
Abstract
We examined self-reported frequency and severity of performance-related musculoskeletal pain disorder (PRMD), trigger point pain (TPP) and depression, social phobia (SPIN) and music performance anxiety (MPA) using the Kenny Music Performance Anxiety Inventory (K-MPAI) in a cross-sectional survey of 377 professional orchestral musicians. Most (84%) musicians had experienced performance-impairing pain; 50% reported current pain. Females reported more performance-impairing pain and more current pain than males. Cluster analysis indicated a complex relationship between depression and PRMD severity. Three clusters showed the hypothesized relationship (i.e., more depression, more pain). Musicians in the fourth cluster denied depression but reported the most severe pain, suggesting a group who somatize their psychological distress. Cluster analysis also revealed a strong relationship between PRMD severity and MPA. Clusters with higher scores on K-MPAI reported higher scores on PRMD severity. TPP was not associated with self-reported PRMD frequency or severity. There was a significant linear relationship between TPP and MPA for females, but males scoring the highest MPA reported lower TPP than those with milder MPA. Neither SPIN nor beta blocker use was associated with PRMD frequency or severity. The complex relationships identified between PRMD, TPP, depression and MPA may have important implications for PRMD management in professional musicians.
Keywords
The term performance-related musculoskeletal disorders (PRMDs) was first proposed by Zaza and Farewell (1997). It was later validated in a risk factor study with classical musicians (Zaza, Charles, & Muszynski, 1998). Pain arising from performance-related musculoskeletal disorders (PRMD) occurs frequently in professional musicians, with a range of studies indicating the high frequency (60–90%) of self-reported musculoskeletal pain (Ackermann & Adams, 2003; Ackermann, Kenny, & Fortune, 2011; Bragge, Bialocerkowski, & McMeeken, 2006; Fry, 1986; Hoppman, 2001; Kaufman-Cohen & Ratzon, 2011; Leaver, Harris, & Palmer, 2011; Zaza, 1998). The cause of musculoskeletal disorders and pain in musicians is multi-factorial, with occupational, environmental, e.g., lack of space and cold temperatures (Hansen & Reed, 2006), biomechanical (Wristen, 2000), including poor practice habits and over-practising (Wu, 2007), psychosocial and psychological (Kenny, 2010, 2011) factors contributing.
The impact of psychological factors, such as music performance anxiety, depression and tendency to somatize, i.e., to express psychological distress through somatic symptoms, on the presence of musculoskeletal symptoms is unclear, with contrasting results reported in the literature (Davies & Mangion, 2002; Leaver et al., 2011). Although relationships between pain, stress, anxiety and depression in different pain populations e.g., fibromyalgia (Normand et al., 2011), chronic pain (Bair, Wu, Damush, Sutherland, & Kroenke, 2008) and primary care patients (Poleshuck et al., 2009) have been explored, there have been few studies that have examined these relationships in professional musicians.
Anxiety and depression are commonly comorbid in clinical populations, including in those presenting with musculoskeletal pain. A study that examined comorbid depression and anxiety on pain intensity, pain-related disability and health-related quality of life (HRQL) in 500 patients with chronic pain found that the additional morbidity of depression and anxiety in people with chronic pain was strongly associated with reports of more severe pain, greater disability and poorer HRQL (Bair et al., 2008). A similar study of primary care patients (Romera et al., 2011) showed that 78% of patients with combined generalized anxiety disorder (GAD) and major depressive disorder (MDD) reported pain compared with 59% with GAD only and 28% with neither GAD nor MDD. These findings may be highly relevant to musicians reporting to physiotherapists with non-specific PRMD.
Pain and depression are frequently comorbid and co-occur in between 30% and 50% of patients (Kroenke et al., 2011). Depressed patients with musculoskeletal pain typically report significantly more psychosocial stressors and more severe anxiety than comparable non-depressed patients with musculoskeletal pain (Poleshuck et al., 2009). Patients with major depressive disorder (MDD) or fibromyalgia both reported hyperalgesia (Normand et al., 2011). It has been difficult to ascertain the temporal and causal relationship between pain and depression, although a recent study of 100 outpatients showed that 77% of anxiety disorders predated the onset of pain, but 63% of depressive disorders followed the onset of pain (Knaster, Karlsson, Estlander, & Kalso, 2012). Pain and depression also appear to have a reciprocal effect. In older adults (65+ years) pain was an independent predictor of the onset of depression two years after baseline measurements were taken; depression at baseline predicted pain onset at two years (Chou, 2007). Increases in pain were associated with increases in depression severity; and increases in pain severity were associated with increased depression in 500 primary care patients who were followed longitudinally over 12 months (Kroenke et al., 2011). Another study (Godfrey, 2007) reported that the number of pain complaints is a better predictor of depression than scales of pain severity and persistence. In severely depressed patients with pain, treatment that focuses on pain management was not effective until the depression had been treated. Given the frequency and severity of reported PRMD in professional musicians, an examination of the relationship between pain and depression in this group is warranted.
A small number of studies on musicians have attempted to assess some of the complex relationships between psychological factors and pain. Kaufman-Cohen and Ratzon (2011) reported on the relationships between biomechanical function (DASH), musculoskeletal symptoms (Standardized Nordic Questionnaire; SNQ and the Rapid Upper Limb Assessment; RULA), job stress (Generic Job Stress Questionnaire) and personal information (BMI, medical history, sport participation) in 59 classical musicians, of whom 83% reported PRMD symptoms in at least one body region in the previous 12 months. Results indicated that biomechanical factors (e.g., number of playing hours, weight of musical instrument) but not job stress factors predicted PRMD. A larger study of 243 orchestral musicians, of whom 86% reported PRMD in the previous 12 months, used standardized psychological tests such as the Brief Symptom Inventory to assess somatization and the Short Form-36 (SF-36) to assess mood (Leaver et al., 2011). Results indicated that location and severity of PRMD were primarily associated with instrument type. However, somatizing scores in the high range increased the odds of reporting regional pain between 2.5 (wrist/hand) and 5.5 (shoulder) times. Risks were higher for female musicians and increased when low mood was present. This study also reported that performance anxiety had no independent effect on PRMD but no details were provided regarding the assessment method used to measure music performance anxiety (MPA). This result may therefore be due to the use of a non-standard and possibly invalid measure of MPA.
