
Abstract
Background
Idiopathic granulomatous mastitis (IGM) is a chronic, unpleasant autoimmune inflammatory condition and is clinically and radiologically often confused with breast malignancy.
Purpose
To investigate the contributions of qualitative and quantitative aspects of acoustic radiation force impulse (ARFI) elastography to the differential diagnosis between IGM and invasive ductal carcinoma (IDC) in the breast.
Material and Methods
Ninety-four women with IDC and 39 with IGM were included in the study. Shear wave velocity (SWV) was calculated for all lesions using quantitative elastography. Next, each lesion’s correspondence on qualitative elastographic images to those on the B-mode images was evaluated: pattern 1, no findings on elastography images; pattern 2, lesions that were bright inside; pattern 3, lesions that contained both bright and dark areas; and pattern 4, lesions that were dark inside. Pattern 4 was subdivided into 4a (dark area same size as lesion) and 4b (dark area larger than lesion size). Sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy were calculated.
Results
The mean SWV based on ARFI elastography was 3.78 ± 1.26 m/s for IGM and 5.34 ± 1.43 m/s for IDC lesions (P < 0.05). Based on qualitative ARFI elastography, IDC lesions were mostly classified as pattern 4b, while IGM lesions were mostly classified as pattern 1 or 2 (P = 0.01). Evaluation of both the qualitative and quantitative aspects of ARFI elastography yielded a sensitivity of 89% and specificity of 84%.
Conclusion
ARFI elastography may facilitate the differential diagnosis between IGM and IDC.
Keywords
Introduction
Idiopathic granulomatous mastitis (IGM) is a rare, benign, chronic granulomatous inflammatory breast disease commonly mistaken for breast cancer both clinically and radiographically. The radiographic and clinical characteristics of IGM can mimic malignancies and other types of mastitis (1,2). On ultrasonographic examination, IGM typically presents as irregular hypoechoic masses, multiple hypoechoic masses, parenchymal heterogeneity, or heterogeneous echogenic areas. Moreover, IGM has no specific radiographic characteristics and cannot be diagnosed radiologically in all patients. Misdiagnosis can lead to unnecessary anxiety for both patients and clinicians. A definitive diagnosis of IGM often requires tissue biopsy (3).
Neoplasia is a pathophysiological process that affects tissue elasticity (4). Ultrasound elastography (USE) has been developed as an objective method for quantification of tissue stiffness. Acoustic radiation force impulse (ARFI) elastography is an US-based imaging technique used in addition to B-mode US to analyze tissue stiffness qualitatively and quantitatively, without compression. ARFI can provide information about both the morphological properties and mechanical hardness of tissue (5). ARFI elastography is more reproducible, and therefore more objective, than strain elastography (6). Furthermore, previous studies have shown that ARFI elastography can improve diagnostic performance as an adjunct to B-mode US (5). Increased amounts of periductal and stromal elastic fibers in breast carcinoma, and the absence of these fibers in non-neoplastic lesions, can be used to distinguish IGM lesions from stiff breast cancer lesions (7). Breast cancer lesions have a higher strain ratio and greater elasticity than benign breast lesions (8). Breast lesions that are abnormally stiff and immobile are often considered as cancerous (4).
There are previous studies demonstrating the performance of elastography in the differential diagnosis of IGM and malignant breast lesions (9,10). As far as we know we have not found any study in which the difference between IDC (the most common breast cancer) and IGM were revealed by elastography. The aim of the present study was to analyze the qualitative and quantitative elastographic characteristics of IGM and IDC on ARFI elastography.
Material and Methods
Patients
This prospective study was carried out between September 2019 and March 2020 at the Van Yuzuncu Yıl University Medical Center Breast Radiology Unit. The study was reviewed and approved by the local ethics committee (26 July 2019, no. 001) and was conducted in accordance with the 1964 Declaration of Helsinki. In all patients, before US, USE, and Tru-cut biopsy, the procedures were explained verbally and written consent was obtained. During the study period, a total of 320 consecutive female patients with suspected malignancy (American College of Radiology [ACR] Breast Imaging Reporting and Data System [BI-RADS] category 4–5) (11) were referred to our radiology clinic from the general surgery department. B-mode US and ARFI elastography images of the lesions were saved in the Picture Archiving and Communication System (PACS). B-mode US and ARFI elastography examinations were carried out by one radiologist with at least five years of experience in breast elastography. The same radiologist also performed Tru-cut biopsy using a 14-G biopsy needle 10 cm in length under US guidance. The data obtained were evaluated by another radiologist blinded to the patient clinical information, US findings, and histopathology results. Patients with invasive ductal carcinoma (IDC) and IGM according to the biopsy results were included in the study. Patients with other breast lesions diagnosed as benign, other types of mastitis, cancers other than IDC, or ductal carcinoma in situ were excluded from the study. Only IDC was included in the study because we were considering demonstrating the elastography characteristics of specific type breast cancer. The final study population consisted of 133 patients diagnosed with IDC (n = 94) or IGM (n = 39).
