
Abstract
The growing risk of the development of problem behaviors in adolescents (ages 10–15) requires effective methods for prevention, supporting self-regulative capacities. Music listening as an effective self-regulative tool for emotions and behavioral adaptation for adolescents and youth is widely studied. However, music therapy enhancing the development of emotion regulation skills in schools is rare. The application of rap in clinical cases of music therapy appears to have a beneficial regulative effect on this population. The aim of this study is to investigate the performance of RapMusicTherapy (RMT) in a non-clinical, school-based program to support self-regulative abilities for well-being and to reduce the risk of low grades attributable to troubled mental health at an early stage.
All adolescents in Grade 8 of a public school will be invited to participate, and randomly assigned, either to RMT or to regular classes. RMT will be applied once a week during 4 months. After obtaining written informed consent by parents, measurements will take place at baseline (start of study), after 4 months (end of RMT) and again after 4 months without RMT (follow-up). Primary outcome data include measures of psychological well-being, emotion regulation, self-esteem, self-description, language development, executive functioning and the rest–activity rhythm. Secondary outcome data consist of subjective experiences of participants, collected in follow-up interviews with experimental group respondents.
RMT is developed for application in school-based settings. This is the first study to focus on RMT as an intervention for emotion regulation in order to evaluate the effects of rap on the self-regulative capacities of adolescents, in support of their well-being. This study protocol aims to outline the method and procedures involved, and to increase attention and awareness of the potential for collaborations involving music, therapy and education for future investigations.
Keywords
According to the Dutch Institute for Youth (Nederlands Jeugdinstituut, 2014), the growing population of children, adolescents, and youth with anti-social behavior (CD/ODD, attachment disorders, ADHD) requires more effective protocols for treatment as well as for prevention of problem behavior. Violence, abuse, and neglect in parental and social environments are typical potential sources for the development of psychopathological behavior (Dam, Nijhof, Scholte & Veerman, 2010). A study evaluated Dutch youth treatment programs for juvenile care (N = 514; mean age = 15), and presented a high rate of levels of trauma: 56% of the males and females showed co-morbidity and trauma, often not or only partly diagnosed (Dam et al., 2010). Reports from the UK support the Dutch findings and state that 1 in 10 children and adolescents aged between 5 and 15 are diagnosed with mental health problems (Carr & Wigram, 2009). A large socio-demographic study from the USA (N = 10,123) claims that one in every four or five adolescents has a mental health disorder: the biggest group showed patterns of anxiety disorder (31.0%), followed by behavior disorders (19.1%), mood disorders (14.3%) and substance use disorder (11.4%) (Merikangas et al., 2010). Additionally, the correlation between well-being and psychopathology in middle school showed a decline in academic achievement of troubled mental health students (N = 300) at a significantly fast rate (Suldo, Thalji & Ferron, 2011).
In order to prevent or reduce the risk for mental health disorders, the development of self-regulative capacities necessary for dynamic and reorganizational processes of emotional and behavioral adaptation is desirable (Blair & Diamond, 2008; Crocker 2002; Diamond & Lee, 2011; Porges, 2011). Difficulties in emotion regulative capacities are reported by clinical studies of patients with ODD/CD, (comorbid) behavioral difficulties, childhood depression, Borderline Personality Disorder and anorexia, caused by stress, traumatic experiences and family dysfunction (Mennin, Heimberg, Turk & Fresco, 2005; Uhlig, Jaschke & Scherder, 2013). Classroom studies demonstrate that the primary sources of difficulties in schools are related to problems with self-regulation, in particular with respect to directing and controlling attention and behavior impulses (Blair & Diamond, 2008; Kovacs et al., 2006; Lewit & Baker, 1995; Raver, 2002). To prevent underachievement at school and to encourage children to develop self-regulation abilities at an early age, interventions for motivational engagement seem particularly appropriate (Aldao, 2013; Blair & Diamond, 2008; Gross, 2002; Turner & Husman, 2008).
