
Abstract
Background
Evaluation of small cystic lesions of the pancreas remains a challenging task, as due to their size appearance can be rather hypodense than clearly fluid-filled.
Purpose
To evaluate whether additional information provided by novel dual-layer spectral-detector computed tomography (SDCT) imaging can improve assessment of these lesions.
Material and Methods
For this retrospective study, we reviewed reports of 1192 contrast-enhanced portal-venous phase SDCT scans of the abdomen conducted between May 2017 and January 2019. On basis of the radiological report 25 small (≤1.5 cm) cystic pancreatic lesions in 22 patients were identified, in which additional short-term follow-up imaging was recommended to confirm/clarify cystic nature. Conventional images (CI) and spectral images (SI) including virtual-monoenergetic images at 40 keV (VMI), iodine-density and iodine-overlay images were reconstructed. Two readers indicated lesion conspicuity and confidence for presence of cystic nature on three-point scales. First, solely CI were evaluated, while in a second reading after a four-week interval, the combination of CI and corresponding SI were reviewed. Quantitatively, ROI-based mean attenuation was measured in CI and VMI.
Results
In the subjective reading, SI significantly improved lesion conspicuity (CI 2 [1–2], SI 3 [2–3], P < 0.001) and confidence regarding presence of cystic nature (CI 2 [1–2], SI 3 [3–3], P < 0.001). Inter-observer agreement depicted by intraclass correlation coefficient improved considerably from 0.51 with only CI to 0.85 when the combination with SI was used. Further, VMI displayed significantly higher signal-to-noise (CI 1.2 ± 0.8, VMI 3.2 ± 1.8, P < 0.001) and contrast-to-noise ratios (CI 2.6 ± 0.8, VMI 4.7 ± 1.9).
Conclusion
Compared to CI alone, combination with SI significantly improves visualization and confidence in evaluation of small equivocal cystic pancreatic lesions.
Keywords
Introduction
Cystic pancreatic lesions are a common finding in computed tomography (CT) imaging of the upper abdomen. Recently, prevalence increased due to improved imaging techniques and an aging population, e.g. in the United States prevalence in patients aged 80–84 years is 8.7% (1). Clinical management of these lesions remains difficult reflected by frequent changes of guidelines (2–4). Imaging follow-up schemes differ depending on lesion size, morphology, and patient age, as recently suggested by the Incidental Findings Committee of the American College of Radiology (1,2). Diagnostic uncertainty mostly occurs in smaller cysts (2), as reliable differentiation to pancreatic ductal adenocarcinoma or pancreatic metastases is hampered as particularly small cystic lesions can appear hypodense rather than fluid-filled (2,5). Pancreatic duct adenocarcinoma still represents the fourth leading cause of death due to cancerous disease in the United States (6) with poor prognosis (7). In clinical management, patients with an equivocal pancreatic cystic lesion therefore often experience additional short-term follow-up imaging to confirm diagnosis before they enter dedicated long-term follow-up schemes (2,5,8,9).
Clinical dual-energy CT scanners that can separate low and high energetic photons are increasingly available. Emission-based technical solutions (e.g. dual-spin, dual-source, split or twin beam, and rapid kilovoltage switching) were introduced first (10). More recently, a new type of scanner has become available that uses detector-based separation of photons, commonly referred to as spectral-detector CT (SDCT). This scanner type uses one X-ray source and a detector with two layers; photons with higher energies are detected at the lower layer, while lower energetic photons are detected at the upper layer (10,11). Identification of iodine using material decomposition allows for the creation of iodine density and iodine overlay images that can be used to establish cystic nature of lesions. Further, absence of iodine uptake can be regarded as a sign of benignancy (12–15). In addition, virtual monoenergetic images (VMI) that correspond to images resulting from true monoenergetic X-ray examinations can be created (8,10,11). These specialized reconstructions can improve visualization and characterization of pancreatic lesions as has been shown for pancreatic ductal adenocarcinoma (16–18). Initial data on cystic pancreatic lesions (19,20) and more recent data on cystic renal lesions (21) demonstrated the potential of dual-energy CT (DECT) to improve visualization and diagnostic confidence.
Small cystic lesions of the pancreas are often defined as equivocal because their size hampers certain determination of their cystic character (2). The aim of the present study was to evaluate the additional value of spectral images for this lesion type and to test whether VMI, iodine density, and iodine overlay images can improve visualization and therefore enhance diagnostic confidence.
