
Abstract
The rubber hand illusion (RHI) is a perceptual illusion in which one experiences an object as part of their body when synchronous visuo-tactile stimulation is applied to one’s hand and the object. There are a variety of factors that can impact the occurrence of the RHI. In the present study, we demonstrate that experimentally induced peripheral ischemia can impact the RHI, namely it can result in larger alterations to the perceived position of one’s hand. This study suggests that alterations to the cardiovascular system may be a source of individual differences in the RHI literature. Future studies with samples of individuals with cardiovascular pathology are recommended.
The rubber hand illusion (RHI) is a perceptual illusion in which one is made to experience a noncorporal object as part of their body when synchronous visuo-tactile stimulation is applied to their hand and the object, while their hand is out of sight (Botvinick & Cohen, 1998). This illusion has become a model paradigm to study body ownership (i.e., experiencing something as part of one’s body) and is believed to be the result of multisensory integration (Ehrsson, 2020).
There are a variety of different factors that can impact the occurrence of the RHI. One factor known to impact/be impacted by the RHI is temperature (Kammers et al., 2011). Namely, it has been found that experiencing the RHI is associated with a decrease in the temperature of the stimulated hand, likely resulting from reduced blood flow when the RHI is elicited (Moseley et al., 2008; see de Haan et al., 2017 for a discussion of the heterogeneity within this literature). Furthermore, it has been found that cooling participants’ hand results in experiencing the RHI more vividly, namely it impacted a measure of the RHI called proprioceptive drift (i.e., feeling as if one’s hand is closer to the rubber hand than it actually is after synchronous stimulation; Kammers et al., 2011). In contrast, warming participants’ hands results in experiencing the RHI less vividly.
Interestingly, it has also been found that individuals with disorders characterized by reduced blood flow, such as anorexia nervosa (AN; Strumia, 2009), experience the RHI more vividly than healthy control subjects (Eshkevari et al., 2012). Namely, individuals with AN have been found to exhibit elevated body ownership questionnaire scores and proprioceptive drift (regardless of whether visuo-tactile stimulation is synchronous). This is noteworthy because the cardiovascular system plays a pivotal role in thermoregulation, and individuals with AN are known to exhibit acrocyanosis (i.e., reduced blood flow to the limbs characterized by blueish purple skin color and reduced limb temperature; González-Alonso, 2012; Strumia, 2009). This suggests that ischemia (i.e., reduced blood flow) may be one of the mechanisms underlying the differences exhibited by individuals with AN. However, there has yet to be a study to demonstrate whether experimentally induced peripheral ischemia can impact the RHI.
To address this gap in the literature, we used a pressure cuff ischemia protocol similar to Gross and Melzack (1978) to examine whether altered peripheral blood flow impacted the RHI. To this end, we conducted two studies. Study 1 evaluated the utility of a modified version of Gross and Melzack’s pressure cuff ischemia protocol. Study 2 used the protocol in Study 1 to see if experimentally induced ischemia altered the experience of the RHI.
Study 1
Gross and Melzack (1978) used a pressure cuff ischemia protocol to alter the perceived location of the participants’ hand, in which a sphygmomanometer was placed on the participants’ left shoulder and inflated to and held at 180 mmHg, and participants were then asked to report where it felt like their hand was after 10, 20, 30, and 40 minutes. The first author (M. T.) tested this protocol on himself, and it resulted in temporary pain and reddish-purple spots on their arm that took 2 weeks to go away. Thus, the first author found the minimum amount of pressure needed to induce ischemia and sensory loss. It was expected that participants would experience numbness and experience their hand as larger than it felt prior to the ischemia protocol (sensory loss is known to be associated with increased body size perception judgments; Gandevia & Phegan, 1999).
Participants
A total of 11 participants (5 female, 6 male) were recruited from the participant pool of a large midwestern state university. The mean age of the participants was 18.9 years (SD = 0.7) and ranged from 18 to 20 years. All participants were right-handed, had normal or corrected to normal vision, and had no history of sensory pathology (e.g., paresthesia), psychiatric disorder (e.g., AN), and/or cardiovascular pathology. One participant discontinued participation due to discomfort and was excluded from all analyses. All participants gave written consent in accordance with the Declaration Helsinki. The study protocols were approved by the Miami University Institutional Review Board (protocol # 01363r).