Therefore, collaboration involving music, therapy, and education seems desirable, to perform multidisciplinary studies, and to bring music back into the classroom to facilitate the healthy development of children and youth (Kraus, Hornickel, Strait, Slater & Thompson, 2014). This study protocol describes the planned performance of a Randomized Controlled Trial (RCT), and presents its characteristics and the challenges of applied music and assessment. RCTs are never sufficient by themselves without further explanation of the complexity of the applied interventions and measures (Victora, Habicht & Bryce, 2004).
Music and self-regulation
The supposed self-regulative capacity of music presented in this study may motivate engagement, modulate impulses, and offer coping strategies for the well-being of adolescents. The interaction of music with neural functions for modulating emotions, affecting mood and stress, has been extensively studied (Janata & Grafton, 2003; Jeffries, Fritz & Braun, 2003; Juslin & Laukka, 2004; Koelsch, 2011; Koelsch et al., 2013; Laiho, 2004; Molinari, Leggio & Thaut, 2007; Saarikallio, 2008; Sloboda & O’Neill, 2001; Stegemann, 2013). Moore (2013) presents preliminary neurological evidence for the specific use of music listening, singing or improvising in facilitating emotion regulation in music therapy. The potential of music in regulating emotions occurs because, if sensory information is unthreatening, amygdala activity decreases. Mostly, music is unthreatening, but some clinical interventions involve therapeutic stimulation to maintain or increase amygdala activity. This in turn intensifies the emotional experience in response to pleasant and unpleasant sounds (Moore, 2013), which are crucial for the regulative process of behavior change. Commonly, music listening is demonstrated as a self-regulative tool for youth (Miranda, 2012; Rentfrow, 2012; Saarikallio, 2008; Saarikallio & Erkkilä, 2007; Thoma et al., 2012), and is viewed as a very individual but cross-culturally accepted, therapeutic instrument (Uhlig et al., 2013). Likewise, increased behavioral self-regulation through singing improved with age, as reported by Winsler, Ducenne, and Koury (2011), who studied 3–4 yearolds. Support for effective self-regulation in clinical cases of music therapy is presented by Plener et al. (Plener, Sukale, Groschwitz, Pavlic & Fegert, 2014; Plener, Sukale, Ludolph & Stegemann, 2010), who worked with self-injuring adolescents using rock music. Similarly, music therapists (Hadley & Yancy, 2011; Viega, 2013) present cases of adverse childhood experiences and difficult-to-engage youth and their ability for emotional transformation. They describe the use of rap for self-regulation, development of coping strategies and behavioral changes. Specifically, rap is used to motivate youth to engage in their personal and social identification process, and to modulate behavior during their music therapeutic treatment. Rap is a “bridge” between talking and singing because it creates a safe environment where primary emotions can be expressed vocally and transformed into words (Uhlig, 2011). Rap is based on rhythm and offers a predictable, grounding pattern, while creating stability and reliability for the expression of “true” feelings (Short, 2013). Rap is often associated with negatively influencing youth due to its promotion of antisocial messages of violence (Short, 2013), whereas the use of rap in music therapy engages and reflects upon these negative themes, supports the expression of the personal, the “true” emotions, and helps them transform. These results from music therapy suggest that rap interventions can aid emotional regulation and might decrease aggressive states (Hakvoort, 2015; McFerran, 2011; Short, 2013, Uhlig, 2011; Uhlig, Dimitriadis, Hakvoort, Jansen & Scherder submitted paper). The preference of youth for popular music, such as rap, hip hop and rock, plays a central role for their personal well-being, as a means of improving insight into their lives by allowing them to express and discuss these emotions and thoughts in music therapy.