Most studies assessing pain in musicians have reported pain perception only and have not included an objective measure of pain (Leaver et al., 2011) such as trigger points, which have been used extensively in work settings to assess pain related to acute overload and overwork fatigue (Simons, Travell, & Simons, 1999). The exception is Rickert, Barrett, Halaki, Driscoll, and Ackermann (2012) who showed that upper trapezius trigger points were sensitive to the frequency, severity and number of current injuries in cellists. “A myofascial trigger point is a hyper-irritable spot, usually within a taut band of skeletal muscle, which is painful on compression and can give rise to characteristic referred pain, motor dysfunction, and autonomic phenomena” (Lavelle, Lavell, & Smith, 2007, p. 841). Trigger points involve autonomic innervations and are thus responsive to psychological stressors; they show elevated electromyography (EMG) readings under stressful task conditions or emotional distress, suggesting a mediating role in trigger point response via the sympathetic nervous system (McNulty, Gevirtz, Hubbard, & Berkoff, 1994; Travell & Simons, 1983).
Trigger points also show increased electromyographic activity in response to psychological stress while adjacent muscles remained non-responsive (Hubbard & Berkoff, 1993; McNulty et al., 1994). Psychological factors may therefore be associated with subjectively reported trigger point pain but this question has not previously been addressed in musicians and hence was included as a research question in this study.
A meta-analysis (Bragge et al., 2006) assessing risk factors associated with PRMDs in pianists reported prevalence rates ranging from 26% to 93%. None of the included papers showed consensus with respect to risk factors. The authors concluded that there is currently insufficient evidence to reliably identify risk factors associated with PRMDs in pianists and that future studies should provide an operational definition of PRMD, use valid, reliable measurement tools, a prospective cohort study design and perform appropriate statistical tests.
Kenny, Driscoll, and Ackermann (2012) showed a complex relationship between music performance anxiety and depression. However, the co-occurrence of PRMD pain, depression, MPA and other anxiety disorders, in particular social anxiety disorder, in professional musicians has not been investigated and awaits elucidation. The aim of this study was to assess these relationships. Because of the novel and exploratory nature of this research, it was premature to offer specific hypotheses. However, guided by associations identified in other studies, and based on the results of our previous research, we were interested, in this study, to identify whether an association was present between PRMDs and psychosocial factors using self-reported data (numerical rating scales), including age, sex, instrument, trait anxiety, music performance anxiety, social phobia (social anxiety disorder) and depression, as well as including an objective physical measure (right and left myofascial trapezius trigger points) in a population of professional orchestral musicians. In addition, we explored the utility of including both perceptual and objective measures of pain associated with PRMD and their degree of association in this population.
Methods
Participants
Eligible participants were all musician members of one of the eight premier state and opera orchestras in Australia, of whom 377 (70% response rate) agreed to participate. The sample comprised 184 males (49%) and 192 females (51%). The mean age of the musicians was 42.1 years (SD = 10.3; Range = 18–68 years).
Procedure
Ethical approval for the study was obtained from The University of Sydney Human Ethics Committee. Information sheets, consent forms and invitations were posted to all musician members of the participating orchestras. Respondents were sent a self-report survey at the commencement of the study, which they returned by mail in self-addressed, stamped envelopes provided by the researchers. This method ensured confidentiality and anonymity of the musicians to all parties except the researchers, who were required to match questionnaire data with the later physical tests that were performed.
Physical tests were performed in situ (i.e., at the orchestra’s location) by trained physiotherapists under the supervision of the second author. A range of tests were performed, but only the trigger point results are reported here.
Measures
A number of standardized tests and tests and rating scales constructed for this study were used to assess the psychological health and self-reported frequency and severity of performance-related musculoskeletal pain disorders (PRMD) of the orchestral musicians. These were:
Psychosocial measures
Only brief descriptions of these measures are given here. For a more detailed coverage of psychometric properties for each scale, see Kenny et al. (2012).
Kenny Music Performance Anxiety Inventory (Revised) (K-MPAI) (Kenny, 2011). This 40-item inventory was developed to assess the emotion-based theory of anxiety proposed by Barlow (2000) as it applies to anxiety in the context of music performance. The inventory is described in detail elsewhere (see Kenny, 2011; Kenny et al., 2012). Questions are answered on a 7-point Likert scale [0 = Strongly disagree to 6 = Strongly agree]. Higher scores indicate greater anxiety and psychological distress. This scale demonstrated excellent internal reliability (Cronbach’s alpha = 0.94) and a stable factor structure across professional and student classical musicians (Kenny, 2011).
Trait questionnaire of the State-Trait Anxiety Inventory (STAI-T) (Spielberger, 1983) is a 20-item scale used to measure state (20 items) and trait (20 items) anxiety. Only the trait questionnaire, which assesses a propensity to worry and feel anxious, was administered in this study. Raw scores (range 20–80) were converted into T scores with mean = 50; SD = 10. High scores indicate higher levels of trait anxiety.
Social Phobia Inventory (SPIN) (Connor et al., 2000). This 17-item self-report inventory reports on the full spectrum of symptoms of social phobia including fear, avoidance and physiological components. Items are scored on a five point scale (0 = not at all; 4 = extremely) and scores range from 0 to 68. A cut-off score of 19 reliably distinguishes correct diagnoses of social phobia from controls, with sensitivity of 0.73 and specificity of 0.84. A SPIN score of 19 was used as the cut-off score in this study.
PRIME-MD Patient Health Questionnaire (PRIME-MD PHQ) is a 2-item questionnaire to screen for depression. Musicians were asked these two questions: 1) During the past month, have you often been bothered by feeling down, depressed, or hopeless? 2) During the past month, have you often been bothered by little interest or pleasure in doing things? These questions are taken from the Primary Care Evaluation of Mental Disorders Patient Health Questionnaire (Kroenke, Spitzer, & Williams, 2003). If the response to both questions is “no”, the screen is negative. If the response is “yes” to either or both question(s), further screening for depression is advised. Whooley, Avins, Miranda, and Browner (1997) compared the 2-question screen to the Quick Diagnostic Interview Schedule (QDIS-III) and reported a sensitivity and specificity of 96% and 57% respectively.
