
Abstract
Background
Chronic thromboembolic pulmonary hypertension (CTEPH), a complication of acute pulmonary embolism, is a potentially curable form of pulmonary hypertension (PH). CTEPH is under-diagnosed for a number of reasons leading to delayed referral or missed diagnosis; however, the frequency of misdiagnosis of CTEPH findings on computed tomography (CT) is currently unknown.
Purpose
To evaluate the extent of misdiagnosis of CTEPH on CT.
Material and Methods
We studied the original CT reports from 35 patients with confirmed CTEPH diagnosis referred to a specialist center for pulmonary endarterectomy during 2011–2016. The patients’ CT reports were assessed according to a standardized form and compared to a consensus reading by two expert radiologists.
Results
The expert reading identified all CTEPH cases. However, in the original reports, the terminology “CTEPH” was only used in two patients. Another seven descriptive reports picked up the combination of PH and vascular signs of CTEPH without making a definitive diagnosis. Taking these nine cases as positive for CTEPH, the overall sensitivity on a diagnostic level was 26%. Pulmonary arterial abnormalities were described in isolation in 63% with no mention of PH or CTEPH. Signs of PH and mosaic attenuation were documented in 53% and 6% of the original reports, respectively, where it could be seen on the CT examination.
Conclusion
The study shows that radiologists frequently miss CTEPH findings, leading to a falsely low sensitivity for CT. There was also a notable discrepancy in how the findings were presented in radiology reports.
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) is defined as a mean pulmonary arterial pressure (mPAP) >25 mmHg at rest combined with signs of pulmonary arterial thrombotic obstruction (1). Even though 25% of CTEPH patients do not have a known history of acute pulmonary embolism (APE) (2), CTEPH is thought to result from non-resolving APE (3). Over the last few decades, CTEPH has gained increasing interest due to advances in therapeutic approaches, including pulmonary hypertension (PH) modifying pharmacological therapies (4) and surgical advances such as the potentially curing procedure pulmonary endarterectomy (PEA) (5,6) and balloon pulmonary angioplasty (7).
It is important to distinguish CTEPH from other groups of PH since it is currently the only form that is potentially curable. It is also important to distinguish CTEPH from isolated vascular findings, corresponding to chronic thromboembolic disease without pulmonary hypertension (CTED) (8,9). However, without any treatment CTEPH carries a poor prognosis, with an estimated five-year survival of 30% in patients with a mPAP > 40 mmHg and 10% in patients with mPAP > 50 mmHg (5). A delayed diagnosis may lead to increased distal vasculopathy and right heart dysfunction due to the elevated PAP (10). It is thought that there often is a delay in diagnosing CTEPH; an international multicenter study by Mayer et al. showed that the median time between onset of symptoms and diagnosis of CTEPH was approximately 14 months (6).
Despite the considerable progress in therapeutic approaches CTEPH remains under- and misdiagnosed for a number of reasons (11). The patients often present with non-specific symptoms such as dyspnea (99%), edema (41%), fatigue (30%), chest pain (17%), and syncope (16%) (6). Other reasons proposed for delays in the CTEPH diagnosis include lack of clinical suspicion, limited knowledge of the condition among the imaging community, non-uniformity in diagnostics despite international guidelines, and delayed referral to specialist centers (12).
With the increasing utilization of computed tomography (CT), a large proportion of patients with suspected CTEPH or breathlessness of unknown cause can be expected to have had a thoracic CT exam. There are a number of mainly small studies indicating a high sensitivity for CTEPH on CT exams (13–16) but there is also a larger study from 2007 on 227 patients that showed a CT sensitivity of merely 51% (17). Thus, the sensitivity for CTEPH on CT examinations remains under debate and the frequency of missed CTEPH findings on CT among radiologists in general has not been evaluated.
The aim of our study was to investigate the current knowledge of CTEPH findings on CT among radiologists by assessing radiology reports from patients with confirmed CTEPH.
