
Abstract
Although patient-preferred live music (PPLM) can be an effective music therapy intervention for addressing cancer-related fatigue (CRF) in adult oncology patients, there is a gap in the literature specific to patients’ experiences of how PPLM impacts CRF. The primary purpose of this interpretivist study was to understand the mechanisms by which PPLM impacts CRF from the patients’ perspectives. The secondary purpose was to gain insight into patients’ song choice rationales and their ensuing function within PPLM. We provided PPLM and conducted semi-structured interviews with adult oncology patients (N = 5) on a blood and marrow transplant unit. We used an inductive approach to thematic analysis to analyze interview transcripts and achieved trustworthiness through independent analyses of transcripts as well as peer review of codes and themes. Participants described how PPLM provided CRF symptomatic relief by facilitating emotional release and being an aesthetically pleasing distraction. Participants noted they chose songs because of memorable experiences and for musical elements and components, while explaining that PPLM facilitated reminiscence, promoted relaxation and restful states, and encouraged reflection through the lyrics. Results provide an initial patient-centric understanding of how and why PPLM might impact CRF. Implications for clinical practice, limitations, and suggestions for future research are provided.
Cancer is the second most common cause of death in the United States and accounts for nearly one of every four deaths (American Cancer Society, 2018a). While the rates of cancer deaths are declining annually due to better detection and treatment, the number of new cases has increased due to population growth and aging (Centers for Disease Control and Prevention, 2018). Therefore, cancer continues to represent a substantial social concern, impacting those who are diagnosed in addition to their social networks.
Cancer is a group of diseases portrayed by the uncontrolled growth and spread of abnormal cells that can lead to death if not contained (American Cancer Society, 2018a). Cancer treatments can include surgery, radiation, chemotherapy, hormone therapy, and immune therapy. When certain types of cancer prevent the body from producing enough healthy blood cells, patients 1 may be treated with a blood or marrow transplant (BMT; National Heart, Lung, and Blood Institute, 2016). A BMT procedure replaces abnormal stem cells with healthy stem cells after radiation or chemotherapy. Depending on a patient’s general health, medical circumstances, and whether chemotherapy and radiation are needed, hospitalization may be necessary for weeks or even months before and after a BMT procedure (National Heart, Lung, and Blood Institute, 2016).
Pharmacological treatments and radiation targeting cancer can cause a variety of symptoms including nausea, vomiting, diarrhea, tiredness, mouth sores, skin rashes, hair loss, or liver damage (National Heart, Lung, and Blood Institute, 2018). However, oncology patients have consistently indicated fatigue as the most persistent and commonly occurring side effect of cancer, its treatments, and BMT procedures (Jacobsen et al., 1999; Stasi, Abriani, Beccaglia, Terzoli, & Amadori, 2003; Visovsky & Schneider, 2003). Cancer-related fatigue (CRF) causes drastically more distress than everyday fatigue, is not relieved by sleep, and can be a distressing and debilitating experience for cancer patients (American Cancer Society, 2018b). CRF can negatively impact mood, physical abilities, work performance, social interaction, family care, cognitive performance, schoolwork, community activities, and sense of self (Curt et al., 2000; Stone & Minton, 2009; Wu & McSweeney, 2007). CRF can cause more distress than pain, nausea, vomiting, or depression and can last years, frequently continuing after treatment ends (American Cancer Society, 2018b). As such, effective treatments for CRF symptom management are imperative.
Although preliminary studies have indicated positive results (Andersen, Pitts, & Silverman, 2012; Fredenburg & Silverman, 2014a, 2014b; Rosenow & Silverman, 2014), research literature concerning music therapy with adult BMT patients is scarce. Fredenburg and Silverman (2014b) found a single session of music therapy in the form of patient-preferred live music (PPLM) to be an effective intervention for positive and negative affect and pain in patients on a BMT unit. In related BMT studies, PPLM was effective in targeting anxiety and fatigue while promoting relaxation and motivation (Fredenburg & Silverman, 2014a; Rosenow & Silverman, 2014). Andersen et al. (2012) evaluated the effects of PPLM on CRF and found a significant between-group difference, with experimental participants having less fatigue than control participants. In addition, experimental participants tended to have slightly higher mean energy scores than control participants. In a randomized controlled study, Reimnitz and Silverman (2018) investigated the effects of PPLM in BMT patients and found significant between-group differences in CRF and pain. However, additional objectivist music therapy CRF research is needed to augment the literature base (Bradt, Dileo, Magill, & Teague, 2016). Interpretivist research investigating mechanisms within music therapy responsible for impacting CRF is also warranted.