Core Self Evaluation Scale (CSE; Judge, Erez, Bono, & Thoresen, 2003) comprises 12 items that are assessed on a 5-point scale (1 = strongly disagree; 5 = strongly agree). (See Bono & Judge, 2003, p. S6.) Core self-evaluation, a meta-trait, comprises four traits that all load onto CSE; they are self-esteem (.91), generalized self-efficacy (.81), neuroticism (-.74) and locus of control (.73). CSE is moderately predictive of job satisfaction (.41) and job performance (.23) (Judge, 2009).
Pain measures
Performance-related musculoskeletal disorder (PRMD)
We presented musicians with Zara and Farewell’s operational definition of PRMD (i.e., “A PRMD refers to any pain, weakness, numbness, tingling or any other symptoms that interfere with your ability to play your instrument at the level to which you are accustomed. This definition does not include mild short-lived aches or pains”) prior to asking a series of questions that assessed the presence of PRMDs (e.g., “Have you EVER experienced pain or injuries that you think are related to playing your instrument?”). Pain frequency and pain severity/intensity of PRMDs were assessed using 11-point numerical rating scales, as recommended by Dworkin et al. (2005) and Kenny, Trevorrow, Heard, and Faunce (2006). Musicians were asked to rate their PRMDs frequency on an ordinal scale with endpoints 0 = “never” and 10 = “constantly” and their PRMD severity on an ordinal scale with endpoints 0 = “no pain” to 10 = “worst imaginable pain”. These scales are simple and valid ways of measuring pain frequency and intensity in clinical populations (Kamper, 2012).
Trigger point
Previous researchers (Hubbard & Berkoff, 1993; Lavelle et al., 2007; McNulty et al., 1994) have used a trapezius myofascial trigger point; hence, the same trigger point, one in each upper trapezius muscle, was selected for this study. Trigger points were palpated by specially trained and highly experienced clinicians as a localized hyperirritable point within a taut band of muscle in the region approximately halfway between the tip of the acromion and the C7 vertebra. This region has been described by Simons et al. (1999) as TP2. It is frequently observed and may be influenced by both mechanical and psychological stressors. The pain pressure threshold was measured by applying a constant increasing rate of pressure perpendicularly to the skin surface directly over the trigger point site. A pressure of 5N was applied and recorded using a hand-held force gauge (Lafayette Manual Muscle tester model 01163; Lafayette Instrument Company, Lafayette, IN, USA). The circular contact area of the gauge tip was approximately 17 x 17 mm in size covered with 3mm thick rubber foam. The experimental protocol involved recording three consecutive pain readings using an 11-point Likert scale once a pressure of 5N was applied to the trigger point site in each trapezius, with the average value of the two closest measures (least difference) resulting in the pain score.
Analysis
Frequencies, descriptives, cross tabulations and chi square analyses were used to describe the univariate relationships among the variables. Correlational analyses assessed the relationship between the psychological measures; analyses of variance with post hoc (LSD) comparisons, where appropriate, were used to identify subgroup differences. Linear regression was applied to identify the predictors of music performance anxiety and two-step cluster analysis was employed to identify subgroup clusters within the sample after linear regression analyses indicated that the relationship between factors was not linear.
Results
The distributions of the PRMD frequency and severity scales were assessed for violations of normality (e.g., skewness and kurtosis) prior to analysis. As the distributions were normal, means are reported throughout.
Three hundred and eighteen musicians (n = 318; 84%); mean age 42 years (SD = 10.2) reported having experienced pain that interfered with their performance. For pain frequency, 100 musicians (26.7%) reported never experiencing PRMD pain; 184 (49.1%) reported pain frequency ratings between 2 and 6; 91 musicians (24%) reported experiencing PRMD pain constantly. For pain severity, 101 musicians (28.3%) reported no pain; 50.7% reported pain severity ratings between 2 and 6; 21% (n = 75) reported that the severity of the pain was the “worst imaginable”. There was a highly significant relationship between the frequency of reported pain and its severity, with those reporting higher frequency much more likely to report higher pain severity (χ2 = 304.84; p = .001).
Female musicians reported significantly more frequent occasions of pain that interfered with their performance (males = 146, 46%; females = 172, 54%; χ2 = 5.62; p = .018). One hundred and eighty seven musicians (50%) reported experiencing current pain during performance, but the difference in proportion between males and females was not significant (males = 85, 46%; females = 102, 54%; χ2 = 1.42; p = .234). There was a significant relationship between reports of current pain and the presence of pain that interferes with performance. Those reporting current pain were more likely to report that they have had, at some previous time, pain that interfered with performance (χ2 = 10.96; p = .001). There were no significant differences between instrument groups in the reporting of current pain during performance; nor were there any differences for the sex by instrument group interaction in report of current pain.
Using the general linear model, the effects of sex and age group on report of PRMD pain frequency and severity were assessed. There were significant main effects for both sex and age but the sex by age interaction was not significant (Table 1). Females had significantly higher mean scores for both PRMD frequency and severity. Post hoc (LSD) comparisons indicated that the age group 41–50 years had higher reports of both PRMD frequency and severity than the other three age groups.
Relationships between sex, age and PRMD frequency and severity.

Observed power is the probability of rejecting the null hypothesis when it is false.
Univariate analyses of pain factors and psychosocial and lifestyle factors
A series of univariate analyses were conducted to determine whether any of the psychosocial or health factors were associated with report of pain frequency and severity. There was a significant association between pain severity and depression (F = 3.90, p = .021). Those answering “yes” to both depression questions had higher mean scores on PRMD severity (4.52; SD = 3.24) compared with those who answered “no” to both questions (3.46; SD = 2.82), with those answering “yes” to one question scoring midway (4.20; SD = 2.91). A similar but non-significant trend was observed for pain frequency and depression.
There was a similar but non-significant relationship for SPIN using the recommended cut-off score of 19. The group exceeding the cut off tended to score higher on both pain frequency (p = .08) and pain severity (p = .09). There were no differences in report of pain frequency or severity for those who engaged in physical activity of any kind, including yoga, swimming, jogging or gym classes.
