
Abstract
Cancer-related fatigue (CRF) is the most persistent and commonly occurring side effect of cancer and its treatments. CRF can negatively impact recovery and there is a lack of music intervention research addressing CRF. The purpose of this randomized study was to determine the effects of a single patient-preferred live music (PPLM) session on fatigue, energy, and pain in adults on a medical oncology/hematology unit. Participants (N = 36) were randomly assigned to experimental or wait-list control conditions and completed measures at pre- and posttest. Experimental participants received an individual PPLM session. Participants were provided with a 35-song menu consisting of music from a variety of genres. The results indicated significant between-group differences in posttest fatigue (p = .004) and pain (p = .027) with experimental participants having more favorable means. Although the between-group difference in posttest energy was not significant, the experimental group had a greater increase in energy from pre- to posttest than the control group. As CRF is common and the existing literature indicates that adults in medical settings tend to prefer receptive interventions, PPLM may represent a practical and effective intervention to address fatigue and pain for adults on a medical oncology/hematology unit. Limitations, implications for clinical practice, and suggestions for further research are provided.
Review of literature
Approximately 38.4% of men and women will be diagnosed with cancer during their lifetime in the United States (American Cancer Society, 2019). Moreover, an estimated 1,762,450 new cases of cancer will be diagnosed in 2019, while 606,880 of those people will die from the disease (American Cancer Society, 2019). Although technological and pharmacological innovations have improved treatments and prognoses, these statistics highlight cancer as a major societal problem.
Oncology patients have consistently indicated fatigue as the most persistent and commonly occurring side effect of cancer and its treatments (Jacobsen et al., 1999; Stasi, Abriani, Beccaglia, Terzoli, & Amadori, 2003; Visovsky & Schneider, 2003). Cancer-related fatigue (CRF) is not relieved by sleep and can be overwhelming as it causes more distress than everyday fatigue (American Cancer Society, 2019). CRF can negatively impact people’s mood, physical ability, work performance, social interaction, family care, cognitive performance, schoolwork, community activity, and sense of self (Curt et al., 2000; Wu & McSweeney, 2007). Moreover, the negative effects of CRF last longer than nausea, depression, and pain (Stasi et al., 2003). Ultimately, CRF can have negative lasting effects on physical, cognitive, emotional, and spiritual wellbeing (Berger et al., 2015) and interventions addressing CRF are warranted.
CRF constitutes a complex phenomenon necessitating a theoretical understanding to design and test effective treatments. Wang (2008) examined the potential causes of CRF by discussing three different domains that lead to the pathophysiology of CRF: the direct effects of tumor burden, treatment-related effects, and comorbidities. Treatment-related effects of CRF can be caused by chemotherapy, radiotherapy, different types of surgeries, and medications (Wang, 2008). Comorbid conditions related to CRF include tumors, different pathophysiological conditions such as malnutrition, infection, hepatic, pulmonary or cardiac failure, renal insufficiency, thyroid dysfunction, as well as psychosocial factors that can include anxiety, depression, stress, environmental factors, and inadequate coping strategies with a chronic illness. Wang highlighted how these factors all have the potential to contribute to CRF because of the physical and psychosocial impact they can have on a person with cancer.
In a systematic review, Bradt, Dileo, Magill, and Teague (2016) found that music interventions can be effective in oncology treatment. However, the researchers identified a lack of research regarding music interventions that specifically addressed CRF. Despite a lack of CRF-specific research, music therapy can be beneficial for people with cancer. More specifically, patient-preferred live music 1 (PPLM) is a music therapy intervention that may be especially relevant for CRF as it does not require physical activity. PPLM involves music selected and preferred by the patient that is performed live by a qualified music therapist. In a systematic review, Silverman, Letwin, and Nuehring (2016) found that PPLM can be an effective and preferred intervention that may positively impact pain, nausea, physiological variables, and affective states among adult oncology and transplant patients.