Material and Methods
The present study was approved by the institutional review board and the standards of the Health Insurance Portability as well as Accountability Act were followed. Informed written consent under Code of Federal Regulations (title 45, §46.116d) was waived due its retrospective nature. In a first step, 1192 contrast-enhanced portal venous phase SDCT scans of the abdomen conducted between May 2017 and January 2019 were identified using the institution’s radiological information system. To be included in the final analysis the following additional criteria were required: (i) mentioned in the radiological report: presence of an incidental pancreatic cystic lesions ≤1.5 cm with advice for short-term follow-up imaging to confirm/clarify cystic nature; (ii) portal venous phase staging and restaging examinations; and (iii) patient age ≥18 years. Following these criteria, 22 patients with 25 target lesions were eligible for study inclusion. As uncertainty more frequently occurs in smaller cysts (2,5) and the guidelines of the American College of Radiology for management of incidental pancreatic cysts lists lesions ≤1.5 cm as a dedicated subgroup with adapted recommendations (2), we chose to set a diameter of ≤1.5 cm as the cut-off for study inclusion.
Imaging protocol
All scans were performed on a clinical SDCT (IQon, Philips, Cleveland, Ohio, USA). Iodinated contrast media (Optiray 350, Guerbet, Bloomington, IN, USA) was administered through peripheral vein with a flow rate of 1.5–2.0 mL/s. Total amount was adapted to the body weight (1.5 mL/kg, maximum amount of contrast media injected was set to 140 mL). Seventy seconds after the administration of contrast media, image acquisition was started. Scan parameters were as follows: collimation = 64 × 0.625 mm; rotation time = 0.33 s; pitch = 0.98; matrix = 512 × 512. Tube voltage was 120 kVp and automatic tube current modulation was applied (DoseRight 3D-DOM, Philips Healthcare). The vendor’s dedicated spectral reconstruction algorithm was used enabling reconstruction of conventional CT images (CI) and VMI in the range of 40–200 keV (increments of 10 keV), iodine density, as well as iodine overlay images (Spectral B, level 3, Philips Healthcare). Slice thickness was set to 3 mm.
Subjective analysis
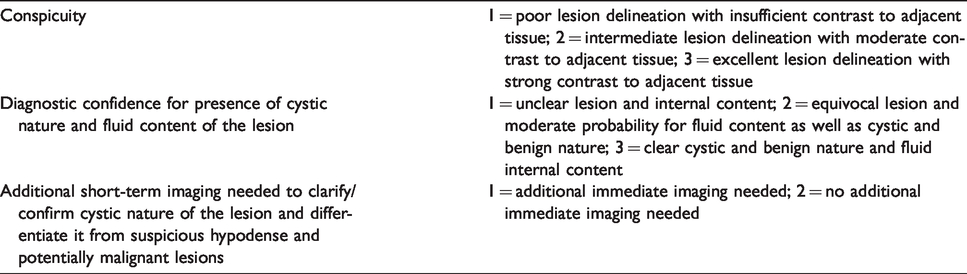
Two radiologists with 17 and 4 years of experience in abdominal imaging performed the subjective reading independently. Both readers were already familiar with spectral images and given exemplary teaching cases which were not part of the original dataset. The reading was performed in two sessions with an interval of four weeks and a differently randomized order to minimize recall bias. In the first session, readers only evaluated the conventional images. In the second session, readers were presented with the same images in combination with the corresponding spectral image set including VMI at 40 keV, iodine density, and iodine overlay images. Readers were asked to evaluate on a 3-point scale the conspicuity of the lesion and diagnostic confidence regarding a cystic character and fluid internal content of the lesion (see Table 1 for more detailed information). Readers were also asked if, due to poor visualization, additional short-term follow-up would be required to clarify cystic character of the lesion and differentiate it from suspicious hypodense and potentially malignant neoplasm (Table 1).
Subjective lesion assessment.
Clinical information.
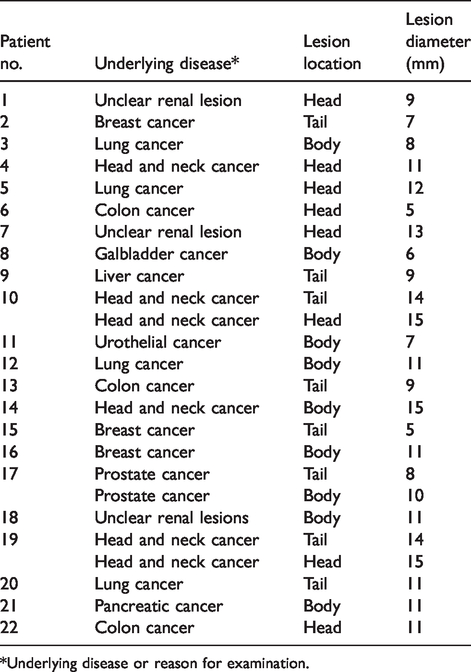
*Underlying disease or reason for examination.