Regression analyses
Linear regression analyses were used to test the hypothesis that the severity of performance-related musculoskeletal pain could be predicted by psychological distress as assessed by the K-MPAI, STAI-T, SPIN, CSE and the depression screen. Table 2 summarizes the descriptives. Because the variables in the predictive model were on different scales, they were converted to z-scores with a mean of 0 and a standard deviation of 1 before being entered into the regression analysis.
Means and standard deviations of factors entered into the regression analyses.
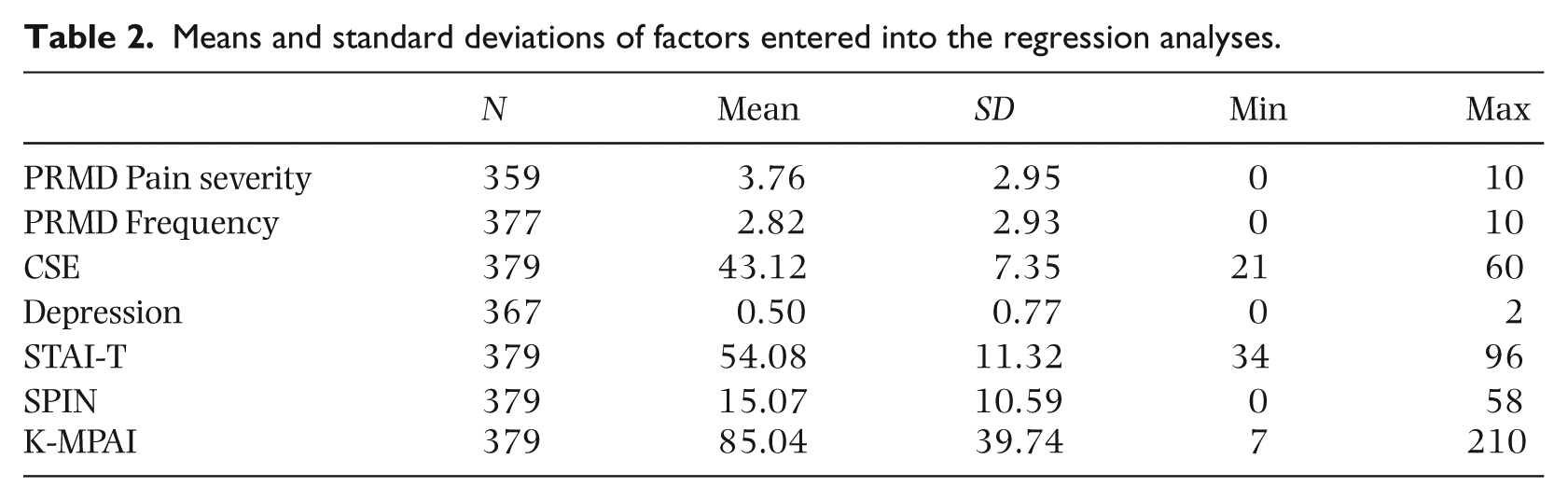
The ANOVA F statistic was significant (F5, 346) = 3.05, p = .01), indicating that the model predicted reported PRMD severity better than chance. However, the model was a poor fit; only 4.4% of the variation in PRMD severity was explained. Prior to finalizing the model, and in view of the high inter-correlations between these measures, multicollinearity of the variables was assessed using collinearity statistics, tolerance and the variance inflation factor. The tolerance is the percentage of the variance in a given predictor that cannot be explained by the other predictors. When the tolerances are close to zero, there is high multicollinearity and the standard error of the regression coefficients will be inflated. The tolerance values indicated that the depression screen (tolerance = 0.718) and SPIN (tolerance = 0.992) contributed the most independent variance to the equation.
A variance inflation factor (VIF) greater than 2 is usually considered problematic. The VIFs for three of the five factors were slightly greater than 2 (CSE, STAI and K-MPAI), indicating a moderate problem with multicollinearity. To improve the variance inflation, a factor analysis was conducted to create a set of independent variables that were uncorrelated. A linear regression analysis was then run on the factor scores. The model was the same as for the model using the original predictors. The collinearity statistics showed that the factor scores were uncorrelated. The only factor that was significant in the new model was the K-MPAI. However, the model’s ability to explain the variation in the severity of pain caused by PRMD was poor (R square = .029). The analysis was rerun using PRMD frequency as the dependent variable. The ANOVA F statistic was significant (F5, 346) = 6.23, p = .01), indicating that the model predicted PRMD frequency better than chance. However, the model was a poor fit and only 2.9% of the variation in PRMD frequency was explained. Only depression (Standardized Beta coefficient = 0.13) contributed significantly to the prediction of reported PRMD frequency.
Cluster analyses
Additional analyses were undertaken to further interrogate the data, in order to better understand the relationship between the psychosocial and pain factors, and to find possible explanations for the apparently poor predictive ability of the psychosocial factors of pain severity. Cluster analysis was conducted to identify the cause of the nonlinearity in the regression findings and to test the possible presence of a somatizing group of musicians. A two-step cluster analysis was conducted, using the K-MPAI with severity ratings of PRMD pain as inputs. The cluster quality was good (Average silhouette = 0.7) and four distinct clusters were obtained as shown in Table 3.
Cluster analysis of pain severity group using K-MPAI.
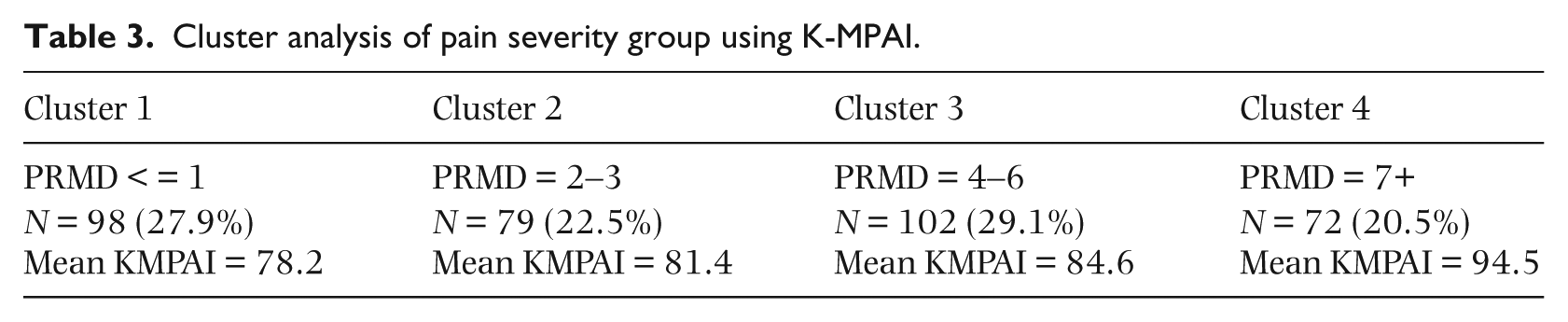
These results indicate a four cluster solution with approximately equal proportions in each cluster. A significant association between pain severity and MPA severity was observed; as reported pain-related PRMD became more severe, mean scores on music performance anxiety increased. When the depression category variable and severity of PRMD-related pain were used as the inputs to define the clusters, the cluster quality was good (Average silhouette = 0.6) and again, four clusters were identified (Table 4).
