
Abstract
Background
Disputes exist regarding whether the apparent diffusion coefficient (ADC) can differentiate the tumor grade, deep myometrial invasion and lymphovascular space invasion (LVSI) in endometrial cancer. The aim of this review was to assess the diagnostic performance of the ADC value in endometrial cancer.
Material and Methods
The PubMed, Web of Science, Embase and Cochrane Library databases were searched for studies that used the ADC value to assess tumor grade, deep myometrial invasion and LVSI in endometrial cancer. We used forest plots to analyze the heterogeneity and generate the pooled sensitivity (SEN) and specificity (SPE). We used summary receiver operating characteristic (SROC) curves to work out the area under the SROC curve (AUC). Likelihood ratios (LRs) were also obtained.
Results
Of the 460 identified studies, 11 studies met our inclusion criteria and were included. Overall, nine studies (491 patients) aimed at differentiating high tumor grade had a pooled SEN, SPE and AUC of 77%, 73% and 81%, respectively; three studies (181 patients) for differentiating deep myometrial invasion had a pooled SEN, SPE and AUC of 71%, 67% and 77%, respectively; and two studies (106 patients) for differentiating LVSI had a pooled SEN and SPE of 66% and 74%, respectively. The positive and negative LRs were 2.77 and 0.35 for the tumor grade, 2.08 and 0.45 for deep myometrial invasion, and 2.48 and 0.45 for LVSI.
Conclusion
This meta-analysis showed that the ADC value had a moderate diagnostic performance for the tumor grade, deep myometrial invasion and LVSI in endometrial cancer.
Keywords
Introduction
In industrialized countries, endometrial cancer is one of the most common malignant gynecological tumors with an increasing morbidity (1,2). Surgical resection remains the main therapeutic and staging approach. The therapeutic decision depends on the tumor grade, depth of myometrial invasion and lymphovascular space invasion (LVSI). Arguments exist regarding whether pelvic lymphadenectomy should be performed in women with early-stage endometrial cancer. Randomized controlled trials have not provided support for routine systematic pelvic lymphadenectomy in low-risk early-stage endometrial cancer (3). Furthermore, for cervical stenosis patients, it is difficult to perform the curettage. Thus, preoperative accurate assessments of the tumor grade and the International Federation of Gynecology and Obstetrics (FIGO) stage in endometrial cancer are essential for the treatment decision, surgical planning and prognosis evaluation (4).
Magnetic resonance (MR) imaging has an excellent spatial resolution and soft-tissue contrast. Its multiparameter imaging capability makes it a good imaging tool for the preoperative evaluation of endometrial cancer. MR imaging has been used to assess tumor grade, myometrial invasion and LVSI (5). Moreover, studies have shown that quantitative apparent diffusion coefficient (ADC) measurement of diffusion-weighted imaging (DWI) provides a new approach for determining these factors in endometrial cancer (6). However, these studies included a limited number of patients and reported varied diagnostic performances (7–10). Thus, there is a need for an updated systematic review assessing the diagnostic value of the quantitative ADC value.
The purpose of this meta-analysis is to determine the diagnostic performance of the quantitative ADC value for the tumor grade, deep myometrial invasion and LVSI in endometrial cancer, using pathological diagnosis as a reference standard.
Material and methods
This meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) recommendations (11).
Search strategy
We conducted online literature searches to identify studies up to 18 December 2018 in a wide range of electronic databases: PubMed, Web of Science, Embase and Cochrane Library. The key words were as follows: ‘endometrial cancer’, ‘ADC’, ‘tumor grade’ or ‘myometrial invasion’, ‘lymphovascular space invasion’ (see supplementary material 1). These searches were performed separately and had no limitation regarding language or time. Two investigators screened the search results to exclude irrelevant articles. The full text was examined for potentially eligible studies, and disagreements were resolved through discussion.