Objective analysis
Quantitative analysis of all lesions was conducted in the vendor’s proprietary image viewer (IntelliSpace Portal v9, Philips Healthcare) on axial images by applying circular regions of interest (ROI) of a standardized size of 40 mm2. ROI size could be adjusted if lesions were very small to a minimum of 15 mm2. To measure the mean and SD of attenuation, two ROIs were placed in the target lesion at different slice positions and the results averaged. Three ROIs were placed and the results averaged in pancreas parenchyma covering head, body, and tail. A single ROI was placed in subcutaneous fat. First, ROIs were placed in conventional images and then copied to VMI to ensure equal size and localization. Signal-to-noise ratio (SNR) of the pancreas and the lesion were calculated and lesion-to-pancreas contrast-to-noise ratio (CNR) were calculated:
Statistical analysis
JMP Software was used for the statistical analysis (V14, SAS Institute). Quantitative results are given as mean ± SD and qualitative results by median and 10/90 percentile. Shapiro–Wilk test was used to test for presence of normal distribution. Wilcoxon-test signed-rank test was used for testing of any difference. Statistical significance was set as P < 0.05. Inter-observer agreement was assessed using intraclass correlation coefficient (ICC) and interpreted as follows: poor <0.40; fair = 0.40–0.59; good = 0.60–0.75; and excellent = 0.75–1.0.
Results
In the final analysis, 25 cystic pancreatic lesions of 22 patients were included (12 women, 10 men; mean age = 74.9 ± 7.8 years). The average lesion diameter was 10.3 ± 3.0 mm (range = 5–15 mm), whereby 11 lesions were ≤10 mm and 14 lesions were between >10 and ≤15 mm. More detailed patient information can be seen in Table 2.
Subjective assessment
In the subjective reading, conventional grayscale images alone allowed for intermediate lesion delineation, whereby a considerable number of lesions (44%) were even rated as poor delineable with insufficient contrast to adjacent tissue (mean score 2 [1–2]; Fig. 1, Table 3). In contrast, the combination of conventional images with spectral images including VMI at 40 keV, iodine density, and iodine overlay images significantly improved lesion conspicuity (mean score 3 [2–3]) and was rated as excellent with strong contrast to adjacent tissue (Fig. 1, Table 3). Conspicuity of the very small lesions < 10 mm was worse compared to the small sized lesions of 10–15 mm in the evaluation of conventional images (P = 0.014) and the combination with spectral images (P = 0.018; Fig. 1, Table 3). Still, also for very small lesions, conspicuity was significantly higher when using the combination of conventional and spectral images (Table 3). For example, using just conventional images, readers found delineation for very small lesions poor with insufficient contrast to adjacent tissue (1 [1–2]) whereas small sized lesions had intermediate lesion delineation (2 [1–2]; Fig. 1, Table 3).