Procedure
After providing informed consent and demographic information, participants were asked to sit in a chair facing a table. Their left arm was placed on the table (with markers indicating where to place their elbow and left hand), and their feet were placed on markers on the floor. Once positioned, the researcher placed a (LotFancy) sphygmomanometer on their left bicep. Participants were then instructed to close their eyes and focus on how their left hand felt until instructed to do otherwise. Once the participant shut their eyes, the sphygmomanometer was inflated to 120 mmHg and was kept at that pressure for 10 minutes. After 10 minutes had passed, participants were asked how their hand felt and if their hand felt “larger, the same size, or smaller” (the order of the sizes was counterbalanced across participants). They were then asked to describe how their hand felt. Participants were informed that they could open their eyes and that the sphygmomanometer would be removed from their left bicep. The participants were then instructed to rapidly open and close their hand to get the blood to return to it. They were then debriefed and thanked for their participation.
Results and Discussion
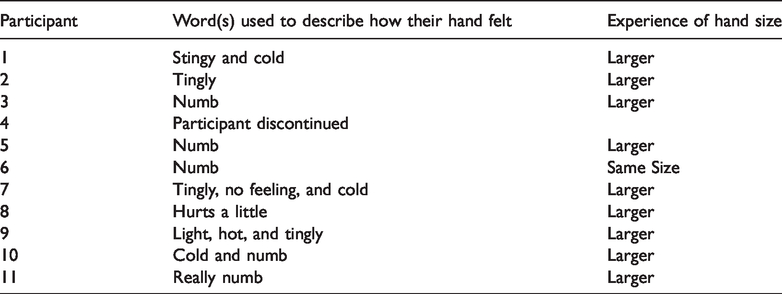
To determine if the modified version of Gross and Melzack’s (1978) pressure cuff ischemia protocol was an effective means to induce ischemia, we compared participants’ reports (consistent with sensory loss) to responding at chance level (33.33%). It was found that 90% of the participants reported experiences suggestive of ischemia (see Table 1 for a list of the words used to describe how their hand). Participants were also asked if their hand felt “larger, the same size, or smaller.” It was found that 90% of participants (9/10) felt that their hand became larger after 10 minutes. Both findings lend support to the conclusion that the modified version of Gross and Melzack’s (1978) pressure cuff ischemia protocol is an effective means to induce peripheral ischemia.
Each Participant’s Experience of the Pressure Cuff Ischemia Protocol.
Study 2
The authors used the pressure cuff ischemia protocol from Study 1 to examine whether altered peripheral blood flow impacted the RHI. Based upon previous work on individuals with AN, it was expected that if ischemia was induced, then participants would experience the RHI more vividly than individuals for whom ischemia was not induced (Eshkevari et al., 2012; Zopf et al., 2016). Namely, they would exhibit more proprioceptive drift and higher scores on questions about body ownership.
Participants
A total of 48 participants (26 female, 22 male) were recruited from the participant pool of a large midwestern state university. The mean age of participants was 19 years (SD= 1.1) and ranged from 18 to 22 years. All participants included in this study were right-handed, had normal or corrected to normal vision, and had no history of sensory pathology (e.g., paresthesia), psychiatric disorder (e.g., AN), and/or cardiovascular pathology.
The study protocols were approved by the Miami University Institutional Review Board (protocol # 01363r). All participants gave written consent in accordance with the Declaration Helsinki. Eleven participants were excluded from analysis, five (3 female, 2 male) of whom discontinued due to discomfort, one participant failed to wear corrective lenses for their eyes, one did not comply with directions, and one reported experiencing paresthesia (after previously reporting not experiencing sensory pathology). Furthermore, two were identified as multivariate outliers using Mahalanobis D2 (p < .05). This measure was computed using body ownership questionnaire scores and proprioceptive drift for both the synchronous and asynchronous conditions.
Experimental Setup
Each participant sat at a table in front of a 36.5 cm × 19 cm × 29 cm wooden structure that had two identical compartments. The participants’ right hand was placed into the right compartment with the palm facing down. In the left compartment, a rubber hand was placed in a configuration identical to the participants’ hand. There was a distance of 20 cm between the rubber hand and the participants’ hand. A black piece of fabric was used to cover the participant’s right arm. The top of the structure lifted to reveal the rubber hand in the left compartment.
