
Abstract
Background
The contribution of the subchondral bone in the development and progression of osteoarthritis (OA) has long been recognized, but its role in cartilage repair procedures has only recently attracted more attention.
Purpose
To explore the correlation between the cartilage repair tissue (RT) and the subchondral bone marrow lesions (BMLs) after matrix-associated autologous chondrocyte implantation (MACI) in the knee joint.
Material and Methods
A total of 30 patients who underwent MACI in the knee from January 2015 to June 2018 and follow-up magnetic resonance imaging (MRI) scan were recruited in this study. The MRI results of cartilage RT were evaluated using T2* relaxation time. Subchondral BMLs were also qualitatively evaluated by use of the two-dimensional proton density-weighted fat-suppressed (2D-PD-FS) and three-dimensional dual-echo steady-state (3D-DESS) sequences.
Results
The univariate analysis displayed a significant negative correlation between subchondral BMLs and cartilage RT (P < 0.01). In the minimally adjusted model (only age, sex, and body mass index [BMI] adjusted), the results did not show obvious changes (β = –6.54, 95% confidence interval [CI] = –10.99 to –2.09; P = 0.008). After adjustment for the full models (age, sex, BMI, defect size, combined injury, and preoperative duration of symptoms adjusted), the connection was also detected (β = –6.66, 95% CI –11.82 to –1.50; P = 0.019).
Conclusion
After MACI, the subchondral BMLs are significantly correlated with cartilage RT-T2* relaxation time. The role of subchondral bone in cartilage repair procedures should not be underestimated.
Introduction
Articular cartilage defects are a common pathology of the knee joint and may accelerate the development of osteoarthritis (OA) (1). Patients with focal cartilage defects may benefit from cartilage repair surgery since it can prevent the progression of early OA in the knee joint (2). Matrix-associated autologous chondrocyte implantation (MACI) has been reported to yield good to excellent clinical and radiological outcomes for larger and full-thickness cartilage lesions (3–7). Magnetic resonance imaging (MRI) has been used to investigate cartilage degeneration and cartilage repair tissue (RT) using the measurement of T2* relaxation time, which was reported to assess collagen content in cartilage (8).
The contribution of the subchondral bone in the development and progression of OA has long been recognized (9), but its role in cartilage repair procedures has only recently attracted more attention (10). Basic experimental studies have reported that complex interplay exists between the articular cartilage RT and its underlying subchondral bone, the more general term “bone marrow lesion” (BML) has become standardized terminology (11). Specific alterations of the subchondral BML associated with cartilage repair have been recently described. These include the following: (i) elevation of subchondral bone plate, defined as elevation of the osteochondral junction into the cartilaginous repair tissue; (ii) formation of intralesional osteophytes, often appears as focal, newly formed bone located apical to the original cement line; (iii) subchondral bone cyst and edema-like signal alterations (10). A comprehensive understanding of the underlying subchondral BMLs is very important. The MRI features of subchondral BMLs are variable: as we know, subchondral bone cyst and edema-like signal alteration were sensitively displayed as a high intensity signal on a two-dimensional (2D) fat-suppressed scan, such as proton density-weighted fat-suppressed (PD-FS). Unfortunately, some changes are often very slight and their visualization remains a problem using 2D conventional sequences, such as the elevation of the subchondral bone plate or the formation of intralesional osteophytes. In clinical investigations, differentiation between elevation of the entire subchondral bone plate and selective, localized formation of intralesional osteophytes is difficult to document. Several authors refer to both phenomena by the term “bony overgrowth” (12,13), which was a common, but important, change associated with cartilage repair procedures, and leaded to a poor prognosis (10). Various three-dimensional (3D) sequences have been developed to improve morphological depiction (14,15). Among them, the isotropic 3D dual-echo steady-state (DESS) sequence provides higher signal-to-noise ratio (SNR) and a clearer bone marrow–cartilage interface. Preferably, a combination of sequences should be used to explore the significance of subchondral BML, also available in routine clinical use.
Knowing that the articular cartilage and the subchondral bone are one closely related functional unit, the aim of the present study was to investigate whether the subchondral BMLs are correlated with the cartilage RT by use of MRI qualitative and quantitative assessment, which then influences the treatment strategies for osteochondral defects.