PPLM is a frequently used music therapy intervention in adult medical settings to address outcomes such as fatigue, pain, mood, and affect (Silverman, Letwin, & Nuehring, 2016). PPLM comprises music, the patient’s preferences, choice and autonomy, and live performance. Potentially contributing to the positive effects of PPLM, researchers have noted that exposure to familiar stimuli and the act of making a choice may be neurologically reinforcing (Ramaswami & Silverman, 2018). In addition, researchers have found preferences for live music—compared to recorded music—during music interventions (Cassileth, Vickers, & Magill, 2003; Chaput-McGovern & Silverman, 2012; Silverman et al., 2016; Standley, 1986).
There is a contemporary emphasis that evidence-informed music therapy integrates patients’ values, experiences, and evaluation of services (Ansdell & Meehan, 2010). To the best of our knowledge, there is no current literature describing patients’ lived experiences of how music therapy in the form of PPLM impacts CRF, their rationales for their preferred song choices, or their perceptions of how those songs functioned for them. These data could better inform music therapy clinicians and generate effective PPLM protocols to augment the quality of care. Therefore, the purpose of this study was to gain an understanding of how oncology patients on a BMT unit experienced PPLM to impact CRF, why patients choose particular songs, and what function the music served. This study addressed the following research questions:
What are patients’ experiences of how PPLM affects CRF?
Why do BMT patients request particular songs during PPLM?
How do song choices within PPLM function?
Method
Participants
Participants (N = 5) were adult oncology patients on a BMT unit within a teaching hospital in the Midwestern region of the United States. Patients on this unit were recovering from a current or previous BMT, returning to the hospital due to infection or other complications, or were undergoing chemotherapy, radiation, or both chemotherapy and radiation in preparation for their BMT procedure. All hospitalized adults ages 18 and above on the BMT unit during the study period who could read and understand English were eligible to participate in this purposely inclusive study. Our university and hospital shared an Institutional Review Board (IRB) that approved the study prior to data collection (STUDY00000572). We completed all required research training to conduct this study and provide PPLM on the BMT unit.
Design
To best answer our research questions, we employed an interpretivist paradigm using qualitative data. To provide music therapy to all interested patients on the unit and be as inclusive as possible, we used a transdiagnostic approach (Silverman, 2015) in a single-session design wherein all patients on the BMT unit were eligible to participate, regardless of cancer type or diagnosis. Participants completed individual semi-structured interviews within a 30-min PPLM session.
Procedure
Upon entering a patient’s room, L.R. introduced herself and inquired whether the patient would like to receive music therapy services. If the patient responded in the affirmative, L.R. then asked if the patient would like to voluntarily participate in a research study. Therefore, patients were given the option to receive PPLM only or to receive PPLM and be a participant in the study. If the patient chose to be a research participant, L.R. provided verbal and written information about the study and then obtained informed consent.
L.R. then discussed music preferences with each participant. Based upon the participant’s responses, L.R. either played the participant’s requested song or provided the participant with a song menu and invited them to choose a song. If the participant chose a song that L.R. did not know or that was not on the menu, L.R. offered to learn the song and perform it at a later time. Supported by existing literature (Haack & Silverman, 2016; Selle & Silverman, 2019a, 2019b), the researchers developed the song menu based upon related clinical work with adults at the same hospital. Upon sharing the song selection, each participant was asked to explain why they chose the song. L.R. then played the desired song and then asked the participant to identify the function that the particular song served for them. This process was repeated for a total of three songs. Following the third song, L.R. proceeded to the semi-structured interview about how PPLM may have impacted participants’ CRF. Although participants were allowed to have multiple PPLM sessions, data were only collected during the initial session. L.R. provided songs using her voice and a steel-string acoustic guitar. L.R. audio recorded the entire PPLM session using an iPad. Due to infection concerns, sessions only included L.R. and each participant.
Semi-structured interview
We developed an initial semi-structured interview with six open-ended questions. We then shared the interview draft with a graduate level music therapy class who provided critical feedback to ensure that all questions were non-biased and addressed the research questions. The final version of the interview is depicted in the Appendix.