Cluster analysis of PRIME-MD using pain severity.
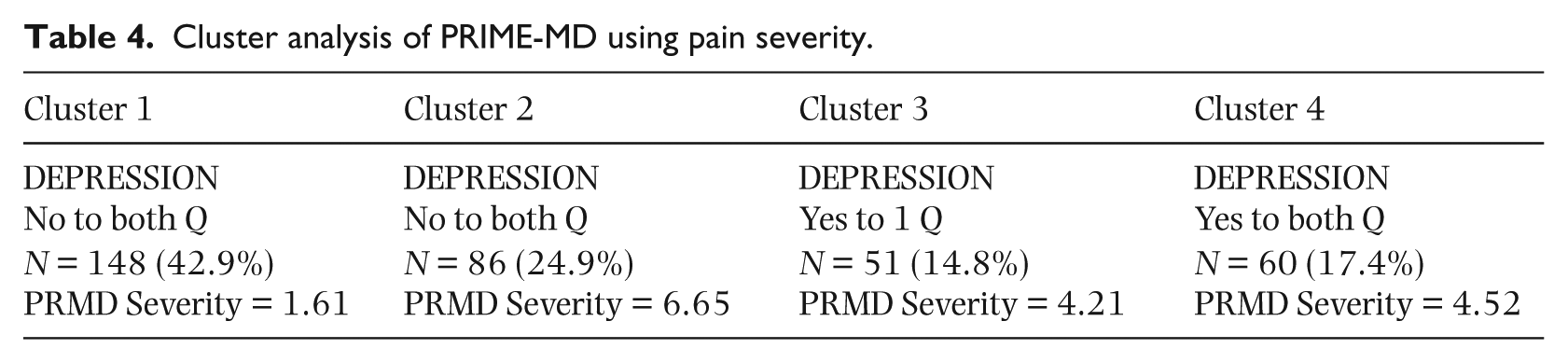
There were two clusters for musicians who reported “no” to both of the depression screen questions. The first group reported minimal PRMD severity (mean = 1.61) – this was the largest cluster with 43% of musicians belonging to this group; the second group, comprising 25% of musicians, reported the highest PRMD severity (mean = 6.65) of all the clusters, including those in clusters 3 and 4 who answered “yes” to either one or both depression questions.
Repeating the analysis with the SPIN cut-off factor, the cluster quality was good (Average silhouette = 0.6) and two clusters were identified. For those musicians scoring below the SPIN cut off for “caseness” for social anxiety (n = 240, 67.2%), the mean for PRMD severity was 3.58. For those screening positive for social anxiety (n = 117; 32.8%), the mean for PRMD severity was 4.15. However, one way analysis of variance showed that the difference in the mean pain severity scores for the two SPIN clusters was not significant (F1, 356) = 2.78, p = .09).
Similarly, those taking beta blockers to relieve performance anxiety (n = 110; 30.8%) scored higher on PRMD severity (mean = 3.96) than those not taking beta blockers (n = 247; 69.2%; PRMD = 3.68). When the subset of musicians who used beta blockers to manage their performance anxiety was examined, three clusters were identified within this subset. The first (n = 41; 37.3%) reported very low pain severity (mean = 0.63); the second group (n = 42; 38.2%) reported moderate pain severity (mean = 4.40); and the third group (n = 27; 24.5%) reported extreme pain severity (mean = 8.33), indicating that musicians used beta blockers across the full range of reported PRMD severity.
Trigger point pain, self report of PRMD frequency and severity, and associations with MPA and depression
The scores for the right and left trigger points were significantly correlated (r = 0.74; p = .001), but there were no significant correlations between the right trigger point with PRMD frequency (p = .07) or PRMD severity (p = .08) or the left trigger point with PRMD frequency (p = .17) or PRMD severity (p = .14). There was a significant sex difference for pain reports for both right (F(1,3) = 8.31; p = .004) and left trigger points (F(1,3) = 10.31; p = .001) for musicians reporting the highest scores on the K-MPAI. Scores for females increased as MPA scores increased, while males in the highest MPA group showed a decrease in report of pain from the trigger points. Figure 1 shows the results for the right trigger point. The pattern was the same for the left trigger point.

Right trigger point scores by K-MPAI and sex.
On pain ratings for the right (F(1,6) = 2.6; p = .02) and left trigger (F(1,6) = 2.54; p = .05) points, those reporting high MPA and affirmative responses to both depression questions had higher trigger point pain ratings than subgroups with lower ratings of MPA. Figure 2 shows the pattern of results for the left trigger point. The pattern was similar for the right trigger point.