Main study
Music intervention
Despite these regulative benefits of music for (non)-clinical populations, quantitative studies of music therapy interventions in schools for the enhancement of emotion regulation skills for well-being are rare. Using rap as a motivational tool for an early intervention to combat possible threats to mental health in adolescence seems a suitable therapeutic application, although behavioral problems are likely develop around the age of 11 (Merikangas et al., 2010). This study is set up as a school-based classroom intervention, to reduce the risk of development of problem behaviors and poor grades. RapMusicTherapy (RMT) employs a therapeutic structure with a regulative rhythmical framework, thereby facilitating the overall emotional expression of singing and rapping, and word development for rhyme in song-lyrics. Through rhythm and repetitive rhythmic engagement (Grahn, 2009; Thaut, 2013), rap might stimulate the brain by integrating and organizing sensations, whereas singing (Callan, Kawato, Parsons & Turner, 2007) can involve a greater emotional component in the brain adaptation necessary for learning (Leins, Spintge & Thaut, 2009). More specifically, the usefulness of rap comes from the application of rhythm for sensory coordination and entrainment, as well as by providing predictable patterns, which can serve as a grounding function. Entrainment, the process in which rhythms displayed by two or more phenomena become synchronized, might develop:
with one of the rhythms often being more powerful or dominant and capturing the rhythm of the other. This does not mean, however, that the rhythmic patterns will coincide or overlap exactly; instead, it means the patterns will maintain a consistent relationship with each other (Bluedorn, 2002, p. 149).
Rhythmic patterns might entrain neural oscillators by stimulating them to maintain consistent relationships with each other, thereby enabling the synchronization of both perception and action (Janata & Grafton, 2003; Molinari et al., 2007; Thaut, McIntosh & Hoemberg, 2015). A melody can provide a recall aid supporting the singer/rapper to express emotions, to identify and recognize them in words, and to encode and retrieve a text by making it more memorable. RMT offers a predictable rhythmical framework in which information can be ‘chunked into phrases’ (Wallace & Hammill, 1994), and both positive and negative emotions can be exposed, processed, transformed, and regulated during live group performances. Individuals and groups of adolescents can take the lead in selecting styles, loops, or lyrics of the songs, and providing a platform for group discussion. The potential modulation of impulses through the rewarding and emotionally evocative nature of music (Patel, 2011) can be a crucial process for adolescents’ development of well-being. Theoretical argumentation for the current protocol and the practices of music therapy for emotion regulation mentioned above are presented elsewhere (Hakvoort, 2015; Moore, 2013; Short, 2013; Travis, 2013; Uhlig et al., 2013).
The study population of “adolescents” is defined as such due to the majority of participants being between 9 and 12 years old. According to a differentiation between “children” and “youth” made by the United Nations: “children” is applied until age of 10, “adolescents” from 10, and “youth” from 15–24 years of age (United Nations, n.d.). Children and adolescents’ early onset of mental disorders begins with anxiety around 6 years, with behavior problems following by 11 years old, mood disorders at 13 years, and substance use at 15 years old. Pathological symptoms increase in severity with age whereby adolescents generally show relatively fewer symptoms compared to (older) youth (Merikangas et al., 2010). The participation in RMT in a school-based setting may help to gain early benefits as a prevention strategy for the complex and emotional transition from adolescence to youth. This article on RMT describes a first investigation of applying rap and singing for emotion regulation in a school-based music (alteration) program for adolescents, promoting their healthy development (Kraus et al., 2014). The RMT method aims to support emotion regulation as a stimulating approach for each individual to express emotions, and to identify and discuss personal, musical and peer preferences through rap and song in a safe therapeutic environment.