Material and Methods
Study design, setting, and participants
A total of 63 patients with cartilage defects in the knee who underwent MACI in our institution between January 2015 and June 2018 were selected in the present study. Patients with International Cartilage Repair Society (ICRS) classification III–IV were included in the study. A flow chart of patient selection is shown in Fig. 1.
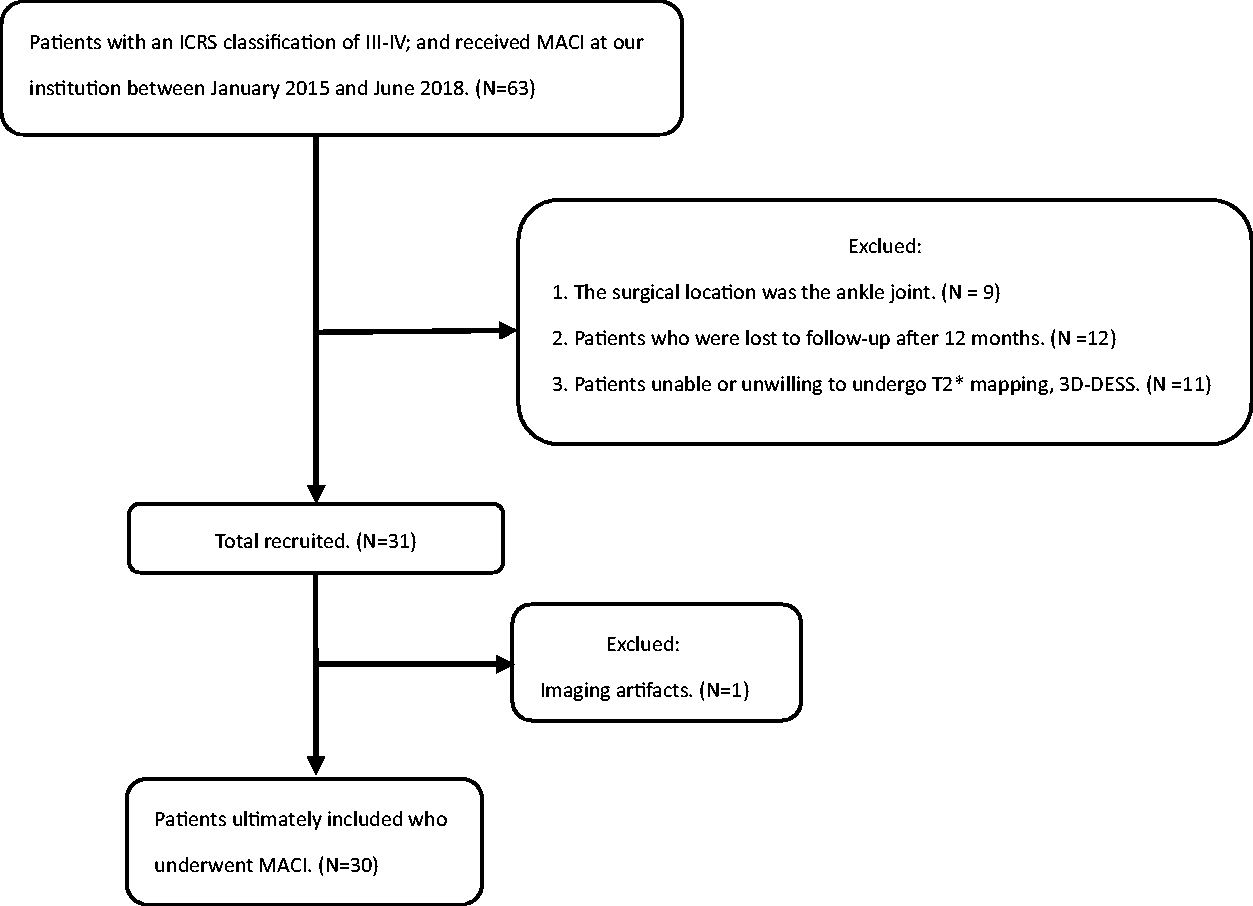
Flow chart illustrating patient selection.
The exclusion criteria were as follows: (i) patients in whom implantation was not performed in the knee; (ii) patients who were lost to follow-up after one year; (iii) patients who were unable or unwilling to undergo the MRI scan; and (iv) the presence of imaging artifacts.
