
Abstract
Background
The deep learning (DL)-based reconstruction algorithm reduces noise in magnetic resonance imaging (MRI), thereby enabling faster MRI acquisition.
Purpose
To compare the image quality and diagnostic performance of conventional turbo spin-echo (TSE) T2-weighted (T2W) imaging with DL-accelerated sagittal T2W imaging in the female pelvic cavity.
Methods
This study evaluated 149 consecutive female pelvic MRI examinations, including conventional T2W imaging with TSE (acquisition time = 2:59) and DL-accelerated T2W imaging with breath hold (DL-BH) (1:05 [0:14 × 3 breath-holds]) in the sagittal plane. In 294 randomly ordered sagittal T2W images, two radiologists independently assessed image quality (sharpness, subjective noise, artifacts, and overall image quality), made a diagnosis for uterine leiomyomas, and scored diagnostic confidence. For the uterus and piriformis muscle, quantitative imaging analysis was also performed. Wilcoxon signed rank tests were used to compare the two sets of T2W images.
Results
In the qualitative analysis, DL-BH showed similar or significantly higher scores for all features than conventional T2W imaging (P <0.05). In the quantitative analysis, the noise in the uterus was lower in DL-BH, but the noise in the muscle was lower in conventional T2W imaging. In the uterus and muscle, the signal-to-noise ratio was significantly lower in DL-BH than in conventional T2W imaging (P <0.001). The diagnostic performance of the two sets of T2W images was not different for uterine leiomyoma.
Conclusions
DL-accelerated sagittal T2W imaging obtained with three breath-holds demonstrated superior or comparable image quality to conventional T2W imaging with no significant difference in diagnostic performance for uterine leiomyomas.
Keywords
Introduction
Many different benign and malignant diseases arise in the uterus. Although ultrasonography is a common and easily accessible imaging modality for the original evaluation of the female pelvic organs, magnetic resonance imaging (MRI) is a problem-solving tool for the diagnosis of abnormal findings detected on ultrasonography (1,2). Leiomyoma in the uterus is a frequent finding, with a prevalence of 4.5%–68.6% in women of reproductive age (3,4). MRI can provide information such as the number, location, and size of leiomyomas for treatment planning (5–7). Furthermore, because leiomyomas have characteristic MRI features, they can be differentiated from other lesions on MRI.
Despite the benefits of functional imaging, such as diffusion-weighted imaging (DWI), T2-weighted (T2W) imaging is the basic sequence for evaluating gynecologic disease. It is recommended to obtain T2W imaging in at least two orientations, including the sagittal plane (8,9). Sagittal T2W imaging is particularly useful for determining the anatomical relationship of the pelvic organs and the location of lesions in the uterus or ovary. Turbo spin-echo (TSE) is one of the most commonly used sequences to perform T2W imaging. Although half Fourier single-shot turbo spin-echo (HASTE) is faster than TSE for acquiring T2W images, TSE has been preferred due to image contrast, anatomic sharpness, and overall image quality (10–12). Therefore, a shorter acquisition time for TSE while retaining image quality may benefit patients.
Deep learning has recently received much attention in the field of radiology. Aside from deep learning algorithms for detecting lesions or assisting in diagnosis, deep learning reconstruction (DLR) is used to reduce noise within the image reconstruction process, which results in faster MRI acquisition or improved image quality. DLR algorithms have been applied to various MRI sequences, such as T2W imaging and DWI (13–16). Breathing generates motion artifacts and lowers image quality in abdominal MRI. As a result, some studies have investigated the effect of a shorter acquisition time with DLR on image quality of T2W imaging in upper abdominal organs such as the liver and pancreas (17,18). Although a few studies have used DLR with female pelvic organs, diagnostic performance was not assessed (19,20). The purpose of this study was to compare the image quality and diagnostic performance of conventional TSE T2W imaging with DL-accelerated sagittal T2W imaging in the female pelvic cavity.