Material and Methods
We performed a retrospective case-control review. The local institutional review board approved the study. Informed consent from the patients was not required for this kind of study.
Cases
All patients attending pre-surgical evaluation regarding PEA during 2011–2016 at a PH referral center were included in the study. A total of 48 cases with confirmed CTEPH were included but 13 cases who did not have preoperative CT pulmonary angiogram (CTPA) were excluded. Among the remaining 35 cases, all had undergone ventilation perfusion scintigraphy (VQ scan,) 33 had preoperative catheter angiography, and 34 were accepted for PEA where all had positive findings of CTEPH. For patients with more than one CTPA during the five-year period, the most recent CT from the referring hospital was selected. Altogether, there were 35 patients (15 women, 20 men; mean age = 59 years; age range = 26–76 years). The CT examinations came from 23 different hospitals; hence there were technical differences in the type of CT scanners, acquisition protocols, and contrast media administration.
Control group
The controls were patients with suspected APE that had undergone CTPA. The controls were selected from the radiology department’s patient flow at the teaching hospital and matched according to age (±5 years), sex, and time of the thoracic CT (±2 years).
Image analysis
All CT examinations were anonymized; cases and controls were mixed randomly before image analysis. Two radiologists read the CT exams: R1 who had 15 years of experience in cardiovascular radiology, with a special interest in PH; and R2 who had three years of experience in thoracic radiology. The results were reported on a standardized form according to recognized CTEPH findings: pulmonary arterial findings associated with CTEPH (arterial bands/webs, eccentric wall-adherent thrombus, calcified thrombus, occlusion, reduced size of segmental arteries, tortuous vessels, vascular pouch), generic cardiovascular signs associated with PH (increased diameter of the main pulmonary artery [MPA], increased ratio between MPA and ascending aorta [AA], right-sided cardiac chamber dilatation, right ventricular hypertrophy [RVH], and systemic arterial collaterals), and mosaic attenuation of the lung parenchyma. In cases of disagreement between the reviewers a consensus reading was performed after individual assessment of the CTPAs.
Assessment of original reports
The original imaging reports for each CT examination were retrieved from the picture archiving and communications system (PACS) archive.
Each report was assessed according to a standardized form similar to the one used by our expert readers. The results from the original reports were then compared to the consensus reading.
Details of the radiology departments were also documented and divided into university hospitals, non-specialist centers, private radiological practices, and telemedicine radiological companies. The CT examinations came from 23 different hospitals: eight were from university hospitals and 15 from non-specialist centers. Of these, one center had used an external telemedicine clinic and one examination was performed in a private clinic.
Statistical methods and data management
Overall sensitivity with 95% confidence intervals (CI) for CTEPH on the CT exams was calculated for the consensus reading. Sensitivity of the original reports compared to the consensus reading was calculated for the overall diagnostic radiological assessment in the original reports, which required a combination of PH and pulmonary arterial signs or mosaic attenuation to be considered positive. Sensitivity was also calculated for positive pulmonary arterial findings associated with CTEPH, cardiovascular signs of PH, and mosaic attenuation, respectively, using MedCalc software (18). We also compared the imaging reports from the university hospitals with the non-specialist centers.
Results
The consensus reading by our expert readers identified all CTEPH cases (sensitivity = 100.0%, 95% CI = 90.0–100.0). Out of the 35 original external reports, only two cases explicitly mentioned the terminology “CTEPH.” Another seven gave a descriptive report of generic features of PH combined with pulmonary arterial abnormalities but failed to make a conclusion of CTEPH. Six CTEPH cases were inaccurately described as APE, five were deemed to be normal, two identified isolated PH, and 13 reports described one or more features of pulmonary arterial abnormalities without picking up the PH or making a conclusion of CTEPH. The sensitivity among the original reports to correctly identify CTEPH was 25.7% (95% CI = 12.5–43.3). The sensitivity among university hospitals was 62.5% (95% CI = 24.5–91.5%) and among non-specialist centers merely 14.8% (95% CI = 4.2–33.7). For an overview of the CTEPH patients, including age, past medical history, hospital category, pulmonary arterial signs, cardiovascular PH features, and pulmonary findings, see Tables 1 and 2.