Ramaswami and Silverman (2019) parsed PPLM into four separate parts including music, familiarity/preference, live performance, and choice/autonomy and provided a neurological rationale for why it might be effective. Because the music in PPLM is performed live within a social interaction with the patient, the therapist is able to adapt to the momentary needs, behaviors, and requests of the patient, thus making it a flexible and malleable music therapy technique (Silverman et al., 2016). The live aspect of PPLM also allows patients to make a number of decisions, including song choice, style, and tempo. This element of choice may promote greater autonomy and control among hospitalized patients, who generally have little opportunity to exert mastery over their environment (Silverman et al., 2016). Congruently, social psychology researchers have indicated that increased autonomy and control is associated with greater psychological health (Benassi, Sweeney, & Dufour, 1988; Ryon & Gleason, 2014). In addition, PPLM can be an accessible music therapy intervention for patients who feel too unwell or fatigued to actively participate in songwriting or clinical improvisation and who may be intimidated by the idea of performing musically (Selle & Silverman, 2020; Silverman et al., 2016). Other researchers have found that adults in inpatient medical settings tend to prefer receptive rather than active music therapy interventions (Burns, Sledge, Fuller, Daggy, & Monahan, 2005; Chaput-McGovern & Silverman, 2012; Crawford, Hogan, & Silverman, 2013).
CRF constitutes a complex phenomenon (Wang, 2008) and represents the most commonly occurring side effect of cancer and its treatments (Jacobsen et al., 1999; Stasi et al., 2003; Visovsky & Schneider, 2003). PPLM can be an effective and accessible intervention for people undergoing cancer treatment. However, there is a consequential gap in the music intervention literature base addressing CRF (Bradt et al., 2016). Therefore, the purpose of this randomized pilot study was to determine the effects of a single PPLM session on fatigue, energy, and pain with adults on a medical oncology/hematology unit. The guiding research question was as follows: Are there between-group differences in fatigue, energy, and pain resultant of a single PPLM session in adults on a medical oncology/hematology unit?
Method
Participants
Research participants (N = 36) were adults on the medical oncology/hematology inpatient unit of a large urban teaching hospital in the Midwestern region of the United States. The only inclusion criteria in this purposely inclusive pilot study were that participants (a) were adult inpatients on a medical oncology/hematology unit, (b) were 18 years or older to provide consent for themselves, and (c) could read and write in English. Prior to data collection, the researchers received approval for the study from the hospital and university shared Institutional Review Board (STUDY00002953) and completed all necessary research training.
Measures
Fatigue was measured using the Lee Fatigue Visual Analogue Scale (VAS-F; Lee, Hicks, & Nino-Murcia, 1990). The VAS-F is an 18-item visual analog scale used to measure the severity of fatigue and energy levels in both healthy and patient populations. This psychometric instrument consists of 13 items in the fatigue subscale and five items in the energy subscale. Each item has a 100-mm visual analog line with bipolar descriptors at each end. Participants mark the line to indicate how they currently feel. The score for each item is the distance in millimeters between the left end of the line and the respondent’s mark. The fatigue score is calculated as the mean of the 13 fatigue items and the energy score is the mean of the 5 energy items. Higher scores on the fatigue scale represent greater fatigue severity, while higher scores on the energy scale indicate higher levels of energy. Fatigue and energy scores are separate and there is no total score for the VAS-F. Lee and colleagues (1990) originally tested the scale for validity and reliability on 75 healthy adults with no complaints of chronic fatigue and 57 patients at a sleep disorders clinic with fatigue. Internal consistency reliability for the 13-item fatigue subscale was 0.96 for the healthy group and 0.95 for the patient group. Internal consistency reliability for the 5-item energy subscale was 0.95 for the healthy group and 0.94 for the patient group.
Participants rated their pain on an 11-point Likert-type scale, with 0 indicating no pain and 10 indicating the highest level of pain. Numerical rating scales such as the one employed in this study are commonly used in medical facilities to expediently measure pain among medical patients (Wells, Pasero, & McCaffery, 2008). Participants were asked to self-report their fatigue, energy, and pain scores in the moment.