Material and Methods
Participants
The institutional review board of our hospital approved this study. The need for informed consent was waived due to the retrospective design of the study.
In this single-center study, 236 consecutive female patients who underwent pelvic MRI between March and August 2021 were eligible for inclusion. After excluding 67 MRI examinations lacking accelerated T2W imaging and 20 patients who had a hysterectomy, 149 patients were included in this study (Fig. 1). We gathered clinical information such as age and the reason for the MRI examination.

Flow chart of patient enrollment.
MRI acquisition
All MRI examinations were performed using clinical 3-T scanners (MAGNETOM Vida; Siemens Healthcare, Erlangen, Germany) with a 30-channel body coil and a 32- or 72-channel spine coil. For patients without absolute contraindication, an anti-spasmolytic agent (Buscopan; Boehringer Ingelheim, Germany) was given intramuscularly. The MRI protocol comprised axial, coronal, and sagittal T2W imaging, axial T1-weighted (T1W) imaging, DWI, and dynamic contrast-enhanced axial and sagittal T1W imaging. Generalized autocalibrating partially parallel acquisitions (GRAPPA) with an acceleration factor of 2 was applied for the conventional sagittal TSE T2W imaging, which was considered the gold standard (acquisition time: 2 min 59 s). DL-accelerated sagittal T2W images, termed DL-BH, were obtained with an acceleration factor of 4 using breath-hold for a net acquisition time of 1 min 5 s (three breath-holds of 14 s each). The employed DLR research application was based on an unrolled variational network and is detailed in previous publications (13,14,21,22). DLR training data were not collected from our institution. Table 1 summarizes the detailed parameters of the two sets of sagittal T2W images. The parameters were set before patient enrollment. Fig. 2 depicts images from two representative cases.
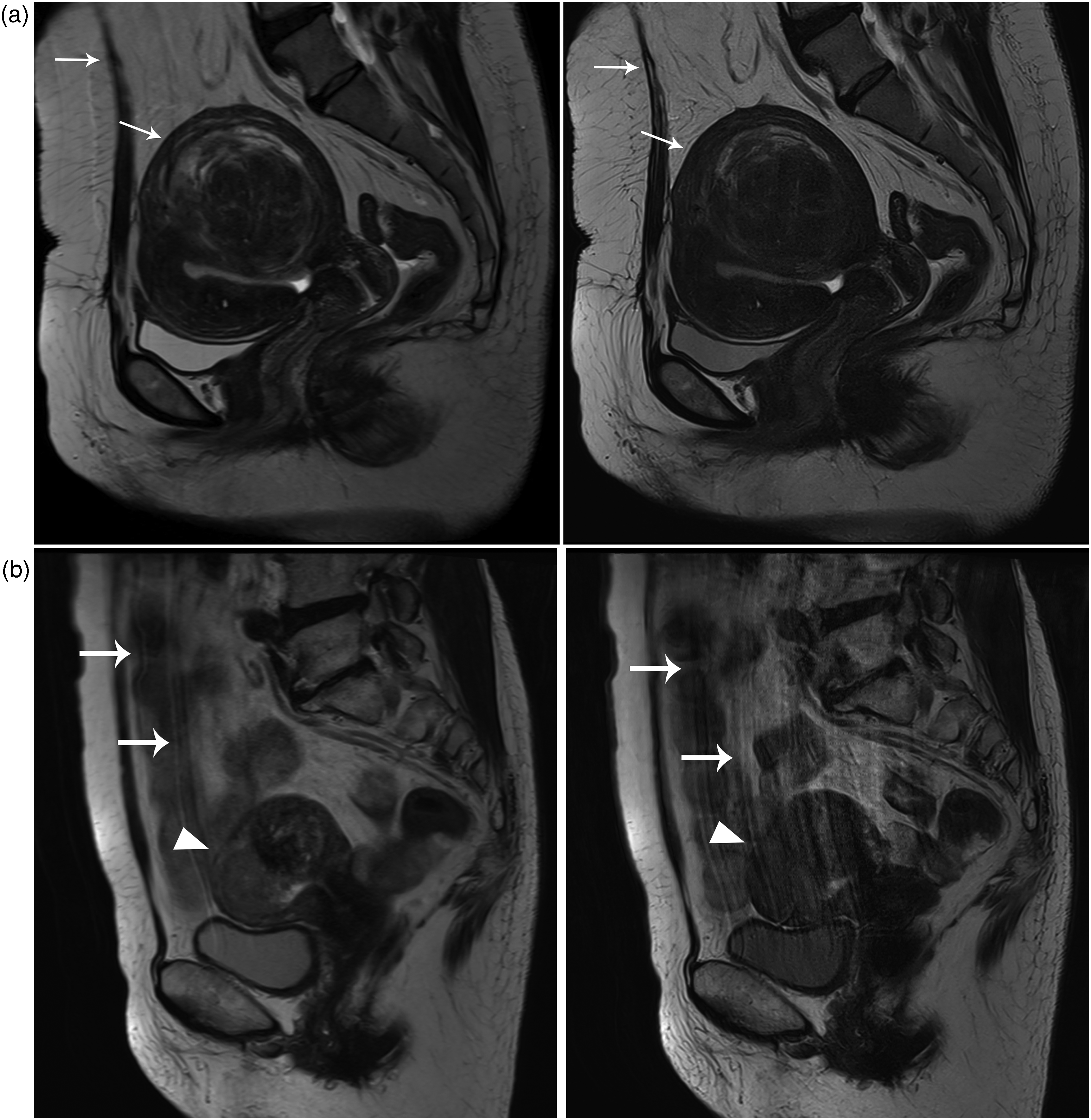