Study inclusion and exclusion criteria
We included studies that met the following criteria:
Types of research: both retrospective and prospective cohort studies. Participants: regardless of the FIGO stage, only the patient whose final stage was based on the results from surgical staging. Target condition: presurgical MR imaging diagnosis of tumor grade, deep myometrial invasion and LVSI in primary endometrial cancer. Index test: DWI-MR imaging sequences with the ADC value of the tumor, without considering the applied protocol of acquisition (method of drawing region of interest (ROI) or using MR imaging or positron emission tomography (PET)-MR imaging). All ADC values were derived from the tumor. Reference standard: pathological diagnosis of tumor grade, presence of deep myometrial invasion and LVSI. Minimum data required: sufficient data to work out the true positive (TP), false positive (FP), false negative (FN) and true negative (TN).
The exclusion criteria were as follows:
Study population fewer than 10 patients. Publication type other than original research (e.g. review articles). Pathological diagnosis was not derived from surgical specimen, such as D & C (endometrial biopsy or dilatation and curettage). Studies enrolled not only endometrial cancer (e.g. mixed endometrial cancer with cervical cancer). Incomplete data to establish the 2 × 2 table.
Data extraction and quality assessment
Two reviewers independently extracted the data of the diagnostic accuracy results and additional useful information. Disagreements were resolved by a third physician. The main outcome indexes extracted were the number of patients with endometrial cancer, sensitivity (SEN) and specificity (SPE) of each original study (If a study had two or more SENs and SPEs, the result with the highest accuracy was extracted). G3 is defined as high grade, and G1 and G2 are defined as low grade. Deep invasion is defined as myometrial invasion greater than 50% of thickness. LVSI is considered positive by referring histological reports. The clinical stage refers to the FIGO classification.
We referred to the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) to assess the quality of the included studies (12). In the Index Test domain, studies that used the mean ADC value from the whole tumor volume were considered low risk. In the Flow and Timing domain, which refers to the time interval between imaging and surgical resection, 30 days was considered appropriate.
Statistical analysis
Meta-disc1.4 (Universidad Complutense, Madrid, Spain), SPSS 20 (IBM, Chicago, IL, USA), STATA 15.0 (Stata Corp, College Station, TX, USA and Open Meta Analyst) and Reveman 5.2 were used to analyze the data. We assessed publication bias using a Deeks’ funnel plot and a Deeks’ asymmetry test (13). The calculation formula of the SEN and SPE were as follows: SEN = TP/(TP + FN); SPE = TN/(FP + TN). TP + FN was equal to the histological positive patient number (patients’ number of G3, deep myometrial invasion or positive LVSI). FP + TN was equal to the negative patient number (patients’ number of G1 + G2, myometrial invasion less than 50% or negative LVSI).
The heterogeneity of the SEN and SPE of each included study was analyzed using the forest plots on the basis of a random-effects model. The summary receiver operating characteristic (SROC) curve was used to assess the pooled diagnostic performance. The presence of heterogeneity was assessed by means of a test on the Q statistic and I square index (14,15). A p value <0.05 indicated the existence of heterogeneity. I square was used to interpret the degree of heterogeneity. The heterogeneity was considered significant when I square was greater than 50%. A Spearman correlation coefficient was used to determine the threshold effect (a strong positive correlation of r > 0.6 or p < 0.05 was suggestive of the threshold effect) (16).
Clinical utility
Positive and negative likelihood ratios (LRs) for the ADC value were obtained to characterize the clinical utility of the ADC value. The posttest probability of endometrial cancer was calculated by LRs (17). The details of the calculation process are shown in supplementary material 1. The ADC value posttest probabilities for G3, deep myometrial invasion and LVSI were calculated separately.
Results
Included studies
A total of 460 studies were identified through the electronic search. The flow chart of the selection process is shown in Fig. 1. Among these studies, 391 studies were discarded after reviewing the title or abstract; 39 studies were discarded after reviewing the full text; and 19 studies were discarded for failing to meet the inclusion criteria. The remaining 11 studies were ultimately included, with 9 studies for the tumor grade (7–9,18–23), 3 studies for the myometrial invasion (9,24,25) and 2 studies for the LVSI (7,9). No additional studies were identified from the references or reviews. No discrepancies occurred between the two reviewers during the study selection.

Flowchart shows the flow of information extraction of this meta-analysis.