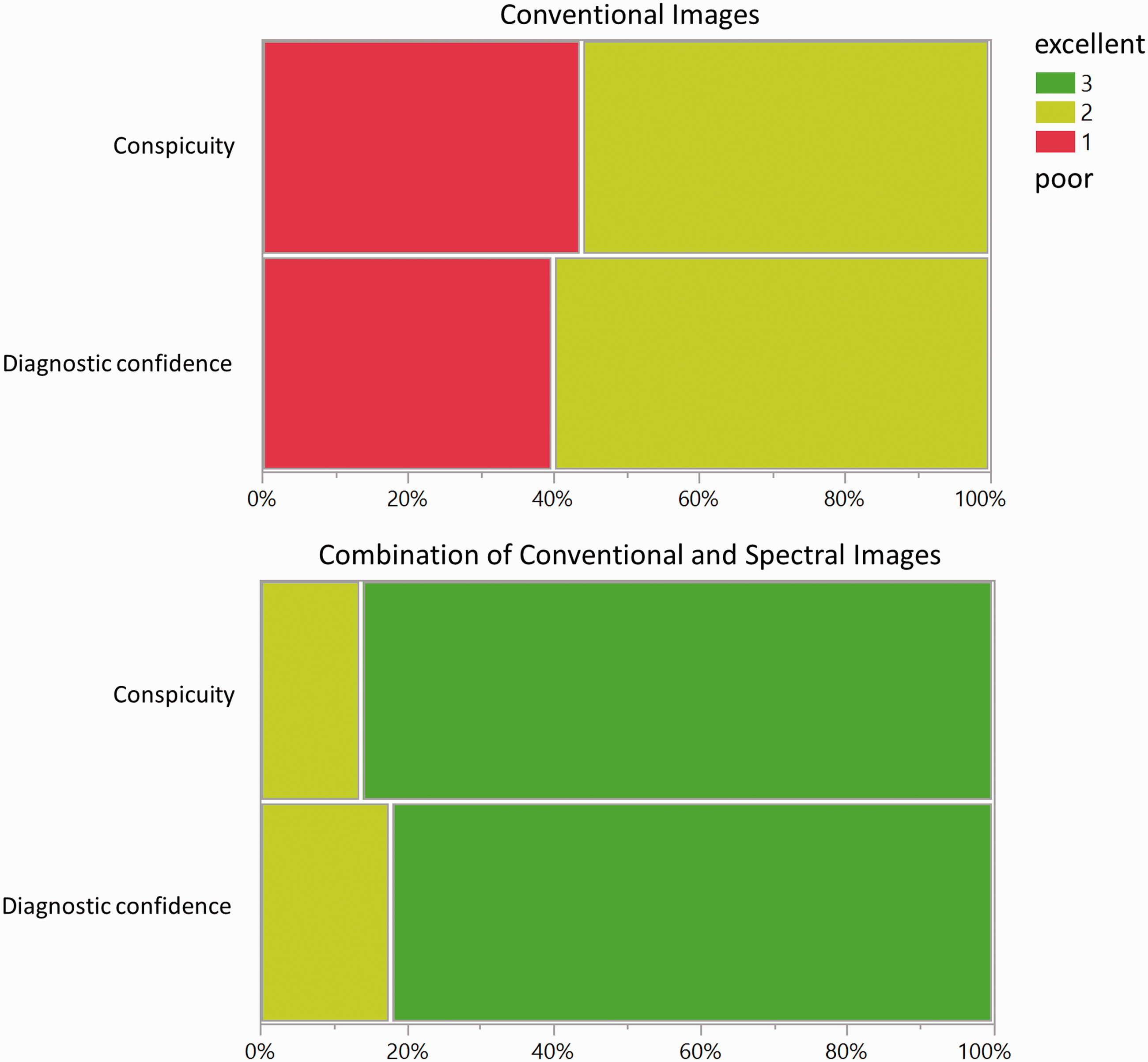
Images show subjective assessment of cystic pancreatic lesions. Substantial shift to higher scores in lesion conspicuity (1 = poor lesion delineation with insufficient contrast to adjacent tissue, 2 = intermediate lesion delineation with moderate contrast to adjacent tissue. 3 = excellent lesion delineation with strong contrast to adjacent tissue) and diagnostic confidence (1 = unclear lesion and internal content, 2 = equivocal lesion and moderate probability for fluid content as well as cystic nature, 3 = clear cystic nature and fluid internal content) occur when the combination of conventional and spectral images (virtual monoenergetic images at 40 keV, iodine density, and iodine overlay images) is provided.
Subjective reading.
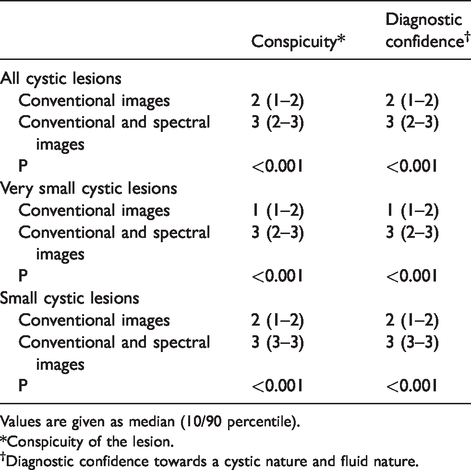
Values are given as median (10/90 percentile).
*Conspicuity of the lesion.
†Diagnostic confidence towards a cystic nature and fluid nature.
The combination of conventional images with spectral images significantly improved diagnostic confidence for presence of pure cystic nature and fluid internal content (mean score 3 [2–3]; Fig. 1, Table 3), diagnostic confidence was high and most lesions were rated as clear cystic lesions and fluid internal content, whereas if just conventional images were used diagnostic confidence was limited and most lesions were rated as equivocal lesions with moderate probability for fluid content and cystic nature (mean score 2 [1–2]; Fig. 1, Table 3).
However, very small lesions showed significantly worse diagnostic confidence than small-sized lesions, for both evaluation from conventional images (P = 0.016) and evaluation of conventional in combination with spectral images (P = 0.003; Table 3).
Confirming the referring radiological reports, both readers recommended additional short-term imaging to confirm cystic nature and differentiate them from suspicious hypodense potentially malignant lesions in all lesions due to poor visualization when only conventional images were used. The combination with spectral images added confidence towards cystic nature in most patients. Therefore, subjective readers only advised for additional immediate imaging in 18% of the cases, so that most patients could have directly entered dedicated long-term follow-up schemes, according to their lesion appearance, size, and risk factors (Figs. 2 and 3) (1,2).
