
Abstract
Background
Although the pathophysiology of white matter hyperintensities remains unclear, we can recently explore the possible relationship with white matter hyperintensities by using quantitative parameter.
Purpose
To demonstrate the relationship between bilateral distal internal carotid arterial tortuosity and total brain white matter hyperintensities volume in elderly individuals.
Material and Methods
A total of 345 patients (age > 65 years) with brain magnetic resonance (MR) examinations were retrospectively included (44.1% men; mean age = 72.1 ± 6.25 years; 55.9% ≥ 70 years). We measured the Tortuosity Index (TI) of the bilateral distal internal carotid artery and basilar artery on MR angiography imaging, and white matter hyperintensities volume on fluid-attenuated inversion recovery MR sequence. Multiple linear regression was used to assess the association of the TI with quantitatively derived brain white matter hyperintensity volume, after adjusting for demographics (age, sex), vascular risk factors (hypertension, diabetes, heart disease), and vessel diameters, total intracranial volume (TIV).
Results
Increased tortuosity of bilateral distal internal carotid artery was associated with greater burden of white matter hyperintensity volume (right: β = 11.223, P = 0.016; left: β = 20.701, P < 0.001). This relationship was independent of age and hypertension, both of which have been considered the strongest risk factors for white matter hyperintensities.
Conclusion
Our results suggest that tortuosity of the bilateral distal internal carotid artery is associated with white matter hyperintensities, independent of age and hypertension.
Introduction
Brain white matter hyperintensities (WMHs) are lesions detected incidentally on cerebral white matter, which are characterized by their bright appearance on T2-weighted (T2W) magnetic resonance imaging (MRI) sequences (1,2). These abnormalities are often found in health elderly adults (3) and clinically related to various suboptimal health conditions, including dementia, stroke, cognitive decline, and increased mortality (4–8). The strongest risk factors for white matter hyperintensities are hypertension and advanced age (9–11); other risk factors—including some genetic factors, homocysteine, and use of tobacco—are also shared (12–14). Postmortem pathologic studies that compared WMHs on brain MRI found that those areas represented ischemic tissue rarefaction with myelin and axons loss, or a varying degree of gliosis (1). WMHs are suggested to reflect cerebral small-vessel disease (CSVD) (15,16), a neurological term describing a series of clinical syndrome caused by brain small vessels damage, which is usually found in normal elderly adults (17,18), although the real pathophysiology of WMHs largely remains unknown.
Recently, some researchers (19–24) suggested that large carotid artery properties (stiffness, diameters, intima-media thickness, stenosis, calcification) were associated with greater burden of WMHs. Few of them investigated the association between large arterial tortuosity and WMHs. Arterial tortuosity indicates the existence of distorted arteries (25). Some studies suggested that arterial tortuosity may be a useful indicator of atherosclerosis, while other researchers considered it as a risk factor resulting in atherosclerosis (26–28).
The volume of WMHs could be quantified with the development of automated and semi-automated software (29). Based on the hypothesis that increased tortuosity of the bilateral distal internal carotid artery (ICA) would be associated with greater volume of WMHs, the aim of the present study was to demonstrate the association between bilateral distal ICA tortuosity and total brain WMH volume in elderly individuals.
Material and Methods
Patients
This retrospective study was approved by our institutional review board, and written informed consent was waived because of the retrospective nature of the study. All patients (aged > 65years) in whom magnetic resonance angiography (MRA) of the brain and routine MRI examinations (T1, T2, fluid-attenuated inversion-recovery T2-weighted [T2-FLAIR]) were performed between 1 January 2018 and 31 December 2018 in our hospital were eligible. All brain MRA and routine MRI examinations were performed within three months. Exclusion criteria were as follows: (i) MRI examinations had substantial motion artifacts; (ii) had traumatic brain injury or congenital cerebral malformation; (iii) had acute strokes confirmed by clinical history; and (iv) concomitant pathologies including hemorrhage, cerebral space occupying lesions, brain arteriovenous malformations, etc.