Methodological quality of included studies
The risk of bias and applicability concerns graph of the selected studies are shown in Fig. 2(a) and (b). We referred to the QUADAS-2 to assess the included studies. In the Patient Selection domain, the studies that did not indicate patients were enrolled consecutively were considered an unclear risk; the studies that did not indicate inclusion or exclusion criteria or clearly describe the reasons for eliminated patients were defined as an unclear risk. In the Index Test domain, one study did not implement blinding (20), while three studies did not describe the blinding (9,19,25); two studies used the quartile ADC and one study used the max ADC from the whole tumor volume (7,8,18), four studies’ mean ADC value, which was derived from the tumor on a single slice, were considered an unclear risk (19–21,23), and two studies’ minimum ADC values derived from PET-MR imaging were considered a high risk (9,25). In the Flow and Timing domain, four studies had an interval time of more than 30 days between MR imaging and the operation (the longest interval time was 51 days) (9,18,23,24), and two studies did not describe the interval time (7,19). Details show in the supplementary material 2. The Deeks’ funnel plot shows no publication bias for the tumor grade
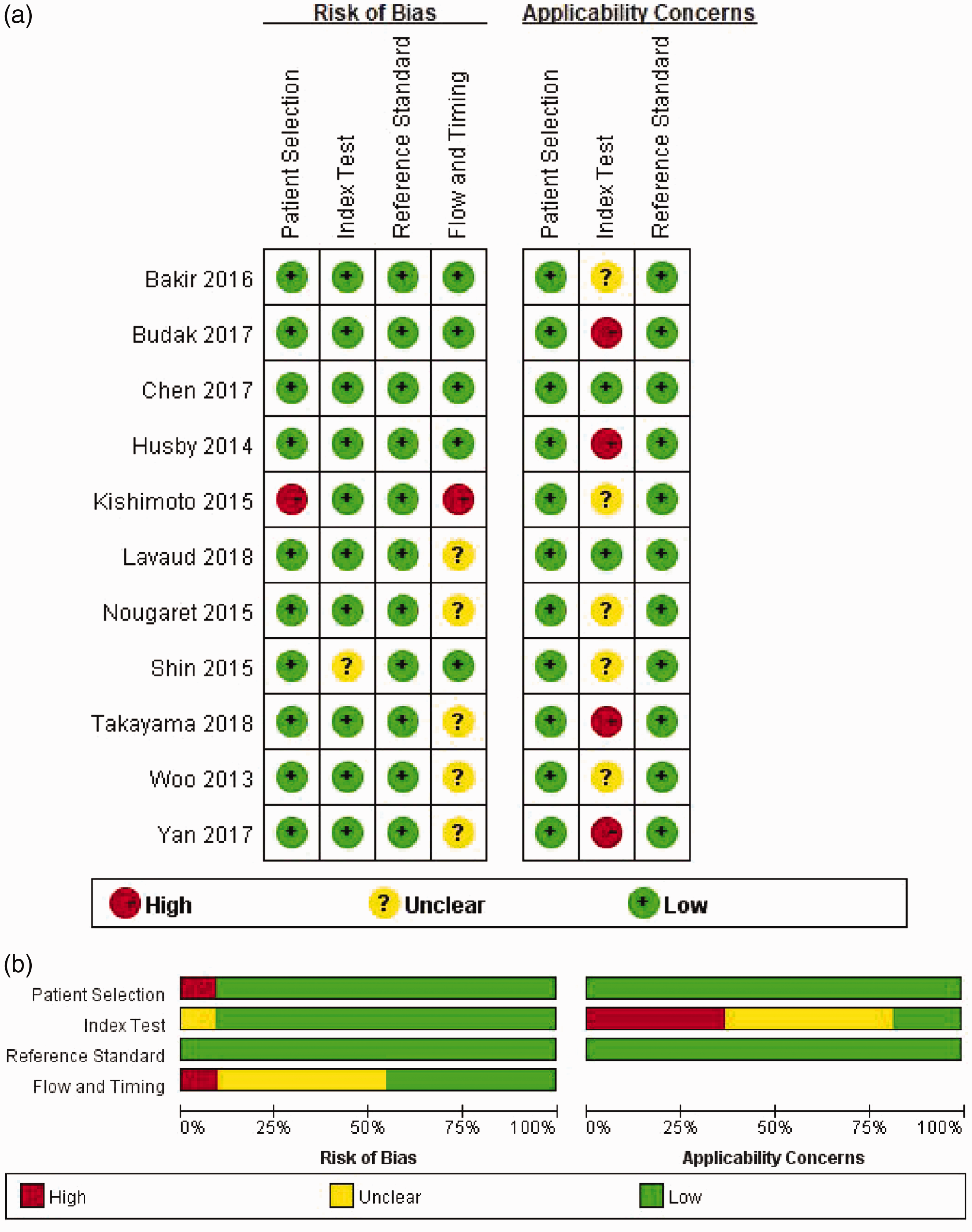