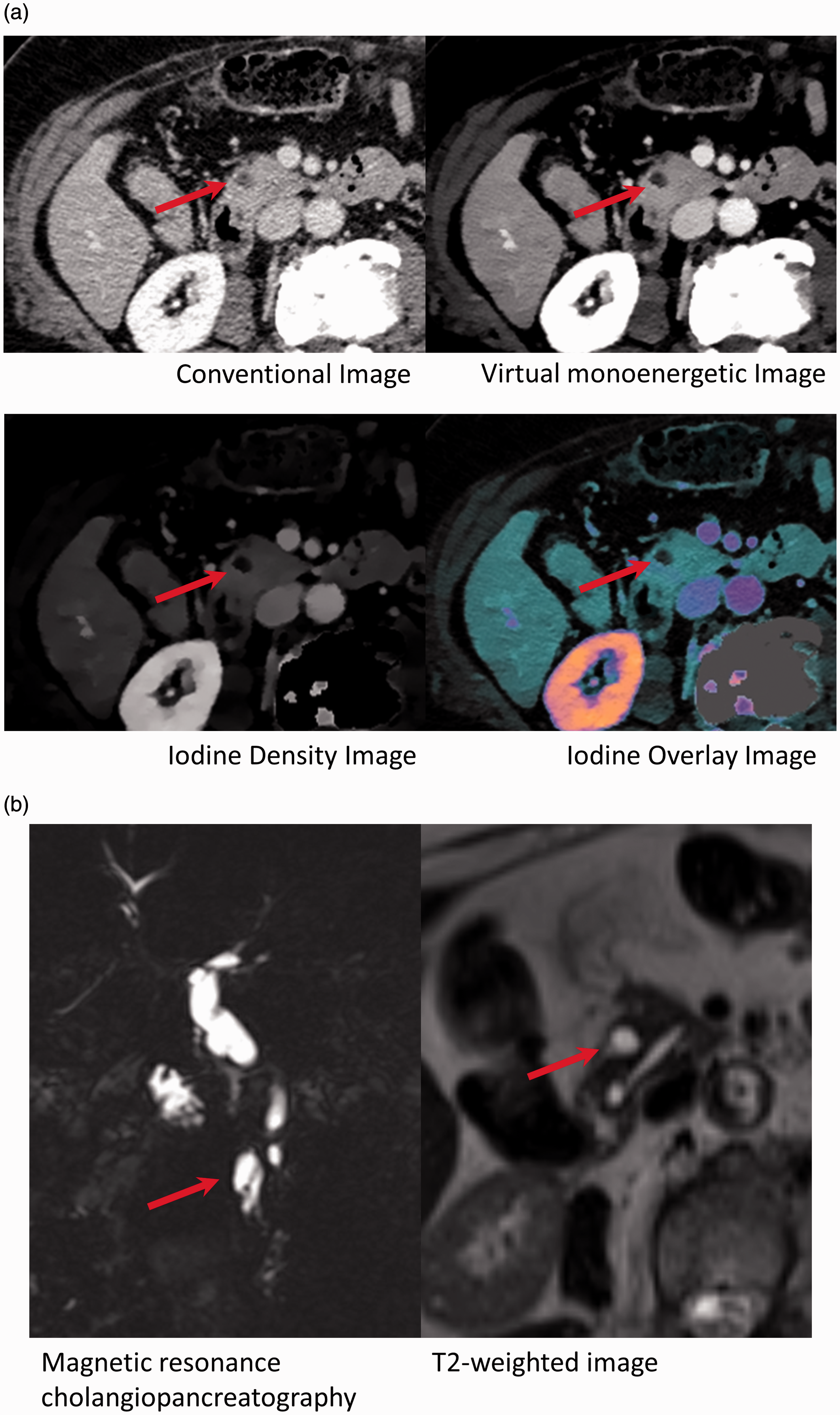
(a) Axial CT images of the upper abdomen in an 88-year-old female patient with unclear renal lesions receiving a contrast enhanced portal venous phase SDCT examination. Depicted are conventional, 40 keV virtual monoenergetic, iodine density and iodine overlay images. In the conventional image, a hypodense lesion can be detected at the junction of pancreas head and neck. The combination with spectral images helps to delineate the lesion more accurately as lesion-to-parenchyma contrast increases and helps to identify the lesion as cystic with fluid content. Both subjective readers did not recommend immediate additional imaging to clarify/confirm low-risk cystic nature when the spectral images were provided indicating the patient could have directly entered dedicated long-term follow-up scheme. (b) Dedicated follow-up MRI was performed five months later in which the lesion has been diagnosed as a side branch IPMN of the pancreas head. IPMN, intraductal papillary mucosal neoplasm; MRI, magnetic resonance imaging; SDCT, spectral-detector computed tomography.