The process of patient selection is presented in Fig. 1. We gathered patients’ demographic data, including sex, diagnosis, and age from the electronic medical records. Vascular risk history, such as diabetes, heart disease, and hypertension, was acquired by means of chart review, self-reported patient interviews, and clinical records. We established each vascular risk factor based on a diagnostic history or documentation of treatment for the condition.

Flow chart of the study.
MRI technique
All MR examinations of the brain were imaged at our institution by using a 1.5-T MR scanner (GE 1.5T Signa HDxt, Boston, Massachusetts, USA), including: axial 3D fast spoiled gradient-echo T1-weighted (T1W) sequence, fast spin-echo T2-weighted (T2W) imaging, T2-FLAIR, and 3D time-of-flight magnetic resonance angiography (3D TOF MRA). Imaging protocols parameters appear in Table 1.
MRI protocol parameters using the GE 1.5-T Signa HDxt scanner.
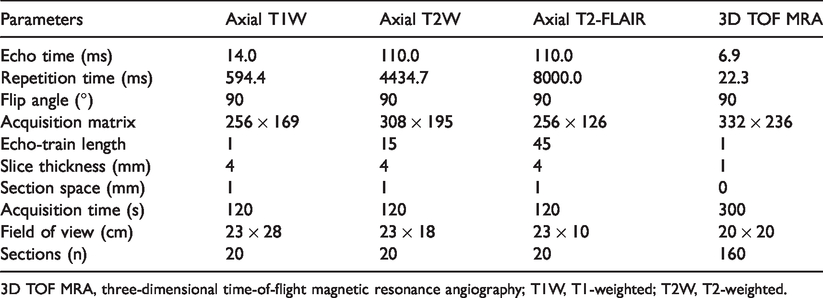
3D TOF MRA, three-dimensional time-of-flight magnetic resonance angiography; T1W, T1-weighted; T2W, T2-weighted.
Measurement of WMH volume
Analyses were performed using a seed-growing method of fuzzy connectivity based on the images’ intensity characteristics on a commercial segmentation tool (Jim, Xinapse System, Leicester, UK). The algorithms used by the tool were based on a relative fuzzy connectedness theory published before (30).
Axial T2-FLAIR images were quantified for WMH volume by one experienced neuroradiologist (Doctor A) who was blinded to patients’ information. Preprocessing steps included intensity inhomogeneity correction, noise reduction, and intensity normalization. All patients were roughly classified as minimal group, moderate group, or severe group depending on the burden of WMH volume by visual check (Fig. 2). Then, all WMH regions in three patients, randomly selected from respective groups, were manually delineated as seed regions for each group. Large vessel infarcts and asymptomatic cerebral lacunar infarctions were visually identified and removed from the WMHs. Next, fuzzy thresholds were decided for different groups by experimenting with 10 patients, randomly selected from respective groups. The minimal group was 0.67, the moderate group was 0.63, and the severe group was 0.60. Images were then entered into the tool; the algorithm grew the seed regions based on the fuzzy affinity between pixels and their neighbors. The fuzzy threshold setting determined a cut-off fuzzy connectedness such that all pixels above the threshold were considered part of the feature. The algorithm would create regions of interest surrounding the fuzzy-connected features that it had found (31). Another consultant neuroradiologist (Doctor B), with 20 years of experience in neuroradiology, then visually checked all labeled WMHs areas for errors, and corrections were made by the consent of them. After that, the software automatically calculated the WMH volume in cubic centimeters for total brain WMH volume, depending on delineated WMH areas and the slice thickness. We decided to maintain the original scale of WMH volume, because log transforming of them had little effect on our analysis. Total intracranial volume (TIV) was derived from the T1 sequence using the same tool.