(a) Risk of bias and applicability concerns summary graph shows review authors’ judgements regarding each domain for each included study. (b) Risk of bias and applicability concerns. Review authors’ judgements regarding each domain present as percentages across included studies. Stacked bar charts of QUADAS-2 scores of methodologic study quality expressed as the percentage of studies that met each criterion. For each quality domain, the proportions of included studies that suggest low, high, or unclear risk of bias and/or concerns regarding applicability are displayed in green, red and yellow, respectively.
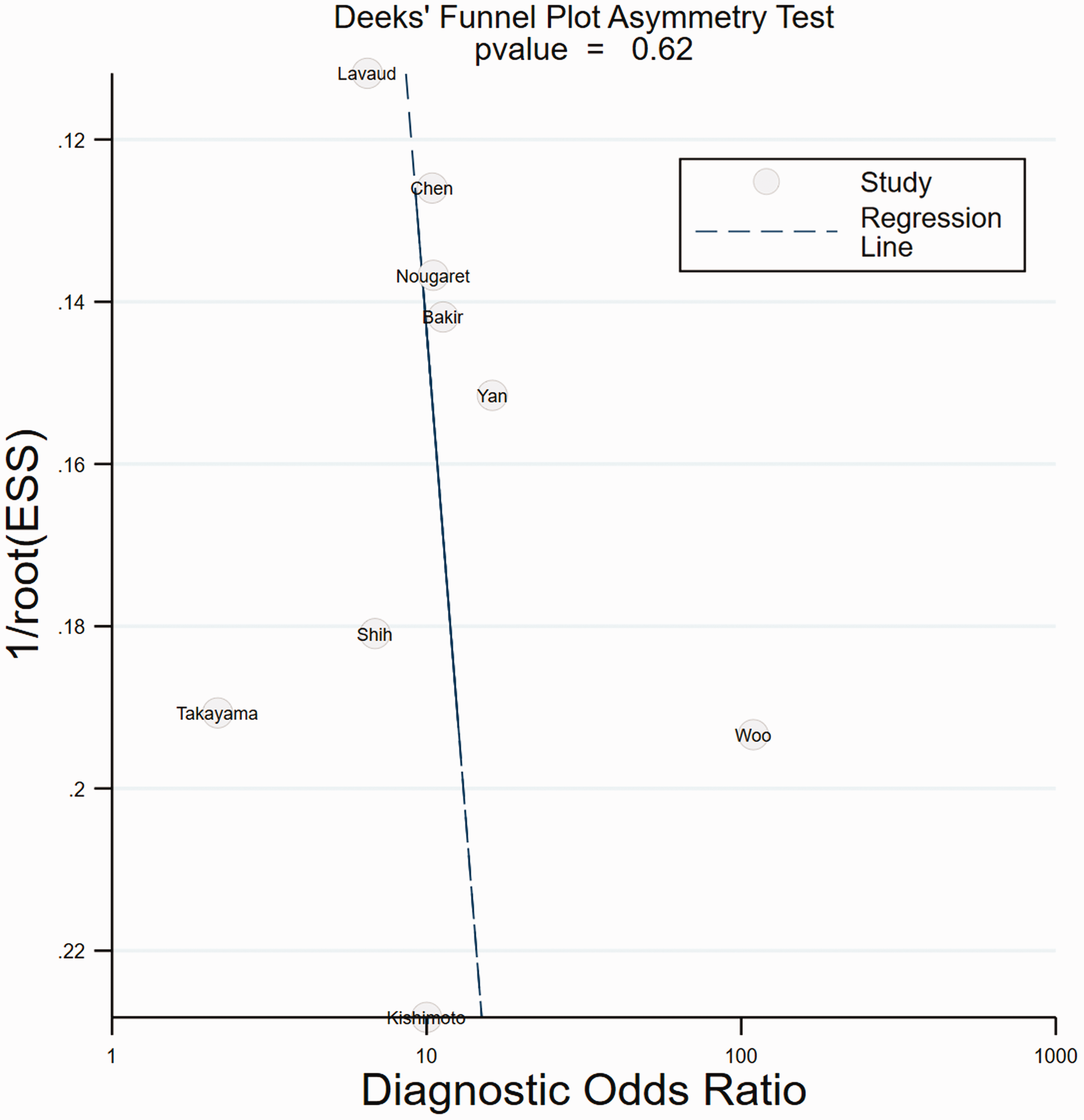
Deeks’ funnel plot for graphical exploration of publication bias for the tumor grade. Deeks’ test for asymmetry is not significant (p = 0.62). Deeks’ funnel plot shows an absence of publication bias.
Characteristics of included studies
A total of 778 patients (491 patients for tumor grade, 181 patients for myometrial invasion and 106 patients for LVSI) in academic diagnostic studies in periods that ranged from January 2005 to March 2016 were included in the final analyses. Overall, four studies were prospective, three studies were performed using 3T MR (two studies used PET-MR), and eight studies were performed using 1.5T MR. There were six studies that enrolled endometrioid and nonendometrioid tumors, while the other studies enrolled only endometrioid tumors. A total of six studies drew ROIs of the whole tumor volume, in which one study included the necrotic area in the ROI and two studies did not describe whether