B-Mode US and ARFI elastography
Conventional US and ARFI elastographic imaging were performed using an ACUSON S2000 US system (Siemens Medical Solutions, Mountain View, CA, USA). B-mode US imaging was performed using a wide-format 50-mm linear array transducer with a bandwidth of 14 MHz). Each lesion was characterized on US based on its shape, orientation, margin, echo pattern, posterior features and the presence of calcifications. If there was more than one lesion in cases, the lesion with the highest BI-RADS score was considered as the index lesion. The US findings were analyzed based on the BI-RADS score (11).
Qualitative (Virtual Touch Tissue Imaging [VTTI]; Siemens) and quantitative (Virtual Touch Tissue Quantification [VTTQ]; Siemens) ARFI technologies were applied using a linear-array transducer with a bandwidth of 9 MHz.
For all elastography measurements, the same imaging parameters were applied and the breast imaging mode was used. The US probe was affixed to the lesion using gel, and no pressure was applied to the skin. A split screen display mode was used to obtain B‐mode and shear wave elastography (SWE) images of the same area. The lesion appeared as a grayscale image on the right, and each patient was instructed to hold her breath while the SWE images were acquired (displayed on the left).
With VTTI, images are produced by combining multiple independently acquired axial tissue displacement images. Starting with the leftmost axial line within the region of interest (ROI), a baseline B-mode US image is obtained. Next, a push pulse is applied to image the displaced tissue. The baseline and post push images are compared using a cross-correlation algorithm that computes the differences in tissue position, with versus without tissue compression, at various points along the axial line (12–15). VTTI generates a grayscale map of tissue stiffness in the ROI. Lesions are classified according to their characteristics and width (12).
In the present study, each lesion’s correspondence on qualitative elastographic images to those on the B-mode images was evaluated: pattern 1 = no findings on elastography images; pattern 2 = if it contained a bright (i.e. soft) area; pattern 3 = if it contained both bright (i.e. soft) and dark (i.e. stiff) areas; and pattern 4 = if it was completely dark (i.e. stiff). According to width, pattern 4 lesions were subclassified as 4a if the lesion size was equal to that in VTTI and as 4b if the lesion was smaller than in VTTI (12,16). Lesion width was compared visually between ARFI elastographic and B-mode images for classification as pattern 4a or 4b.
The shear wave velocity (SWV) of breast lesions was measured by VTTQ (7,12,17). To generate and numerically analyze shear waves, excitation and tracking pulses were applied and the SWV was calculated in meters per second (5,6). To measure SWV with ARFI, an equal number of ROIs of 1 × 1 mm were placed in the brightest (softest) and darkness (stiffest) visible areas in the centers of the lesions. The number of ROIs placed was determined according to the size of the lesion. The values thus obtained were averaged for each lesion. SWV > 10 m/s was outside the measurement range of the system.
Statistical analysis
Descriptive statistics for the continuous variables are presented as mean ± standard deviation (SD) and ranges, while categorical variables are presented as numbers and percentages. Student’s t-test was used to compare the IGM and IDC group means for all variables of interest. The chi-square test was used to analyze categorical variables. The independent samples t-test was used to compare SWV between the IGM and IDC. The optimal cut-off for SWV was determined by receiver operating characteristic (ROC) curve analysis, for both IGM and IDC. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and diagnostic accuracy values were obtained. At VTTI evaluation, while all pattern 1 and 2 lesions were benign, all pattern 4b lesions were considered malignant, and it was predicted that patterns 3 and 4a could be observed in both groups (12). A second cut-off value was determined in SWV for patterns 3 and 4a that seen in both IDC and malignant lesions. After all, the final sensitivity, specificity, PPV, NPV, and accuracy values were obtained by interpreting SWV and VTTI methods together. A two-way Anova test was used to find the relationship between mean SWV values measured in IGM and IDC lesions according to VTTI. SPSS software (ver. 13.0; SPSS Inc., Chicago, IL, USA) was used for all statistical analyses, and P < 0.05 was taken to indicate statistical significance.