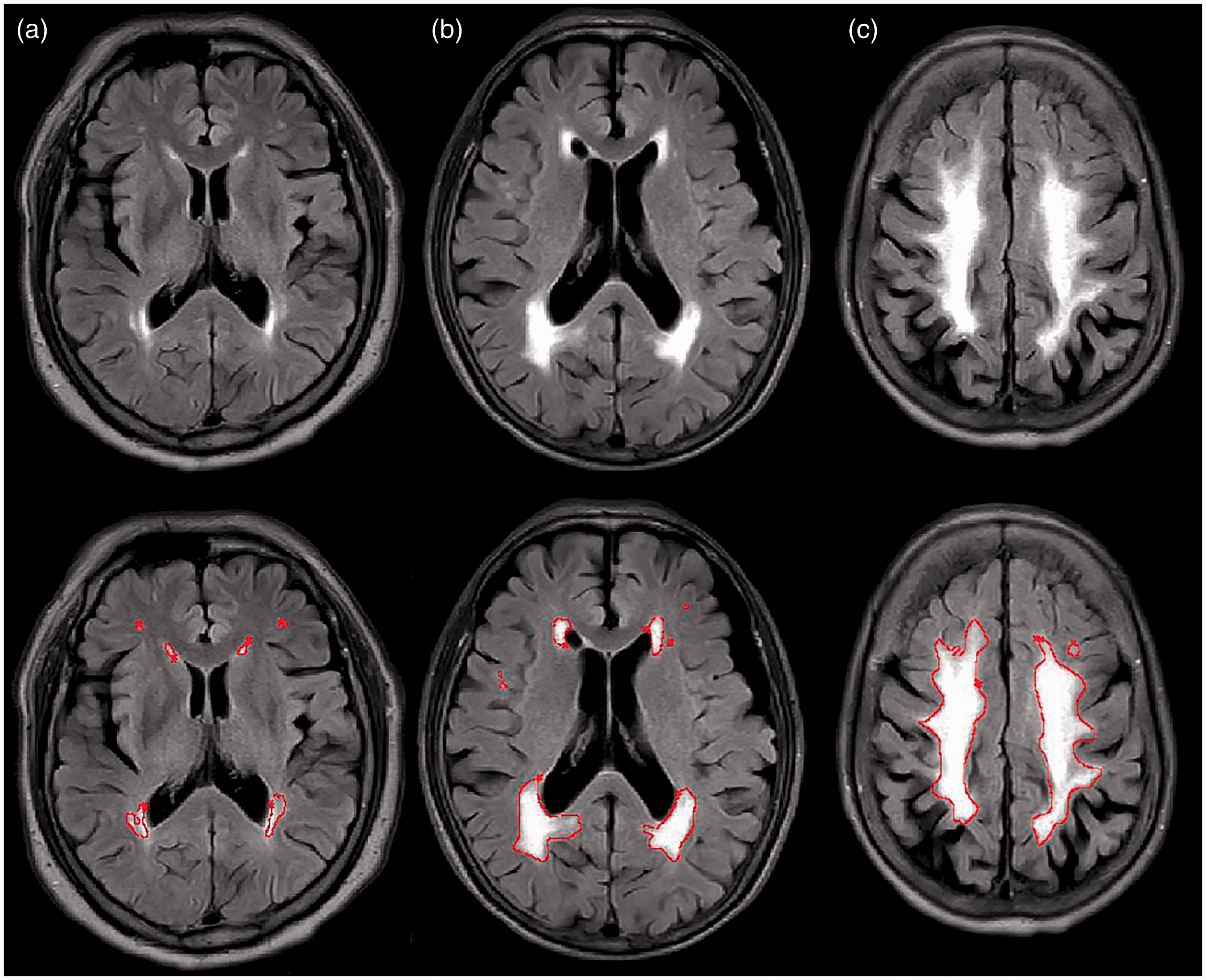
Three sample images of WMHs on T2-FLAIR, labeled for quantification using a semi-automated segmentation tool. (a) Minimal WMHs. (b) Moderate WMHs. (c) Severe WMHs. WMH, white matter hypertensity.