Representative cases of two different patients with (left) conventional T2W imaging and (right) DL-BH. (a) The borders of the abdominal wall and the uterus are slightly blurred (arrows) in conventional T2W imaging. The abdominal wall and the uterus have the sharp border (arrows) in DL-BH. (b) In conventional T2W imaging, the borders of the abdominal wall, bowel, and uterus are blurred with ghosting artifacts (arrows) parallel to the abdominal wall, but the uterine mass (arrowhead) is well-delineated. Multiple fine lines (ghosting artifacts) parallel to the abdominal wall (arrows) impact the signal intensity of the uterus, resulting in a blurred margin uterine mass (arrowhead) in DL-BH. BH, breath-hold; DL, deep learning; T2W, T2-weighted.
Image acquisition parameters of sagittal T2-weighted imaging of the uterus.
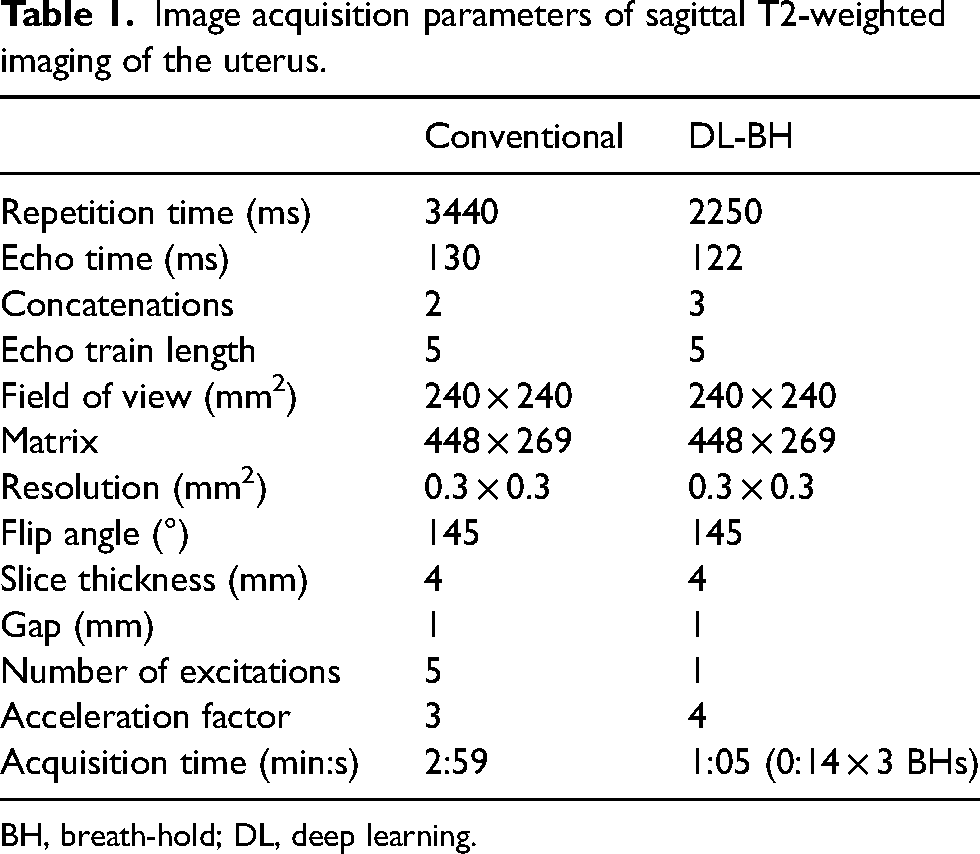
BH, breath-hold; DL, deep learning.
Image analysis
Two radiologists, with 13 and 8 years of expertise, respectively, independently reviewed the images without knowing the clinical information or the name of the sequence. Anonymized T2W imaging data from 149 patients totaled 298 sets, which were arranged in a random order. They evaluated the uterus for the existence of leiomyoma. The gold standard for the presence of uterine leiomyoma was determined by a consensus reading of the two radiologists for discordant cases after individual review. Furthermore, they graded their diagnostic confidence using a 5-point scale ranging from 1 (not at all confident) to 5 (very confident).
The radiologists conducted qualitative analysis to evaluate the four features of image quality using a 5-point scale: 5 = excellent; 4 = good; 3 = fair; 2 = poor; and 1 = non-diagnostic. For the sharpness of the uterus, a score of 1 indicates very severe blurring, while a score of 5 indicates a sharp boundary without blurring. A higher score for artifacts and subjective noise indicates fewer artifacts or less noise. The radiologists were provided with sample images for each score (Supplementary Fig. 1). The overall image quality was subjectively rated using the same 5-point scale.
