
Abstract
Background
The demand for homogeneous and higher vascular contrast enhancement is critical to provide an appropriate interpretation of abnormal vascular findings in coronary computed tomography angiography (CTA).
Purpose
To evaluate the effect of various contrast media concentrations (Iohexol-370, Iohexol-300, Iohexol-240) and image reconstructions (filtered back projection [FBP], hybrid iterative reconstruction [IR], and deep learning reconstruction [DLR]) on coronary CTA.
Material and Methods
A total of 63 patients referred for coronary CTA between July and October 2021 were enrolled in this prospective study, and they randomly received one of three contrast media. CTA images were reconstructed with FBP, hybrid IR, and DLR. The CT attenuation, image noise, signal-to-noise ratio (SNR), and contrast-to-noise ratio (CNR) were calculated for all three images. The images were subjectively evaluated by two radiologists in terms of overall image quality, artifacts, image noise, and vessel wall delineation on a 5-point Likert scale.
Results
The application of DLR resulted in significantly lower image noise; higher CT attenuation, SNR, and CNR; and better subjective analysis among the three different concentrations of contrast media groups (P < 0.001). There was no significant difference in the CT attenuation of the left ventricle (P = 0.089) and coronary arteries (P = 0.072) between hybrid IR at Iohexol-300 and DLR at Iohexol-240. Furthermore, application of DLR to the Iohexol-240 significantly improved SNR and CNR; it achieved higher subjective scores compared with hybrid IR at Iohexol-300 (P < 0.001).
Conclusion
We suggest that using DLR with Iohexol-240 contrast media is preferable to hybrid IR with Iohexol-300 contrast media in coronary CTA.
Introduction
Computed tomography angiography (CTA) has been widely used owing to technological improvements in its ability to detect obstructive coronary artery disease. The demand for homogeneous and high-vascular contrast enhancement is critical for CTA to provide an appropriate interpretation of abnormal vascular findings (1,2). Coronary artery enhancement at a CT attenuation above 250 Hounsfield units (HU) is suggested for evaluating atherosclerotic changes and stenosis in coronary CTA (3). Generally, vascular enhancement is determined by scanning acquisition and reconstruction parameters (scan duration, tube voltage, and tube current), patient-related factors (heart rate, body weight, and cardiac output), injection rate, and contrast media concentration (4–6). Although reducing the tube voltage can reduce the radiation dose and improve vascular attenuation, higher image noise and artifacts are major problems (7–9). The linear relationship between the injection parameters of contrast media (total amount of contrast media, flow rate and concentration of contrast media, and saline chaser) and the degree of vascular attenuation has also been investigated in several studies (10,11). Increasing the flow rate of contrast media may result in contrast extravasation (12). Thus, a contrast media with higher iodine concentration is preferred to obtain a greater vascular enhancement. However, higher iodine concentration is not recommended for patients with cardiovascular disease because they are susceptible to contrast-induced nephropathy (13). Thus, an effective contrast media delivery method using a lower iodine concentration is preferable for the safety of patients and evaluation of abnormal changes in CTA.
The image reconstruction algorithm can improve the vascular enhancement without increasing the iodine concentration of the contrast media in CTA. Previous studies focused on the advantages of deep learning reconstruction (DLR). DLR was developed to reduce the image noise and improve spatial resolution through deep neural networks and its high-quality model-based iterative reconstruction (MBIR) or filtered back projection (FBP) training images, referred to as advanced intelligent clear-IQ engine (AiCE) (14) and TrueFidelity (15), respectively. Several clinical studies have demonstrated that the lesion detection rate and image quality of DLR are higher than those of iterative reconstruction (IR) for low-dose chest CT, abdominal CT, brain CTA, and coronary CTA (16–21); however, there has been no evidence proving the effect of different contrast media iodine concentrations on DLR in coronary CTA. Enhancing vascular attenuation through DLR decreases the iodine load in patients with renal impairment.
The aim of the present study was to evaluate the effect of various contrast media concentrations (Iohexol-370, Iohexol-300, and Iohexol-240) on coronary CTA using the same flow rate and image reconstruction algorithms (FBP, hybrid IR, and DLR). Furthermore, this study identified the image reconstruction method that yields the highest image quality with the lowest possible iodine concentration.
Material and Methods
Participants
All individuals gave written informed consent for inclusion before they participated in this prospective study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Inje University Seoul Paik Hospital (file no. 2021-06-009). A total of 63 patients (43 men; mean age = 59.32 years; age range = 26–86 years) referred for coronary CTA were enrolled in this study from July to October 2021 and randomly received one of three different contrast media (each was received by 21 patients). We used three different iodine concentrations of contrast media: Iohexol-370 (Bonorex 370; Central Medical Service, Republic of Korea); Iohexol-300 (Bonorex 300; Central Medical Service, Republic of Korea); and Iohexol-240 (Bonorex 240; Central Medical Service, Republic of Korea). The volume and rate of contrast media were consistent among the three different iodine concentrations. A total of 80 mL contrast media was injected into the antecubital vein at a rate of 4.5 mL/s via a power injector (CT Motion; Ulrich Medical, Ulm, Germany), followed by a 30-mL saline flush at a rate of 5.0 mL/s. The scan was triggered using the automatic bolus-tracking program (Surestart; Canon Medical Systems Corporation, Otawara, Japan) in the descending thoracic aorta (trigger threshold was set as 250 HU). Patients with a prior allergic reaction to iodine-containing compounds, pregnancy, impaired renal function (glomerular filtration rate <60 mL/min), hyperthyroidism, psychiatric disorder, or clinical instability were excluded.
Scanning protocols
All coronary CTAs were performed using a 320 multidetector volume scanner (Aquilion ONE Prism; Canon Medical Systems Corp., Otawara, Japan). Each patient underwent a non-contrast acquisition process for the analysis of coronary artery calcification, followed by coronary CTA. The following parameters were used for coronary CTA: detector collimation = 130 × 0.5 mm; field of view = 416 mm; gantry rotation time = 0.4 s; wide-volume scanning pitch = 0.813; slice thickness = 1 mm; and tube voltage = 100 kVP. Each section was 140 mm in the longitudinal direction. An automatic exposure control function (SD 20) was performed for tube current. All examinations were performed with prospective electrocardiography triggering methods covering 30%–85% of the cardiac cycle of the patients. The patients received no additional beta-blockers.
Image reconstruction
The raw data were retrieved from a CT scanner and reconstructed using the following three algorithms: FBP; hybrid IR with standard FC14 reconstruction kernel (adaptive iterative dose reduction 3-D [AIDR-3D] (17,22), Canon Medical Systems Corporation, Otawara, Japan); and DLR with body sharp option (AiCE; Canon Medical Systems Corporation, Otawara, Japan).