Each patient underwent a single MRI examination, and their height and weight were recorded to calculate body mass index (BMI).
MRI examination
MR images were obtained with a 3.0-T MRI scanner (Siemens Prisma, Erlangen, Germany) with a dedicated 15-channel knee coil. The three MRI scan sequences and orientations were as follows: (i) sagittal PD-FS sequence: TR/TE = 2700/40 ms; field of view (FOV) =160 × 160 mm; matrix size = 256 × 256, slice thickness = 3 mm, slice gap = 0.3 mm, and scan time = 3 min 20s; (ii) sagittal 3D-DESS sequence: TR/TE =15.1/5.11 ms, FOV = 160 × 160 mm, matrix size = 250 × 250, in-plane resolution = 0.6 × 0.6 mm, slice thickness = 0.6 mm, and scan time = 6 min 30 s; and (iii) T2* mapping sequence: the sequence acquired 5 echoes at TE = 4, 11, 18, 26, and 34 ms, respectively, TR = 1010 ms; FOV = 160 × 160 mm; matrix size =256 × 160, slice thickness =3 mm, slice gap = 0.3 mm, and scan time = 6 min 25 s.
Image analysis
All MRI data were independently analyzed by two senior radiologists specializing in musculoskeletal imaging who are unaware of the clinical data. When the opinions on the formation were inconsistent, the two doctors discussed and came to an agreement.
Qualitative MRI analysis of subchondral BML
Morphological MR images (2D-PD-FS and 3D-DESS sequences) were used for the qualitative evaluation of subchondral BMLs, using RadiAnt DICOM Viewer 5.0.1. Subchondral BMLs were defined as a zone of altered signal intensity or morphological changes seen on fat-suppressed sequences in the subchondral bone marrow (16,17). Based on the presence or absence of subchondral BMLs, 30 patients were divided into two groups: the BML group and the intact group.
T2* relaxation time measurements
T2* relaxation times were calculated pixelwise from spin-echo images using a mono-exponential non-negative least squares fit analysis with custom-built software (Syngo Workplace, Siemens). The region of interest (ROI) was drawn manually to cover the full thickness of the cartilage RT by combined sagittal 3D-DESS and 2D-PD-FS sequences, which were considered the optimal sequence combination for the observation of cartilage RT. Regions of healthy control femoral cartilage (HC) in the intra-knee femur were chosen to ensure an equal size when compared with the RT area.
Statistical analysis
All statistical analyses were performed using EmpowerStats (http://www.empowerstats.com) and R (version 3.2.3). For all statistical tests, P < 0.05 was considered statistically significant. Normally distributed variables were expressed as the mean ± SD. The distribution of all data was tested for normality using the Kolmogorov–Smirnov test; for non-normally distributed variables, the results were shown as the median (interquartile range) and non-parametric tests were used.
Inter-reader reproducibility was assessed separately and cartilage RT-T2* relaxation time was assessed in all patients.
For the comparison of T2* relaxation times between the cartilage RT and HC region, and comparison of T2* relaxation times between the BML group and intact group, the Mann–Whitney U test or t-test was used, respectively. A univariate analysis model was used to examine whether subchondral BMLs and other characteristics were correlated with cartilage RT-T2* relaxation time. Next, we performed a multivariate linear regression analysis to assess the correlations between subchondral BMLs and cartilage RT-T2* relaxation time.
Results
Participants
From an initial cohort of 63 patients with an ICRS classification III–IV who underwent MACI at our institution between January 2015 and June 2018, a total of 30 patients (28 men, 2 women; mean age = 31.6 ± 5.84 years; cartilage defect size = 3.0 [range = 2.57–4.20]; mean BMI = 23.74 ± 3.14) were ultimately included in the study (Fig. 1). There were no statistically significant differences in demographic characteristics (age, sex, and BMI) between the two groups (Table 1).
Patient characteristics in the two groups.