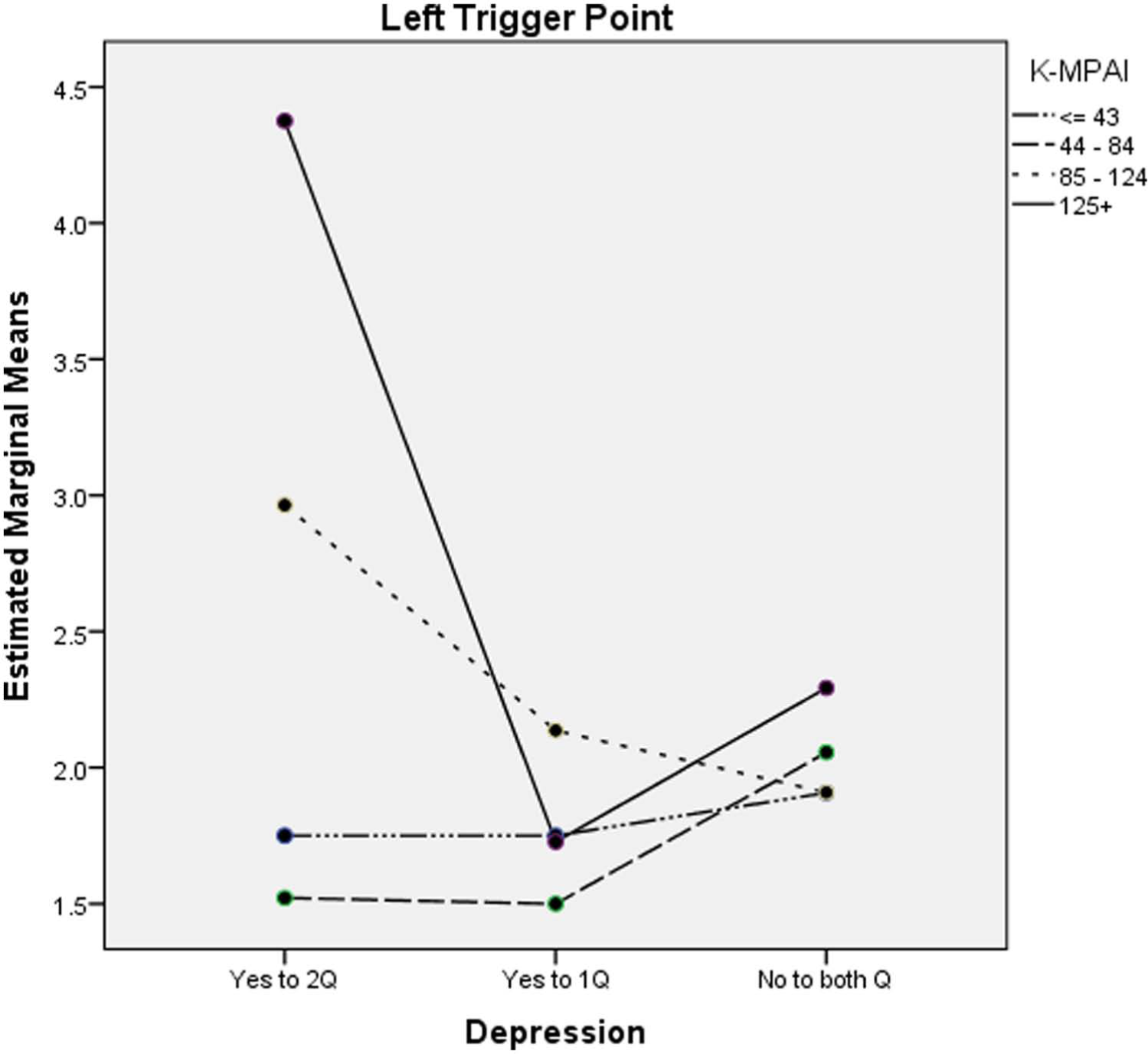
Left trigger point scores by K-MPAI and depression.
There were no differences across depression categories for trigger point scores between those using beta blockers and those not using them. Trigger point scores increased with increasing scores on K-MPAI in the same manner for those meeting criteria for a diagnosis of social phobia and those not meeting the diagnosis (Figure 3).
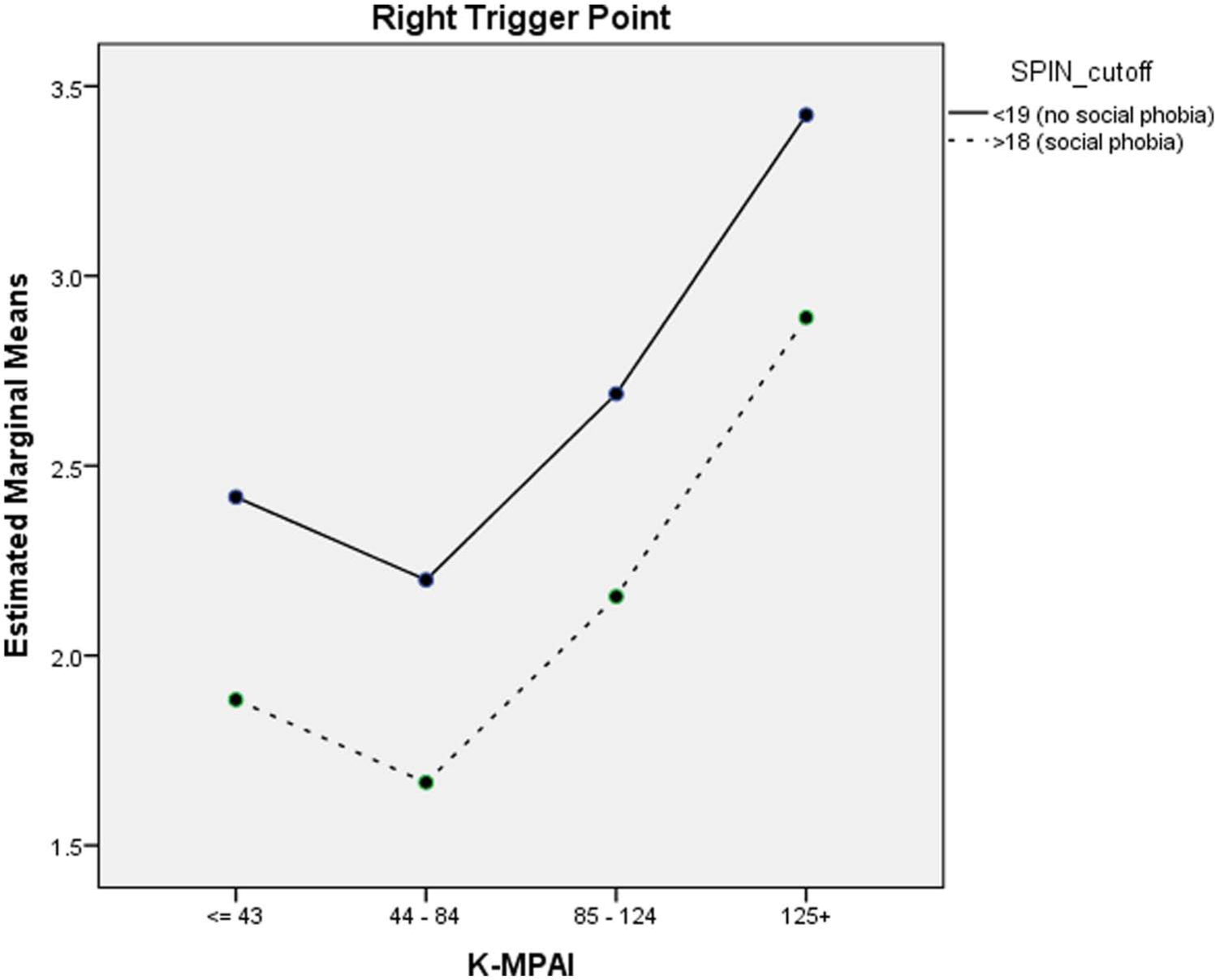
Right trigger point scores by SPIN and K-MPAI.