Design and procedure
This study used a two-group randomized pre- and posttest wait-list single-session design. Randomization was determined via a computer program (www.randomizer.org). Participants in the experimental group completed pretests, received 20–30 min of PPLM, and then completed posttests. Participants in the control group completed pretests, waited 20–30 min, completed posttests, and then had the option to receive PPLM. Due to the inclusive nature of the pilot study, the authors were not able to have a consistent wait-listed control condition between the pre- and posttests. As such, control participants were able to do various sedentary activities in their rooms between the pre- and posttests, including watching television or interacting with visitors. Although family members were sometimes present, all sessions were individual due to inpatient oncology setting.
The principal investigator (PI) approached each patient and asked if they wanted to receive a session of PPLM. If the patient responded in the affirmative, the PI then asked if they wanted to voluntarily participate in a research study. For patients who selected study participation, the PI obtained informed consent and followed procedures according to the predetermined randomization protocol. Participation in the study was voluntary. To provide music therapy to as many people on the unit as possible, all patients had the option to receive PPLM regardless of study participation. Patients who remained on the unit for extended time periods were able to receive multiple sessions of music therapy, but were only eligible for study participation during their first PPLM session with the PI.
To control the independent variable and facilitate decision making and autonomy, the PI provided each participant with a song menu (see Appendix 1) consisting of 35 songs from a variety of genres. Although this limited the participant’s music selection, the use of a song menu was consistent with Walworth (2003), who found that playing a song by a person’s preferred artist or within the preferred genre can be as effective in reducing anxiety as using a specific song. Based from the existing literature noting that autonomy, control, and choice can lead to greater psychological health (Benassi et al., 1988; Ryon & Gleason, 2014), the menu also served as a prompt for participants to select music rather than requesting that the PI play whatever she preferred. 2 The use of a song menu also ensured that the PI could prepare the music in advance and therefore play it in an aesthetically pleasing and highly competent manner. The PI encouraged participants to select songs they wanted to hear and to choose how they would like the song to be played in regard to tempo and dynamics. The PI also provided participants with autonomy for the duration of the session and the number of songs selected. Sessions typically consisted of four or five songs but ranged from one to eight songs. Regardless of the condition, the PI sang all songs and accompanied herself on a steel string acoustic guitar.
Theoretical framework
Elwyn and colleagues (2012) translated existing conceptual descriptions of shared decision making into a practical three-step model: (a) introducing choice, (b) describing options by integrating the use of patient decision support, and (c) helping patients explore preferences and make decisions. The model supports the process of deliberation, patient values, and informed preferences throughout the three steps. This framework is congruent with PPLM as patients are given autonomy and agency: Patients choose music that is valuable to them, the music is performed live within a social interaction with the patient, and the therapist is able to adapt to the momentary needs, behaviors, and requests of the patient. The live aspect of PPLM also allows patients to make a number of decisions, including song choice, style, and tempo. The choices inherent within PPLM may promote greater control among hospitalized patients who typically have little autonomy. As such, PPLM constitutes a flexible and malleable music therapy intervention (Silverman et al., 2016) congruent with shared decision making. Through supporting participants’ choices, options, and decisions within the PPLM process, the authors hypothesized that the experimental group would have more favorable fatigue, energy, and pain outcomes than the control group.
Power analysis and data collection period
Fifty-four participants would have been required to achieve a medium effect size (.25) when α = .05 for a power of .95 using an analysis of variance (ANOVA) with two independent treatment groups. Data were collected between September 2018 and March 2019. Because the PI was a student, data collection was discontinued at the conclusion of the academic year. As a result, the sample size in this pilot study was 36 participants.
Statistical analyses
Chi-square tests were conducted to determine whether there were between-group differences in gender and race. In addition, t-tests were used to determine whether there were between-group differences in age, length of hospitalization, and pretest scores for fatigue, energy, and pain. To determine whether there were significant between-group differences in posttest fatigue, energy, and pain scores, the researchers conducted analysis of covariance (ANCOVA), with pretest scores as covariates, posttest scores as the dependent measures, and treatment group as the fixed factor in SPSS version 25. Effect sizes were interpreted according to Kotrlik, Williams, and Jabor (2011): small ⩽ .08; medium .09–.24; large ⩾ .25.