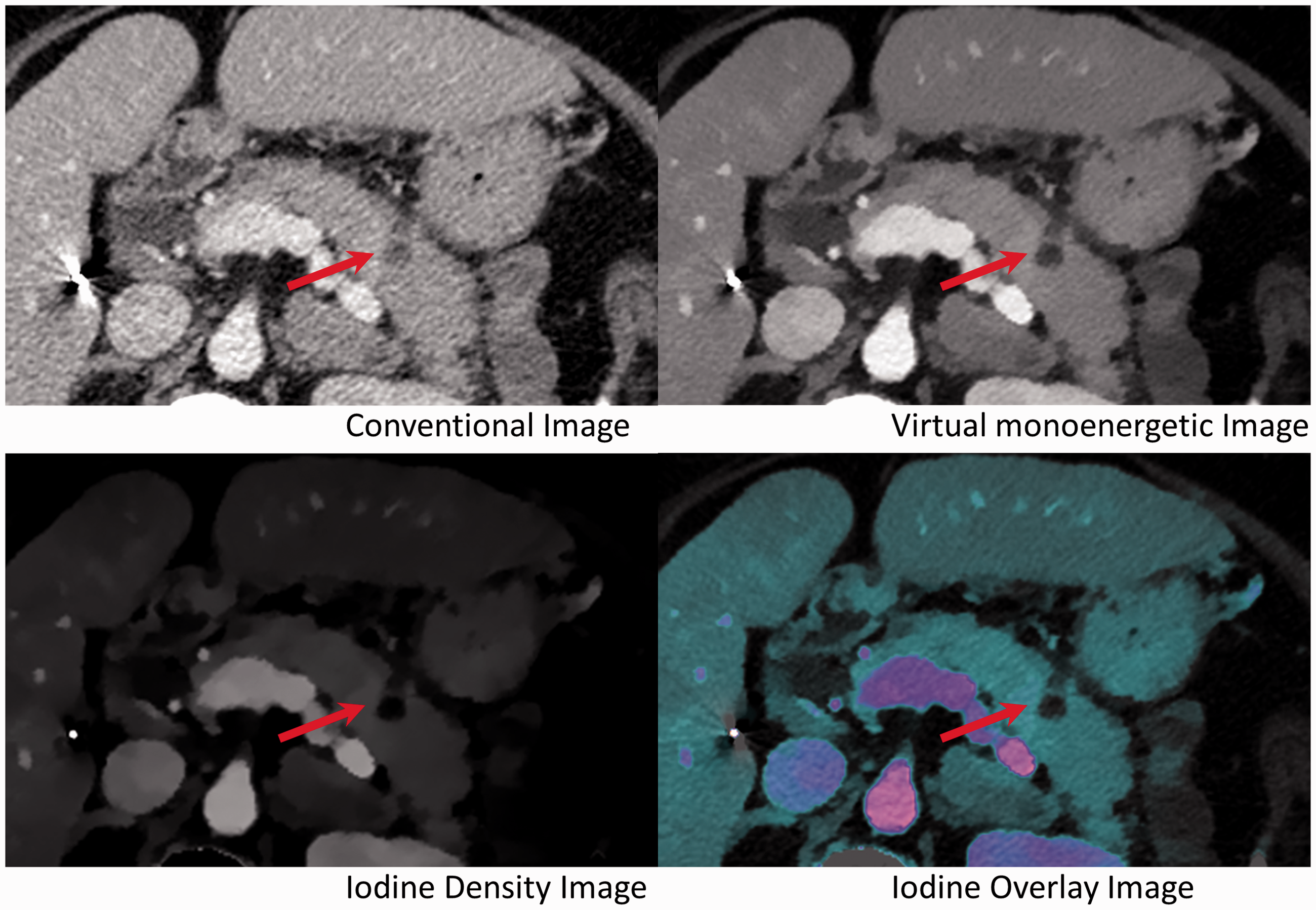
Axial CT images of the upper abdomen in a 63-year-old female patient with breast cancer receiving a contrast-enhanced portal venous phase SDCT examination. Depicted are conventional, 40-keV virtual monoenergetic, iodine density, and iodine overlay images. In the conventional image, a hypodense lesion in the pancreas distal body/tail can be detected with a questionable septation. Due to improved visualization and conspicuity, the septation can be seen much more clearly in the spectral images. Because of the now clear septation, both readers still evaluated this lesion as equivocal and recommended additional short-term imaging, before the patient could potentially enter dedicated long-term follow-up scheme. However, recommended short-term follow-up scan was not performed in this patient and no later imaging of this patient was available. SDCT, spectral-detector computed tomography.
Inter-observer agreement improved considerably, shown by increasing values for ICC from fair (0.51) for conventional images to excellent (0.85) when the combination with spectral images was employed.
Objective assessment
Attenuation was lower in cystic lesions (19.9 ± 11.7 HU) compared to the surrounding pancreas parenchyma in the portal venous phase (86.3 ± 13.9 HU, P < 0.001; Fig. 4, Table 4). Attenuation significantly increased in VMI at 40 keV in pancreas parenchyma (202.0 ± 41.8, P < 0.001) and pancreatic lesions (65.7 ± 33.9 HU, P < 0.001; Fig. 4 and Table 4); however, this trend was considerably stronger in the pancreas parenchyma. Image noise depicted by SD of attenuation was on the other hand comparable in CI and VMI at 40 keV in pancreas parenchyma, cystic lesions, and subcutaneous fat (P > 0.05; Table 4). Due to stronger increase in attenuation than image noise, SNR of the pancreas parenchyma and lesion significantly improved (both P < 0.001; Fig. 4, Table 4). Lesion-to-parenchyma CNR also significantly improved in VMI at 40 keV (P = 0.002; Fig. 4, Table 4), supplementing the improved conspicuity demonstrated in the subjective reading when spectral images were used.