Discussion
Consistent with other recent research (Leaver et al., 2011), the majority (84%) of elite professional musicians in this study reported having experienced performance-related musculoskeletal pain severe enough to interfere with their performance; 50% of the sample reported current pain. A significant minority also reported that their pain was constant (24%) and severe (21% of this sample reported their pain as the “worst imaginable,” with a further 29% reporting moderately severe pain). This is consistent with the reported sensitization that occurs in the central nervous system in response to chronic pain conditions, as well as the possible development of fear avoidance behaviours, such as altering normal technique, which may further impact on normal function and potentially further aggravate symptoms (National Pain Strategy, 2010).
Higher proportions of females reported both more severe performance-impairing pain and more frequent occasions during which they experienced pain of this severity. Musicians in the age range 41–50 years reported higher frequency and severity of PRMD compared with both younger and older groups. There are a number of possible explanations as to why this age group is more vulnerable to performance-related pain. Manturzewska (1990) proposed that “professional stabilisation and expansion” peaks from 30–45 years of age, and is followed by signs of psychological and physical decline in the 45–55 years old age group, with change to teaching interests over performance. Alternatively, Smith (1992) mused on the results of the Fishbein study of European orchestras (Fishbein, Middlestadt, Ottati, Strauss, & Ellis, 1988) that showed the peak of injury occurred at age 35 and then decreased in older groups. He suggested that this trend may be due to disappearance via early or medical retirement of the musicians with problems from the orchestras, or potentially to an increased tolerance for such problems that are lifelong and about which they reduced their complaining with age. In the last two decades, research has focused primarily on skill development in the younger population, with no new research investigating issues across the full lifespan of the professional musician (Brodsky, 2011).
Engagement in physical activity of any kind, including yoga, swimming, jogging and gym classes did not bestow any protection against reported PRMD frequency or severity, possibly because generic exercise does not specifically support the act of playing a musical instrument and does not target imbalanced muscle groups (van Hees, 1997). In contrast, positive impacts on performance-related pain have been noted in exercise programs that were designed specifically for music students (Ackermann & Adams, 2003; Kava, Larson, Stiller, & Maher, 2010).
Cluster analyses of PRMD severity and music performance anxiety severity showed that increasing PRMD severity ratings mapped linearly onto increasing mean K-MPAI scores across the four clusters identified in the analysis. These results, reported for the first time in musicians, are consistent with a longitudinal study of medical patients with a depressive and/or anxiety disorder who reported higher pain scores and pain chronicity, which was linked with a worse course of existing anxiety and depressive disorders (Gerrits et al., 2012; Pennix, Leveille, Ferrucci, Van Eijk, & Guralnik, 1999). A recent review noted that there was a shortcoming in research investigating specific anxiety disorders and their effect on the chronic pain experience (Asmundson & Katz, 2009). The results from the current study highlight the need for further investigation.
Univariate analyses revealed a significant relationship between PRMD severity and depression, but not between PRMD frequency and depression. Cluster analysis further assessing this relationship between PRMD severity and depression is of considerable clinical and theoretical interest. Cluster 2, which represented one quarter of the sample, reported no depression while simultaneously returning the highest ratings for PRMD pain severity, which were even greater than those reported in clusters who answered “yes” to one or both of the depression screen questions. Similar discordances have been observed in studies of anxiety and physiological arousal, but no comparable study has examined this phenomenon in depression. Hence, it is instructive to understand the possible explanations for the discordance between various measures of anxiety and physiological arousal that have been observed in non-musical populations. Weinberger, Schwartz, and Davidson (1979) showed that inconsistencies in physiological responsiveness between low and high trait anxious people (i.e., between people prone to react anxiously in a wide range of situations) was accounted for by a sub-group in the low trait anxious self-reporters who had high scores on measures of social desirability. Social desirability is a phenomenon that reflects people’s need to gain approval. Put simply, social desirability is the tendency to give responses that make the individual look good (Holden & Passey, 2009). This sub- group was classified as “repressors.” Physiological reactivity was subsequently assessed for these three groups in that study. Results indicated that the “true” low trait anxious group (low scores on both social desirability and anxiety measures) had the lowest physiological reactivity, followed by the “true” high trait anxious group (high scores on both social desirability and anxiety measures) followed by the repressors. This finding has been replicated many times in many different domains (Shedler, Mayman, & Manis, 1993) showing that humans are susceptible to defensive and self-presentation biases in most areas of human endeavour, a phenomenon that is heightened when people are asked to self-report undesirable traits or characteristics (Thomas, Turkheimer, & Oltmans, 2003).