Objective analysis
The CT attenuation, image noise, signal-to-noise ratio (SNR), and contrast-to-noise ratio (CNR) were calculated at the same position in images reconstructed with FBP, hybrid IR, and DLR for each patient. The CT attenuation was measured by placing the region of interest (ROI) of 100 mm2 in the left ventricle and ROI of 2 mm2 in the proximal segments of the main coronary arteries, including the right coronary artery (RCA), left main coronary artery (LCA), left circumflex artery (LCX), and left anterior descending artery (LAD). The ROIs were placed in the center of the main coronary arteries while avoiding the inclusion of the vessel walls. The image noise determined from subcutaneous fat (ROI of 30 mm2) and muscle (ROI of 20 mm2) was used as a reference to calculate SNR and CNR. The SNR was calculated by dividing the attenuation of the main coronary arteries and left ventricle by the image noise. The CNR was assessed as the difference between the CT attenuation of the main coronary arteries and left ventricle and the attenuation of the muscle divided by the image noise. Histogram analysis was performed for the left ventricle, subcutaneous fat, and muscle by placing the ROI (100 mm2, 30 mm2, and 20 mm2, respectively) in the adjacent seven slices; the mean and standard deviation were measured in HU. The histogram analysis was conducted offline using MATLAB version 8.2.0 (MathWorks, Natick, MA, USA).
Subjective analysis
The images were subjectively evaluated by two radiologists (with three and eight years of reading experience in diagnostic radiology). The observers were blinded to the image reconstruction methods and randomly evaluated the images in terms of overall quality, artifacts, and image noise. A 5-point Likert scale was used for the analysis (Table 1). The coronary arteries were divided into 15 segments according to the American Heart Association classification, and the vessel delineation was rated as follows: 5 = perfect vessel wall definition; 4 = very good vessel wall definition; 3 = good vessel wall definition; 2 = poor vessel wall definition; and 1 = insufficient vessel wall definition (23–25).
Subjective image analysis criteria.
Statistical analysis
Continuous variables are given as mean ± standard deviation. The Shapiro–Wilk and Kolmogorov–Smirnov tests were used to evaluate normality. The CT attenuation, CNR, SNR, and image noise were compared using one-way analysis of variance (ANOVA) among the three image reconstruction methods (FBP, hybrid IR, and DLR) and three iodine concentration contrast media (Iohexol-370, Iohexol-300, Iohexol-240), followed by a post-hoc test using possible pairwise comparison by a Tukey–Kramer test. Concurrently, a two-sample paired t-test was performed to compare image reconstruction methods and different iodine concentrations of contrast media groups. Subjective image scores were compared using the Wilcoxon signed-rank test. Inter-observer agreement in the qualitative evaluation was assessed with Cohen's kappa coefficient (k), where k < 0.20, 0.31 < k < 0.40, 0.41 < k < 0.60, 0.61 < k < 0.80, and 0.81 < k < 1.00 represent poor, fair, moderate, substantial, and near-perfect agreement, respectively. All statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Post-hoc power analyses of the results yielded 80.0% power of the test with a sample size of 63, an effect size of 0.4, and an alpha level of 0.05 (G*power version 3.1.9.6, Düsseldorf, Germany). P < 0.05 was considered to represent a statistically significant difference.
Results
Table 2 describes the characteristics of the 63 patients. The image noise was significantly lower in DLR (Iohexol-370: 10.2 ± 2.4; Iohexol-300: 9.1 ± 2.0; Iohexol-240: 9.8 ± 2.2) compared with hybrid IR (Iohexol-370: 23.1 ± 6.0; Iohexol-300: 21.2 ± 4.8; Iohexol-240: 22.6 ± 3.4) and FBP (Iohexol-370: 48.3 ± 6.9; Iohexol-300: 39.2 ± 8.5; Iohexol-240: 43.6 ± 7.9) for all three iodine concentrations (P < 0.001).
Patient characteristics.
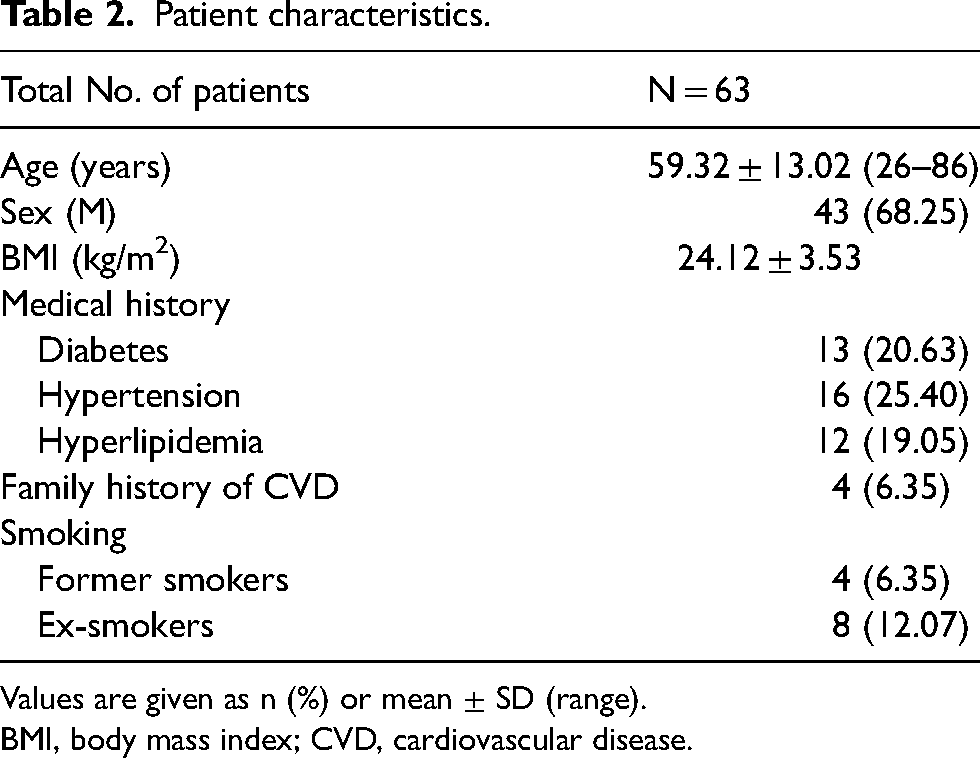
Values are given as n (%) or mean ± SD (range).
BMI, body mass index; CVD, cardiovascular disease.
CT attenuation: Iohexol-370 versus Iohexol-300 versus Iohexol-240
Fig. 1 and Tables 3 and 4 present the scatter plot results of CT attenuation in the left ventricle, coronary arteries, fat, and muscle among the different iodine concentrations (green square = FBP; blue circle = hybrid IR; red diamond = DLR). The mean CT attenuation of the left ventricle was highest among different image reconstructions and iodine concentrations as follows: Iohexol-370 (DLR: 662.9 ± 115.4; hybrid IR: 548.7 ± 83.6; FBP: 550.3 ± 84.7); Iohexol-300 (DLR: 456.1 ± 94.8; hybrid IR: 402.9 ± 66.8; FBP: 404.8 ± 69.2); and Iohexol-240 (DLR: 370.3 ± 69.7; hybrid IR: 336.7 ± 48.8; FBP: 338.9 ± 53.9) (P = 0.136). A post-hoc Tukey's test revealed significant differences (P < 0.001) between each of the different groups (FBP vs. DLR, hybrid IR vs. DLR, Iohexol-240 vs. Iohexol-300, Iohexol-300 vs. Iohexol-370, and Iohexol-240 vs. Iohexol-370). However, no significant difference was found between FBP and hybrid IR (P = 0.558). In addition, the mean CT attenuation value of the coronary artery vessels including LCA, RCA, LAD, and LCX did not show significant differences between Iohexol-370 (DLR: 610.7 ± 98.4; hybrid IR: 505.1 ± 73.9; FBP: 525.0 ± 78.5), Iohexol-300 (DLR: 435.2 ± 84.8; hybrid IR: 384.8 ± 57.5; FBP: 392.2 ± 61.7), and Iohexol-240 (DLR: 352.3 ± 65.1; hybrid IR: 319.5 ± 50.9; FBP: 331.5 ± 55.7) (P = 0.096). Post-hoc Tukey's test resulted in significant differences (P < 0.001) in all possible pairwise comparisons between image reconstructions and iodine concentrations. Therefore, DLR showed significantly higher CT attenuation in the left ventricle and coronary arteries compared with FBP and hybrid IR, regardless of iodine concentration. The CT attenuation of fat (FBP vs. DLR, P = 0.919; hybrid IR vs. DLR, P = 0.995; FBP vs. hybrid IR, P = 0.953) and muscle (FBP vs. DLR, P = 0.974; hybrid IR vs. DLR, P = 0.933; FBP vs. hybrid IR, P = 0.989) was not significantly higher for different iodine concentrations and image reconstructions. Similar to the results of CT attenuation, the histogram plots for the left ventricle show a shift to the right in DLR at different iodine concentrations compared with the images reconstructed with FBP and hybrid IR (Fig. 2). The distribution of attenuation in the histogram plots for fat and muscle was maintained for all image reconstructions at different iodine concentrations. Furthermore, the narrower DLR distribution indicates its lower variability in image noise and CT attenuation compared with FBP and hybrid IR. Notably, DLR boosted CT attenuation in the left ventricle and coronary arteries more than in fat and muscle.