Patients’ age, sex, medical history, and hospital category performing the CTPA.

*Patient with known CTEPH; still, the pulmonary arterial signs were missed.
PH, pulmonary hypertension; APE, acute pulmonary embolism; DVT, deep venous thrombosis; VTE, venous thromboembolism.
The relevant findings described in the original report and the findings described by our radiologists.
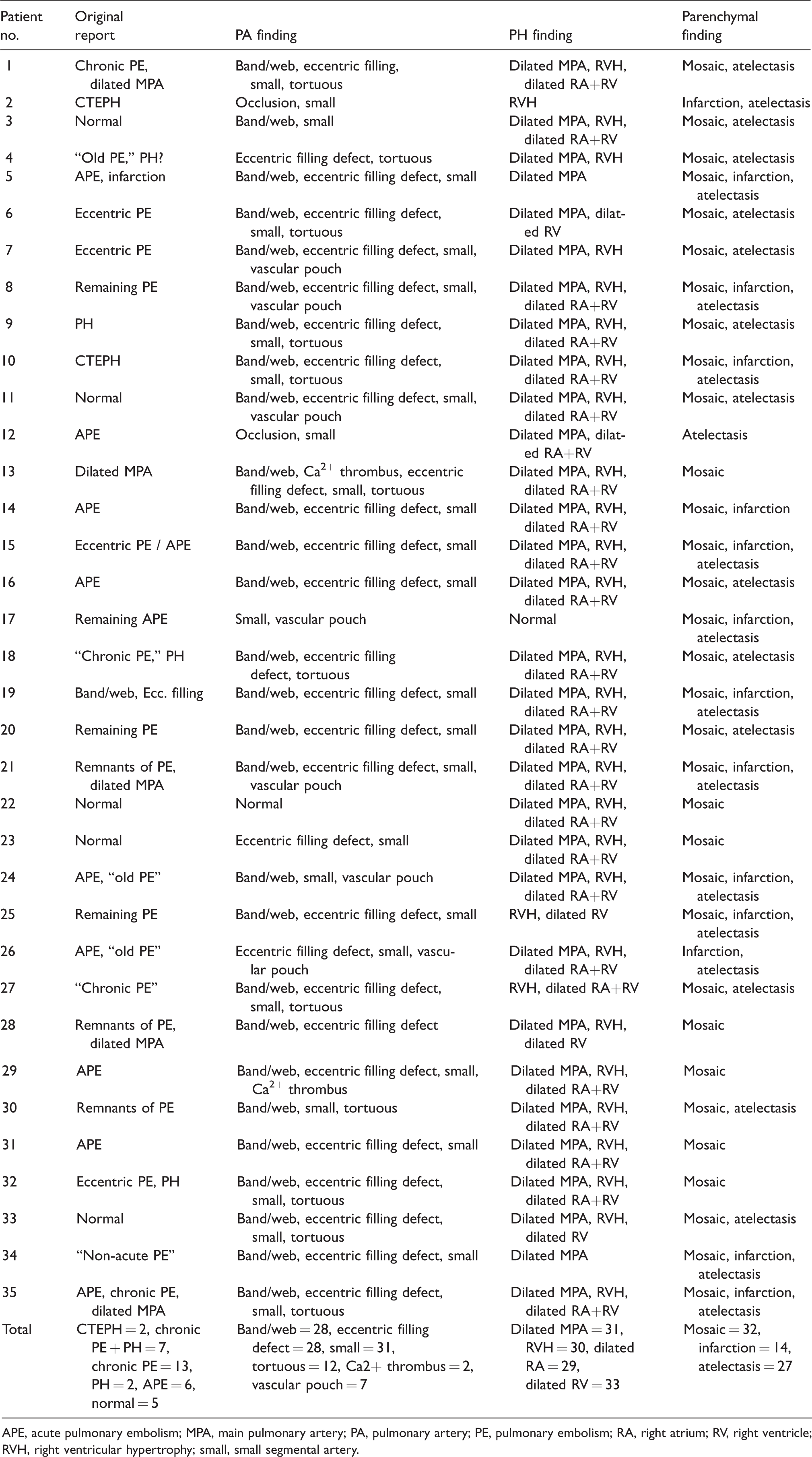
APE, acute pulmonary embolism; MPA, main pulmonary artery; PA, pulmonary artery; PE, pulmonary embolism; RA, right atrium; RV, right ventricle; RVH, right ventricular hypertrophy; small, small segmental artery.