A quantitative analysis was also performed by two radiologists. They reviewed the two sets of T2W images together and selected the best images to represent the uterus and piriformis muscle. They drew regions of interest (ROIs) in the uterus and piriformis muscle on conventional T2W images and replicated the ROIs to DL-BH images. The average signal intensity (SI) and standard deviation (SD), which were regarded as noise, were recorded for the uterus and muscle. Signal-to-noise ratios (SNRs) of the uterus and muscle were calculated as the average SI/SD in each organ. The contrast-to-noise ratio (CNR) of the uterus was computed as follows: (average SI of the uterus –average SI of the muscle)/SD of the muscle. We calculated CNR using the SD of the piriformis muscle because noise in the air, a typical reference of noise, was not reliable on images using DLR.
Statistical analysis
In the qualitative and quantitative analyses, we used the intraclass correlation coefficient (ICC) to assess inter-reader agreement. The ICC values were interpreted as follows: <0.5 = poor; 0.5–0.75 = moderate; 0.75–0.9 = good; and >0.9 = excellent agreement. The results of radiologist 1, who had more experience, were used for the quantitative analysis. The Kolmogorov‒Smirnov test was used to determine the normality of the variables. Non-parametric analyses were used since all variables were not normally distributed. Differences in parameters between the two sets of T2W images were examined using Wilcoxon signed rank tests. The differences in parameters between the images are shown by box-and-whisker plots. Using a visual grading characteristics (VGC) analysis, the ratings of overall image quality were compared between conventional T2W imaging and accelerated T2W imaging (23,24). A VGC curve was plotted with conventional T2W imaging on the x-axis and accelerated T2W imaging on the y-axis. An area under the curve (AUC) of 0.5 implies that no image is superior to another.