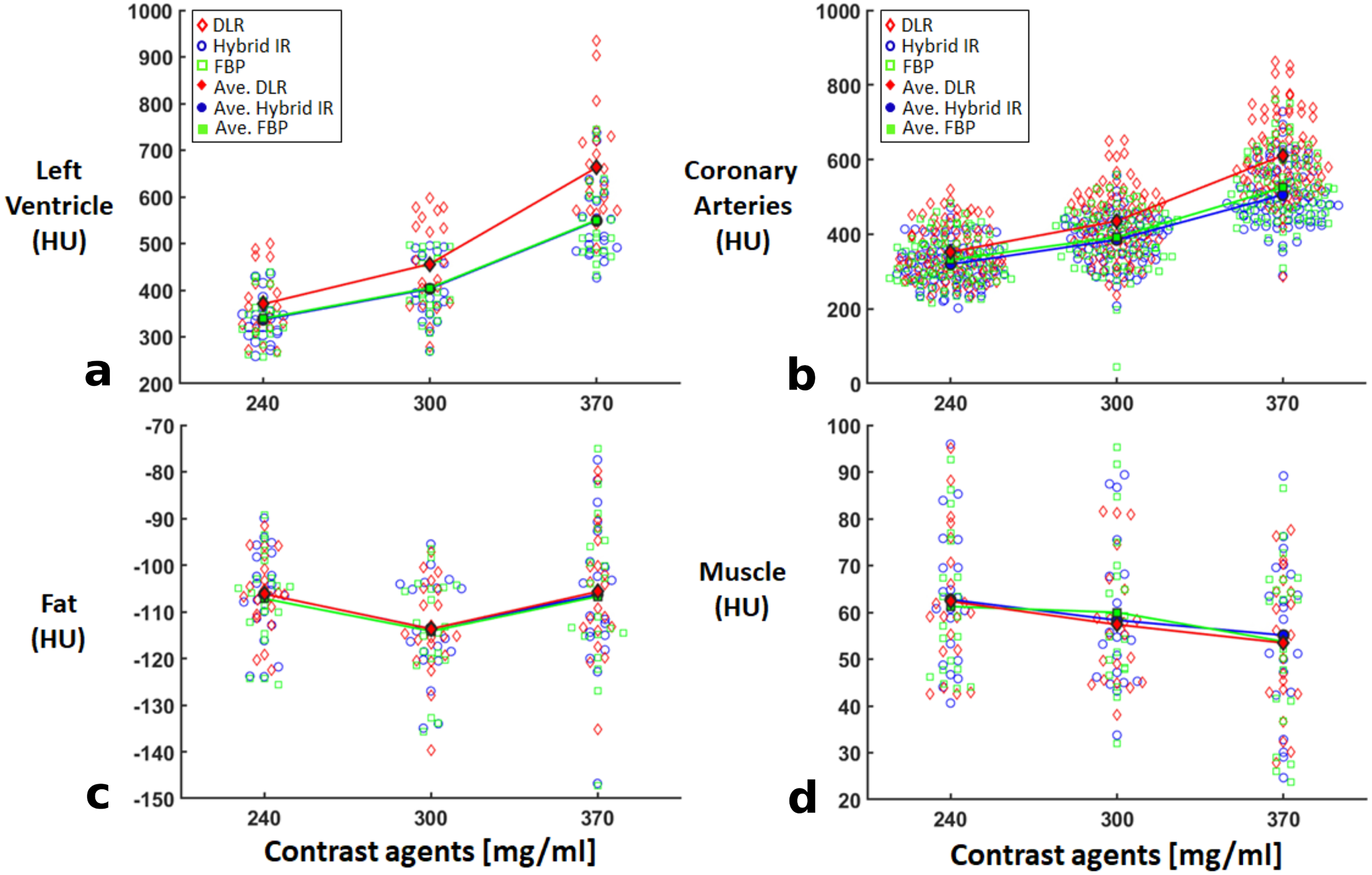
CT attenuation results among different iodine concentrations. The mean CT attenuation value of the (a) left ventricle, (b) coronary arteries, (c) fat, and (d) muscle were comparable among different image reconstructions (green square = FBP; blue circle = hybrid IR; red diamond = DLR) and iodine concentrations. Post-hoc Tukey's test resulted in a difference between each group in all three iodine concentrations of contrast media (FBP vs. DLR, P < 0.001; hybrid IR vs. DLR, P < 0.001). For better representation, the comparison of the mean CT attenuation with different image reconstructions is illustrated by the solid line between different iodine concentrations. CT, computed tomography; DLR, deep learning reconstruction; FBP, filtered back projection; IR, iterative reconstruction.