Regarding pulmonary arterial findings, 11 of the original reports correctly identified eccentric filling defects, three reported a reduced size of segmental vessels due to post-thrombotic remnants, and two described webs. Other signs of CTEPH could be seen in most patients but were not reported. Three original reports described remaining or reduced embolus load compared to previous CT exam performed 1–8 months before the current exam. There were 13 original reports falsely described as normal or APE. The sensitivity in the original reports to mention vascular findings associated with chronic thromboembolic disease was 62.9% (95% CI = 44.9–78.5). An example of missed pulmonary vascular findings can be seen in Fig. 1.
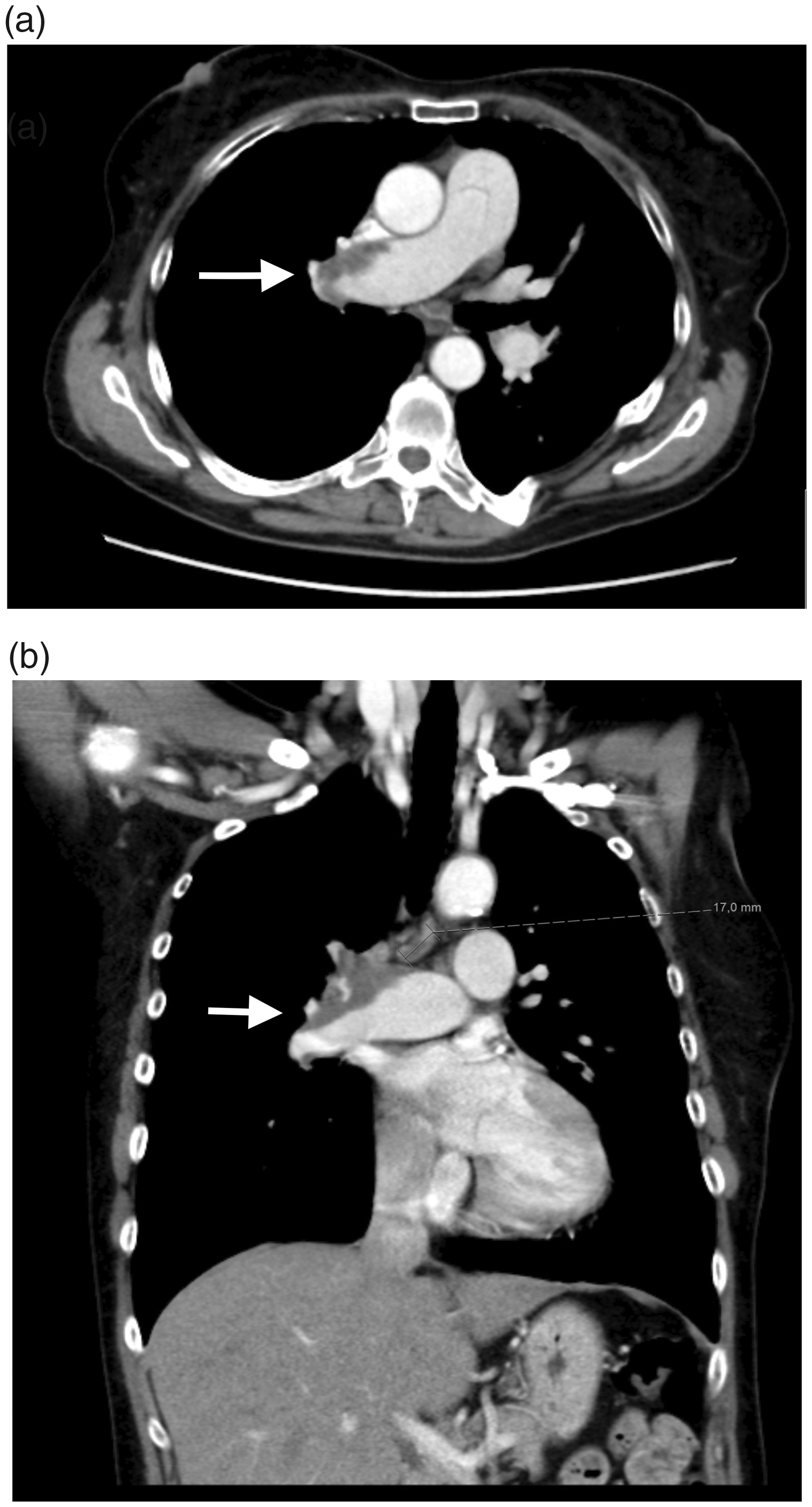