Results
IDC were more common than IGM lesions in older patients (P < 0.05). The lesions in both groups were compared according to the B-mode US findings; IDC tended to show spiculated contours, while IGM lesions tended to show angular contours (P < 0.05). Posterior acoustic shadowing, which is caused by a desmoplastic reaction, was observed more frequently in IDC than IGM lesions (P < 0.05). Calcifications were more frequent in IDC (P < 0.05). Based on the B-mode US findings, all of the lesions in both groups were classified as BI-RADS ≥ 4.
The mean internal SWV was significantly higher for IDC lesions than IGM lesions (5.98 ± 0.12 and 3.78 ± 1.26 m/s, respectively, P < 0.05). With regard to the differential diagnosis, there was a significant difference in SWV internal value between IGM lesions and IDC (P < 0.05).
IDC were mostly pattern 4b, and none were pattern 1 or 2 (Figs. 1 and 2) and there did not seem to be any confusion for these two patterns. The IGM lesions were mostly patterns 1–3 (P < 0.05). Although pattern 3 was more common in IGM lesions, it was also observed in IDC (Table 1). Patterns 3 and 4a were observed in both IDC and IGM lesions, but internal SWV values were higher for IDC than IGM lesions (Figs. 3 and 4) (Table 2). In addition, 80% of the IDC classified as pattern 3 were > 2 cm in diameter, which was a significantly higher rate than in the IGM pattern 3 lesions (P = 0.02).
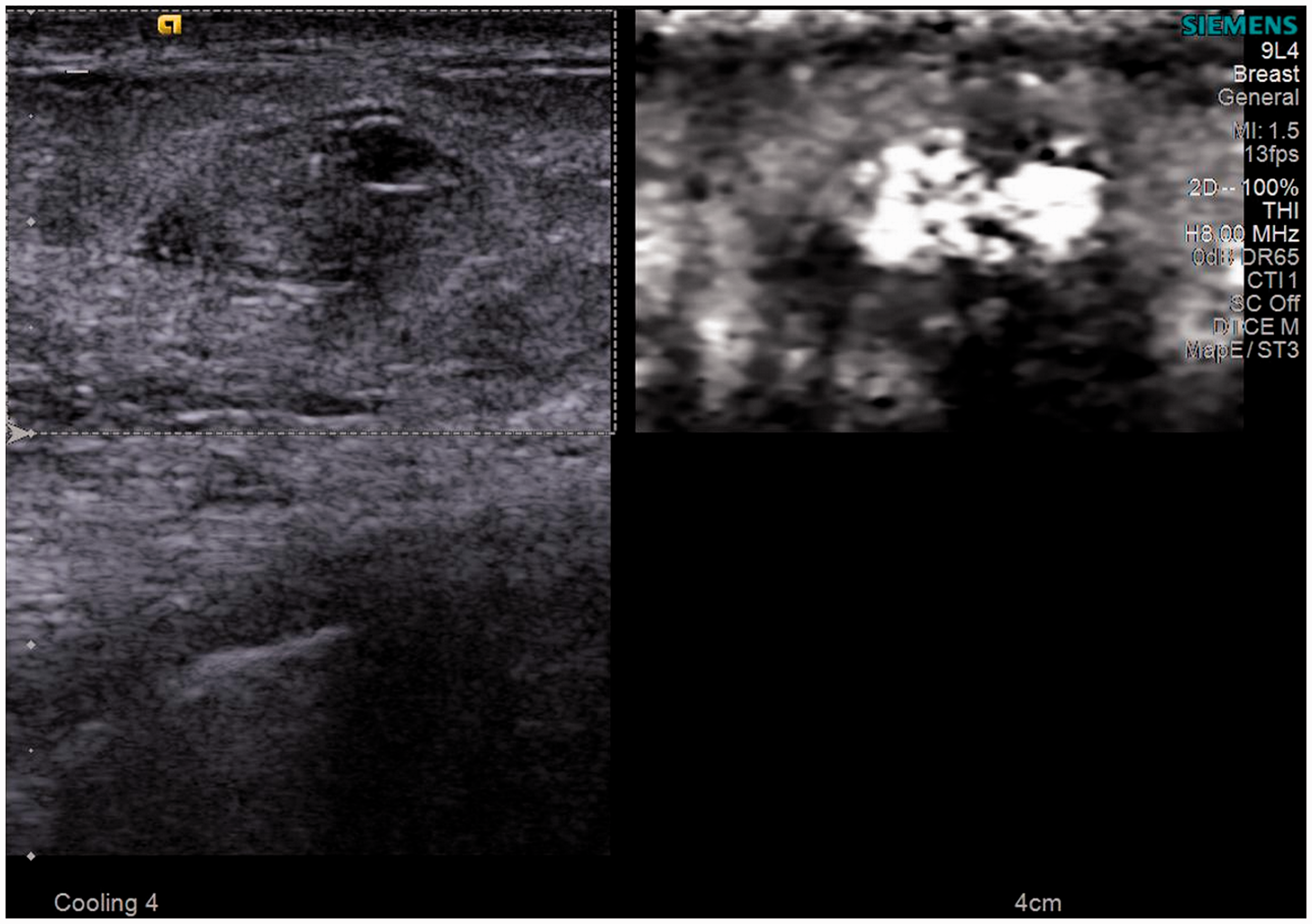
A 35-year-old patient with idiopathic granulomatous mastitis. The lesion was classified as BI-RADS 4a on B-mode ultrasound due to the “angular margin,” which was classified as pattern 2 on Virtual Touch Tissue Imaging.