Method
Design
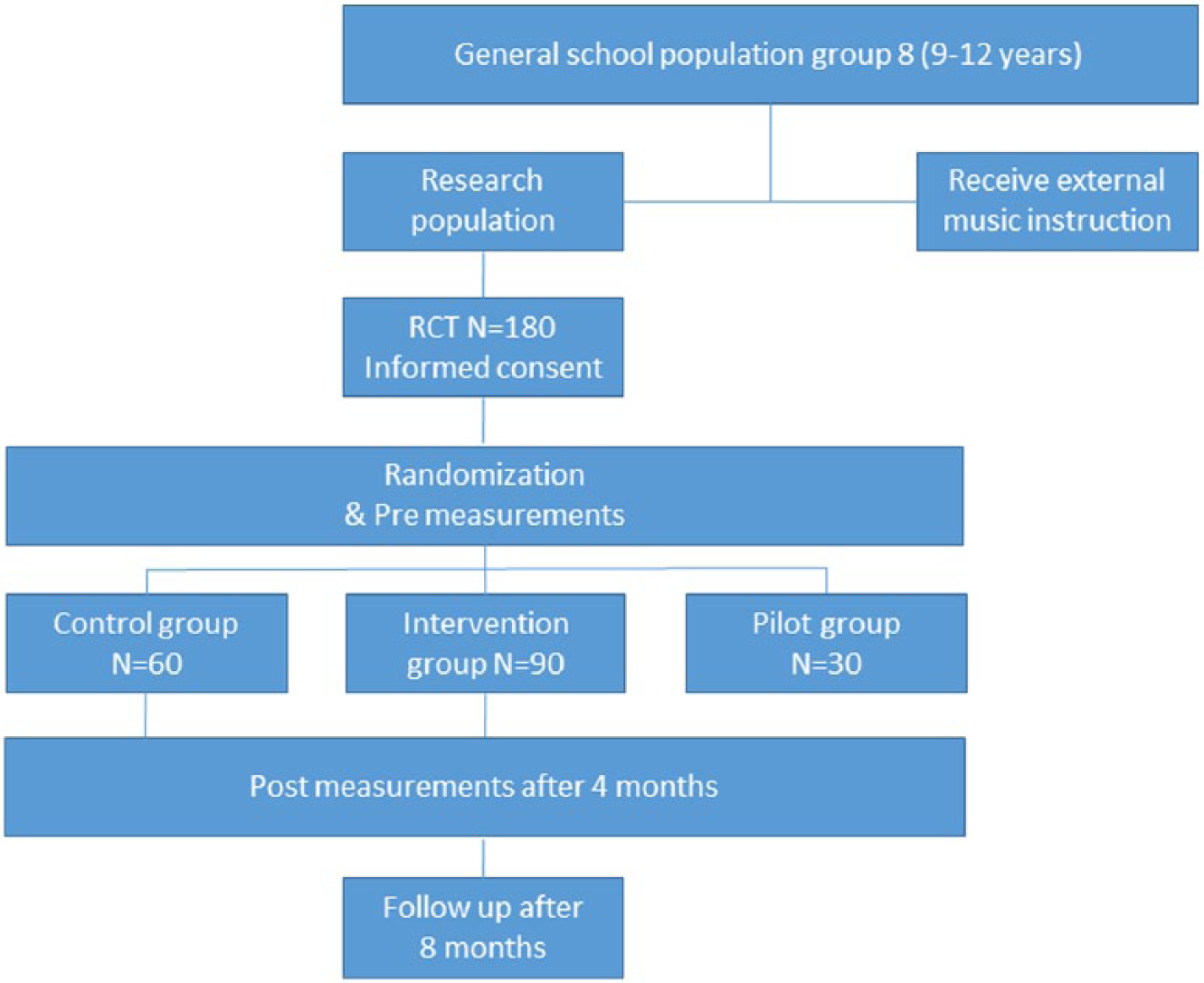
This study is designed as a randomized controlled trial (RCT) with adolescents in a public school in the Netherlands (see Figure 1). Furthermore, with the described intervention we will study the potential of rap and singing to support self-regulation of emotional processes and behavior. The development and performance of RMT is designed as an active music intervention. This study protocol articel describes this development and the characteristics of RMT prior to data analysis, as it is needed for RCT trials, to support analyses for adequacy and plausibility (Michie et al., 2011; Victora et al, 2004).
Trial design.
Randomization
All participating adolescents from Grade 8 will be assigned to music interventions (8 classes). Two classes will participate in an external music program and will be excluded from this research. Six classes will be selected for the RMT and will be randomly assigned for participation in this study (180 children): three classes will form the experimental groups (90) and two classes will form the control groups (60). One class will be assigned to the pilot sessions (30) and will be excluded from the main research. A list of six classes will be sent to an independent researcher from Vrije Universiteit Amsterdam who will select the pilot, experimental, and control groups, blinded to the identity of the classes. After obtaining written informed consent from parents (for the pilot population as well), the researchers will start with the preparation of the RMT. Four performing music therapists of the RMT will be uninformed about adolescent’s school records, behavior problems, difficulties, and diagnoses as well as which adolescents actually partake in data collection.