The diagnostic performance of each radiologist in detecting uterine leiomyoma was evaluated with sensitivity and specificity and compared between two sets of T2W images using McNemar's test. A P value <0.05 was considered statistically significant. SPSS version 23.0 (IBM Corp., Armonk, NY, USA) and GraphPad Prism version 8.0 (GraphPad Software, Inc., La Jolla, CA, USA) were used for statistical analyses.
Results
The median age of the 149 patients was 41 years (interquartile range = 35–46 years). The majority of patients underwent MRI to evaluate a uterine mass (83.9%) followed by an ovarian mass (8.7%) and cervical cancer (6.0%).
Among the qualitative analytical parameters, artifacts and overall image quality on DL-BH had the highest ICCs of 0.839 and 0.832, respectively (Table 2). ICCs for subjective noise and sharpness showed poor to moderate agreement. Mean muscle SI showed excellent agreement in the quantitative analysis, whereas most other parameters showed moderate to good agreement.
Inter-reader agreement between two radiologists on two sets of sagittal T2-weighted images.
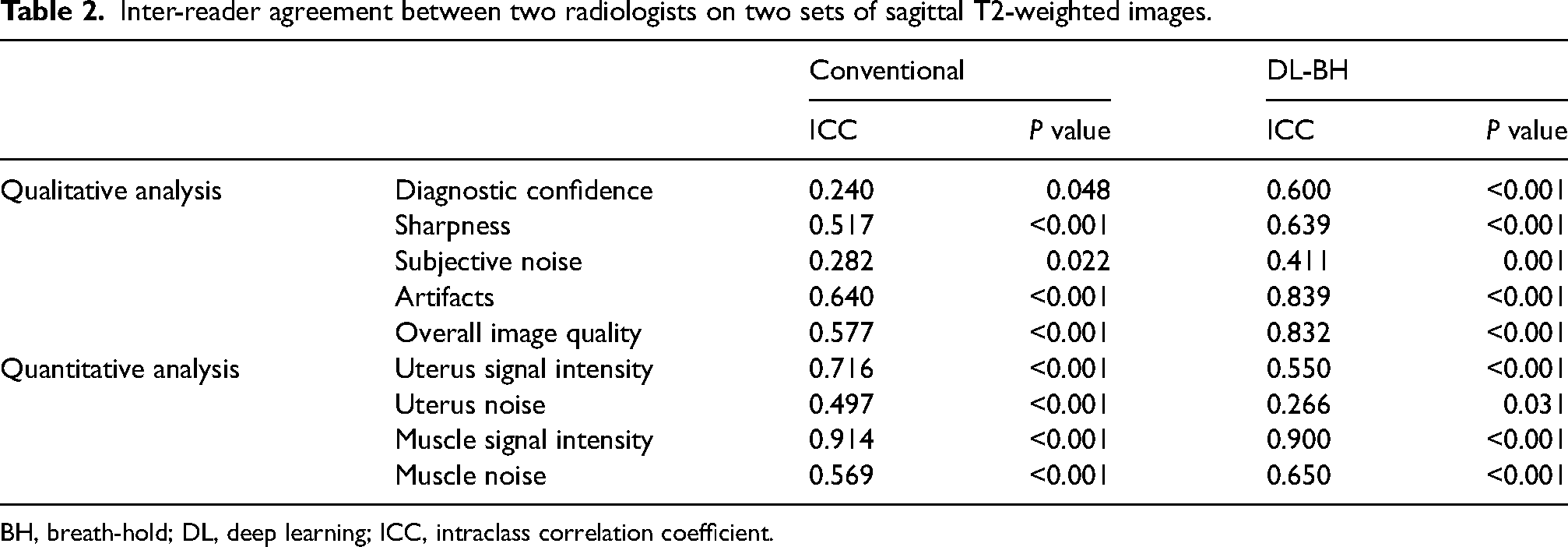
BH, breath-hold; DL, deep learning; ICC, intraclass correlation coefficient.