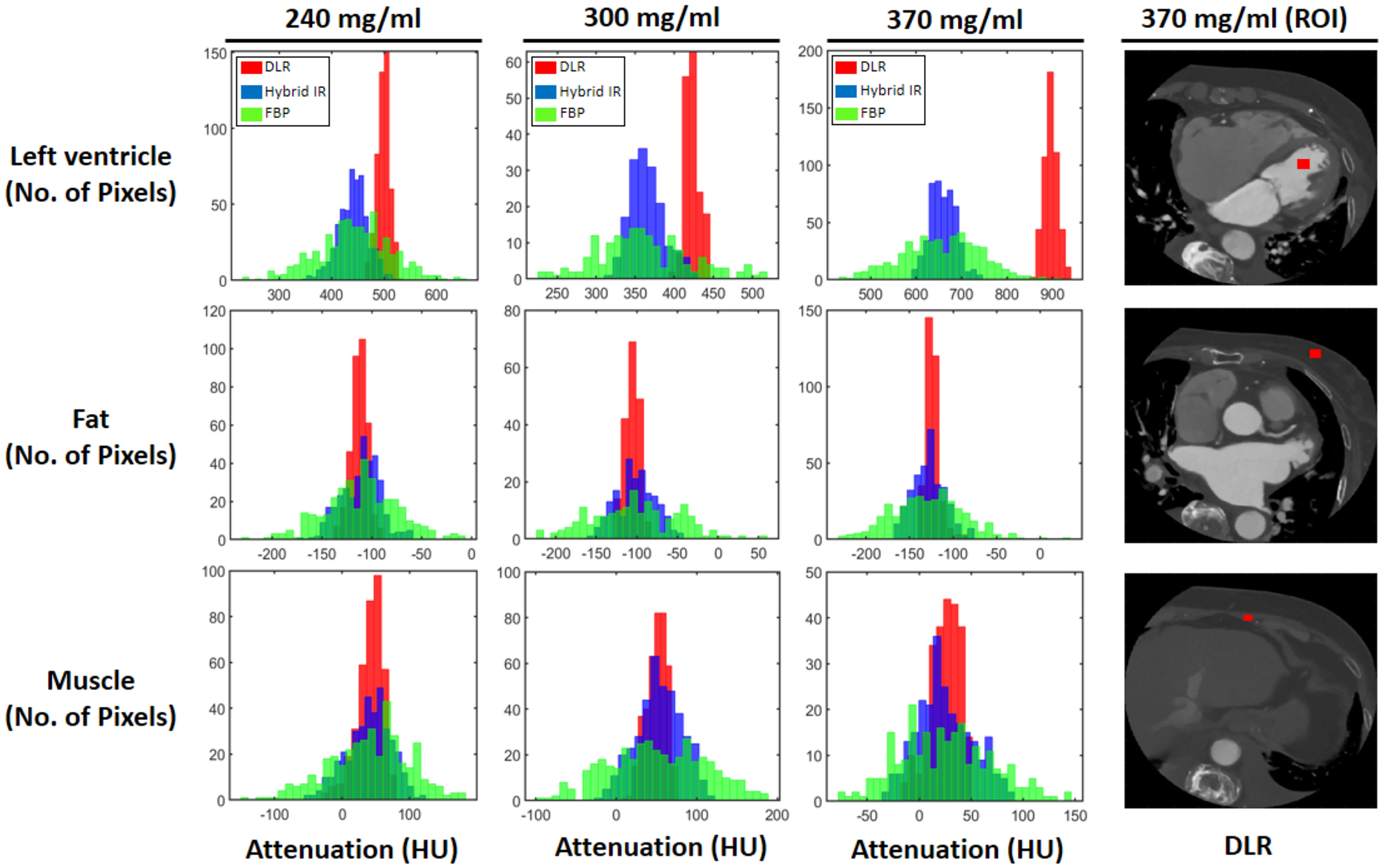
Histogram plots with different image reconstructions at various iodine concentrations (iohexol-370, iohexol-300, and iohexol-240). CT attenuation was measured by placing a circular ROI (red square) in the muscle, fat, and left ventricle in axial coronary CTA (representing CTA image, reconstructed with DLR at Iohexol-370, right column). The histogram plots of the left ventricle show a narrow width and shift to the right in DLR (red color) at different iodine concentrations compared with images reconstructed with FBP (green color) and hybrid IR (blue color). The distribution of attenuation in the fat and muscle was maintained for all image reconstructions at different iodine concentrations. Furthermore, a narrower DLR distribution indicates its lower variability in image noise and CT attenuation compared with FBP and hybrid IR. Notably, DLR particularly boosted CT attenuation in the left ventricle and coronary arteries compared to fat and muscle. CTA, computed tomography angiography; DLR, deep learning reconstruction; FBP, filtered back projection; IR, iterative reconstruction; ROI, region of interest.
CT attenuation results at different iodine concentrations.
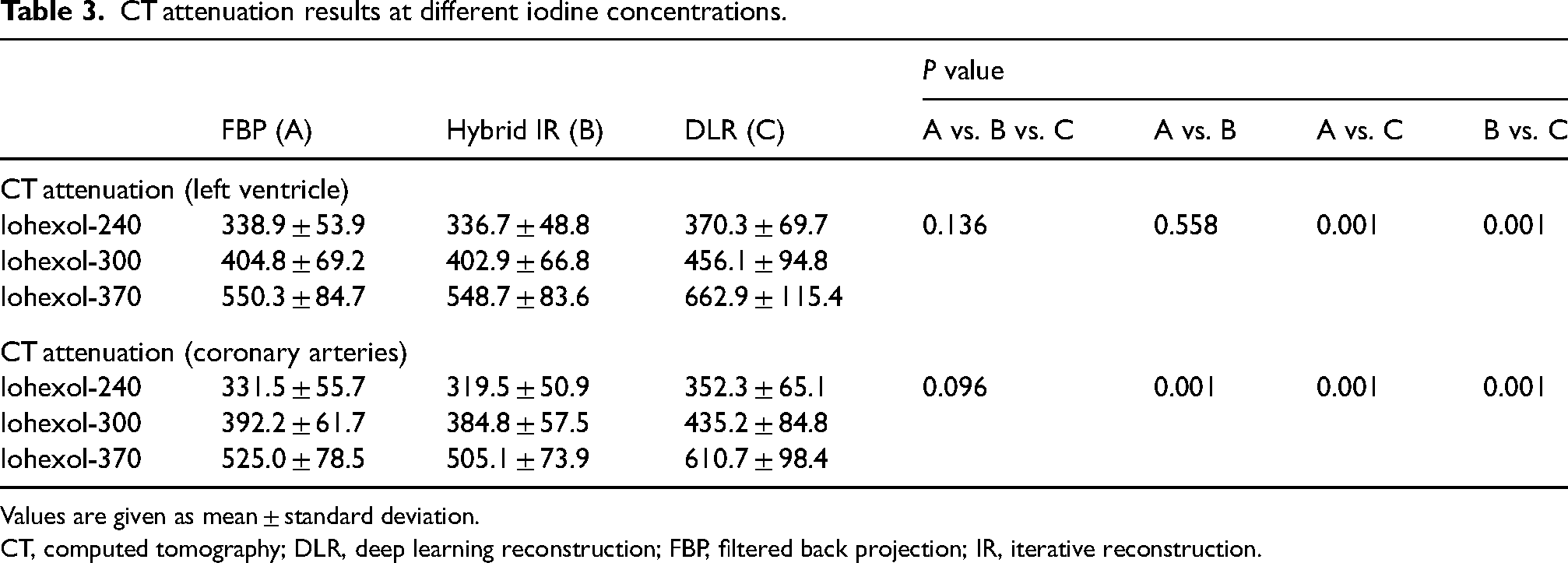
Values are given as mean ± standard deviation.
CT, computed tomography; DLR, deep learning reconstruction; FBP, filtered back projection; IR, iterative reconstruction.
Comparison of CT attenuation among different iodine concentrations.