Measurement of arterial tortuosity
We used the Tortuosity Index (TI), or Distance Factor Metric, which was defined as the percent ratio of calculated line distance between two endpoints divided by actual vessel curve length considered (25), to describe arterial tortuosity. Tortuosity of the basilar artery (BA) and bilateral distal ICA were measured manually using commercially available software (Materialise Mimics Inovation Suite 21.0 Medical/Research). The raw images utilized in our study were acquired from 3D TOF MRA. Briefly, postprocessing of source images involved five steps: (i) two endpoints were determined; (ii) vessel segment; (iii) reconstructed to volume rendering (VR) images without any smoothing methods employed; (iv) centerline extraction of the targeted arteries; and (v) automatically calculated TI (Fig. 3). More details for step1 should be mentioned: the third trained neuroradiologist (Doctor C), who was blinded to the patients’ information, independently defined segments of the vessel by respectively designating two points for the distal and proximal ends of the BA and ICA. The origin of BA was defined as the confluence point of bilateral vertebral artery (VA), and the termination end was the point where it bifurcated into the posterior cerebral arteries. For ICA (Bouthillier Classification), we extracted the initial horizontal portion of C2 segment to distal C7 segment as the targeted course (32). The average diameters of the targeted BA and ICA were also calculated using its three measurements, 2 mm from each end and in the middle.

Illustration of the left distal ICA tracking, centerline extraction, and tortuosity descriptor calculation. TI was defined as the percent ratio of calculated line distance between two endpoints (L2) divided by actual vessel curve length considered (L1). The arrows indicated the starting point of the targeted ICA course (the initial horizontal portion of C2 segment). ICA, internal carotid artery; TI, Tortuosity Index.
Statistical analyses
Data were presented as frequencies with percentages for categorical variables and mean with standard deviation (SD) for continuous variables. We predetermined the statistical analysis plan before data analyses. We used a t-test to evaluate the average differences in TI and WMH volume for each categorical covariate. In this univariate analyses, we also transformed WHM burden and age (continuous variables) into categorical variables, stratified the WHM burden into two strata—≥ median value (high burden) and < median value (low burden)—as well as the age—≥ 70 years and < 70 years. This age cut-off was close to the mean of the age distribution in our study. We set total brain WMH volume as the dependent continuous variable and entered the TI of bilateral distal ICA and BA as the independent variable. Linear regression was then performed to assess the relationship between TI and WMH volume with four sequential models. First, we evaluated the association without adjusting for any other factors in model 1, and then additionally controlled for sex and age (≥ 70 vs. < 70 years) in model 2. We further added hypertension, diabetes, and heart disease in model 3. Finally, we adjusted for vessel diameters and total intracranial volume in model 4. The inter-observer reproducibility of the TI measurement was assessed using 50 patients who were randomly selected; these patients were then evaluated by the fourth experienced neuroradiologist (Doctor D), who was blinded to the patients’ information. The third neuroradiologist (Doctor C) mentioned before also re-evaluated these 50 patients for the assessment of intra-observer reproducibility. Intraclass correlation coefficients (ICCs) were calculated. ICCs > 0.75, 0.60–0.74, 0.40–0.59, and < 0.40 indicated excellent, good, fair, and poor reproducibility, respectively. Statistical analyses were performed by Doctor E, with four years of experience in statistical analysis using SPSS (version 25; IBM, Armonk, NY, USA). We considered a P value < 0.05 as statistically significant for all analyses.
Results
Patient sample characteristics
A total of 643 consecutive patients (age > 65 years) with brain MRI examination between 1 January 2018 and 31 December 2018 in our hospital were included in this study. After excluding patients who did not meet the study criteria, 345 patients were finally included in our analysis (Fig. 1). The characteristics of the patients are showed in Table 2. In brief, the mean age was 72.1 ± 6.25 years with 51.0% ≥ 70 years, and 44.1% of the patients were male. The mean total brain WMH volume was 7.75 ± 7.00 mL and the median value was 6.9 mL. The mean TI of the BA, right distal ICA, and left distal ICA, was 0.067 ± 0.049, 0.419 ± 0.075, and 0.421 ± 0.079, respectively.
Characteristics of the 345 patients and values for measured diameters, TI and WMH volume.