Radiologist 2 gave the significantly higher diagnostic confidence score for DL-BH than conventional T2W imaging (Fig. 3). The sharpness of the anatomical structure for DL-BH was significantly greater than that for conventional T2W imaging. Radiologist 1 assigned the higher subjective noise score to conventional T2W imaging, and radiologist 2 assigned the higher score to DL-BH, with statistically significant differences from other images. Despite a statistically significant difference compared with conventional T2W imaging only noted by radiologist 2, artifacts and overall image quality received the higher score for DL-BH from both radiologists. In terms of overall image quality, both radiologists commonly preferred DL-BH over conventional T2W imaging according to the VGC curves (Fig. 4).

Qualitative image quality comparison between two sets of sagittal T2-weighted images by (a) radiologist 1 and (b) radiologist 2.

VGC curves for overall image quality assessment between conventional and accelerated T2W imaging. T2W, T2-weighted; VGC, visual grading characteristics.
The mean signal intensities of the uterus and piriformis muscle in DL-BH were substantially lower than those in conventional T2W imaging (P <0.001) (Table 3). Noise was significantly less in the uterus but greater in the muscle on DL-BH than on standard T2W imaging (P <0.001). Conventional T2W imaging showed a significantly higher SNR in both the uterus and muscle, as well as a higher CNR, than DL-BH (P <0.001).
Quantitative analysis in two sets of T2-weighted images.
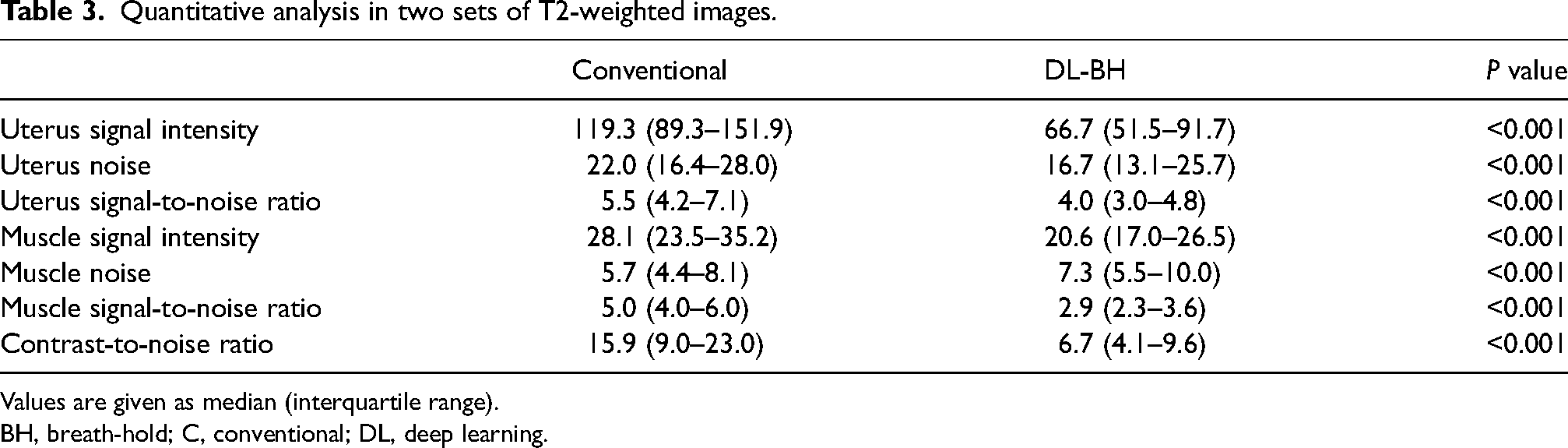
Values are given as median (interquartile range).