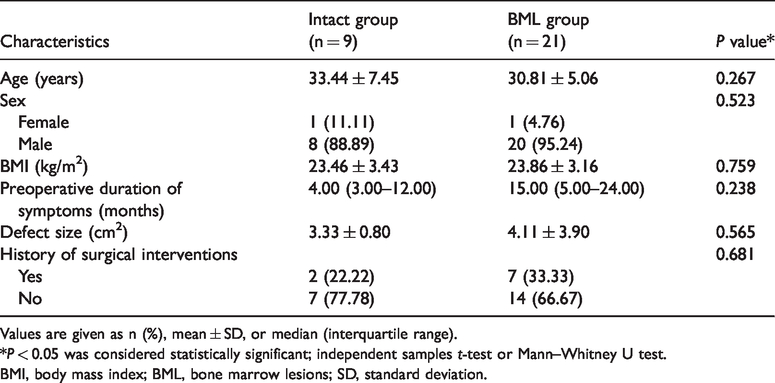
Values are given as n (%), mean ± SD, or median (interquartile range).
*P < 0.05 was considered statistically significant; independent samples t-test or Mann–Whitney U test.
BMI, body mass index; BML, bone marrow lesions; SD, standard deviation.
Eight patients with a history of knee surgery were not excluded: seven patients with a history of anterior cruciate ligament reconstruction, meniscal repair, or both; and one patient with medial patellofemoral ligament reconstruction.
Postoperative evaluation
The inter-observer reliability was very good for measurements of T2* relaxation time, with an intraclass correlation coefficient of 0.987 and 0.952 (P < 0.05).
Among the 30 patients, 21 showed subchondral BMLs. The mean cartilage RT-T2* relaxation time in all patients was significantly lower when compared with the HC of the intra-knee femur (23.02 ± 1.29 ms vs. 34.46 ± 1.30 ms; P < 0.0001) (Fig. 2a); The T2* relaxation time of the cartilage RT was significantly higher in the intact group than that in the BML group (28.70 ± 1.30 ms vs. 21.30 ± 1.72 ms; P = 0.008) (Fig. 2b). The defect size, preoperative duration of symptoms, and history of surgical interventions did not differ between the two groups (Table 1).

Comparison of T2* relaxation time between cartilage RT and HC at intra-knee femur (a). Comparison of T2* relaxation time between the intact group and the BML group (b). BML, bone marrow lesion; HC, healthy control femoral cartilage; RT, repair tissue.
The univariate analysis displayed a significant negative correlation between cartilage RT and subchondral BMLs (β = –6.54, 95% confidence interval [CI] = –11.00 to –2.09; P = 0.008) (Table 2).
Correlations between patient characteristics and cartilage RT metrics.
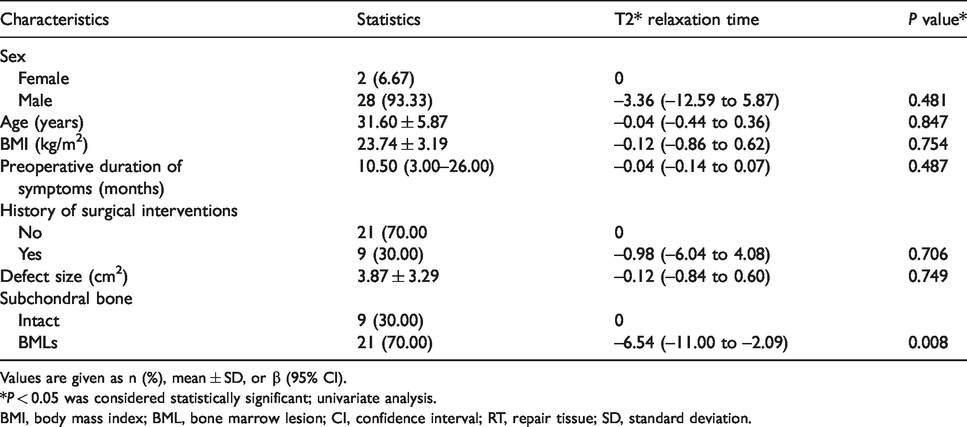
Values are given as n (%), mean ± SD, or β (95% CI).
*P < 0.05 was considered statistically significant; univariate analysis.
BMI, body mass index; BML, bone marrow lesion; CI, confidence interval; RT, repair tissue; SD, standard deviation.