Results
The flow of participants throughout the study is depicted in Figure 1.
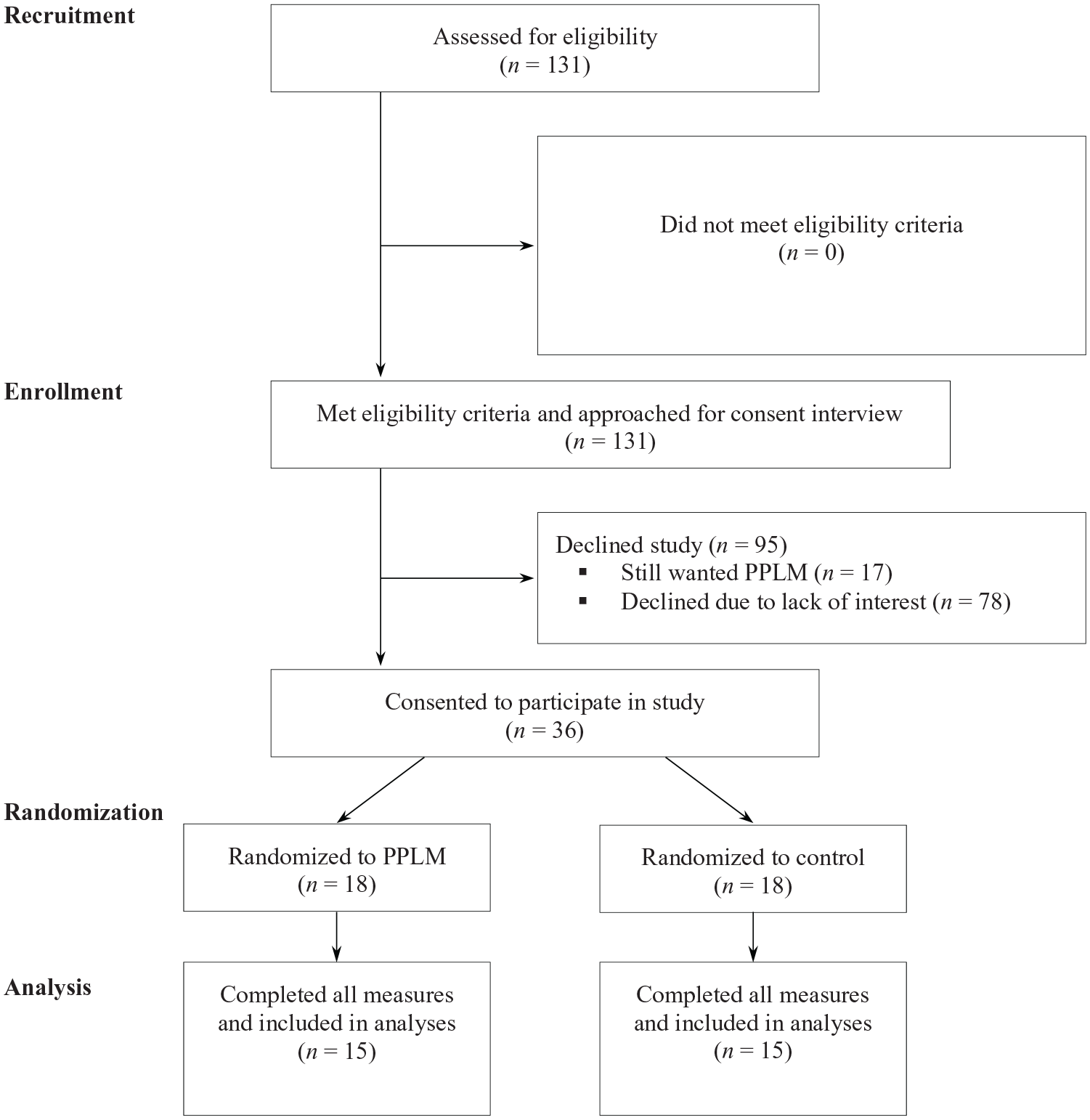
Participant Flow Through Study.