(a, b) A 65-year-old woman with central wall-adherent CTEPH, the peripheral dark gray area in the right pulmonary artery (arrow), misinterpreted as enlarged lymph nodes.
Increased MPA diameter was seen in 31 patients, but only reported in 10 of them. No radiologists appreciated the MPA:AA ratio. There were 30 patients with RVH ranging from mild to severe, but this was mentioned only in one report. The sensitivity in the original reports for reporting cardiovascular signs was 53.1% (95% CI = 34.7–70.9). An example of missed MPA diameter can be seen in Fig. 2.
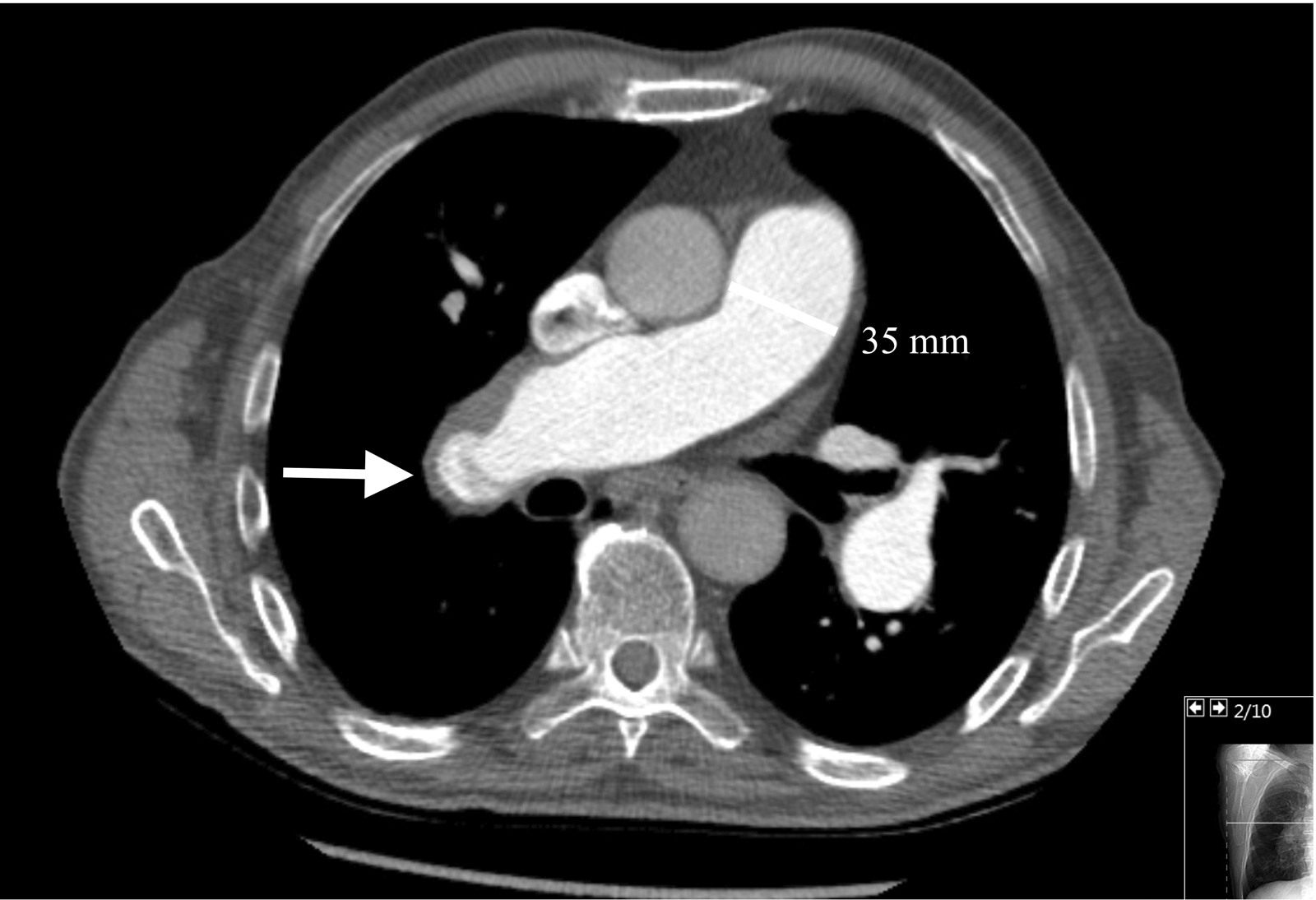
A 74-year-old man with a dilated MPA (35 mm) not mentioned in the original report. In the right pulmonary artery, wall-adherent CTEPH and webs can be seen (arrow); the web is seen as linear structures inside the vessel.