Intervention
Previous school-based prevention research suggests 8–12 sessions of 50–60 minutes is adequate for effectiveness of the program (Calear & Christensen, 2010; Merry, McDowell, Wild, Bir, & Cunliffe, 2004). This study will employ an estimated 16 sessions of 45 minutes a week. Ninety Adolescents, divided into three classes, will receive the RMT. This intervention is designed for large groups of 30 adolescents per class. Two music therapists will work together during 8 weeks in one class, after which the classes will be split into subgroups of 2 × 15 adolescents per class. Each therapist will then continue with a subgroup of 15 adolescents, working on specific group and individual themes, and preparing the group for recordings of individual or group rap-songs. Experienced music therapists, experts in using rap, will be hired and trained prior to performance of the RMT. Therapists and assistants will undergo supervision and evaluation sessions regarding verbal boundaries during rap, and considerations about therapeutic themes, such as relationships (Short, 2013), provided by the first author during the research project. Both RMT and control groups will receive instructions for 45 minutes a week during school time. The RMT will be performed by trained music therapists, and the controls will receive non-specific music instructions by classroom teachers.
RapMusicTherapy
The RMT protocol is designed to stimulate regulative emotional processing. A detailed description of the music-based intervention program of RMT, as performed in this study, will be presented in other studies for further research and transparency, as recommended by Moore (2013) and Robb, Burns and Carpenter (2011). The protocol is constructed around components of cognitive behavior therapy and psycho-education, and is based on three elements of music used for RapMusicTherapy: (1) rhythm, (2) vocal expression of singing and rapping, and (3) development of vocal work, words and song lyrics (Uhlig, 2011). These elements are elaborated on below.
Rhythm and rhythmic stimulation have profound effects in sensory coordination input to entrain timing functions (Thaut, 2013; Thaut et al., 2014), supporting synchronization of perception and action. By offering rhythmic patterns using programmed rhythms (loops) and body-percussion, motor control and speech in particular will be activated. Body percussion exercises combine visual and physical expressions and encourage synchronization and develop predictability. By repeating the rhythmic patterns of participants, adjusting their tempi and dynamics, the therapist establishes moments of entrainment and facilitates a grounding pattern for group stability.
Singing engages an auditory-motor feedback loop in the brain more than other musical modes (Wan, Rüber, Hohmann, & Schlaug, 2010). Singing reflects both right-side dominance and left-side activity and involves greater emotional engagement, thereby stimulating alternative ways of information exchange in the brain (Callan et al., 2006). By offering vocal sounds or words in a rhythm (rap), participants are invited firstly to imitate sounds, and secondly to stimulate the creation of more words. By fitting improvised or written lyrics into a rhythm and structuring vocal sounds, chunking words and developing poetic patterns, rhythmic speech and singing melodic lines induce mood changes. During vocal interaction the imitation of vocal sounds implements a call-and-response technique, with the aim of stimulating feelings of comfort, trust and pleasure.
Vocal work encourages learning of verbal material through song (Leins et al., 2009). By creating simple vocal rhythmical patterns, rapping or singing alone or together, repeating vocal sounds of participants to develop dialogue and contain feelings, a sense of safety and decreased anxiety is induced. Production of individual lyrics/poems is stimulated by combinations of methods applying a fill-in-the-blank technique, integrating increased communication during the interaction, exchanging emotions and feelings in sound, stimulating word recall and supporting further language development by rhyming more words.