Qualitative analysis
Due to the exploratory nature of the study, we used an inductive approach to thematic analysis (Braun & Clarke, 2006) as a guiding framework to understand perceived mechanisms targeting CRF and song choice rationale and function of PPLM for adults undergoing BMT. An inductive thematic analysis requires researchers to code data without a pre-existing framework. This “situates the analysis in an open-ended perspective that does not predetermine what should be found in the data” (Potvin, Bradt, & Kesslick, 2015, p. 141). By using this interpretation, researchers are allowed to depict an authentic representation of the participants’ perceptions and descriptions.
We used Braun and Clarke’s (2006) six phases of thematic analysis as a guiding framework for analyzing the transcripts. These steps are detailed below.
Familiarization with the data. L.R. and a paid research assistant transcribed all audio recordings verbatim into word documents. L.R. then reviewed transcripts and compared them with audio recordings. We familiarized the research assistant with the study prior to transcribing interviews.
Generation of initial codes. L.R. began to shape the raw data into meaningful structured units by searching for powerful statements to code within the transcriptions and logging them in the margins of the document or highlighting them directly in text. Initial codes were sent to M.S. to review.
Searching for themes. L.R. used an excel spreadsheet to transfer codes with similar qualities into categories. Similar codes were then grouped together allowing the opportunity to compare and contrast codes between participants. Each code was color-coded to provide additional detail and organization. Broad categories were guided by the research questions. After review, revision, and discussion, themes emerged from the related code categories. The spreadsheet was then sent to M.S. to provide feedback and confirm that themes emerged organically from verbatim participant quotes and experiences.
Reviewing themes. L.R. reviewed audio recordings to refresh her outlook and hear participants’ vocal expressions throughout the interviews. Transcripts were then reread from start to finish without making any changes or additional comments. L.R. then reviewed the excel spreadsheet with color-coded themes to make modifications to the existing interpretation of the data set. To ensure trustworthiness, L.R. and M.S. met to discuss data, review codes, resolve discrepancies, clarify themes, and verify that quotes were grounded in the themes. Feedback was then integrated into the development and refinement of the themes. These data were then triangulated with existing literature.
Defining and naming themes. L.R. worked through the identified themes to ensure that the participants’ experiences and perspectives were accurately represented in each theme.
Producing the report. L.R. and M.S. used direct participant quotes within the descriptions of each theme to help illuminate participants’ experiences and provide insight and understanding into how they felt throughout the process.
Authors’ lens and biases
At the onset of data collection, L.R. was a music therapy graduate student with 1 year of previous experience conducting clinical objectivist research on the same BMT unit using PPLM to address fatigue and pain. M.S. had over 16 years of music therapy experience as a clinician with adults in mental health settings and over 8 years conducting research on the BMT unit. Therefore, data interpretation within this study was informed and shaped by our ongoing clinical, educational, and research experiences. These elements informed our thought processes, ways of knowing, reflexive processes, and interpretation of the data (Stige, Malterud, & Midtgarden, 2009).
Trustworthiness
We shared and discussed transcripts, codes, and themes with two peers who reviewed the data and made suggestions about codes and emerging themes. Although both peers were qualified music therapists, they were unfamiliar with the BMT unit and were therefore able to offer a novel perspective.
After deliberation, we decided that having participants review the themes would not be practical due to the difficulty of following up with them after they had been discharged from the hospital. We recognize that this decision may have lessened trustworthiness. However, this choice ensured the privacy of the participants, avoided reiteration of CRF and the hospital experience, and was thus congruent with our patient-centric approach.
Results
Research question 1: what are patients’ experiences of how PPLM affects CRF?
At the onset of data collection, it became apparent that participants separated how they described CRF and how they described the way PPLM impacted their CRF. We therefore separated themes regarding the description of CRF itself (RQ1A) from themes addressing the impact of PPLM on CRF (RQ1B). Throughout the “Results” section, we depicted codes to support emerging themes and enhance transparency. We included participant quotes to highlight participants’ voices and experiences, provide further contextual support, and to increase transparency.
Description of fatigue (research question 1A)
We identified three major themes related to participants’ descriptions of CRF.