BH, breath-hold; C, conventional; DL, deep learning.
Uterine leiomyoma was present in 112 patients and absent in 37 patients. The two radiologists’ diagnostic performance for uterine leiomyoma on the DL-BH were comparable to conventional T2W imaging (P = 0.267 and >0.999 for radiologists 1 and 2, respectively). The two radiologists showed an accuracy >90% on both T2W images (Table 4).
Diagnostic performance on sagittal T2-weighted imaging for uterine leiomyomas.
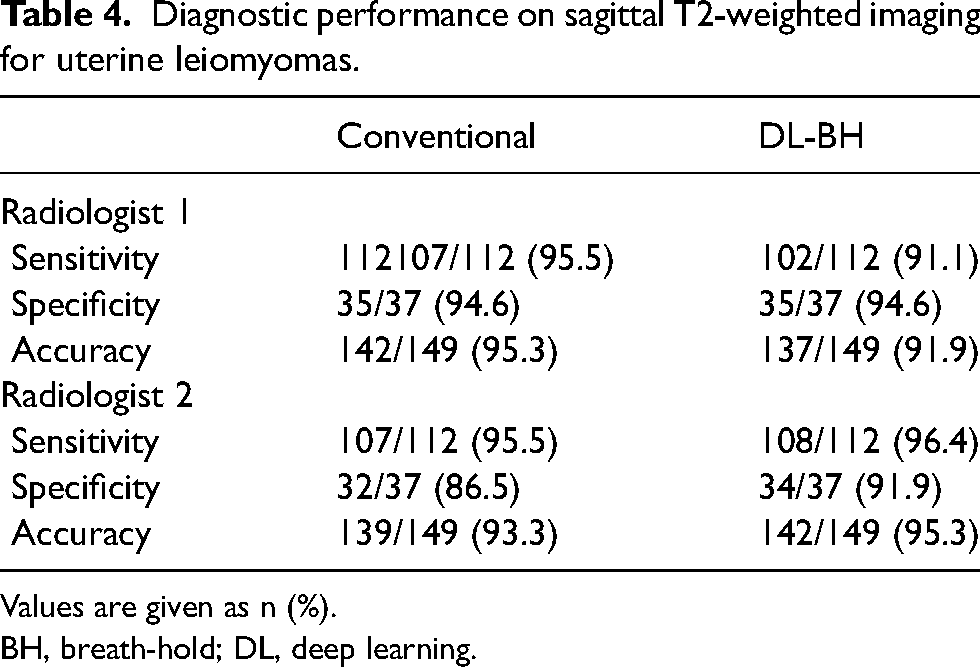
Values are given as n (%).
BH, breath-hold; DL, deep learning.
Discussion
This study evaluated the image quality and diagnostic performance of DL-accelerated sagittal T2W imaging in the female pelvic cavity. Sagittal T2W imaging is important in understanding the relationship between the uterus and other organs or localizing focal lesions. Because DLR allowed for a reduction in scan time, accelerated T2W imaging with breath-hold (DL-BH) was tried. Most qualitative image quality features were similar to or greater than conventional T2W imaging in DL-BH. The results of the study showed that the accuracy of the accelerated T2W imaging was similar to that of conventional images in detecting uterine leiomyomas. Thus, we suggest that the use of DL acceleration and BH acquisition is feasible in a clinical setting for evaluating uterine leiomyomas.
Although motion artifacts from breathing normally do not affect the pelvic cavity, some abdominal wall artifacts are seen in sagittal T2W imaging due to the wide field of view. If the MRI is obtained without breathing, it may reduce the breathing-related motion artifacts from the abdominal wall. BH acquisition is impractical for conventional T2W imaging due to the relatively long acquisition time, which requires multiple breath-holds (more than 10). We obtained accelerated T2W imaging for a total of 1 min and 5 s (63.7% reduction of acquisition time) using three 14-s breath-holds.