Next, we assessed correlations between subchondral BMLs and cartilage RT by multivariate linear regression, with covariate screening for possible confounding factors, including age, sex, BMI, defect size, preoperative duration of symptoms, and history of surgical interventions. There was a significantly negative correlation between subchondral BMLs and cartilage RT; the T2* relaxation time decreased with the occurrence of subchondral BMLs (β = –6.66, 95% CI = –11.82 to –1.50, P = 0.019) (Table 3, Figs. 3 and 4).
Independent correlations between subchondral bone and cartilage RT metrics.
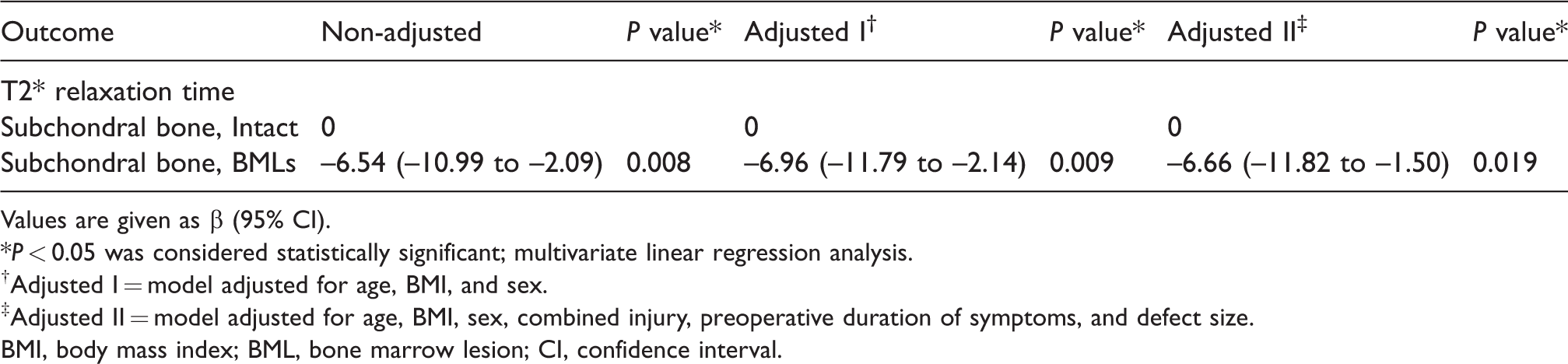
Values are given as β (95% CI).
*P < 0.05 was considered statistically significant; multivariate linear regression analysis.
†Adjusted I = model adjusted for age, BMI, and sex.
‡Adjusted II = model adjusted for age, BMI, sex, combined injury, preoperative duration of symptoms, and defect size.
BMI, body mass index; BML, bone marrow lesion; CI, confidence interval.
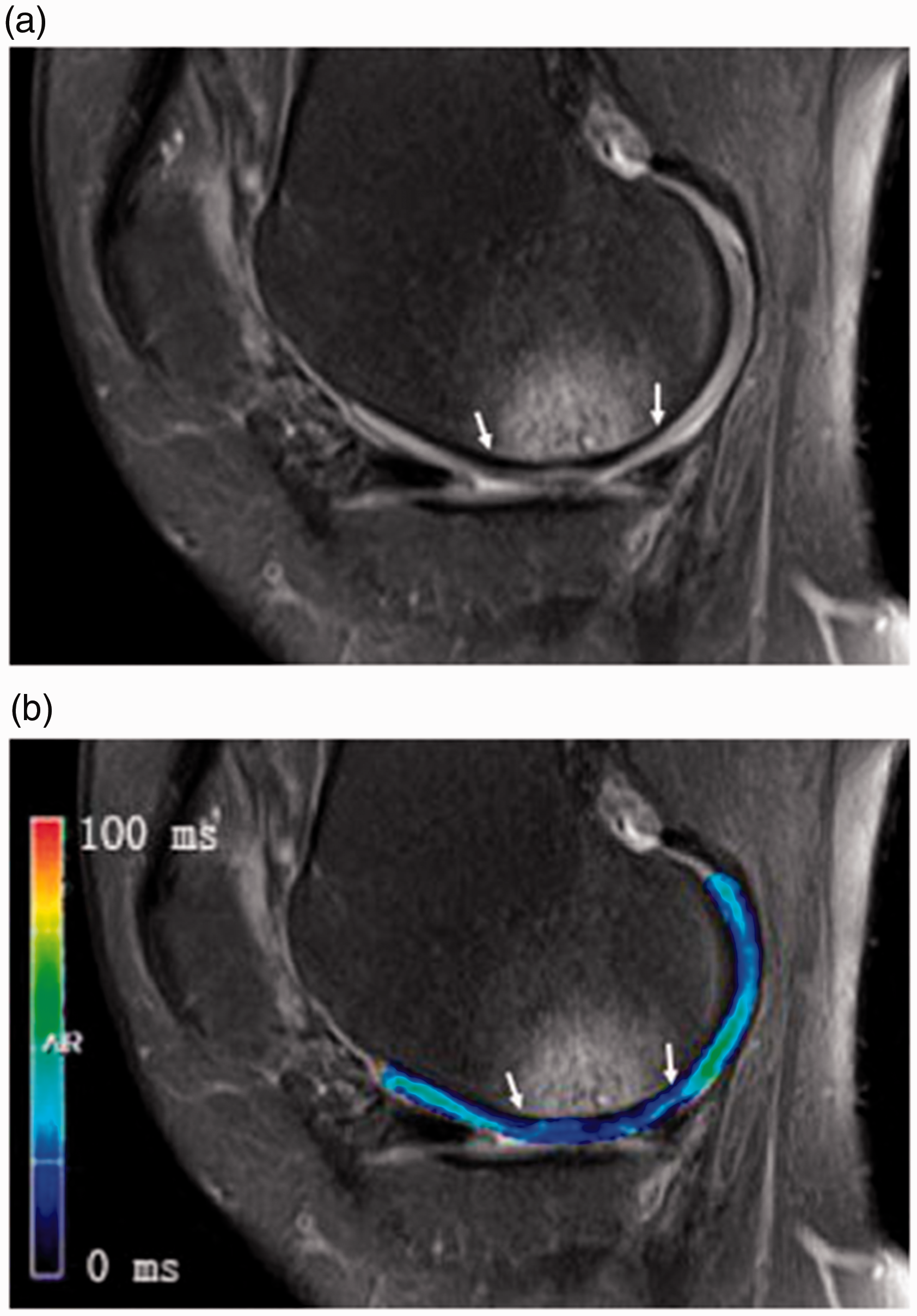
A 32-year-old man 20 months after MACI with subchondral bone edema-like signal alterations. (a) Representative sagittal 2D-PD-FS sequence displayed subchondral bone edema-like signal alterations at the repair site (between white arrows). Cartilage RT-T2* relaxation time was 23.3 ms (b). T2* relaxation time of the HC region at intra-knee femur was 34.4 ms. FS, fat-suppressed; HC, healthy control femoral cartilage; MACI, matrix-associated autologous chondrocyte implantation; PD, proton density-weighted; RT, repair tissue.
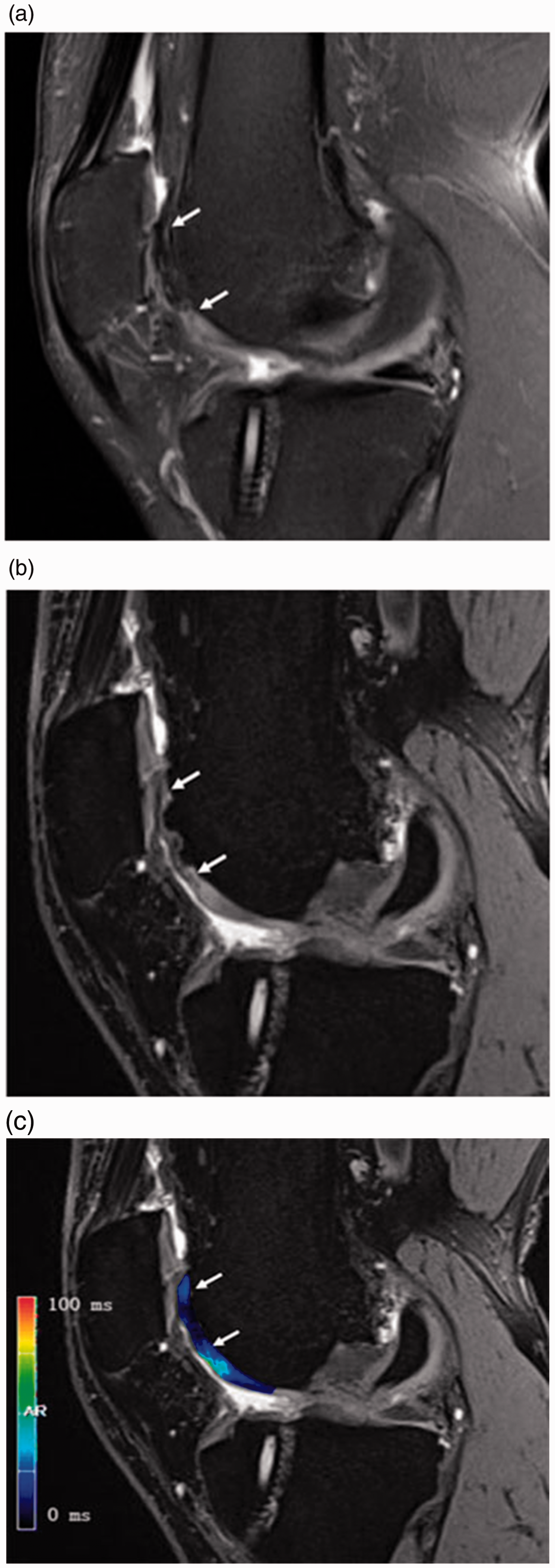