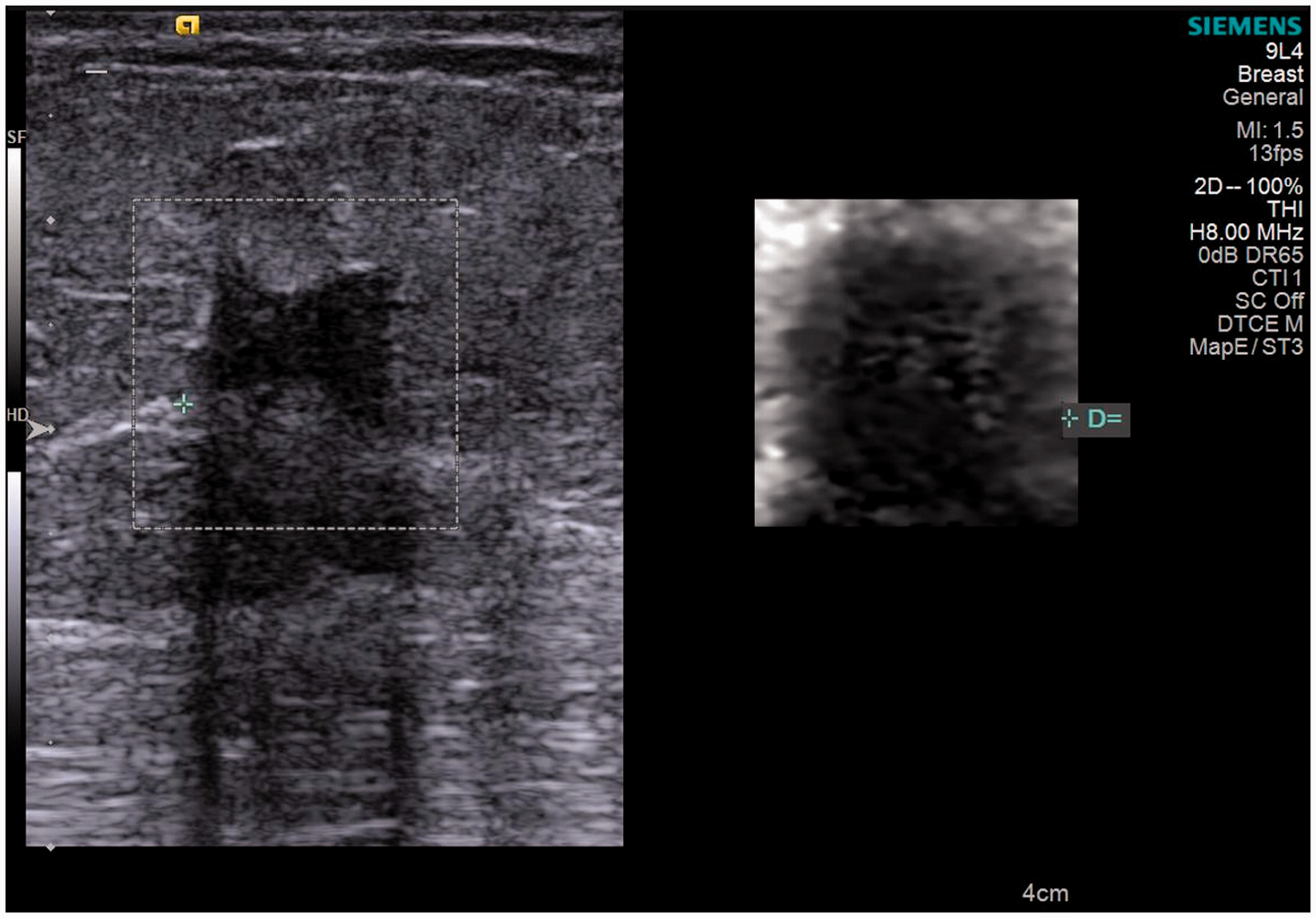
A 52-year-old patient with invasive ductal carcinoma. Pattern 4b on Virtual Touch Tissue Imaging. The lesion diameter on the qualitative elastography image shown on the right was greater than that in the B-mode ultrasound image shown on the left.