Research question 1A, theme 1: lack of stamina for activities of daily living
Codes: cognitive tasks, physical endurance, recovery, easily tired, physiology
Participants expressed an overwhelming “frustration” regarding inability to complete activities of daily living. These activities included “difficulty carrying on a conversation,” “getting up and out of bed,” “going to the bathroom,” and “walking down the hall.” When speaking about their experiences of CRF, participants articulated an overall “lack of stamina,” and “malaise.” Participants described experiencing “difficulty recovering” and “tiring quickly” from normal tasks, such as using the bathroom, getting out of bed, or walking up a flight of stairs. One participant attributed these difficulties specifically to nutrition and severe weight loss in a short period of time:
It’s a lack of stamina. So, I can do an activity for a short period of time, but then I get very tired quickly and then it takes me a while to recover. It’s just any time I get up and move around, you know, if I have to go from my upstairs bedroom to the bathroom in the main level of the house, going down the stairs, using the bathroom, washing up, going back up the stairs, you know, just a thing you wouldn’t think twice about, normally. It takes me at least twice as long to recover from it, to feel like I’m comfortable and relaxed again. (P2) I just can’t, you know, mentally get it together, and carry on a good conversation. I mean I’m doing okay but that’s even hard work, you know, just carrying on a conversation. (P7)
Research question 1A, theme 2: emotional distress
Codes: lack of mental focus, worry of future
Participants articulated that they experienced “severe emotional fatigue” directly related to their BMT procedures and diagnoses. Participants characterized emotional CRF as temporary “memory loss” or forgetfulness, “distress” about the future and loved ones, and “difficulty talking or following a conversation”:
Emotional fatigue is strong. You know, just worried about the future and I’ve got young kids still . . . so, I just worry about whether I’ll be there for them. At home when you’re mentally fatigued, you don’t have as much physical energy. (P5)
Research question 1A, theme 3: hospital fatigue
Codes: hospital equipment, sleep interference
Participants recognized that many factors influencing their fatigue were directly related to hospital care. These factors included equipment such as intravenous machines, heart-rate monitors, oxygen tanks, and other machines that were necessary for their treatment. In addition, participants discussed experiencing CRF as a result of “little sleep,” frequently caused by “beeping monitors,” “staff coming in the room” throughout the night, bright lights, and inability to “get comfortable”:
Just feeling like you’re drained, you just can’t do anything, partly because of all the things that are going on, the chemo, the machines, and lack of sleep because they’re always coming in and waking me up in the middle of the night and the pumps are always beeping, you know. (P5)
PPLM and CRF (research question 1B)
Specific to PPLM mechanisms that impacted CRF, participants noted that PPLM provided symptomatic relief, facilitated “emotional release,” and provided an aesthetically pleasing “distraction.”
Research question 1B, theme 1: PPLM provides immediate symptomatic relief
Codes: relaxation, less fatigue, symptoms
When speaking about how PPLM directly impacted their fatigue, participants expressed feeling a “relief” from symptoms. One participant noted that PPLM “certainly didn’t make it [fatigue] worse.” Another participant felt that the music therapy shifted her focus from negative symptoms during the session. One participant shared that music therapy was helpful for her and aided her ability to “finally sleep”:
(Music) it’s helpful. It was nice, it helps me relax so I can sleep. Otherwise I haven’t slept all night. It’s as effective as like guided imagery or something like that. I mean, music always makes me feel less fatigued. (P3)
Research question 1B, theme 2: PPLM promotes space for emotional release
Codes: feelings, mental distress, release
Participants reported that PPLM functioned as an “emotional release,” a “release of everything.” While talking specifically about “mental distress” caused by fatigue and diagnosis, one participant expressed ability to “get a little emotional” and “let out whatever emotions were inside”:
Well, it’s just because it’s a release of your emotions and your feelings and, I mean, exercise is good too, but this (music therapy) I always feel way more relieved by. (P5)
Research question 1B, theme 3: PPLM is a distracting aesthetic pleasure
Codes: feels good, sounds good, distract, enjoy
Participants had difficulty articulating exactly why PPLM was a positive experience but noted that it was aesthetically pleasing in some way. Participants noted, “mentally I thought it made me feel good,” and “it distracted me.” Another participant articulated, “I like it and I like listening to it, it really feels good.”
Research question 2: why do BMT patients request particular songs during PPLM?
After choosing a song from the song menu, participants were prompted to explain or rationalize their song choice. Following the explanation, L.R. played the preferred song. In the following section, we outline themes specific to song choice rationale within PPLM.