A 35-year-old man 15 months after MACI with subchondral bony overgrowth. Compared with the sagittal 2D-PD-FS sequence (a), the sagittal 3D-DESS sequence could display the interface between bone marrow and cartilage more clearly, demonstrating subchondral bony overgrowth and a thinning of the cartilage RT (between white arrows) (b). Cartilage RT-T2* relaxation time was 12.3 ms (c), T2* relaxation time of the HC region at intra-knee femur was 35.6 ms. DESS, dual-echo steady-state; FS, fat-suppressed; HC, healthy control femoral cartilage; MACI, matrix-associated autologous chondrocyte implantation; PD, proton density-weighted; RT, repair tissue.
Discussion
In this cross-sectional study, the quality of cartilage RT was assessed with T2* relaxation time, and PD-FS and 3D-DESS sequences were used to qualitatively evaluate subchondral BMLs to determine the correlation between the cartilage RT and subchondral BMLs. Cartilage RT begins to mature six months after MACI (18). Previous studies have reported that one-year postoperative MRI outcomes could predict long-term efficacy (maximum follow-up period = 17.8 years) (19). Therefore, we selected patients for the present study who had MACI at least 12 months previously. The results demonstrated that the presence of subchondral BMLs was significantly negative correlated with cartilage RT in patients undergoing MACI. The T2* relaxation time decreased with the occurrence of subchondral BMLs after adjusting for the full model.