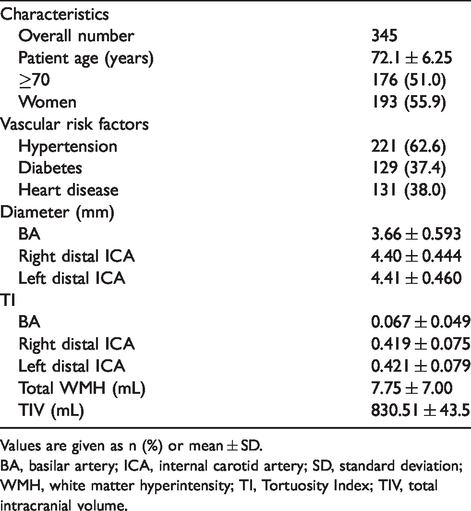
Values are given as n (%) or mean ± SD.
BA, basilar artery; ICA, internal carotid artery; SD, standard deviation; WMH, white matter hyperintensity; TI, Tortuosity Index; TIV, total intracranial volume.
Inter- and intra-observer reproducibility
The inter-observer reproducibility was excellent for the TI of the BA (ICC = 0.975; 95% confidence interval [CI] = 0.956–0.986) and good for the TI of the right distal ICA (ICC = 0.625; 95% CI = 0.421–0.768) and the left distal ICA (ICC = 0.688; 95% CI = 0.509–0.810). The intra-observer reproducibility was excellent for the TI of the BA (ICC = 0.946; 95% CI = 0.906–0.969) and good for the TI of the right distal ICA (ICC = 0.662; 95% CI = 0.473–0.793) and left distal ICA (ICC = 0.676; 95% CI = 04921–0.802) .
Relationship between TI and total brain WMH volume
In univariate analyses, the burden of WMHs stratified by a threshold of median value (6.9 mL) was associated with the TI of the bilateral distal ICA. Age was significantly associated with total brain WMH volume and TI of the BA. Sex was associated with total brain WMH volume and the TI of the left distal ICA. Hypertension was only associated with total brain WMH volume (Table 3).
The mean differences in TI and WMH volume sorted by each categorical covariate.
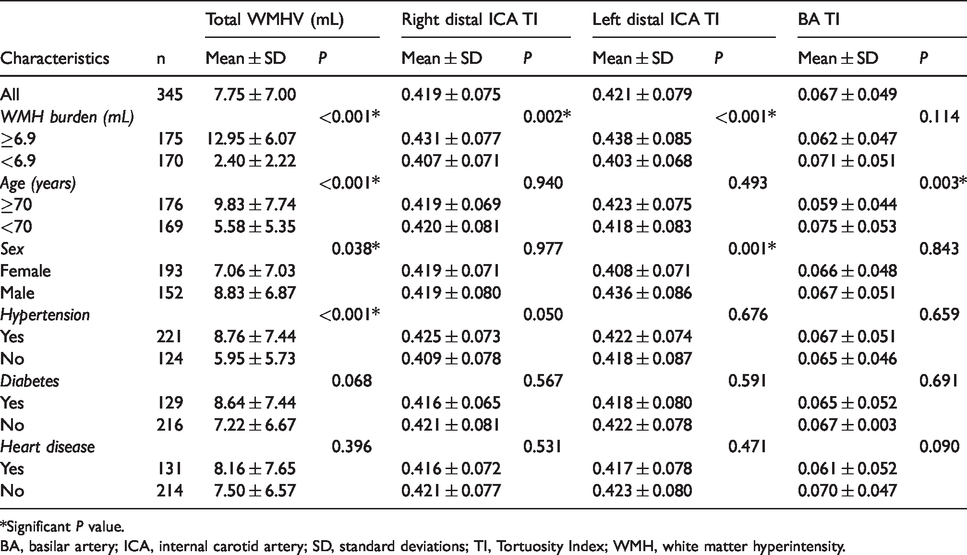
*Significant P value.
BA, basilar artery; ICA, internal carotid artery; SD, standard deviations; TI, Tortuosity Index; WMH, white matter hyperintensity.