Research question 2, theme 1: patients choose songs because of memorable experiences
Codes: life events, symbolism, familiarity, religious assurance
When asked to rationalize their song choices, participants gave both long and short explanations. Some responses were as simple as “I know the words” or “it’s just one of my favorites” without going into further details. Other participants provided specific details about a memory or an event that they associated with the song, such as “I heard this song for the first time when I was down in New Orleans at our church.” In addition, one participant consistently chose religious music, saying, “It gives me assurance of heaven” and “I just like hymns because I used to play the piano in church.” These details were frequently related to specific life events, symbolized a certain time in their life, or were just chosen because of familiarity with the song in general:
Well, when my wife passed away in 2008, I had Leonard Cohen sing that . . . well his recording anyways, at the service and he passed away about a year later while doing a live performance. (P4)
Research question 2, theme 2: patients choose songs for music-based elements and components
Codes: rhythm, writing style, accompaniment, lyric representation, artist, genre
Participants articulated preference to music-based elements and components when choosing songs. These components included artist, genre, accompaniment style, lyric representation, rhythm, and writing style. One participant said, “I like Randy Newman’s writing style, and the rhythm of the song.” Another participant said, “I like this one, I like the music that goes with it.” Another noted, “I’ve just always liked him, I just love every Leonard Cohen song.” While most participants provided relatively brief illustrations of components that they enjoyed, one participant described why the song resonated with him and directly influenced his song choices:
. . . I mean (Bob) Dylan is, you know . . . first of all, there’s that whole Minnesota connection thing, but . . . that song in particular is one that I think is more, a more accessible one of his, you know, it’s not quite as heavy-hitting. I mean I’m sure that there’s all sorts of stuff in his lyrics, but this one seems to be more of a pop song. (P2)
Research question 3: how do song choices within PPLM function?
After L.R. played the preferred song, participants were prompted to describe their reaction to the song and how it made them feel. In the section below, we outline themes specific to function of song choices within PPLM.
Research question 3, theme 1: PPLM facilitates reminiscence
Codes: memories, reminiscence
Similar to participants’ rationales for choosing their preferred music based upon a memory associated with each song, some also expressed that hearing the song provided them with the ability to “bring back memories” and reflect on past experiences. One participant stated, “the memories are soothing” while another noted the music “brings back memories.”
Research question 3, theme 2: PPLM promotes relaxation and restful states
Codes: aesthetic, soothing, fun, relax, calm
All participants described a feeling of relaxation or pleasure after hearing their preferred song. One participant said, “it’s just peaceful, it relaxes me.” Another participant said, “it makes me feel warm and snuggly and it’s just such a soothing song.” Others stated, “I liked it, it just felt good,” or “it makes me feel good.”
Research question 3, theme 3: PPLM encourages reflection through the lyrics
Codes: symbolic, emotional, reflect, introspective
In several instances, participants reflected on the lyrics of their chosen song and applied it to their current situation or to their life across time. After choosing the song “Lean on me,” one participant expressed that it “reminds me that I can lean on people.” Another participant who chose the same song said, “it kind of makes you feel good, like you have somebody to lean on.” Another participant chose “You’ve got a friend in me” and stated, “it’s a tribute to the two people in the song, a casual bond, they trust each other.” Finally, after requesting a hymn, one participant explained how it symbolized the “importance of prayer” and functioned to give her “peace.”
Resultant of mapping, we created Figure 1 to depict the relationships between themes. This figure shows how the rationale and function of songs chosen by patients impact CRF through PPLM.