In the qualitative analysis, DL-BH demonstrated sharper margins of the anatomic structures with less subjective noise. Furthermore, when DL-BH was compared to conventional T2W imaging, diagnostic confidence, artifacts, overall image quality, and diagnostic performance were comparable or better. The VGC analysis also demonstrated that both radiologists assessed the overall image quality of DL-BH higher than conventional T2W imaging. In a previous study, BH TSE T2W imaging produced fewer motion artifacts and required less acquisition time than non-BH T2W imaging (25). Because the conventional T2W imaging employs a number of excitations (NEX) of 5, there is motion averaging that is reflected in blurring of the abdominal wall. The DL-accelerated sequences apply NEX 1, motion averaging is not used. As a result, DL-BH shows less blurring than conventional T2W imaging. However, it should be noted that DL-BH may be limited in patients who are unable to hold their breath. Ghosting artifacts from the abdominal wall may be more apparent and sharper, as seen in a sample case.
The average T2 SI of the uterus was lowest on DL-BH in quantitative analysis, probably due to the different repetition times (TRs). We chose the shorter TR for DL-BH because the images were obtained with three breath-holds. Despite having lower qualitative and quantitative noise levels, the lower mean T2 SI on DL-BH resulted in lower SNR and CNR than conventional T2W imaging. In this study, the objective and subjective decrease in noise is more relevant than the difference in T2 contrast since DLR is focused on noise reduction caused by accelerated image acquisition but does not modify the image contrast. Although different T2 SI did not appear to affect the diagnostic performance to detect uterine leiomyomas, radiologists may need some time to become acquainted with the differences in SI generated on DL-accelerated images.
Inter-reader agreement for artifacts and overall image quality was moderate to good, whereas it was poor to moderate for other parameters. The qualitative analysis was based on the subjective analysis of both radiologists, who may have had different standards of image quality. Despite poor to moderate inter-reader agreement for some qualitative features, both radiologists showed similar tendencies. In quantitative analysis, most parameters in the uterus had lower inter-reader agreement than muscle parameters. This could be due to the uterus's innate heterogeneous SI in comparison to the muscle.
The present study has some limitations. First, we evaluated the diagnostic performance just for uterine leiomyomas. Therefore, the detection of other lesions in the uterus and ovary was not investigated, and further research is necessary. Second, the gold standard for uterine leiomyomas was defined by the consensus reading of two radiologists based on MRI. Pathological diagnosis was not possible since the majority of uterine leiomyomas were not surgically treated. Third, DLR was only used on sagittal T2W imaging. The outcomes of DLR on axial T2W imaging in the female pelvis could not be guaranteed. We believed that sagittal T2W imaging was the most useful sequence to outline the anatomy and disease. Even though the same DLR showed good results in different organs and different planes, employing DLR on axial T2W imaging in the female pelvis should be investigated further (15,22).
In conclusion, DL-accelerated sagittal T2W imaging could be performed for three breath-holds and demonstrated superior or comparable image quality to conventional T2W imaging with no significant difference in diagnostic performance for uterine leiomyomas.
Supplemental Material
sj-docx-1-acr-10.1177_02841851241228192 - Supplemental material for Deep learning-accelerated T2-weighted imaging versus conventional T2-weighted imaging in the female pelvic cavity: image quality and diagnostic performance
Supplemental material, sj-docx-1-acr-10.1177_02841851241228192 for Deep learning-accelerated T2-weighted imaging versus conventional T2-weighted imaging in the female pelvic cavity: image quality and diagnostic performance by Hokun Kim, Moon Hyung Choi, Young Joon Lee, Dongyeob Han, Mahmoud Mostapha and Dominik Nickel in Acta Radiologica
Footnotes
Declaration of conflicting interests
The authors disclosed the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DH, MM, and DN are employees of Siemens Healthineers or Siemens Healthcare, but they did not influence the results of this study; MHC is currently receiving a research grant from Siemens Healthineers and the research is not related to prostate MRI. The other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.