In the unadjusted linear regression model, increased TIs of the bilateral distal ICA (right: β = 11.770, P = 0.016; left: β = 21.827, P < 0.001) were associated with greater total brain WMH volume. When we added age and sex in model 2 (right: β = 12.346, P = 0.008; left: β = 19.556, P < 0.001), additionally controlled for hypertension, diabetes, and heart disease in model 3 (right: β = 11.065, P = 0.017; left: β = 20.017, P < 0.001), further adjusted artery diameters and total intracranial volume in model 4 (right: β = 11.223, P = 0.016; left: β = 20.701, P < 0.001), the association between the TI of the bilateral distal ICA and total brain WMH volume did not significantly change. The TI of the BA was not associated with total brain WMH volume in any of our analyses (Table 4).
Association between TI and total WMH volume.
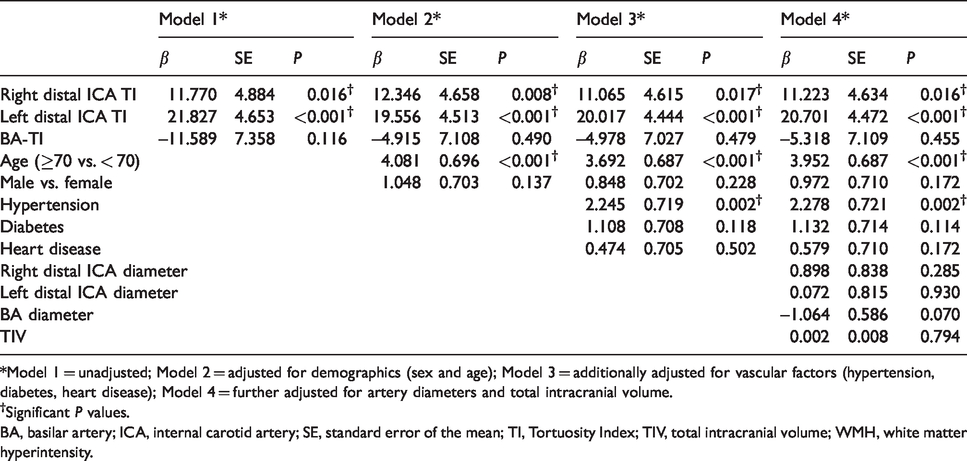
*Model 1 = unadjusted; Model 2 = adjusted for demographics (sex and age); Model 3 = additionally adjusted for vascular factors (hypertension, diabetes, heart disease); Model 4 = further adjusted for artery diameters and total intracranial volume.
†Significant P values.
BA, basilar artery; ICA, internal carotid artery; SE, standard error of the mean; TI, Tortuosity Index; TIV, total intracranial volume; WMH, white matter hyperintensity.
Age was strongly associated with total brain WMH volume in all models (P < 0.001 for all three models). In fully adjusted model 4, hypertension (P = 0.002) was significantly associated with total brain WMH volume (Table 4).
Discussion
In the present study of elderly people, we reported a strong association between the TI of bilateral distal internal carotid artery and total brain WMH volume. This relationship was independent of age and hypertension, both of which have been considered as the strongest risk factors for WMHs. Advancing age and hypertension were associated with loss of elasticity in the large arteries and muscular arterioles and increased arterial stiffness, which could lead to excessive transmission of blood pressure pulsation to the brain, damaging the small vessel wall, and finally manifesting as WMHs (9–11). Our findings might shed new light on the pathophysiology of WMHs besides advancing age and hypertension.