There was no significant between-group difference in gender, race, age, or length of hospitalization (all p > .05). Participant demographic information is depicted in Tables 1 and 2. There was no significant between-group difference in pretest measures of fatigue, energy, or pain (all p > .05). Correlational analyses of pre- and posttest data indicated significant relationships for fatigue, energy, and pain (all p < .05).
Demographic frequency data by condition.
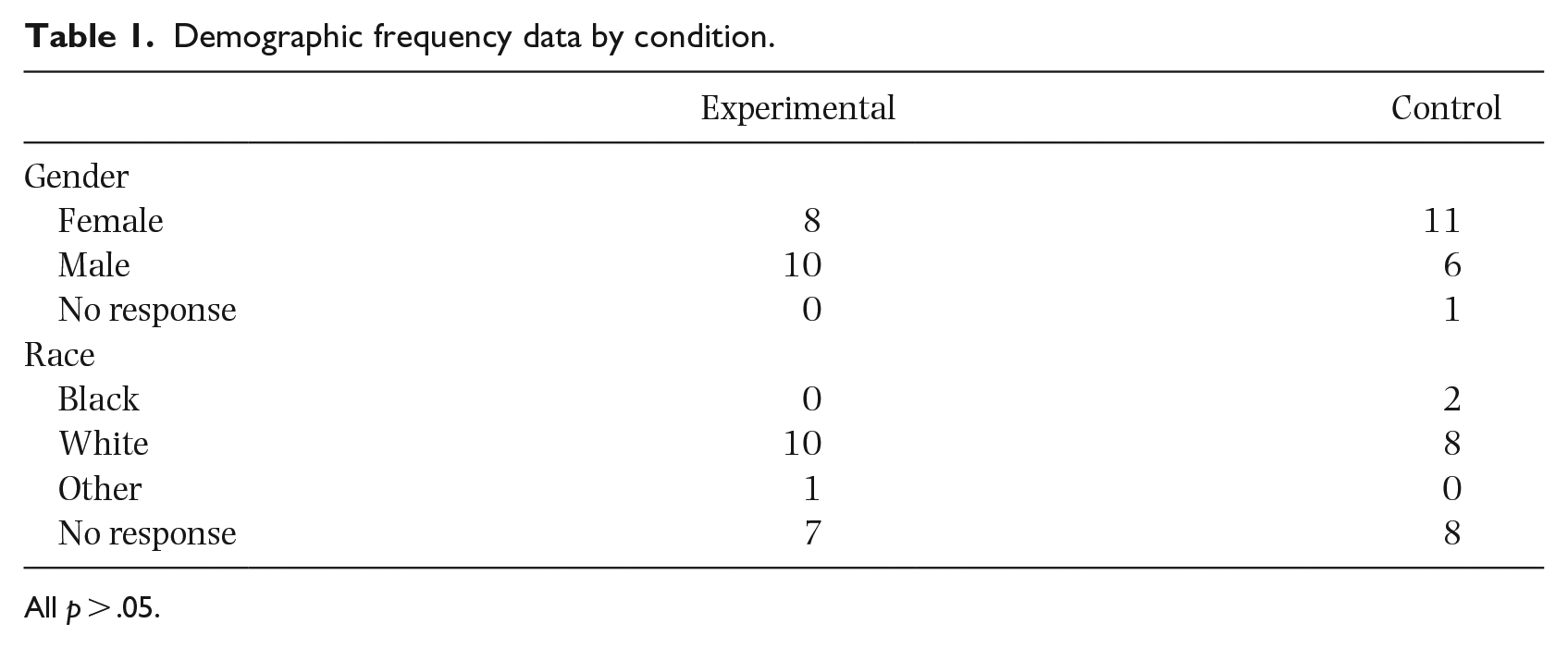
All p > .05.
Descriptive statistics of participants’ ages and length of hospitalization.