The experience of emotional satisfaction when expressing and sharing pleasure, sadness or aggression in a rap or song will indicate individual changes. Trained therapists provide a structured and therapeutic environment, anticipate strong emotional expressions like offensive language used in rap or song (Short, 2013), and handle ethical themes with care. According to the need for adjustments, themes about performance or transfer will first undergo therapeutic consideration and will be completed by offering participants recordings to share their personal rap or song developments with outsiders (peers, parents and teachers).
Participants
All adolescents of Grade 8 of a public school (N = 180) in the Netherlands will be informed about this study. The head of school granted permission to ask parents for consent for data collection with their adolescents and to perform the research during school hours as part of a regular (music) program. Participants will be recruited by the researchers and the classroom teacher at De Lanteerne, a Jena-plan-school in Nijmegen, centered around the concept of community and learning through self-discovery. All participants will be boys and girls aged between 9 and 12 years old, as the Jena-plan-school includes different ages in one class. All participants will partake in the project of their own class during regular school hours. Two classes will receive external music instructions, therefore six out of the eight classes will participate in the RMT. No selection process for indication of behavior and/or developmental problems will be held beforehand, thus no child will be excluded from the music experience. Both adolescents with and without behavior and/or developmental delays will be included in the same study condition. Applied RMT is designed for these populations and ages with sufficient flexibility for therapeutic adjustments based on developmental levels and capacities of children. All parents of Grade 8 students will be informed about the study by verbal and written introductions explaining the content and procedures of this study. Parents consenting to data collection from their child will be required to sign informed consent forms for permission to participate and to allow audio and video recordings during the sessions. Standardized tests will be used at the beginning and end of the study for adolescents, parents and teachers participating in data collection. Adolescents partaking in the RMT without parental permission for data collection will not be tested nor interviewed.
Measurements and procedures
All participants will undergo two measurements: baseline measurements (start of the study) and post measurements (end of music intervention). The two measurements consist of three different assessments to investigate whether a change has occurred in an adolescent’s emotional or behavioral functioning. Assessment of psychological well-being has three standardized written tests (A); assessment of cognitive function has one standardized written school test, and three tests of executive function using an iPad application (B); and assessment of rest–activity rhythm incorporates the use of Actiwatches, with which the sleep–wake patterns of participants can be recorded (C). The follow-up study will be performed by interviewing the experimental group (four months after intervention). Due to pilot study experiences, adjustments will be made to the follow-up study: a personal investigation of each individual participant is needed instead of a third “text-based-test” assessment. Assessing qualitatively seems to rely closer on participants’ experience, whereas quantitative assessments were rated as “distant” by adolescents during their individual emotional experience of music. Through the interviews (D), we aim to present a qualitative inquiry of the “lived experience” of the adolescents and weave a complementary multi-methodical approach into the RCT. Psychological and iPad measurement tests will be combined in one session, with a duration of about 40–60 minutes (dependent on the participant). Trained students of the Clinical Neuropsychology master of the Vrije Universiteit Amsterdam will administer the tests and perform the interviews. During the weeks of the psychological testing (pre- and post-measurements), participants will wear an Actiwatch activity monitor for one week. Measurement methods A–D are elaborated upon below.
Primary outcome measures
Assessments of psychological well-being
A1. Emotion regulation: Difficulties in Emotion Regulation Scale (DERS) is designed to evaluate the functionality of emotion regulation (Gratz & Roemer, 2004). The DERS is used for adults, adolescents up to the age of 13, and will in this study be used with younger adolescents (9–12), as recommended by Neumann, van Lier, Gratz and Koot (2009).
A2. Self-esteem: Self-perception Profile for Children (CBSK; Competentie Belevingsschaal voor kinderen) for children aged 8–11 years. Children’s self-esteem will be measured to indicate their own self-perception (Treffers et al., 2004).
A3. Self-description: Strength and Difficulty Questionnaire (SDQ) to identify children’s risk of psychiatric disorders, ages 4–16 years. The SDQ gives a description of the child’s strengths and difficulties, including reports about parent and teacher SDQ, and will be used for the prevention of health problems in the youth population (Muris, Meesters, Eijkelenboom, & Vincken, 2004).