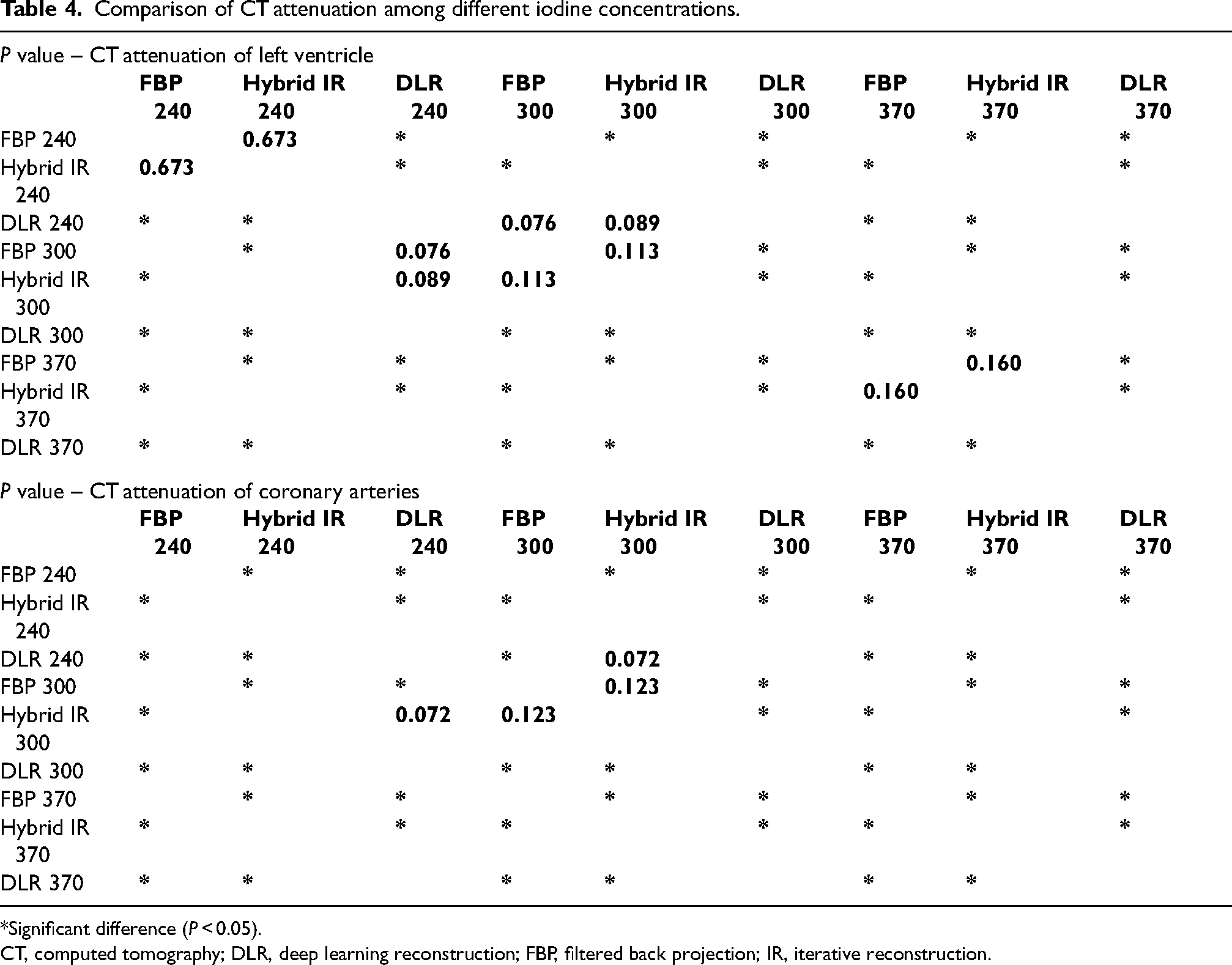
*Significant difference (P < 0.05).
CT, computed tomography; DLR, deep learning reconstruction; FBP, filtered back projection; IR, iterative reconstruction.
SNR and CNR: Iohexol-370 versus Iohexol-300 versus Iohexol-240
Fig. 3 presents the bar graph results of the SNR and CNR in the left ventricle and coronary arteries among the different iodine concentrations (green = FBP; blue = hybrid IR; red = DLR). The SNR and CNR in the left ventricle and coronary arteries were significantly higher in DLR compared with FBP and hybrid IR among different iodine concentrations (P < 0.001).
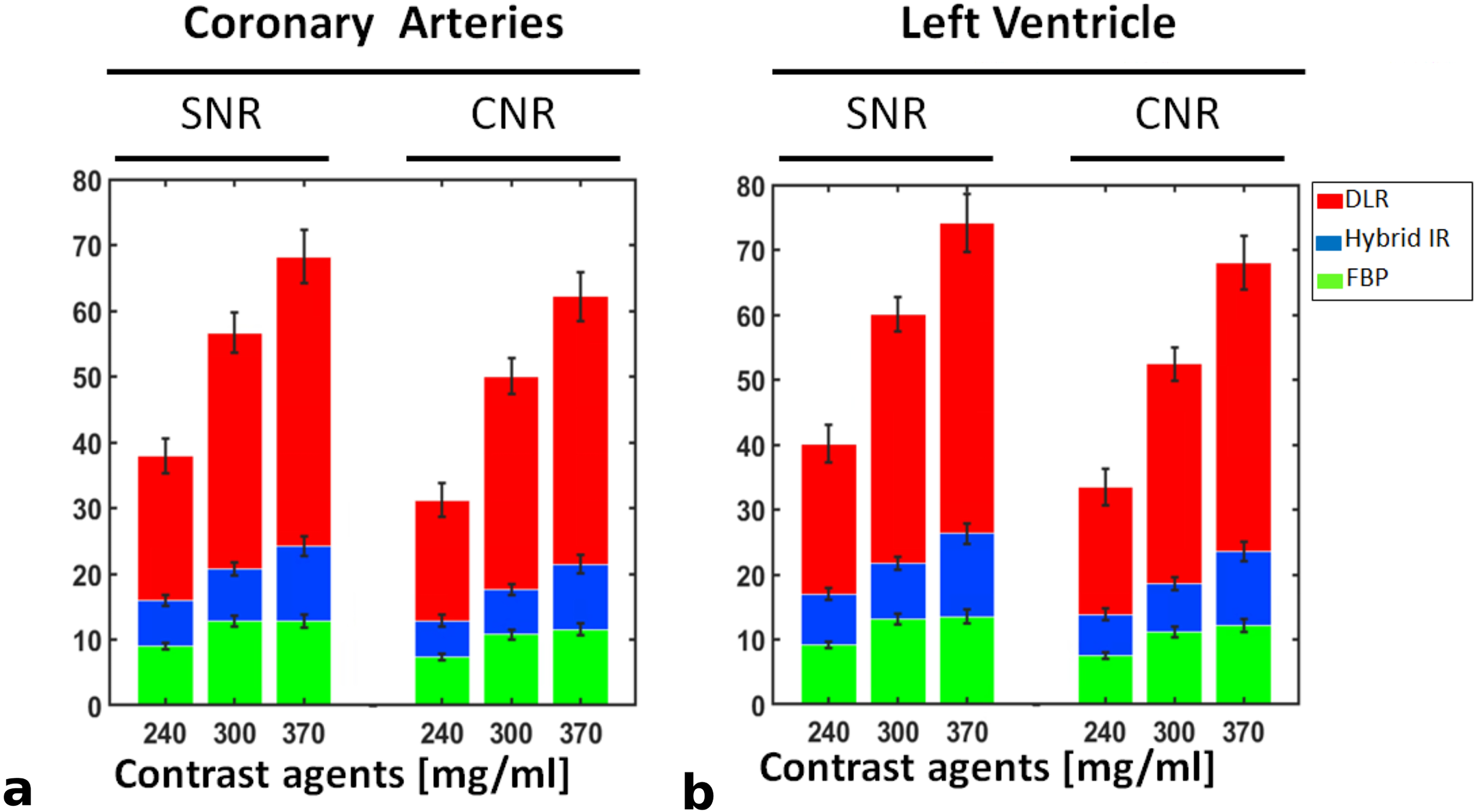
The results of CNR and SNR. SNR and CNR in the (a) coronary arteries and (b) left ventricle were significantly higher in DLR (red color) than in FBP (green color) and hybrid IR (blue color) at all concentrations. In particular, DLR with the lowest iodine concentration resulted in significantly higher SNR and CNR compared with FBP and hybrid IR with the highest iodine concentration. The length of the error bars represents the SEM. CNR, contrast-to-noise ratio; DLR, deep learning reconstruction; FBP, filtered back projection; IR, iterative reconstruction; SEM, standard error of the mean; SNR, signal-to-noise ratio.
