% (95% CI = 19–58). Regarding inclusion criteria, Goel et al. (27) and Tayal et al. (4) only included adult TBI patients in their studies. The remaining studies (3,28,29) comprised TBI and non-TBI patients suspected of having IICP. Although meta-regression analysis did not find significant differences in DOR according to pathology (TBI vs. TBI and non-TBI), additional analyses based on individual participant data are needed to confirm our results.
Recently, authors have increasingly compared US OSND and opening LP pressure (30). Amini et al. (30) reported that mean ONSD values in the IICP (defined as opening pressure > 20 cmH2O) and non-IICP groups were 6.7 ± 0.6 and 4.6 ± 0.4 mm, respectively, with US ONSD > 5.5 mm showing a sensitivity and specificity of 100% for IICP detection. Caffery et al. (31) investigated the diagnostic value of ONSD ≥ 5 mm for IICP on LP in non-trauma patients and found a sensitivity and specificity of 75% (95% CI = 53–90) and 44% (95% CI = 25–65), respectively. In a Chinese population, OSND of 4.1 mm was suggested as an optimal cut-off for identifying increased opening pressure, with a sensitivity of 95% and a specificity of 92% (22). However, opening LP pressure tends to be higher than actual ICP (32,33). In addition, procedural success depends on patients' spinal characteristics such as stenosis degree, lordosis, and degenerative changes. Therefore, additional studies are merited to determine an optimal US ONSD cut-off for IICP demonstrated by LP.
In this meta-analysis, we did not include ONSD series with invasive ICP monitoring as the reference; we aimed to provide a single ONSD cut-off point for detecting IICP seen on CT in adult patients. For CT, we defined IICP as significant brain edema, midline shift, compression of ventricle or basal cistern, effacement of sulci, insufficient gray/white differentiation, and transfalcine herniation (1,4). However, most study authors incorporated invasive ICP measurement to define an optimal ONSD cut-off and predicted that absolute ICP values are > 20 mmHg (34). Accordingly, direct correlation between ONSD and ICP monitoring is a major interest. In addition, the best cut-offs have varied considerably between studies, in the range of 5.0–6.0 mm (34). According to Ohle et al. (8), heterogeneity of diagnostic ONSD accuracy increased when they included studies with different IICP detection methods such as based solely on CT or combination of CT and clinical symptoms or ICP monitoring probe. Therefore, we only included ONSD series with CT as the reference to reduce bias due to different reference values.
Based on the results of this study, we do not suggest that US ONSD can replace CT or ICP catheter monitoring. US can offer real-time bedside tracking of ICP without procedural complications within 5 min, whereas the average time from ED arrival to ICP probe catheter insertion is more than 1 h (26). In addition, unstable patients who have multiple lines are challenging for serial ICP assessment using CT (1). Under these clinical circumstances, US ONSD may be useful for rapid IICP detection, particularly US ONSD > 5.0 mm, which has a pooled sensitivity of 99%.
Nevertheless, this study has some limitations. First, the relatively small number (n = 352) of patients from six studies could have led to the lack of statistic power. Second, heterogeneity in specificity was noted in one meta-analysis, reflected as non-overlapping CI and variation in specificity (8). Variations in pretest probability and normal ONSD in the populations in each study, and a threshold effect originating from physicians who checked ONSD, could account for the heterogeneity in specificity. In addition, ONSD methods varied among studies in terms of number of measurements and time intervals between CT and US ONSD (8). Although DOR was 178 (Suppl. Fig. 1) and relative DOR according to clinical characteristics such as US probe, QUADAS quality, IICP prevalence rate, and pathology at admission was not significantly different though meta-regression, additional meta-analysis based on individual patient-level databases in larger populations is needed to assess the diagnostic accuracy of ONSD for detecting IICP (35).
In conclusion, in our meta-analysis, US ONSD > 5.0 mm exhibited pooled sensitivity of 99%, specificity of 73%, and DOR of 178, indicating good diagnostic accuracy for detecting IICP demonstrated by CT in adult patients. Therefore, US ONSD > 5.0 mm can be used as an initial IICP assessment to identify patients who require timely treatment in ED and ICU settings.
Supplemental Material
Supplemental material for Ultrasonographic optic nerve sheath diameter to detect increased intracranial pressure in adults: a meta-analysis
Supplemental material for Ultrasonographic optic nerve sheath diameter to detect increased intracranial pressure in adults: a meta-analysis by Sung-Eun Kim, Eun Pyo Hong, Heung Cheol Kim, Si Un Lee and Jin Pyeong Jeon in Acta Radiologica
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by BioGreen 21 (PJ0131392018) of the Rural Development Administration and National Research Foundation of Korea grant funded by the Ministry of Science, Information and Communication Technologies and Future Planning of the Korea Government (no. 2017M3A9E8033223).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.