the ROI included the necrotic area. The main patient characteristics of the primary studies are listed in Table 1. The age was similar across studies (range 24–93 years). The menstrual status of patients was not taken into consideration.
Characteristics of included studies.

Mean of three random ROIs.
*Data derived from PET-MRI.
ADC: apparent diffusion coefficient; EEA: endometrioid endometrial adenocarcinoma; LS: largest slice (slice containing the largest tumor cross-section); mixed: endometrioid endometrial adenocarcinoma and other histological subtypes; MRI: magnetic resonance imaging; NA: not available; PET: positron emission tomography; Pro: prospective; Retro: retrospective; ROI: region of interest; SS: single slice.
Diagnostic performances of ADC value in preoperative diagnosis
The diagnostic performances of the ADC value for the tumor grade, deep myometrial invasion and LVSI are shown in the forest plots of Fig. 4 and in the SROC plots of Fig. 5.
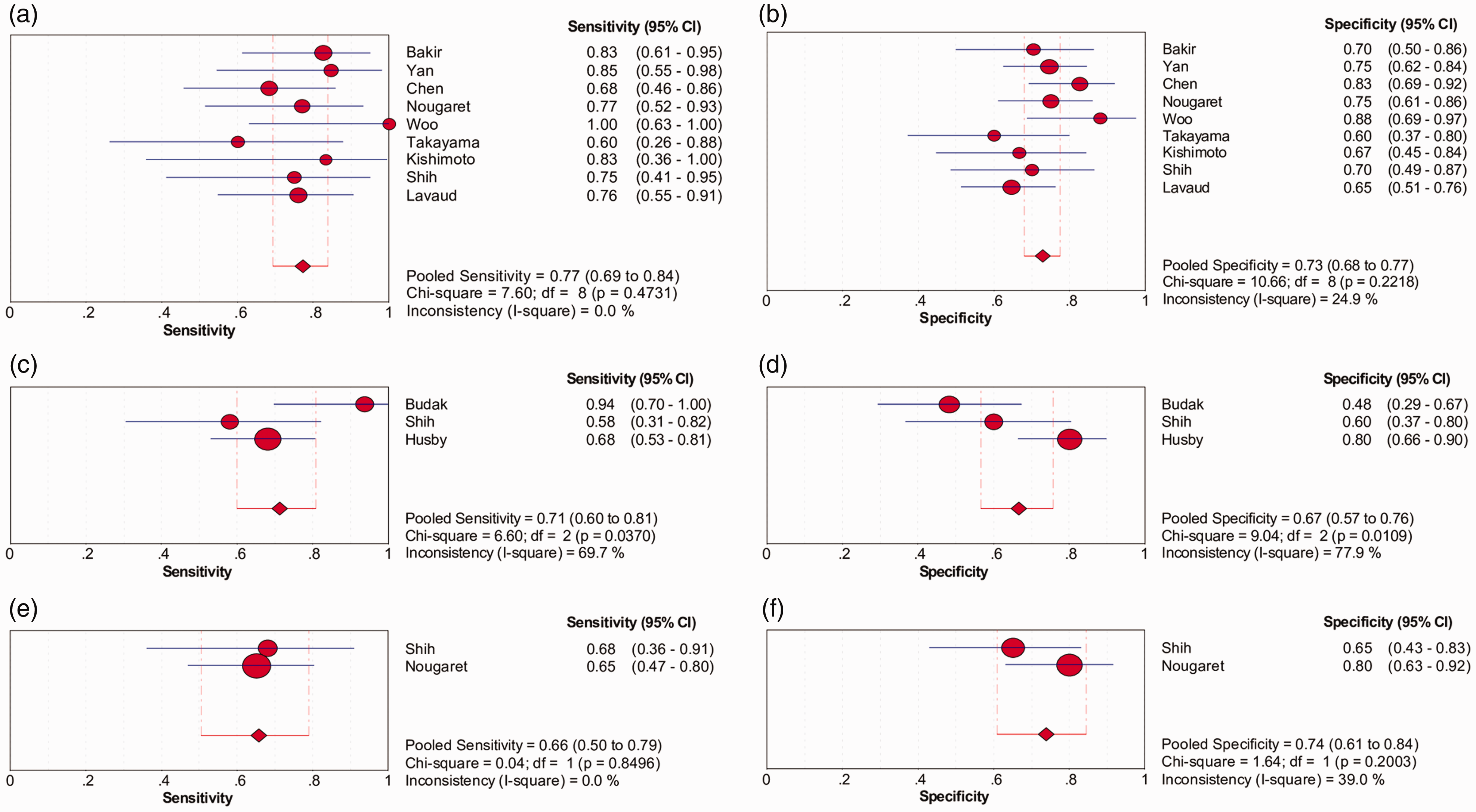
Forest plots of diagnostic performance (sensitivity and specificity) of each study for the tumor grade (a, b); the deep myometrial invasion (c, d) and the LVSI (e, f). Horizontal lines indicate a per-node basis with 95% CIs. Diamond at bottom and vertical dotted line indicate the pooled sensitivity or specificity with 95% CIs. Heterogeneity statistics (I square value, Q value) for sensitivity and specificity are also shown.