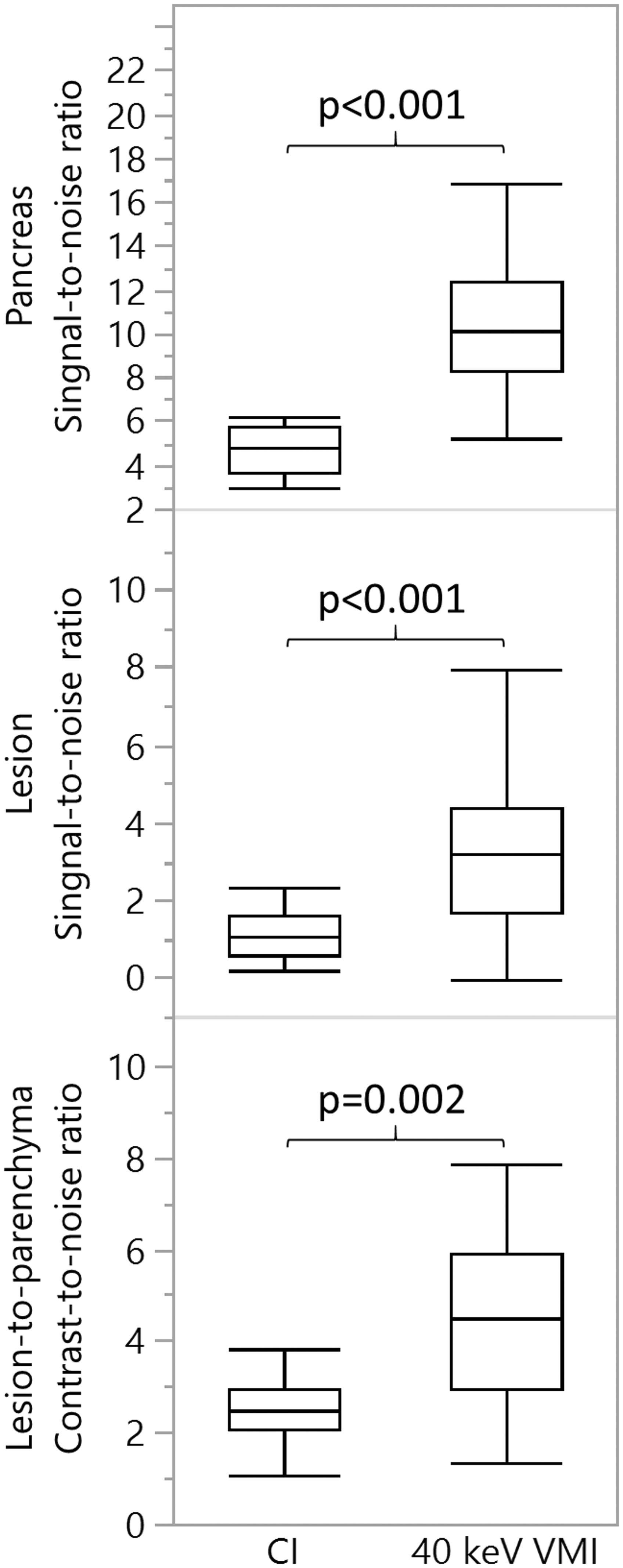
Box plot diagram displaying SNR in pancreas and cystic pancreatic lesions and lesion-to-parenchyma CNR for CIs and 40 keV VMI. Image quality metrics significantly improved in 40 keV VMI. CI, conventional image; CNR, contrast-to-noise ratio; SNR, signal-to-noise ratio; VMI, virtual monoenergetic image.
Objective image analysis.
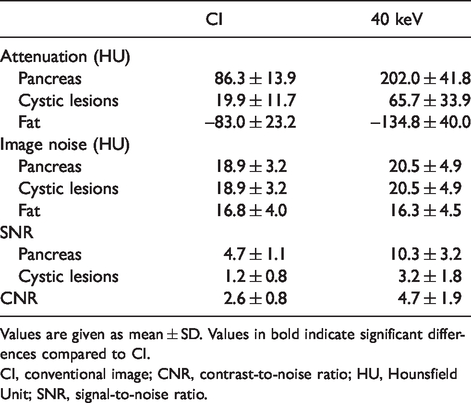
Values are given as mean ± SD. Values in bold indicate significant differences compared to CI.
CI, conventional image; CNR, contrast-to-noise ratio; HU, Hounsfield Unit; SNR, signal-to-noise ratio.
Discussion
The present study investigated the application of SDCT for evaluation of equivocal small cystic lesions of the pancreas. Qualitatively, lesion conspicuity and diagnostic confidence improved significantly when both conventional and spectral images were used compared to conventional CT images only. These subjective findings were consistent with the results of the quantitative image assessment which revealed an increased lesion-to-parenchyma contrast in low-keV VMI.