Subjective analysis: Iohexol-370 versus Iohexol-300 versus Iohexol-240
Table 5 summarizes the subjective image analysis scores (overall image quality, artifacts, and image noise) for image reconstructions with different iodine concentrations. The subjective analysis scores for DLR were significantly higher than those of FBP and hybrid IR with Iohexol-370, Iohexol-300, and Iohexol-240 (P < 0.001). DLR was rated acceptable for image quality with minor artifacts and below-average image noise compared with FBP and hybrid IR for all iodine concentrations. The inter-observer agreement for the image quality between two observers was substantial (k = 0.69).
Results of subjective image analysis.
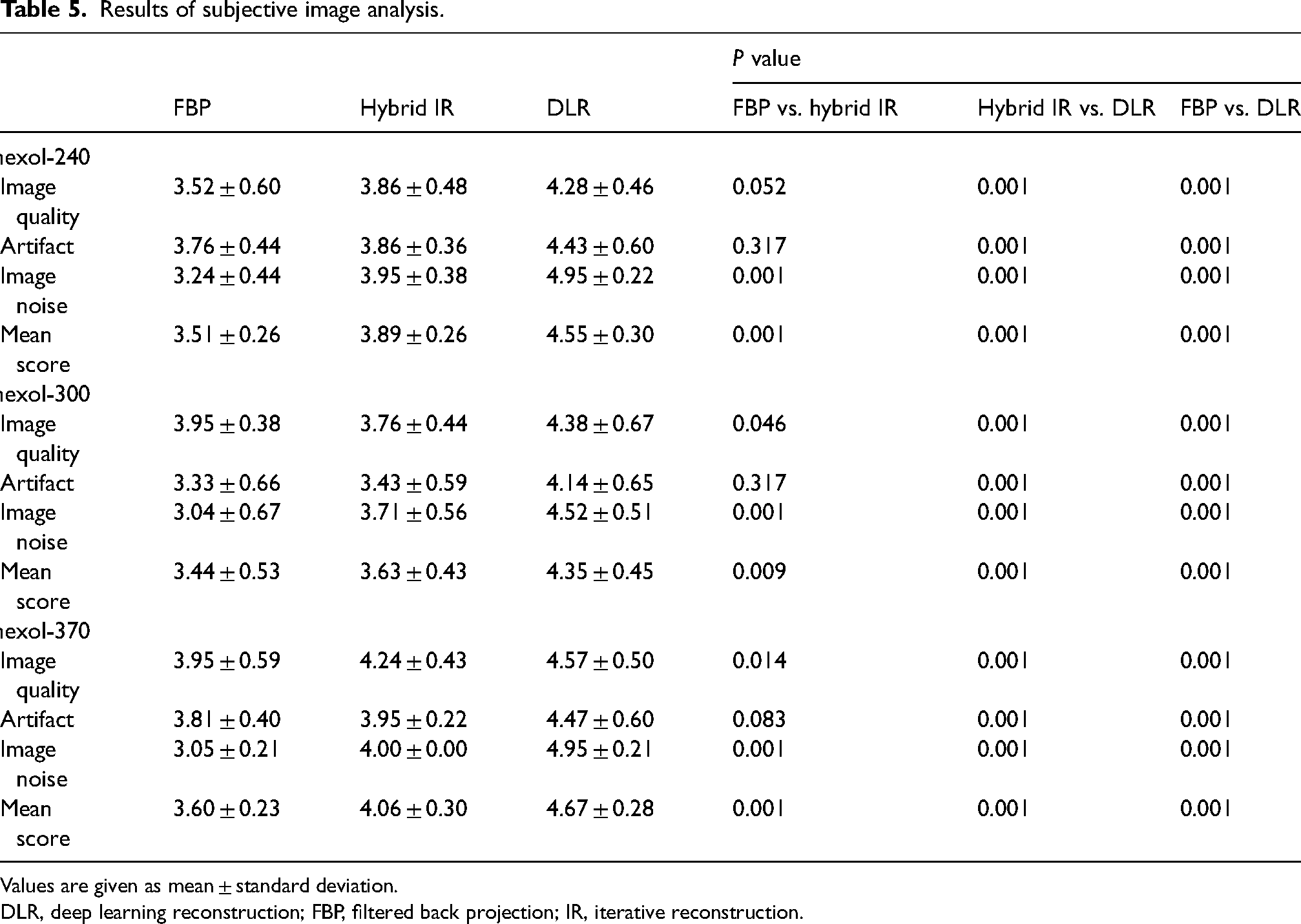
Values are given as mean ± standard deviation.
DLR, deep learning reconstruction; FBP, filtered back projection; IR, iterative reconstruction.
CT attenuation: DLR at Iohexol-300 versus hybrid IR for Iohexol-240
The CT attenuation values in the left ventricle were not significantly different between hybrid IR with Iohexol-300 and DLR with Iohexol-240 (P = 0.089). Moreover, CT attenuation of the coronary arteries was equivalent between hybrid IR with Iohexol-300 and DLR with Iohexol-240 (P = 0.072). Fig. 4 shows an example of coronary CTA image reconstructed with hybrid IR and DLR with the administration of Iohexol-300 and Iohexol-240 contrast media.