Until now, micro-computed tomography (CT) is the only imaging tool that can quantify the microstructure of subchondral bone, such as bone mineral density and trabecular thickness, but only for ex vivo specimens and animal models (20,21). In most patients, good or excellent clinical outcomes were achieved and there was no need for histological biopsy. Clinically, MRI is considered the most accurate method for the evaluation of subchondral bone and cartilage. Most current researches were focused on the correlation between subchondral bone edema-like signal alterations and cartilage RT (22). Additionally, subchondral bony overgrowth was a specific phenomenon after cartilage repair procedures, and was found in more than half of the defects in animal models (10). However, it was still rarely recorded due to the lower image resolution techniques of conventional 2D sequences compared to experimental studies. The advantages of 3D-FS sequences can clearly outline the thickness and surface of uncalcified cartilage. Therefore, combined with the 3D-DESS sequence, we could show the phenomena more clearly. In the present study, subchondral bony overgrowth was seen in 15 of 30 patients, but five of them were not detected by the 2D-PD-FS sequence. This important finding indicated that subchondral bony overgrowth was a previously underestimated factor for patients undergo MACI. We speculated that the combination with the 3D-DESS sequence could be more sensitive to detect the alterations in the interface between subchondral bone marrow and cartilage, but it must be emphasized that the small sample size lacked the necessary statistical power, and it can be seen as an incentive for future research under the same theme.