Researchers in health have long known about the unreliability of self-report measures in assessing psychological well-being or predicting health outcomes. Such measures are unable to differentiate those who are genuinely psychologically healthy from those who maintain “a facade or illusion of mental health based on denial and self-deception,” or who somatize their psychological distress, and that “clinically derived assessment procedures that assess implicit psychological processes may have advantages over self-report mental health measures” (Cousineau & Shedler, 2006, p. 427). One of the key reasons that standard self-report measures are limited in this way is that the relevant psychological processes may be implicit, that is, they are not available to awareness and thus, cannot be directly reported upon. A great many cognitive and affective processes, including memory, cognition, affect, motivation and attitudes can be implicit (Wilson, Lindsey, & Schooler, 2000). The cluster of musicians with this complex psychological presentation that is analogous to somatization (i.e., those who denied depression but reported the most severe PRMD pain) deserve closer scrutiny using measures devised to tap into implicit processes. It is possible that this cluster is describing a group who somatize their psychological distress. Alternatively, they may simply be a group with no psychological issues experiencing a lot of pain. Future research will hopefully clarify the characteristics of this cluster.
Two additional cluster analyses were conducted; one using SPIN (social phobia) showed those with “caseness” for social phobia had higher scores on PRMD severity than musicians who fell below the cut off. The other examined the subset of musicians who used beta blockers to manage their music performance anxiety. Results indicated that the best fit was a three-cluster solution grouping musicians into those with low, moderate and high pain severity. Musicians who used beta blockers experienced PRMD across the full range of reported PRMD severity.
To our knowledge, this is the first research to examine the relationship between trigger point pain, self-reports of PRMD frequency, and severity and associations with MPA and depression. We have reported the results for both left and right trigger points, as it was of interest, first, to ascertain whether the results were similar, whether instrument type affected which side was most impacted, and also as a form of reliability analysis of the measure. There were no significant relationships between right or left trigger points and PRMD frequency or severity. In contrast to the study by Rickert et al. (2012) where a specific instrumental group (cello) with high neck and shoulder loads during performance was studied, this study evaluated a wide range of instrumentalists, which may have required more trigger points to be assessed to reflect the specific mechanical loading of the different instruments. The use of trigger points in only one region of the body may have reduced the association between reported PRMD frequency and severity and trigger point sensitivity as most reported associations of trigger point sensitivity and pain are located within the region of pain (Freeman, Nystrom, & Centeno, 2009). Trigger points are directly influenced by factors such as biomechanics (movement patterns) and asymmetrical postural loading (Travell & Simons, 1983). This is clearly the major source of loading for this population, who spent an average of 44 hours playing their instruments per week (Rickard et al., 2012). By comparison, handedness is not relevant to instrumental performance because the instrument drives the movements determining how the instrument is played (Kopiez et al., 2012). In contrast, anxiety is linked to elevations in EMG threshold without an increase in local muscle activation in pain free subjects (McNulty et al., 1994). Thus, research to date suggests that trigger points may only appear sensitive with local pain and this may account for the absence of any general pain effect.
However, trigger points do seem to be sensitive to psychological phenomena. In our study, there were significant sex differences for both right and left trigger points for musicians falling into the highest score category (125+) on the K-MPAI. Females’ scores continued to rise in linear fashion across levels of severity of MPA (i.e., higher MPA was associated with greater trigger point sensitivity) while the trigger point scores for males in the highest K-MPAI category decreased sharply. When depression was included, results indicated that the most depressed and performance anxious musicians had significantly higher trigger point scores than other groups with lower depression and MPA. The pattern of results was the same for right and left trigger points. It is, at this stage of our understanding and knowledge, difficult to account for these findings. We have speculated that male musicians may reach a level of anxiety that has an impact on how they execute motor actions when playing their instrument and the sensitivity of those movements. One study that may be useful in understanding these findings examined changes in forearm movement and stress reactivity in a population of workers experiencing work-related upper extremity disorders (WRUED) (Van Galen, Muller, Meulenbroek, & Van Gemmert, 2002). While this study confirmed that high frequency usage, static postures of the proximal musculature, and high force levels in the context of repetitive actions are strongly associated with the onset of WRUEDs, psychosocial factors, in particular, anxiety, had a mediating role in the onset and severity of WRUEDs. These authors proposed that anxiety and other psychosocial stressors, such as time pressure, task difficulty and emotional threat, increase muscular stiffness, which contributes to the onset of WRUEDs. When placed under stress, highly anxious, but not low anxious participants, who were required to move their forearms to perform a task, showed increased static muscle activity, that is, antagonistic activation. However, the reverse relationship between high and low anxious participants was seen for the response of the wrist stabilization muscles, leading the researchers to conclude that task stressors and anxiety may exert different effects on proximal and distal musculatures. A similar finding regarding the effects of task stressors on proximal and distal musculatures was reported in a study of EMG activation in the left trapezius muscles of tertiary level flute players (Kenny, Fortune, & Ackermann, 2011).
The relationship between anxiety, depression and musculoskeletal pain is very frequently observed but difficult to disentangle, particularly with respect to the role of gender in these associations. A recent study of 500 primary care patients with musculoskeletal pain, of whom 250 were also diagnosed with depression, found that depressed patients reported more psychosocial stressors and more severe anxiety and these factors in turn were associated with more severe depression. There were no sex differences in these effects (Poleshuck et al., 2009). The effects of gender were ambiguous in the Van Galen et al. (2002) study and we are unable to clearly account for the differences between males and females in trigger point pain scores at the highest level of MPA in our study. In fact, an experimental pain study (Frot, Feine, & Bushnell, 2004) reported opposite results to ours. That study compared pain responses of men and women to pain induced by topical capsaicin. Results indicated that women rated pain intensity higher than men, consistent with our findings, but that men reported more anxiety related to pain, even at lower pain intensity ratings.
This paper has confirmed the consistent findings of previous studies that professional orchestral musicians endure significant performance-related pain in the execution of their duties. It is the first study to reveal the complex relationships between PRMD, trigger points and psychosocial factors. In particular, depression and music performance anxiety may have important implications for the management and treatment of PRMD in professional musicians. The results suggest that PRMD may not be able to be treated effectively without considering the observed relationships between PRMD, depression and music performance anxiety. Future studies should examine whether the treatment for PRMD in professional musicians would be more effective if depression and/or music performance anxiety were assessed and, where indicated, treated concurrently.
Footnotes
Funding
This paper forms part of the Sound Practice research project, which was funded by the Australia Research Council (ARC) (Project ID: LP0989486) and The Australia Council for the Arts (ACA), and which received in-kind support from the eight major symphony and pit orchestras of Australia.