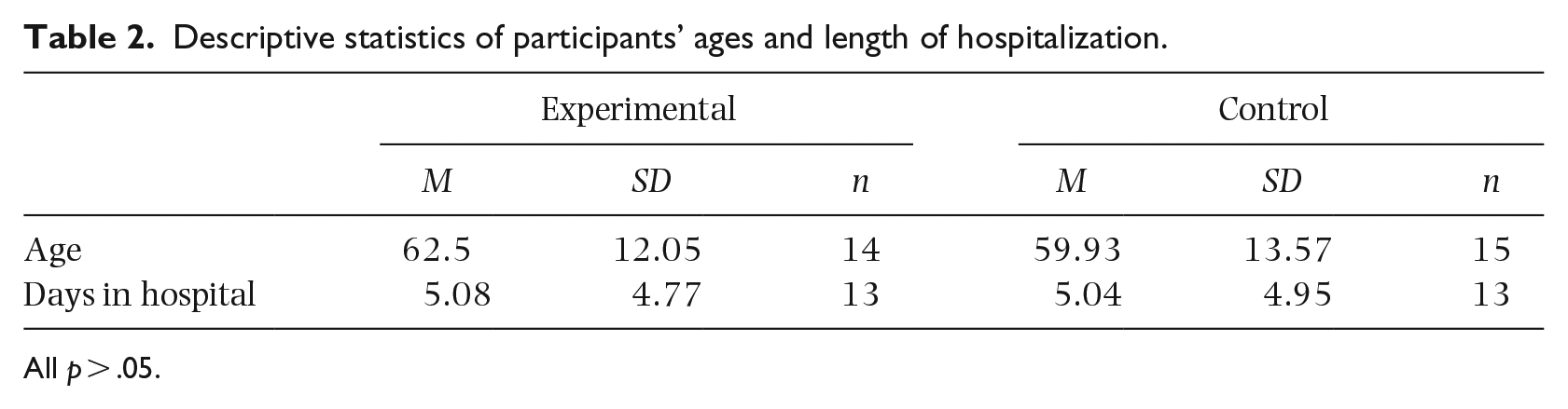
All p > .05.
The results from the posttest ANCOVAs with pretest scores as a covariate indicated that there were significant between-group differences in posttest measures of fatigue (p = .004) and pain (p = .027). Participants in the experimental group had more favorable mean posttest scores for fatigue and pain when compared with participants in the control group. Effect sizes for fatigue and energy were in the medium range. Although there was no significant between-group difference for energy (p = .151), the mean score for the experimental group at posttest tended to be slightly higher than that of the control group. It should be noted that some participants did not complete all measures. Descriptive statistics for pre- and posttest fatigue, energy, and pain are depicted in Table 3. Table 4 depicts the ANCOVA results.
Fatigue, energy, and pain descriptive statistics.

ANCOVA results.

Discussion
CRF represents a major social problem for adults with cancer and there is a lack of music intervention research addressing CRF (Bradt et al., 2016). Therefore, the purpose of this randomized pilot study was to determine the effects of a single music therapy session in the form of PPLM on fatigue, energy, and pain with adults on a medical oncology/hematology unit. The results indicated significant between-group differences in posttest fatigue and pain, with the experimental group having more favorable scores. Although the between-group energy difference was not significant, the experimental group tended to have higher mean energy than control participants at posttest. Strengths of the current study include the use of a randomized controlled design, a menu to control the independent variable, and an established psychometric instrument to measure fatigue and energy. As a less physically active intervention for adults with CRF, it would seem that PPLM may be effective as a gateway intervention to future music therapy sessions (Silverman et al., 2016) addressing psychosocial factors such as coping (Hogan & Silverman, 2015), hope (Verstegen & Silverman, 2017), mood (Bergh & Silverman, 2018), and resilience (Letwin & Silverman, 2017).