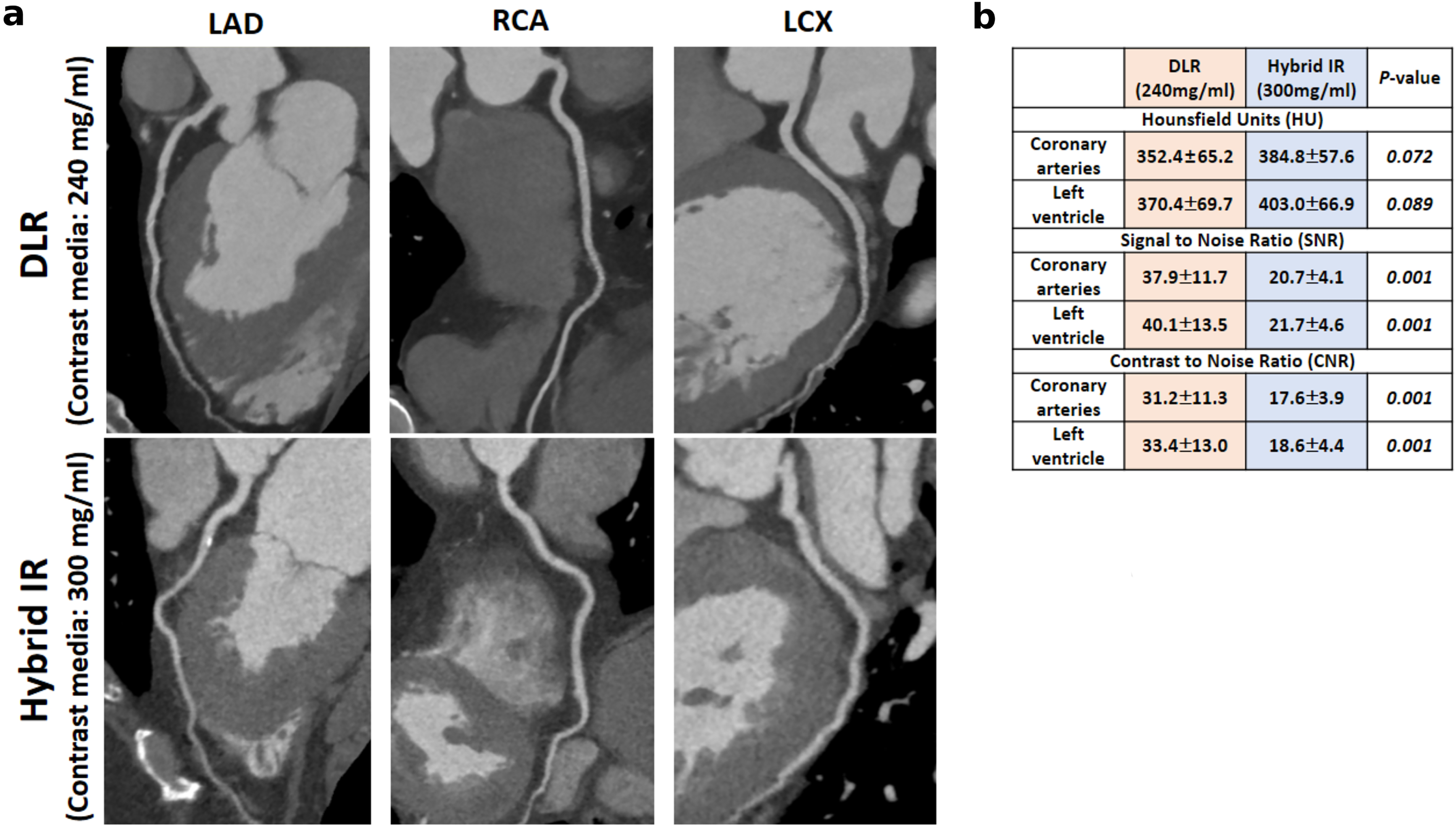
Visualization of coronary arteries by hybrid IR with Iohexol-300 and DLR with Iohexol-240. (a) For the vessel wall delineation, DLR with Iohexol-240 was scored as very good, while hybrid IR with Iohexol-300 was rated as good (P < 0.001). (b) DLR with lower iodine concentration (Iohexol-240) obtained comparable CT attenuation to hybrid IR with Iohexol-300, whereas higher SNR and CNR were found using DLR. CNR, contrast-to-noise ratio; CT, computed tomography; DLR, deep learning reconstruction; FBP, filtered back projection; IR, iterative reconstruction; SEM, standard error of the mean; SNR, signal-to-noise ratio.
SNR and CNR: DLR at Iohexol-300 versus hybrid IR for Iohexol-240
Although there was no significant difference in the CT attenuation of the left ventricle and coronary arteries between hybrid IR with Iohexol-300 and DLR with Iohexol-240, we discovered that application of DLR with Iohexol-240 significantly improved SNR and CNR in the left ventricle (40.1 ± 13.4 and 33.4 ± 12.9) and coronary arteries (37.9 ± 11.6 and 31.2 ± 11.3) compared with hybrid IR with Iohexol-300 (21.7 ± 4.6; 18.58 ± 4.4 and 20.73 ± 4.08; 17.6 ± 3.8, respectively; P < 0.001) (Fig. 4).
Subjective analysis: DLR at Iohexol-300 versus hybrid IR for Iohexol-240
Besides rating the overall image quality, artifacts, and image noise for image reconstructions at different iodine concentrations, the vessel wall delineation was rated between the results of hybrid IR with Iohexol-300 and DLR with Iohexol-240. The vessel wall delineation is notably higher for DLR with Iohexol-240 groups (score 5 = 8.7%; score 4 = 66.3%; score 3 = 21%; score 2 = 4%) compared with hybrid IR with Iohexol-300 (score 5 = 6.0%; score 4 = 51.3%; score 3 = 38.34%; score 2 = 4.3%), resulting in good vessel wall definition, as shown in Fig. 5. The inter-observer agreement for the visualization of the coronary artery delineation between two observers was substantial (k = 0.76).
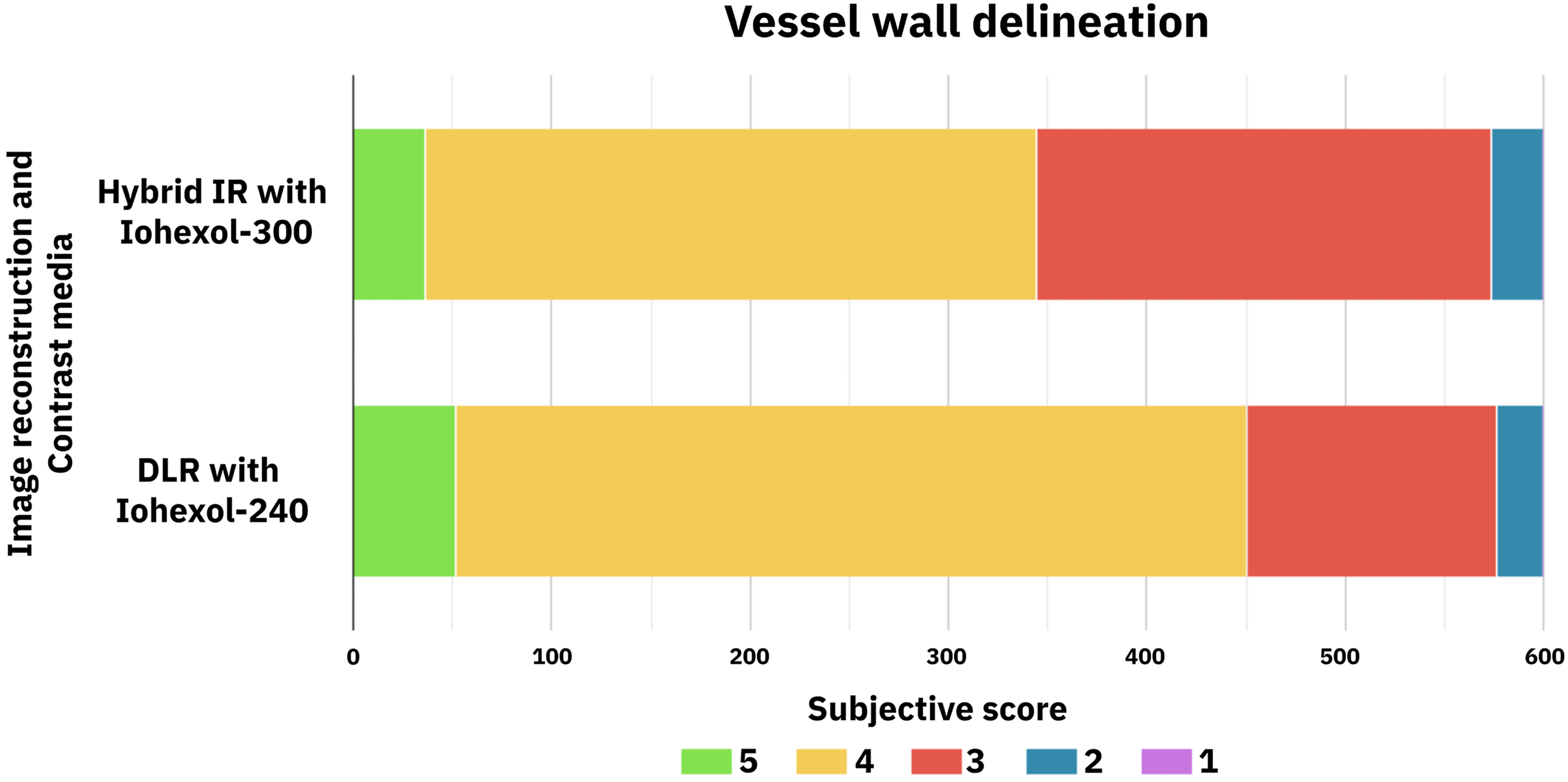
Subjective image analysis scores between DLR with Iohexol-240 and hybrid IR with Iohexol-300. The coronary arteries were divided into 15 segments, and the vessel wall delineation was rated on a 5-point Likert scale. DLR with Iohexol-240 achieved higher subjective analysis scores for vessel wall delineation compared with hybrid IR with Iohexol-300. DLR, deep learning reconstruction; IR, iterative reconstruction.