SROC curve of the included studies using ADC values to differentiate the G3 tumor (a) and the deep myometrial invasion (b).
All analyses were performed in a random-effects model. No significant heterogeneity was identified for the SEN or SPE in the tumor grade (p = 0.47 and I square = 0.0% and p = 0.22 and I square = 24.9%, respectively). Significantly heterogeneity was identified for the SEN and SPE in deep myometrial invasion (p = 0.04 and I square = 69.7%, and p = 0.01 and I square = 77.9%, respectively). Meta-regression could not be performed to explain the significant heterogeneity of myometrial invasion because of the limited included studies. No significant heterogeneity was identified for the SEN and SPE in LVSI (p = 0.85 and I square = 0.0% and p = 0.20 and I square = 39.0%, respectively). The Spearman rank correlation analysis showed that the correlation coefficient was -0.45 (p = 0.22) for the tumor grade and 0.5 (p = 0.67) for myometrial invasion, which indicated no threshold effect in the tumor grade and deep myometrial invasion. The pooled SEN, SPE and AUC were 77% (95% confidence interval (CI): 69.3–84.0%), 73% (95% CI: 67.9–77.4%) and 81% (95% CI: 78.2–83.5%), respectively, for tumor grade; 71% (95% CI: 60.1–80.8%), 67% (95% CI: 56.6–75.8%) and 77% (95% CI: 69.9–83.1%), respectively, for deep myometrial invasion; and 66% (95% CI: 50.5–79%) and 74% (95% CI: 60.8–84.5%) for LVSI. The SROC could not be established due to only two studies being included.