It is known that changes in the subchondral bone may alter the thickness, density, vascularity, biochemical composition, and mechanical properties of the subchondral plate and then influence the long-term survival of the repair tissue after the cartilage repair procedure (23). The influence of subchondral BMLs on clinical prognosis is different. Niethammer et al. (22) reported that mid-term clinical results of MACI showed a substantial amount of subchondral bone edema-like signal alteration over a 36-month follow-up, but it did not correlate with worse clinical outcome. Compared with subchondral bone edema-like signal alteration, other formation of subchondral BMLs may lead to a worse prognosis and may most likely impair surgical revision procedures (24). Previous clinical research reported on subchondral bony overgrowth after cartilage repair procedure by MRI, demonstrating a overgrowth of the subchondral bone with resultant relative thinning of overlying repair tissue (25). Similar findings were confirmed by histological study: Beck et al. (21) observed subchondral bone changes in all patients with clinically failed total knee arthroplasty (TKA) and found significantly worse abnormal calcification and vascularization in patients with TKA, and suggested endochondral ossification may play a pivotal role in the clinically failed patient. Therefore, the detection of subchondral bony overgrowth is of great significance after a cartilage repair procedure.
In addition, it should be noted that subchondral BMLs may also occur secondary to other issues. The cartilage RT after MACI may not be sufficient to protect the underlying subchondral bone from mechanical forces and thus lead to the progressive formation of subchondral BMLs (9). In the present study, the cartilage RT-T2* relaxation time of 30 patients was 23.02 ms after MACI on MRI follow-ups, which was significantly lower (P < 0.0001) than that of the healthy cartilage of the femoral trochlear in the same knee, which was 34.46 ms. Moreover, the T2* relaxation time of cartilage RT in the BML group was significantly lower than that of the intact group (21.30 ± 1.72 ms vs. 28.70 ± 1.30 ms; P = 0.008). Our results suggested that there may be more fibrous tissue in the cartilage RT in the BMLs group, which was considered inferior quality tissue. This hypothesis is supported by previous histological studies: Enea et al. (26) reported that MACI yielded a predominantly hyaline cartilage matrix in only 21% of the cases; Bartlett et al. (27) found that biopsies taken from patients treated with MACI showed 51% of them were fibrocartilage at the one-year follow-up; and Hollander et al. (28) found that 43% of patients had fibrocartilage 6–25 months after the MACI procedure. Therefore, we believed that the newly synthesized cartilage RT does not own the same biomechanical properties compared to the hyaline articular cartilage, especially in patients in the BML group. This may possibly result in ultimately osteoarthritic joint degeneration (29).
The present study has some limitations. First, the present study lacks a gold standard; invasive follow-up arthroscopies are no longer performed in a clinical setting, and the subchondral BMLs cannot be sufficiently evaluated by arthroscopy. Second, we did not exclude patients with a history of surgical interventions, which may be a confounding variable; however, the regression analysis in our study showed that it did not affect the outcomes. Finally, no quantitative analysis of the trabecular bone was performed, which is a major limitation because there are still no clinical imaging methods for the quantitative examination of subchondral bone in living humans. The following studies should focus on the texture measures of trabecular bone microstructure.
In conclusion, we used 2D-PD-FS and 3D-DESS sequences in the present study to evaluate comprehensively the underlying subchondral BMLs, and identified that subchondral BMLs were significantly correlated with cartilage RT-T2* relaxation times. These deteriorations of the subchondral bone are likely an additional, previously underestimated factor that influences the outcome of cartilage repair strategies. Our study found that the quality of cartilage repair tissue depended on the integrity of the underlying subchondral bone. The future of cartilage repair lies in better diagnostics to properly recognize alterations in subchondral bone that might compromise the cartilage RT, as well as advanced treatment options that will allow us to restore the entire osteochondral unit. Thus, osteochondral defects require not only cartilage repair but also the repair of subchondral bony defect.
Footnotes
Acknowledgements
The authors thank Yuli Wang and Xixiong Qiu for reviewing the cases, Haofei Hu for his useful suggestions in data statistics, and Ruishen Chen for processing the figures.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: This study has received funding by the Project of Shenzhen Municipal Health Commission Foundation (SZFZ2018061) and the Project of Shenzhen International Cooperation Foundation (GJHZ20180416164801042).