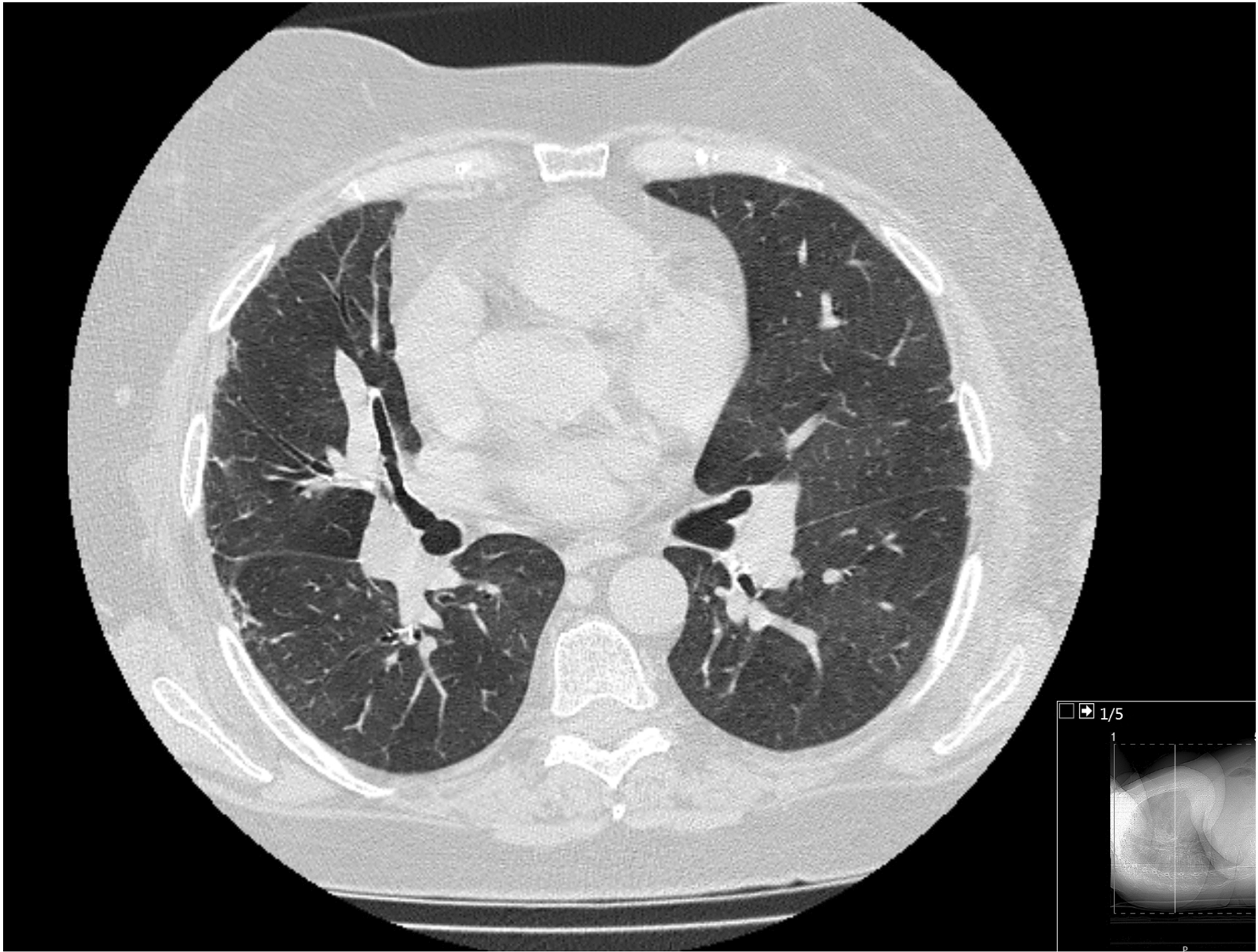
A 37-year-old woman with varying attenuation in the lung parenchyma misinterpreted as GGOs in the original report (arrow).
There were 32 patients with mosaic attenuation. In the original reports, mosaic attenuation was mentioned twice. There were four patients with mosaic attenuation incorrectly described as ground-glass opacities (GGOs) and three described as “ill-defined infiltrates.” There were 14 patients where the lung parenchyma was described as normal, but all of them had mosaic attenuation. In six original reports, the lung parenchyma was not mentioned at all; of these, mosaic attenuation was clearly evident in two patients. There were also a number of reports that described other incidental pulmonary findings such as fibrosis, infarctions, and tumors but failed to mention the presence of mosaic attenuation. The sensitivity among the original reports to describe mosaic attenuation was 6.3% (95% CI = 0.8–20.1). An example of misinterpreted mosaic attenuation can be seen in Fig. 4.
Discussion
The principal finding in our study was that only 9/35 CT exams with clearly visible signs of CTEPH were identified in the original reports, giving an overall sensitivity of 25.7% on a diagnostic level. It should be mentioned that the terminology “CTEPH” was only used in two patients. In another seven reports, a combination of PH and vascular signs of CTEPH was described but no conclusion was made with regards to the actual diagnosis. It should also be noted that our reference standard, the consensus reading, identified all CTEPH cases.