Comparison of the idiopathic granulomatous mastitis and invasive ductal cancer findings.
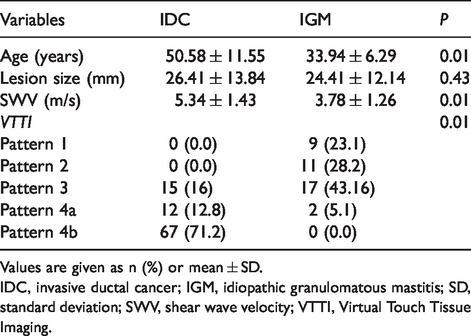
Values are given as n (%) or mean ± SD.
IDC, invasive ductal cancer; IGM, idiopathic granulomatous mastitis; SD, standard deviation; SWV, shear wave velocity; VTTI, Virtual Touch Tissue Imaging.

(a, b) A 46-year-old patient with invasive ductal carcinoma with a pattern 3 lesion according to qualitative elastography. The mean shear wave velocity based on quantitative elastography was 5.98 m/s.

(a, b) A pattern 3 lesion was observed on qualitative elastography in a 28-year-old patient with idiopathic granulomatous mastitis. The mean shear wave velocity value based on quantitative elastography was 3.16 m/s.
Relationship of SWV measured in IDC-IGM with pattern models in VTTI.
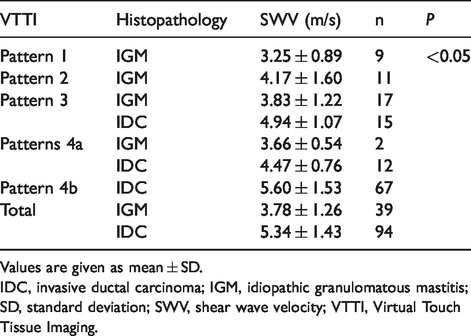
Values are given as mean ± SD.
IDC, invasive ductal carcinoma; IGM, idiopathic granulomatous mastitis; SD, standard deviation; SWV, shear wave velocity; VTTI, Virtual Touch Tissue Imaging.
For only SWV assessment, the area under the ROC curve (AUC) was 0.796 (95% confidence interval [CI]) (P < 0.001). To distinguish between IDC and IGM; the optimal SWV cut-off value was 4.34 m/s (sensitivity, 74%; specificity, 72%; accuracy, 70%; PPV, 86%; NPV, 51%). Based on the literature, while all pattern 1 and 2 lesions were benign, all pattern 4b lesions were considered malignant, and it was predicted that patterns 3 and 4a could be observed in both groups (12). At qualitative analysis, quantitative combined evaluation the area under the ROC curve (AUC) was 0.802 (95% CI) (P < 0.001). Then, the SWV’s secondary cut-off value was found to be 3.95 m/s according to the VTTI patterns. According to this, when both qualitative and quantitative ARFI elastography data were evaluated, when an SWV cut-off value of 3.95 m/s was used to distinguish them at patterns 3 and 4a, seen in both IDC and IGM, the sensitivity, specificity, accuracy, PPV, and NPV were 89%, 84%, 88%, 89%, and 76%, respectively.