In 2012, Chu et al. (15) showed on a dual-source scanner in 19 cystic pancreatic lesions that iodine density can help to establish presence of cystic nature. In 2014 and 2016, Lin et al. (22) and Li et al. (20) presented promising data that additional spectral imaging data could help to differentiate serous oligocystic adenoma and mucinous cystic neoplasm. Both studies were conducted using rapid kilovoltage-switching scanners. For cystic lesions of the kidneys, recent large-scale studies have shown that characterization of cystic renal lesions improves by employing iodine density and iodine overlay images allowing for better differentiation from malign neoplasms (23,24). In the present study, the application of spectral CT to a group of small equivocal cystic lesions proved valuable: the combination of conventional images with spectral images significantly improved conspicuity and diagnostic confidence regarding the cystic character and fluid content. Moreover, in the subjective assessment, iodine density and iodine overlay series supplemented CI and provided additional information regarding missing or minor iodine of cystic lesions compared to surrounding pancreas parenchyma.
In small cystic lesions ≤2 cm, both single-energy and DECT struggle with exact depiction of attenuation and quantification of iodine content due to pseudoenhancement, which can result in an artificial increase of attenuation and, additionally for DECT, an overestimation of iodine content especially at low keV reconstructions (25–27). This is true for all DECT solutions despite their differences in technical specifications (25,27). Pseudoenhancement is caused by inadequate correction for beam hardening, which has most commonly been reported for renal cystic lesions (25,27). This increase of attenuation was also encountered at lower keV VMI in our study population (25). Still, the objective analysis showed significantly better SNR of pancreas and cystic lesions as well as improved lesion-to-parenchyma CNR. Attenuation of iodine increases at decreasing energy levels; therefore, at 40 keV VMI, iodine concentration differences are accentuated. This improves lesion discrimination from its surrounding tissue as iodine concentration in pancreas parenchyma is relatively high at portal venous phase (10,28,29). In hypodense liver lesions, a recent study showed that low keV VMI yield improved visualization and lesion-to-parenchyma contrast that differed strongly between hypodense metastases and cystic lesions, potentially allowing for better discrimination of these two lesion types (29). Low keV VMI were also used for better conspicuity and lesion-to-parenchyma CNR of ductal pancreatic adenocarcinoma (17,18). Further, a study conducted on a dual-source scanner showed in seven cystic pancreatic lesions that low-keV VMI improved image quality and were preferred by readers (19). Better conspicuity and higher image quality could improve detection of small cystic pancreatic lesion. This is relevant as incidences of pancreatic lesion in CT imaging are lower compared to magnetic resonance imaging, which is generally regarded superior for lesion visualization (3,30).
In our analysis, we could confirm that diagnostic confidence is dependent on lesion size (2): very small lesions (≤10 mm) showed significantly worse conspicuity and diagnostic confidence compared to small lesions (>10 mm to ≤15 mm). Although conspicuity and diagnostic confidence significantly improved when the conventional images were combined with spectral images, very small lesions still received significantly lower scores, which needs to be regarded as a limitation of this approach.
For clinical decision making, certainty of diagnosis is an important aspect. The inter-reader agreement, depicted by the ICC, increased between the two readers when conventional plus spectral images were used for both lesion conspicuity and confidence for cystic nature. Further, the subjective evaluation demonstrated that immediate additional imaging was needed less often to confirm cystic nature when the combination with SI was used. In clinical routine, this could help to better and earlier differentiate low risk small cystic pancreatic lesion from high risk hypodense lesions (e.g. pancreatic ductal adenocarcinoma or pancreatic metastases) (2,5). Ideally, patients could then faster and directly enter dedicated follow-up schemes for cystic pancreatic lesions (1,2) or when malignancy is suspected additional diagnostic measures and/or treatment could potentially be initiated earlier and with more confidence (2,5).
The following limitations to this study need to be considered. First, we conducted the patient selection based on the radiological report, so we did not evaluate if spectral information increases detection rate of small cystic pancreatic lesions. Second, no histopathologic ground-truth information on the cystic pancreatic lesions was available as cystic pancreatic lesions are not biopsied or resected on a regular basis. Third, we did not include any clearly malignant pancreatic lesions such as ductal pancreatic adenocarcinoma or pancreatic metastases. However, the in-vivo characterization of these small pancreatic lesions was beyond the purpose of this study which focused on the confident visualization of small pure cystic pancreatic lesions with a high unlikelihood of pancreatic cancer. In addition, our patient cohort was relatively small due to the focus on a specific lesion size and type. Lastly, although we evaluated the impact of the combination of conventional with spectral images for necessity of additional short-term imaging for clarification, our study design was retrospective and we could not assess the real impact on clinical decision making.
In conclusion, compared to conventional CT alone, the combination with spectral image information from SDCT significantly improved visualization and diagnostic confidence for evaluation of small equivocal cystic pancreatic lesions.
Footnotes
Acknowledgements
The authors thank Sandra Halliburton for reviewing the manuscript and her technical advice.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NGH received speakers’ honoraria from Philips Healthcare.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by Philips Healthcare under a research agreement with University Hospitals Cleveland Medical Center and Case Western Reserve University.