The LRs of the ADC value were derived from the included nine studies (491 patients) for the prediction of tumor grade; from the three studies (181 patients) for the prediction of deep myometrial invasion; and from two studies (106 patients) for the prediction of LVSI. The positive LRs of the ADC value for the tumor grade, deep myometrial invasion and LVSI were 2.77 (95% CI: 2.22–3.45), 2.08 (95% CI: 1.27–3.39) and 2.48 (95% CI: 1.47–4.20), respectively, and the negative LRs were 0.35 (95% CI: 0.26–0.48), 0.45 (95% CI: 0.25–0.82) and 0.45 (95% CI: 0.30–0.69), respectively. The pretest probabilities were 28% for G3 tumor grade, 44% for deep myometrial invasion and 40% for LVSI. The posttest probabilities of ADC value used to diagnose G3 tumor, deep myometrial invasion and LVSI, were 52% (95% CI: 46–57%), 62% (95% CI: 50–73%) and 62% (95% CI: 54–77%), respectively. The posttest probabilities of ADC value used to exclude G3 tumor, deep myometrial invasion and LVSI, were 12% (95% CI: 9–16%), 26% (95% CI: 16–39%) and 23% (95% CI: 16–31%), respectively.
Discussion
Histological grade, depth of myometrial invasion and LVSI are important prognostic factors strongly associated with the management strategies and survival of individuals with endometrial cancer (26). In this meta-analysis, the preoperative diagnostic ability of the ADC value in these three factors was investigated.
Previous studies have shown that the ADC value was correlated with the tumor grade and could be used to differentiate low grade from high grade endometrial cancers. It has been suggested that high risk tumors tend to have a low ADC value due to the tumor’s high cellularity, proliferation and perfusion and less extracellular space (27,28). Previous studies have reported that the SEN and SPE for the tumor grade ranged from 55–100% and 70.4–89%, respectively (7–9,18–23). This meta-analysis showed a moderate diagnostic performance, with the pooled SEN and SPE of 77% and 73%, respectively. However, controversy exits regarding whether the ADC value can be used to differentiate the tumor grade (29,30). A considerable overlap of the ADC value has been found between low grade and high grade endometrial cancer in previous studies, which indicates other factors, such as nuclear atypia and the different pathological proteins, may contribute to the tumor grade that cannot be displayed by the ADC value (31,32). Furthermore, ADC values are different in various histological subtypes of endometrial cancer. According to the study of Takeuchi et al., the ADC value of carcinosarcomas is higher than that of G3 endometrioid adenocarcinomas (33). Carcinosarcomas have a higher frequency of necrosis and epithelial cystic components, which can increase the tumor’s ADC value. Moreover, this meta-analysis included not only endometrioid adenocarcinoma but also nonendometrioid adenocarcinomas. Furthermore, the difference in the genomic characterization of endometrial cancer may be attributed to the different biological behavior of the same traditional histology tumor grade (34). Thus, the performance of the ADC value may be affected.
Previous studies have shown that the ADC value could be used to assess deep myometrial invasion, with the SEN and SPE ranging from 47.6–78% and 57–88%, respectively (9,24,25). In this meta-analysis, moderate SEN and SPE were identified in evaluating the deep myometrial invasion. In contrast, DWI could show the boundary of the tumor and normal myometrium more clearly than T2-weighted imaging, and a high b-value-DWI had a high contrast-to-noise ratio.(35) The SEN and SPE of DWI were 86% and 86%, respectively, for deep myometrial invasion, which indicates a higher diagnosis performance achieved than the ADC value (36). Furthermore, the ADC value measurement seriously depended on drawing the ROI on the ADC map which has a low signal-to-noise ratio. Moreover, it is difficult to draw an accurate ROI along with an unclear tumor boundary because many patients had small tumors and an atrophic uterus, and it is also affected by the movement or position of the uterus. Thus, substantial useful information would be missed.