Consistent with previous music therapy research on adult medical populations (Lee, 2016) and with efforts by hospitals to manage pain without pharmacological interventions (Wells et al., 2008), the researchers included pain as an outcome measure in the current study. There was a significant between-group difference in posttest measures of pain, favoring the experimental group. In addition, experimental participants’ mean pain scores decreased from pre- to posttest, whereas control participants’ scores increased from pre- to posttest. These results are congruent with those from Lee’s (2016) meta-analysis, indicating that music interventions had statistically significant effects in decreasing pain among medical patients. These findings have implications for addressing pain among hospitalized patients without using pharmacological interventions. Given the severity of the opioid epidemic, these results warrant further inquiry.
There were numerous limitations of the current study. The first of these limitations is the small sample size. The PI approached 131 potential participants and 95 of them declined study participation. People declined study participation for many reasons, including experiencing pain and fatigue, having prior family or physician engagements, or being discharged from the hospital. The high percentage of people who declined participation is consistent with existing research with medically hospitalized adults (Fredenburg & Silverman, 2014; Selle & Silverman, 2017). In addition, as noted in the “Results” section, some participants did not complete all measures. While this constitutes a limitation, the authors were careful not to pressure participants or have participants overexert themselves. Moreover, not finishing all measures may have been a result of CRF itself and the authors are grateful to the participants for whatever self-report measures they were able to complete despite their symptoms. Another limitation of this inclusive pilot study was the inability to control what happened during the time between the pre- and posttests within the control condition. Other limitations include the lack of follow-up measures to determine potential maintenance of treatment gains and the dual role of the PI who acted as both a clinician and a researcher. Consistent with the Hawthorne Effect, the dual role of the clinician-researcher could have resulted in participants reporting more favorable scores at posttest. Moreover, the results are limited by the transdiagnostic approach to this purposely inclusive pilot study, wherein all patients on the unit had the option to participate in the research and receive PPLM regardless of the specific type of cancer (participants had a variety of different types of cancer, including but not limited to lymphoma, throat cancer, hemophilia, and leukemia). 3 In addition, the researchers and participants were not masked to treatment allocation due to PPLM, the consent process, and the wait-listed design. Finally, the results may not generalize to other healthcare practitioners using music due to the unique academic and clinical training qualified music therapists receive. The researchers urge caution in generalizing the results of this study due to these limitations.
Future investigators could increase the music therapy dosage and then track more traditional data, including length of stay, re-hospitalizations, and quality of life. In addition, as the current researchers used self-report measures, future researchers might study bio-physiological measures, including cortisol. When the body experiences high levels of stress, cortisol can alter or shut down certain functions in the body, including the digestive system, reproductive system, or immune system. This can lead to further health problems including difficulty sleeping or fatigue. As such, collecting cortisol levels might provide a biological measure in future PPLM research. Researchers could also consider using music therapy in a more educational manner to address healthy lifestyles post-cancer treatment. Investigators might also study ways to enhance accepting music therapy and participating in research studies. For example, researchers could study different ways in which music therapists present treatment and the opportunity to participate in research to hospitalized adults. Future researchers could include follow-up measures to track maintenance of treatment gains and the use of research assistants to collect pre- and posttest data to avoid the effects of the dual clinician-researcher role. In addition, researchers could investigate the influences of who selects the music by comparing researcher-selected music with participant selected music. Interpretivist and mixed-methods paradigms could also be implemented to better understand participants’ experiences and potential PPLM change mechanisms. However, future investigations of CRF will require sensitive and nuanced approaches to collect meaningful data while not exacerbating symptoms. Future research on music interventions for CRF and pain are warranted, especially as hospital guidelines continue to incorporate nonpharmacological options for pain management (Wells et al., 2008).
The purpose of this randomized pilot study was to determine the effects of a single music therapy session in the form of PPLM on fatigue, energy, and pain with patients on a medical oncology/hematology unit. With results indicating significant between-group differences in posttest fatigue and pain measures, it seems that PPLM can be effective in addressing both CRF and pain among adults on a medical oncology/hematology unit. Due to the relatively small sample size and other noted limitations, the authors urge caution in generalizing the results of this study. Future research regarding the use of music therapy for CRF and pain is warranted to replicate findings and to further contribute to the development of evidence-based practices.
Footnotes
Appendix 1
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the University of Minnesota Undergraduate Research Opportunities Program.