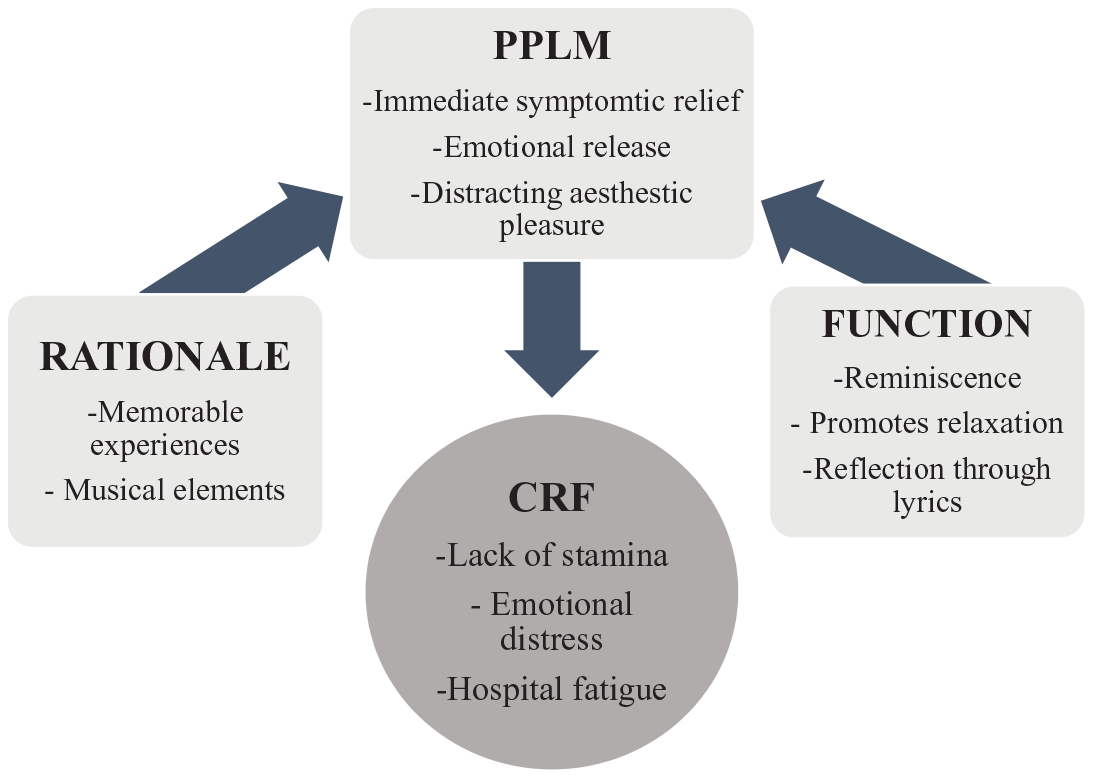
Results of How and Why PPLM Impacts CRF.
Discussion
CRF is an important treatment target as it negatively impacts health and quality of life. As hospitalized adults seem to favor non-physically active music therapy interventions (Silverman et al., 2016), PPLM can function as a preferred and effective intervention to provide symptomatic relief through releasing emotions and distracting patients through an aesthetically pleasing intervention. Results from our study help provide an initial patient-centric understanding of how and why PPLM might impact CRF. Our study is unique as, to date, no researcher has investigated why PPLM might be able to positively impact CRF or song choice rationale and function during PPLM.
Although this study used the interpretivist paradigm, results are congruent with existing objectivist literature supporting the use of PPLM with adult oncology patients (Silverman et al., 2016; Yates & Silverman, 2015). Integrating results of this study with the existing literature, it seems that PPLM is a valued psychosocial treatment that can effectively address various symptoms associated with both cancer treatments and CRF, including emotional distress and sleep. Anecdotally, L.R. observed that participants seemed to value the sense of control that was provided to them throughout PPLM.
One of the challenges inherent in conducting this study was CRF itself. As a negative construct, it was difficult to ask participants to describe and elaborate on their CRF. CRF may have been a contributing factor to participants’ brief responses. As further articulating their CRF within the interview sometimes seemed to exacerbate it, L.R. used her therapeutic intuition and was careful to not excessively probe participants during interviews. These factors may have contributed to a lack of depth in participants’ responses. Moreover, some potential participants were unable to complete the interviews due to CRF. We acknowledge and appreciate the courage, determinism, and altruism of the five participants who shared their experiences while enduring CRF.
Evidence-based practice continues to constitute an important aspect of contemporary health care. Designed to assist and guide practitioners toward making informed, patient-centric, and research-based clinical decisions, evidence-based practice is typically described as the integration of three components: The best research available, the clinician’s expertise, and the patient’s characteristics, culture, values, and preferences (Rubin, 2008; Sackett, Straus, Richardson, Rosenberg, & Haynes, 2000). Results from our study indicate that participants seemed to value and prefer PPLM. Moreover, although randomized controlled trials are important for documenting the effectiveness of psychotherapeutic interventions (i.e., if the intervention was effective or not), it is also crucial to understand mechanisms responsible for change (i.e., why was the intervention effective or not) so that protocols can be designed to include these effective components. Thus, this study fills gaps in the literature that (1) helps to understand mechanisms of change within PPLM, (2) identifies how and why PPLM might be effective for addressing CRF, and (3) develops items for inclusion within PPLM protocols.