It is controversial whether the ADC value is able to identify the LVSI (7,9). Our meta-analysis included only two studies, which limited us to come to a conclusion. We thought that the different stages of endometrial cancers included may affect the ADC value to identify the LVSI.
Several potential explanations for the moderate diagnostic performance of the ADC value in these three predictive factors are as follows: first, the tumor’s ADC value may be different from the tumor invasion area’s ADC value, and it also cannot represent the invasion area. Second, the acquisitions of the ROIs were different in the included studies. Tumor heterogeneity was represented more accurately using the tumor volumetric ADC value than the selected ROI ADC value (37). Third, a different ROI drawing approach had a significant difference in the ADC value (38). Fourth, the different menstrual status and phase influence the ADC value (39).
The clinical usefulness of an examination is well expressed by the LRs. Clinically useful tests should have a high positive LR (>5.0, ‘good for confirming disease’) and a low negative LR (<0.2, ‘good for ruling out disease’) (17). The positive LR of 2.77 and the negative LR of 0.35 indicated limited clinical usefulness of the ADC value in diagnosing a G3 tumor. In patients with G3 tumors, a positive ADC value would increase the probability from a pretest of 28% to a posttest of 52%. This finding indicated that only 52% of the patients diagnosed as G3 tumors by the ADC value were actually G3 tumors. Insufficient studies were available for drawing a powerful conclusion in the deep myometrial invasion and LVSI. Therefore, for endometrial cancer, a single quantitative ADC value had a limited diagnostic performance for these three factors. Combined with other techniques, such as endometrial cancer radiomics, a quantitative ADC value might be more helpful to assess the tumor invasiveness (40).
There were several limitations in this meta-analysis. First, a small number of studies, particularly for deep myometrial invasion and LVSI, were included in this study, which did not enable investigation of all potential causes of heterogeneity. Second, we did not separately analyze the three predictive factors to reduce the interaction, and comparisons of the ADC value between superficial and deep myometrial invasions were not performed in different tumor grades. Third, we did not analyze the diagnostic performance of the ADC value of different ROIs.
In conclusion, this meta-analysis showed that the ADC value had a moderate diagnostic performance for the tumor grade, deep myometrial invasion and LVSI in endometrial cancers. Further studies that combine the ADC value with other techniques of analysis and imaging are warranted.
Supplemental Material
Supplemental Material1 - Supplemental material for The diagnostic performance of ADC value for tumor grade, deep myometrial invasion and lymphovascular space invasion in endometrial cancer: a meta-analysis
Supplemental material, Supplemental Material1 for The diagnostic performance of ADC value for tumor grade, deep myometrial invasion and lymphovascular space invasion in endometrial cancer: a meta-analysis by Bi Cong Yan, Mei Ling Xiao, Ying Li and Jin Wei Qiang in Acta Radiologica
Supplemental Material
Supplemental Material2 - Supplemental material for The diagnostic performance of ADC value for tumor grade, deep myometrial invasion and lymphovascular space invasion in endometrial cancer: a meta-analysis
Supplemental material, Supplemental Material2 for The diagnostic performance of ADC value for tumor grade, deep myometrial invasion and lymphovascular space invasion in endometrial cancer: a meta-analysis by Bi Cong Yan, Mei Ling Xiao, Ying Li and Jin Wei Qiang in Acta Radiologica
Footnotes
Acknowledgements
Bi Cong Yan and Mei Ling Xiao contributed equally to the writing of this article. The author contributions were as follows:
Bi Cong Yan: literature research, acquisition of data, quality assessment, drafting of the manuscript.
Mei Ling Xiao: literature research, acquisition of data.
Ying Li: quality assessment, acquisition of data, statistical analysis.
Jin Wei Qiang: study concept and design, critical revision of the manuscript for important intellectual content, study supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Shanghai Municipal Commission of Health and Family Planning (No. ZK2015A05)
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.