Assessment of cognitive functions
B1. Wechsler Intelligence tests for children: language development (WISC 4: Verbal Comprehension Index, VCI). Vocabulary: the examinee is asked to define a provided word. The verbal examination aims to investigate affiliations between music and language (Ettlinger, Margulis & Wong, 2011).
B2. Tower of London Test (TOL), to measure neuropsychological executive functions or problem-solving skills. This is a computerized planning test to research correlation between self-control and executive function and music (Anderson, Anderson & Lajoie, 1996; Diamond & Lee, 2011).
B3. Trailmaking test (TMT), to measure neuropsychological executive functions or impairment in multiple cognitive domains. The Trail-Making Test is a measure for mental speed and mental flexibility. This is a computerized test, which aims to investigate the enhancement of executive function through music (Bialystok & DePape, 2009; Degé, Kubicek, & Schwarzer, 2011; Schellenberg, 2011).
B4. Stop test (ST) to measure neuropsychological executive functions of self-control, performance on cognitive tasks of inhibition, and working memory (Oosterlaan, Logan, & Sergeant, 1998). This is a computerized test, studying development of self-regulation skills through music (Winsler et al., 2011).
Assessment of rest–activity rhythm (Actiwatch)
Actiwatch (AW 2), to test sleep wake pattern of participants. Actiwatches and sleep log information will be gathered over 5 consecutive days, using a sleep-monitoring device (Actiwatch®, n.d.; Gaina, Sekine, Chen, Hamanishi, & Kagamimori, 2004). Investigation of Actiwatch data of children is important, because a good sleep is recuperative. In this way the correlation with cognitive problems, like inattention as well as emotional instability and impulsivity from shorter sleep duration, can be assessed (Gruber, Cassoff, Frenette, Wiebe, & Carrier, 2012). Furthermore, intensity and regulation of sleep problems (El-Sheikh & Buckhalt, 2005) and sleep duration and regularity associated with behavioral problems (Pesonen et al., 2010) can be studied. Analysis of sleep patterns include start, latency, end, time, and efficiency of sleep, and will be related to psychological testing, and for the first time related to music, as a non “text-based test,” as Schellenberg (2011) has defined.
Secondary outcome measures
Interviews
A qualitative inquiry will be set up to collect information about “how” music affects adolescents, and their emotional reality as “lived music experience.” Adolescents’ participation will consist of accounts of their subjective experiences, yielding narrative data on the application of the intervention. Insight into what conditions are required for an effective application of intervention is useful information for refinement and further development of the intervention protocol (Hesse-Biber, 2012), as well as the detection of unexpected effects that otherwise go unnoticed.
Demographic and control variables
Demographic data information will be provided by parents, consisting of age, gender, marital status of parents and family structure, working status, parents’ education, parents’ interests and hobbies, family activities, and former music education. From the perspective of the outcome measures it will be investigated whether there are correlations with demographic and family circumstances for each child (Rescorla et al., 2007; Silk, Steinberg & Morris, 2003). To define whether a alteration has occurred in a child’s emotional and behavioral functioning, several questions will be asked during the condition assignment to compare baseline with later test sessions and circumstances.
Statistical analysis
Statistical analysis will be performed on intention to treat (ITT) to preserve the sample size (Gupta, 2011) and to minimize uncontrolled covariates whose effects may be confounded with the intervention effect (Porta, Bonet & Cobo, 2007). Differences between the music and control group in the two sessions of measurements will be analyzed with a repeated-measures design. Differences between participants in school, class, time, age, and gender will be considered as within-between interaction variables. Measuring the possible effects of the RMT regarding effects on rest–activity rhythm, the analysis of the Actiwatch is constructed around the primary outcome of baseline measurements.