Discussion
The efficacy of a combination of qualitative ARFI elastography and SWV measurements was evaluated for distinguishing between IGM lesions and malignant breast lesions (IDC) in this study. IGM lesions often show signs of inflammation. However, some IGM masses may not present with inflammatory signs on US, which complicates the differential diagnosis between these and malignant lesions (3). In the present study, all pattern 1 and 2 lesions based on qualitative ARFI elastography assessment were diagnosed as IGM. In the literature, patterns 1 and 2 are classified as benign lesions with high NPV, which was consistent with our findings (7,12,13). Focal enlarged ductal content or a pseudocyst appearance of IGM can be misinterpreted as a solid lesion (18). The pattern 2 IGM lesions in the present study probably contained viscous fluid, i.e. they were not solid masses.
The SWV values measured by VTTQ in the present study were higher for IDC than IGM lesions. Yagci et al. (9) evaluated IGM and malignant breast lesions using strain elastography and reported that the strain ratio was higher in the latter lesions. Similarly, Teke et al. (10) evaluated IGM and malignant lesions using ARFI elastography and reported higher SWV values in malignant lesions. The SWV values found for IGM lesions in the present study were higher than the SWV values detected for benign lesions in the literature (19,20). Some previous studies reported that IGM lesions exhibited SWV values as high as those of malignant lesions and indicated that the use of quantitative elastography indices alone may lead to false-positive results (21–23).
VTTI, an ARFI-based technique that allows qualitative assessment of lesions, has been shown to be useful for visualizing the desmoplastic reaction surrounding malignant lesions (7,12,16). On VTTI, pattern 4b lesions are associated with peritumoral invasion (12). The size of these lesions on VTTI is larger than on B-mode US, which is attributed to peritumoral invasion by malignant lesions (12). In the present study, similar to previous reports (7,10,12,24), malignant breast lesions were classified as pattern 4b; this pattern reliably distinguished between IGM and IDC.
Although pattern 3 is often associated with benign lesions, it was detected in both groups in the present study, although at a higher rate in IGM than IDC. While the detection of pattern 3 lesions in both lesion groups was unexpected, the SWV values were higher in IDC than IGM pattern 3 lesions (4.94 ± 1.07 m/s and 3.83 ± 1.22 m/s, respectively, P = 0.01). We suggest that lesions may be classified as pattern 3 on VTTI based on central necrosis. The large size of IDC lesions and therefore central necrosis may explain the incidence of pattern 3. It was reported previously that although malignant lesions may exhibit central necrosis, they are unlikely to show liquefaction necrosis and may have stiff fibrotic tissue in areas of necrosis (21). This may provide insight into the high SWV values of malignant pattern 3 lesions. Differential diagnosis of IGM and IDC could be facilitated by the use of SWV in combination with qualitative assessments.
SWV, which is associated with lesion stiffness, is partly operator-dependent. It is well-known that benign breast lesions may be mischaracterized as malignant based on high SWV values (25,26). In the present study, the mean SWV values of IGM lesions were higher than those of lesions defined as benign in the literature (19,20). Similarly, some previous studies indicated that IGM lesions exhibited similarly high SWV values to those of malignant lesions, and that the use of a quantitative method alone may lead to false-positive results (21–23). For distinguishing between IGM and IDC, our results indicated that the combined use of qualitative and quantitative aspects of ARFI elastography increased sensitivity, specificity, PPV, NPV, and diagnostic accuracy.
The present study has some limitations. First, it used a single-center design and included a small patient population and all examinations were performed by a single physician. Second, Ciurea et al. (27) suggested that lesion depth has a significant effect on outcomes, but this was not measured when obtaining the SWV measurements in the present study (27). Third, the sizes of pattern 4b lesions measured on B-mode US and VTTI were not expressed as numerical values; instead, they were assessed based on subjective visual inspection. Diagnostic decisions based on numerical data would have been more objective. Fourth, the mean SWV values were obtained by placing an equal number of ROIs on the stiffest and softest tissues within the lesion; although we considered this measurement approach to be more favorable for non-homogenous lesions, further studies are needed to compare malignant and benign lesions with SWV values based on a single ROI. Finally, we could not compare IGM lesions with inflammatory breast cancer as there were no cases of the latter in our cohort.
In conclusion, the present study indicated that qualitative and quantitative assessment by elastography improved diagnostic performance, i.e. helped distinguish between IGM and IDC. Further development of VTTI, for distinguishing cystic IGM lesions with a malignant appearance from IDC lesions, can aid diagnosis without the need for biopsy. In distinguishing IGM from other types of breast cancer and especially soft cancers such as mucinous cancer, and lobular cancers that tend to be multifocal, we believe that studies using the VTTI method showing desmoplastic reaction of malignancies are needed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.