The RHI Questionnaire
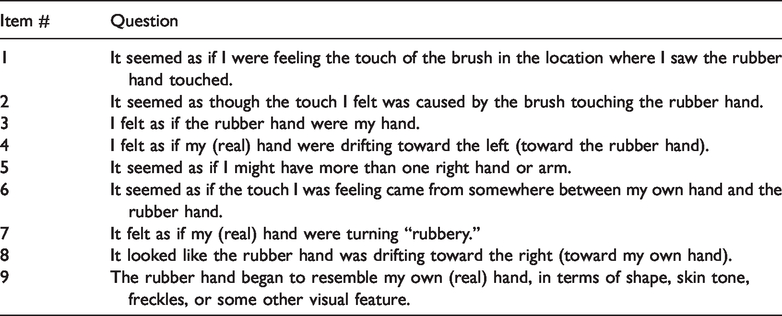
The RHI questionnaire was administered after each visuo-tactile stimulation condition (Botvinick & Cohen, 1998). This questionnaire involves having the participant rate their agreement with a number of illusion-related items on a 7-point Likert scale (3 = strongly agree, –3 = strongly disagree). It should be noted that items were modified to reflect the fact that the participant’s right hand was stimulated. See Table 2 for the items each participant answered after synchronous and asynchronous stimulation.
Rubber Hand Illusion Questionnaire Items.
Procedure
After providing informed consent, participants were randomly assigned to one of two conditions: pressure cuff inflated (sphygmomanometer inflated to 120 mmHg) or pressure cuff uninflated. The participant was then asked to sit down at a table and place their right hand into a box (described earlier). After the experimenter positioned their hand, a sphygmomanometer (LotFancy) was placed on their right bicep. Depending upon the condition the participant was assigned to, the sphygmomanometer was either inflated or left uninflated (to help rule out the possibility of bias). The participant was then asked to sit with their eyes shut, focusing on how their right hand felt.
After 10 minutes had passed, each participant was asked to make a judgment about where it felt like their right hand was at, by placing a sticky tab to the bottom of the table in the corresponding location. They were then asked to open their eyes and were shown the rubber hand that they were asked to look at. The experimenter then brushed the participants’ and rubber hand’s middle finger for a total of 90 seconds. After 90 seconds, the participant was asked to close their eyes and stick another sticky tab to the bottom of the table where it felt like their hand was currently at. They were then asked to complete the RHI questionnaire (Botvinick & Cohen, 1998) by indicating which number the experimenter should circle. After completing the questionnaire, the procedure was repeated again (not including the pressure cuff inflation). Each participant completed a trial where they received synchronous visuo-tactile stimulation and a trial where they received asynchronous visuo-tactile stimulation. The order that each participant completed the synchronous and asynchronous trial was counterbalanced and randomly assigned a priori. Upon completion of both trials, the participant was debriefed and thanked for their participation.
Results: Proprioceptive Drift Analysis
Proprioceptive drift was calculated by subtracting the distance between the rubber hand and perceived hand location after stimulation from the distance between the rubber hand and perceived hand location before stimulation. Thus, positive numbers indicated that the perceived location was closer to the rubber hand after stimulation. This was computed for both the synchronous and asynchronous visuo-tactile stimulation conditions. The resulting measures were subjected to a 2 × 2 mixed factorial analysis of variance (ANOVA) to examine the effects of visuo-tactile stimulation synchrony and pressure cuff inflation on proprioceptive drift. There was a statistically significant main effect of pressure cuff inflation, F(1, 38) = 6.84, p < .05,
Results: Body Ownership Analysis
Due to concerns about using an ANOVA to analyze ordinal data, a body ownership composite score was computed. This score was computed by finding the average of items one, two, and three for each participant (in both the synchronous and asynchronous condition). The resulting means were analyzed using a 2 × 2 mixed factorial ANOVA to examine the effects of visuo-tactile stimulation synchrony and pressure cuff inflation on body ownership scores. It was found that there was a statistically significant main effect of stimulation synchrony, F(1, 38) = 9.50, p < .01,

RHI questionnaire scores for the synchronous and asynchronous conditions separated by inflation condition. The error bars represent the standard error.Note. Please refer to the online version of the article to view the figure in colour.
Discussion
The aim of the present studies was to evaluate how the RHI is impacted by peripheral ischemia. To this end, we used a pressure cuff ischemia protocol when inducing the RHI. This study is the first to show that experimentally induced peripheral ischemia can increase proprioceptive drift resulting from synchronous visuo-tactile stimulation.