Discussion
This study investigated the influence of three different image reconstructions (FBP, hybrid IR, and DLR) on different contrast media iodine concentrations (Iohexol-370, Iohexol-300, and Iohexol-240) in coronary CTA. The mean CT attenuation values of the left ventricle and coronary arteries were significantly higher for DLR compared with FBP and hybrid IR regardless of iodine concentration. In addition, SNR, CNR, and subjective image analysis showed the best results for DLR at all iodine concentrations. In particular, we observed that using DLR with lower iodine concentration (Iohexol-240) yielded comparable CT attenuation to hybrid IR with Iohexol-300, whereas higher SNR, CNR, and subjective analysis scores were found for DLR.
Contrast enhancement in CTA can be effectively achieved with a higher injection rate of contrast media at a lower concentration. Lubbers et al. (26) assessed the intraluminal opacification and image quality between Iodixanol 270 (iso-osmolar contrast media, injection rate 5.6 mL/s) and Iopromide 300 (low-osmolar contrast media, injection rate 5.0 mL/s or 5.8 mL/s) contrast media. They reported that less heat discomfort was associated with the administration of iso-osmolar contrast media at a higher injection rate. Similarly, Mihl et al. (6) concluded that the use of low-iodine-concentration contrast media (contrast media 240 mg/mL at 9 mL/s) with high flow demonstrated no significant differences in the attenuation of coronary arteries compared with contrast media 300 mg/mL at 7.2 mL/s. Consequently, there were no significant differences in the attenuation of the left ventricle and coronary arteries with the administration of Iohexol-240 contrast media for DLR and Iohexol-300 contrast media for hybrid IR at the same flow rate. Additionally, DLR with Iohexol-240 showed better results for SNR, CNR, and subjective image analysis compared with hybrid IR with Iohexol-300. Therefore, DLR is more advantageous to patients with impaired renal function as it requires the administration of lower-iodine-concentration contrast media without increasing the injection rate.
We compared the image quality of coronary CTA among FBP, hybrid IR, and DLR using image noise, SNR, CNR, and subjective image analysis. Previous studies concluded that the image quality of coronary CTA was significantly higher for DLR, with lower image noise, higher SNR, higher CNR, and sharper images compared with FBP and hybrid IR (17). In this study, we investigated the image quality between different image reconstructions besides the administration of various iodine concentrations of contrast media. As shown in Fig. 3, that application of DLR at different iodine concentrations resulted in superior image quality, including higher CNR, higher SNR, and less image noise compared with hybrid IR and FBP. Although DLR at the lowest iodine concentration (Iohexol-240) resulted in significantly lower CT attenuation in the coronary arteries compared with hybrid IR (Iohexol-370), DLR showed better image quality in terms of SNR, CNR, and subjective analysis. This pattern was confirmed by a marked reduction of image noise with DLR at different iodine concentrations compared to FBP and hybrid IR, which led to improved SNR and CNR. Based on the results of this study, the administration of low-iodine-concentration contrast media (Iohexol-240) with an increase in flow rate of contrast media in DLR could achieve comparable CT attenuation to higher-iodine-concentration (Iohexol-370) hybrid IR. We believe this clear contrast enhancement in the left ventricle and coronary arteries with DLR is due to the advanced MBIR training images. Several studies have shown a marked improvement of vascular contrast enhancement with MBIR compared with FBP and IRs (22,27).
Previous studies investigated low tube voltage protocols to achieve better CT attenuation with lower radiation dose. However, this method is not appropriate for larger patient datasets (28). Moreover, the presence of calcification in the vessels and higher blooming artifacts caused blurring of the coronary vessels, which led to misdiagnosis and streak artifacts in the low tube voltage (28,29). This study demonstrated that DLR with the lowest iodine concentration (Iohexol-240) resulted in significantly higher SNR and CNR compared with hybrid IR with the highest iodine concentration (Iohexol-370) at the same flow rate and tube voltage. Furthermore, it has been reported that DLR provides lower image noise at lower tube voltage (30). In addition, the blooming artifact reduction is significantly improved with DLR compared with FBP and hybrid IR (21). These advantages could be applied to DLR with a lower radiation dose scanning protocol. In addition, the contrast enhancement boost is a newly introduced technique designed to improve the strength of contrast enhancement. This technique has been applied to the visualization of Type-II endoleaks in abdominal CTA (31). The diagnostic value of CTA directly depends on the degree of vascular enhancement (32). Thus, further work is required to investigate the effect of the contrast enhancement boost technique on various iodine concentrations of contrast media with DLR in coronary CTA.
The present study has some limitations. First, we did not assess hemodynamic changes (heart rate, blood pressure, and patient discomfort) during the administration of contrast media. The injection rate of contrast media was the same for all iodine concentrations. Previous studies examined pain, heat, and discomfort with higher flow rate and iodine concentrations of contrast media (26). Nevertheless, patients with renal impairment who receive lower iodine concentrations would experience less discomfort and toxicity. Second, this is a single-center study with a small sample size. Further studies are required to evaluate the diagnostic performance among various iodine concentrations with DLR. Third, all investigations were only performed on Aquilion ONE Prism CT vendor. The effect of various image reconstructions with different kernels and options for image quality could be different depending on the CT vendor, and this may have affected the results of this study.
In conclusion, we suggest that using DLR with Iohexol-240 contrast media is preferred over hybrid IR with Iohexol-300 contrast media in coronary CTA.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JKR and HJS are employees of Canon Medical Systems Korea, Seoul, Republic of Korea (the subsidiary in Korea of Canon Medical Systems Corporation, Otawara-si, Japan).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Korea Medical Device Development Fund grant funded by the Korea government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health & Welfare, the Ministry of Food and Drug Safety) (project no. 1711139017).