Sample size
The calculations for adequate sample sizes are based on the outcomes of the literature review on applied music intervention, resulting in a modest sample size of N = 90 for the first study of school adolescents (ages 9–12). In line with the literature review, no existing studies apply a music (therapeutic) intervention for emotion regulation in school settings. Primarily, measurements of music effects for emotion regulation purposes are based on verbal questionnaires without applied music interventions (Uhlig et al., 2013). Accordingly, our study calculates an effect size of f = 0.15, which is to be considered a small effect (Faul, Erdfelder, Lang & Buchner, 2007). For a required 80% power threshold, the estimated sample size requirement per group is 45, with two planned measurements. Anticipating dropout rates, the study population is targeted at 120 participants. The feasibility of a small effect size (f = 0.15) for the planned sample size, involving six school classes, allows for a reduced risk of Type II errors (Banerjee, Chitnis, Jadhav, Bhawalkar & Chaudhury, 2009).
Ethical and legal consideration
The study protocol has been reviewed and approved by the scientific and ethical review committee of the Vrije Universiteit Amsterdam (Vaste Commissie Wetenschap en Ethiek; VCWE), an independent advisory board of the Faculty of Psychology and Education. Ethical aspects of the protocol were approved and the study has been included in the research registration system of VCWE registration number 2500. VCWE registration and approval was sufficient, consequently no CCMO (Central Committee on Research Involving Human Subjects) or Medical Ethical Committee registration was required, which permits performing this research in a non-clinical school setting.
Discussion
The goal of the present study is to examine the effects of RMT on emotion regulation. The study focuses primarily on rap and singing for self-regulative purposes in a school-group setting: on the individualized motivation to express both joyful and uncomfortable feelings, which are sensitive to emotional and behavioral difficulties. Alongside this, the identification of personal and peer themes for coping or well-being and possible prevention purpose will be assessed. Typical peer themes of adolescents are bullying and victimization (harassment, teasing, bothering) as well as hidden and embarrassing feelings and thoughts about love and friendship (Olweus, 2003; Roede & Felix, 2009).
A secondary focus of the study is to contribute to development of “practice-based” and “evidence-based” methods; RMT assesses the effects of applied motivational usage of rap and singing interventions.
The strength of this study is the application of RMT for evaluation of its impact on short-term effects of the self-regulative ability of adolescents (over 4 months). To our knowledge, the current study is the first offering an individualized focus on the under-represented subject of music and emotion regulation in a school group setting. This study brings music back into the classroom without high costs and individual encounters; rap and singing interventions do not require specific fine-motoric skill training, nor the use of expensive instruments. Also, the self-regulative ability for emotional and behavioral adaptation is assessed during a regular school activity in a typical peer environment.
Challenges of this study are the short RMT cycles of 45 minutes once a week over 4 months (16 sessions). Adolescents participate in extra-school activities (preparation for holidays or vacations) and due to absence from school, interference with music schedules may limit the number of sessions. Another concern is the diversity of the group in a school, representing realistic class conditions; this might influence outcomes. Possibly a small number of children with psychopathological or sensitive developmental patterns will participate, compared to children with normal progress. Some parents might not allow their child to participate in the study because of the risk of “over-testing.” A central concern is the use of psychological tests, which should be approached with caution. Specialized, validated instruments are needed for the assessment of effects of the emotion regulative processes (Aldao, 2013; Gratz & Roemer, 2004), and the applied music interventions (Robb et al., 2011). Therefore, this study addresses Schellenberg’s (2011) concern, as associations between music interventions and emotional (regulative) intelligence might not be evident from “text-based tests” of emotion regulation and “verbal intelligence.”
In conclusion, the RMT is an innovative approach examining the possible benefits of rap and singing on emotion regulative processes, executive functions, and rest–activity rhythm monitoring. Results of the study are expected to contribute substantially to the application of music in classroom settings for dynamic regulative purposes, and to reflect on methods to study suitable tests/measures of music experiences. Use of standardized protocols, such as RMT, can make it easier to carry out future studies maintaining the comparability of results between studies. Lastly, this study protocol prior to analysis is well-regarded for use in RCT’s, enabling readers to comprehend the characteristics and development of the investigation which are otherwise difficult to understand. It aims to elicit more attention and awareness for collaborations involving music, therapy, and education, by giving insight into what methods are applied in order to plan future investigations into music interventions in schools.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.