We found that individuals who experienced experimentally induced peripheral ischemia experienced more proprioceptive drift than the control participants, when the visuo-tactile stimulation was synchronous but not asynchronous. A possible explanation for this is that the reduction of tactile sensation resulting from pressure cuff ischemia protocol resulted in multisensory enhancement (such a possibility is consistent with the law of inverse effectiveness; Billock & Havig, 2018). The lack of difference in the asynchronous condition lends support to this possibility.
Alternatively, it is possible that pain elicited by the pressure cuff ischemia protocol resulted in increased proprioceptive drift. Previous work has demonstrated that nociceptive stimuli can be used to elicit the RHI and can elicit more proprioceptive drift than nonnociceptive tactile stimuli when stimulation is synchronous (though the difference was not statistically significant; Capelari et al., 2009). However, we do not believe this is the case because the present study did not synchronously/asynchronously apply a painful stimulus to the rubber hand (as was done in Capelari et al., 2009). Furthermore, painfully cold stimuli (which are more phenomenologically similar to the present study) have been found to result in less proprioceptive drift than a neutral temperature—not more (Kammers et al., 2011).
Contrary to our hypothesis, the RHI body ownership questionnaire scores were not impacted by peripheral ischemia (though they were impacted by visuo-tactile synchrony). While surprising, the findings of the present study bear a striking resemblance to Kammers et al. (2011), who cooled participants’ hands (which is known to reduce nerve conduction velocity/efficacy) and found that it also increased proprioceptive drift when visuo-tactile stimulation was synchronous but did not impact body ownership questionnaire scores. One possible explanation for the pattern of results in the present study and Kammers et al. (2011) is differences in neuroanatomical networks underlying body ownership and proprioceptive drift (Brozzoli et al., 2012). Namely, the network associated with proprioceptive drift that includes neuroanatomical regions such as the posterior parietal cortex may be more sensitive to sensory reductions/lags than higher level cortices (such as the premotor cortex) that are associated with body ownership (Brozzoli et al., 2012). Regardless of the mechanism(s) underlying this pattern of results, the lack of difference lends support to the growing literature that suggests that proprioceptive drift and body ownership are dependent on different mechanisms (Abdulkarim & Ehrsson, 2016; Rohde et al., 2011).
The present study has several limitations that should be noted. One of which is the fact that no measures of pain were used by the present study or Gross and Melzack (1978). Thus, it is unknown whether pain may be partially responsible for the difference found in the present study. It should also be noted that there was not a control drift (i.e., no brushing) condition. Thus meaning it remains unclear if the pressure cuff ischemia protocol would alter proprioceptive drift in nonillusion conditions, such information would provide us with a better understanding of whether it altered visuo-proprioceptive integration or visuo-tactile-proprioceptive integration. However, the present study was designed with the intention of making it similar to studies on the RHI in individuals with AN (e.g., Eshkevari et al., 2012), which did not have a no brushing condition. Future studies are needed to better characterize the mechanism(s) by which the pressure cuff ischemia protocol, described in the present study, altered proprioceptive drift.
In summary, the present study examined the impact of peripheral ischemia on the RHI using a pressure cuff ischemia protocol. It was found that peripheral ischemia increases proprioceptive drift (if visuo-tactile stimulation is synchronous) but does not affect body ownership questionnaire scores. Surprisingly, there was not a main effect of visuo-tactile stimulation on proprioceptive drift. The reason for this lack of main effect is not readily apparent; however, one possible explanation is that pressure cuff ischemia protocol resulted in a more pronounced difference between the synchronous and asynchronous stimulation, thus meaning that a larger control group may be needed before a main effect for visuo-tactile synchrony can be detected. The findings of the present study suggests that alterations to the cardiovascular system may impact one measure of the RHI (i.e., proprioceptive drift) and thus may be a source of individual differences with regards to susceptibility to the RHI. Furthermore, this study lends support to the growing literature suggesting that proprioceptive drift and body ownership are the result of different mechanisms. Clearly more work is needed to better understand how the cardiovascular system impacts measures of the RHI. We recommend studies on individuals with cardiovascular pathology (e.g., arterial diseases or AN) as well as neuroimaging studies that use manipulations similar to that of the present study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.