Regarding pulmonary arterial findings, the sensitivity in the original reports was 62.9%. Eleven of the original reports described eccentric filling defects, three reports mentioned the reduced size of segmental arteries, and two reports noted webs. There were also four reports that mentioned pulmonary arterial emboli of “chronic” character, without any further specification. According to the reference standard, the CT exams contained findings of bands/webs, calcified thrombi, eccentric filling defects, occlusions, reduced size of segmental arteries, tortuous vessels, and vascular pouches; most CT exams showed a combination of the findings mentioned. The results indicate that, except for wall-adherent eccentric thrombi, the knowledge of the other vascular findings in CTEPH is limited. It is also important to distinguish CTED from CTEPH, where the latter also has signs of PH although CT is less sensitive than right heart catheterization for making this distinction. However, among the 22 patients with positive vascular findings, the cardiovascular signs of PH were only assessed among ten. A meta-analysis from 2006 found that complete resolution of APE is not routinely achieved despite anticoagulation treatment. In fact, 52% of patients still have defects on imaging six months after diagnosis, whereas a plateau phase is reached (8). Thus, signs of isolated vascular findings or CTED should be expected frequently on CT in patients with a previous history of APE and should not cause a change in the treatment regimen without clinical correlation. A vague CT report could potentially result in unnecessary escalation of anticoagulation treatment and bleeding complications that easily could have been avoided.
The sensitivity of cardiovascular signs of PH in the CT reports was 53.1% compared to the reference standard. Increased MPA diameter was reported in 10 out of 31 cases where it was seen. None of the reports mentioned right-sided cardiac chamber dilatation. RVH was mentioned in only one of the 30 patients with RVH. It is likely that the reporters did not evaluate the cardiovascular structures besides the pulmonary circulation, even though assessment of the heart and vasculature should be a routine part of any radiological review of a thoracic CT.
The poorest knowledge among the radiologist was regarding mosaic attenuation, where only two out of 32 cases of mosaic attenuation were correctly mentioned corresponding to a sensitivity of only 6.3%. Mosaic attenuation was also frequently misinterpreted as GGOs or “ill-defined infiltrates.” The distinction between mosaic attenuation and GGO is crucial as they represent two entirely different pathological processes. In mosaic attenuation, the gray areas represent normally perfused lungs, while the darker areas are abnormal with reduced vessel count and this is a feature of pulmonary vascular disease. In GGOs, the gray areas indicate abnormally increased density and differentials include pulmonary parenchymal diseases. It has previously been proposed that the parenchymal findings in CTEPH might mimic other lung diseases such as air trapping in small airway disease (11), which leads to so-called mosaic attenuation pattern. The recognition of mosaic attenuation among radiologists in our study was surprisingly low.
The referring clinician may be of assistance to guide the radiologist by specifically mentioning relevant past history such as venous thromboembolism in the request. Furthermore, a specific query regarding CTEPH as well as pertinent questions such as the presence or exclusion of specific signs of pulmonary vascular features, cardiovascular signs of PH, and mosaic attenuation would be desirable. This would allow the radiologists to concentrate on the appropriate findings, using a structured reporting format that includes these features would be of immense assistance. The CT findings associated with CTEPH have been extensively described in literature for instance by Castaner and Ruggiero (19,20).
In our material, the sensitivity was better among the university hospitals at 63%. It should be noted that a few of the false-negative cases from university hospitals were reported by non-cardiothoracic radiologists.
Among the limitations in our study were the relatively small study population. However, in the general population, patients diagnosed with CTEPH are rather uncommon. The study population also represented a selected group, since it was constituted by patients referred to surgery. It is likely that patients referred to surgery have more advanced disease, which makes it even more noteworthy that the findings to a large extent were missed in the original reports. The study is also limited because it was conducted in a single country and the education and knowledge among radiologists may differ among countries. Still, we would argue that it is likely that the knowledge of CTEPH findings among radiologists is similar in other countries. The results in Tunariu’s study from the UK for instance shows similar results compared to our results among university hospitals (17). A comparison between radiologist’s performance on CT exams on CTEPH patients in different countries could be investigated in a separate study.
In conclusion, our study indicates a poor knowledge of CTEPH findings on CT among radiologists, leading to a falsely low sensitivity for CT. Discrepancies in CT interpretation will always occur due to failures of perception and misjudgments, but the lack of knowledge about CTEPH among the imaging community is an important additional source of error and should be addressed by appropriate education.
Footnotes
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Swedish Heart and Lung Foundation, the Swedish Society of Medicine and Stockholm City Council.