Our study built on previous studies that suggested an association between arterial properties (disease) at different locations and WMHs. In the Framinghan Heart Study, descending thoracic aortic plaque burden was associated WMH volume in men (33). The Rotterdam Scan Study reported a strong relationship between abdominal aortic atherosclerosis and the existence of WMHs (34). Similar findings were observed in the Second Manifestations of ARTerial disease Study, in which researchers investigated WMH volume among participants concomitant with abdominal aneurysm and peripheral arterial disease (35). Some other studies demonstrated the positive association between carotid arterial properties (disease) and WMH burden, such as carotid arterial calcification (24), stiffness, diameters (23), intima-media thickness (20), and stenosis (22). These studies indicated that WMHs may be a manifestation of something else besides CSVD (36–38); arterial properties (disease), especially in terms of ICA, may also be a maker of WMHs. Arterial tortuosity is a commonly observed angiographic finding that may affect a range of arterial bed, from large artery to small size vessels in almost any organ systems. Weibel and Fields (39) reported that ICA tortuosity had a prevalence of 35% in an angiographic study including 1438 consecutive patients. The causation and promoting factors of tortuous arteries remained largely unknown. However, some studies have showed that mechanical factors played an significant part in vessel tortuosity (40).
We reported that increased tortuosity of the bilateral distal ICA may be associated with greater volume of WMHs. Although there is no similar study reported in the literature, previous studies have demonstrated that proximal ICA tortuosity could led to cerebral vascular deficiencies (41–43). Nevertheless, cerebral abnormalities considered in these studies were not focused on WMHs. The impairment of arterioles was considered to be associated with WMHs in postmortem studies, which suggested that cerebral arteriosclerosis could be a key maker in the pathophysiology of WMHs (44). Arterial tortuosity had a controversial role in the pathophysiology of atherosclerosis, it may be a useful indicator of atherosclerosis, meanwhile it could also be a risk factor resulting in atherosclerosis (26–28). Increased tortuosity of the bilateral distal ICA promotes hemodynamic changes in cerebral blood flow (CBF), including flow resistance, pressure loss, more wall sheer stress (WSS), and secondary flow (45,46). Changes in the tortuosity of the bilateral distal ICA could alter the brain micro-circulation and lead to CBF damage. Low CBF could eventually result in chronic brain hypoxia, a generally accepted risk factor for WMHs. Furthermore, some studies (47,48) showed that the WSS of the carotid was significantly correlated with the presence of WMHs. WSS is a known mediator in atherosclerosis and vascular reactivity (49). Changes in the WSS of the bilateral distal ICA can affect the pulsating wave energy which transmits into the brain micro-circulation (23). The brain micro-circulation is especially susceptible to increased pulsating wave energy that finally results in the impairment of micro-vascular and WMHs (50).
The present study had some limitations. First, the single-center, retrospective design did not allow any conclusion on the possible causal relationship between increased tortuosity of the bilateral distal ICA and greater burden of WMH volume. Second, we derived WMH volume from the FLAIR sequence in a semi-automatic tool with manual intervention required. The FLAIR sequence is prone to losing sensitivity or specificity in line with the different spatial location of the lesion; it can lead to hyperintense artifacts on the FLAIR image. Since human eyes are adept in differentiating WMH regions from noise, manual delineation or correction can avoid false-positive errors to the utmost. Despite the time-consuming process compared to other automatic algorithms, the measurement of WMH volume by semi-automatic tool was considered to perform well (reproducibility and accuracy) (51). In addition, we only chose a simple index (TI) to describe arterial tortuosity for the present study. There is no standardized, universally accepted method to measure and report the tortuosity of arteries. Currently, some methods are used in research or clinical practice with a diversity of models ranging from qualitative to quantitative; they can be mathematically simple to sophisticated. Although complex mathematical approaches, such as sum of angles metric, may more closely describe arterial tortuosity, a simple index can account for most of the variation in tortuosity (52). Moreover, we decided to designate the ICA starting point as the initial horizontal portion of the C2 segment instead of the proximal C2 segment (the entry point of the carotid canal), since it was difficult to identify on MRA images, and the measurement of the TI of the ICA in our analysis demonstrated a good reproducibility.
In conclusion, the present study showed a significant association between the TI of the bilateral distal ICA and total brain WMH volume independent of age or hypertension, and the association may be explained by the fact that increased tortuosity of the bilateral distal ICA might promote hemodynamic changes in CBF.
Footnotes
Acknowledgements
The authors thank Xiongfeng Yu, Lizhen Wei, Meigui Chen, and Wenhan Huang for their assistance with the data collection and valuable discussion.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.