Although common fatigue may often be alleviated by sleep, people who experience CRF describe difficulty sleeping (American Cancer Society, 2018b). Researchers have indicated that exercise, psychoeducational, and psychosocial interventions, and cognitive-behavioral therapy can be effective in the treatment of insomnia as a result of CRF specifically (National Comprehensive Cancer Network [NCCN], 2013). Moreover, the NCCN (2013) has specifically regarded psychosocial interventions as a priority in providing the best level of care for effective CRF management. Although not a theme, some participants in this study recognized that PPLM may facilitate sleep. As hospitals are placing increased emphasis on nonpharmacological interventions, music therapists could work collaboratively with patients to create unique playlists to facilitate sleep or even record their PPLM sessions for later use when the music therapist is not available.
As BMT patients are typically hospitalized for longer durations than adults on other medical units, are unable to participate in hospital wide services due to the standard confinement to prevent infection, and experience immense symptom burden, BMT patients should receive frequent nonpharmacological interventions (Yates, Beckmann, Voss, Anderson, & Silverman, 2018). A qualified music therapist may add intrigue to normal hospital routines as patients may consider them non-medical personnel. PPLM may be ideal for creating meaningful relationships and expediently building therapeutic alliance, providing the opportunity to gain deeper access to underlying problems, concerns, and ways to cope with CRF. Congruent with evidence-based practice, we suggest that the appropriate considerations be taken to properly incorporate patients’ values and preferences concerning psychosocial treatments in the medical setting.
Results of the study are limited by the makeup of our research team. As it would be impossible to separate our clinical and educational experiences from our ways of knowing, interpreting, and understanding the data, results are limited by our worldviews. The small sample size, limited geographic area, and inclusive and transdiagnostic approach (Silverman, 2015) also represent limitations. Due to the lack of available resources for this project, L.R. served in a dual role of clinician and researcher. Although L.R. encouraged participants to be candid and honest, responses may have been biased and, therefore, resulted in a lack of negative cases. The implementation of research assistants in future studies may help to eliminate the potential for bias. It is also important to recognize that the authors were qualified music therapists. Therefore, musicians who do not have academic and clinical music therapy training may have different results and could potentially induce additional CRF by over-exerting patients. Finally, the use of a song menu limits PPLM. We acknowledge music therapists will not be able to play every song that is requested in PPLM. However, as we value musicality and feel this is a critical component of PPLM, we decided to use menus based on the importance of being able to play songs on the menu at a high level (Haack & Silverman, 2016; Selle & Silverman, 2019a, 2019b). It should be highlighted that if a patient requests a song that was not on the PPLM menu, the music therapist can offer options similar to the requested genre or artist and obtain comparable benefits (Walworth, 2003). The music therapist can then learn the requested song and bring it back to the patient at a later time if their length of hospitalization permits.
Future research is warranted to explore BMT patients’ experiences of PPLM and other music therapy interventions on symptoms, psychosocial well-being, medication used, and length of hospitalization. Investigators could measure the benefits of PPLM in facilitating symptom management and sleep within cancer care. As it was common for adult oncology patients experiencing CRF to have difficulty carrying on a conversation or completing an interview, it is important to consider assessments or interviews that are less fatiguing. Investigators need to be sensitive and compassionate to avoid exacerbating CRF. As CRF constitutes a complex construct, researchers should implement multidimensional fatigue assessments to gain access to deeper information and pinpoint the different components of CRF so interventions can be specifically designed to target these aspects.
The primary purpose of this interpretivist study was to understand the mechanisms by which PPLM targets and impacts CRF from the patients’ perspectives. The secondary purpose was to gain insight into patients’ song choice rationales and their ensuing function within PPLM. This study adds patients’ voices to the existing PPLM and BMT literature base and indicates that adults with cancer on a BMT unit value PPLM as it can work to lessen the impact of CRF. Emphasizing the importance of patient preferences and decision-making within a music therapy session, it seems that PPLM is favored by adult oncology patients and it may provide symptomatic relief, lessen emotional distress, and provide aesthetic pleasure.
Footnotes
Appendix
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Graduate Summer Research Fellowship from the School of Music and College of Liberal Arts at the University of Minnesota.