
Abstract
This study investigates the convergent and predictive validity of behavioral crime scene indicators of sexual sadism in the context of rape and sexual homicide. The study is based on a sample of 268 adult males sentenced to a federal penitentiary in Canada. Information regarding crime scene behaviors was gathered from police records, a clinical interview with a psychologist, and a semistructured interview with the offender. A series of logistic regressions were performed to determine whether behavioral crime scene indicators of sexual sadism were associated with an official diagnosis of sexual sadism and were able to distinguish between sexual aggressors against women and sexual murderers. Findings suggest that several crime scene behaviors overlap with an official diagnosis of sexual sadism as well as being able to distinguish between sexual aggressors of women and sexual murderers. Importantly, the majority of crime scene behaviors associated with a clinical diagnosis of sexual sadism are not the same as those associated with sexual homicide.
Introduction
Over the years, there have been several attempts to describe the individual characteristics and behaviors of the sexually sadistic offender. In fact, Proulx and Beauregard (2009) correctly pointed out that sadistic sex offenders have received numerous labels, such as the “assaultive” offender (Gebhard, Gagnon, Pomeroy, & Christenson, 1965) and the offender characterized by a “fusion of aggression and sex” (Cohen, Garofalo, Boucher, & Seghorn, 1971). Similarly, the empirical literature on sexual homicide has identified a subgroup of sexual sadists, referred to as the “organized” sexual murderer (Ressler, Burgess, & Douglas, 1988), the “compulsive” sexual murderer (Revitch & Schlesinger, 1981), the murderer “motivated to carry out fantasies” (Beech, Fisher, & Ward, 2005) and the “sexually motivated” murderer (Brittain, 1970). Several things stand out from these numerous labels. First, when describing this group of offenders, researchers seem to highlight the fact that the offence is sexually motivated. In other words, the act of sexual assault, whether it escalates to a sexual homicide or not, is driven by the need for sexual gratification through the infliction of pain. Also, sexual sadism often co-occurs with sexual homicide and is thought to underlie the phenomenon. This suggests that, among all types of rapists identified by researchers (e.g., Cohen et al., 1971; Groth & Birnbaum, 1979; Knight & Prentky, 1990), sexual sadists might be one of the groups most likely to escalate their violence to a homicide. Furthermore, the criminal behavior of sexual sadists is often described as highly planned and structured, compulsive and ritualized, as well as violent. Finally, the numerous labels used by the scientific community might be indicative of a lack of consensus about what sexual sadism is and how it is defined. In other words, researchers are not satisfied by the generally agreed on clinical definition of sexual sadism and its measurement in the Diagnostic and Statistical Manual of Mental Disorders (DSM; Hucker, 1997; Yates, Hucker, & Kingston, 2008). The various labels used to describe conceptually related phenomenon and the dissatisfaction with the clinical definition and criteria of sexual sadism are reflective of conceptual and methodological issues with the measurement of sexual sadism. More precisely, there are no valid and reliable measures of sexual sadism to assist researchers, clinicians, or police investigators. The current study is a step in that direction. The first goal is to investigate the convergent validity of a series of crime scene indicators of sexual sadism with that of a clinical diagnosis of sexual sadism using the DSM. Crime scene indicators are the focus here given that they represent more objective behavioral indicators of the offender’s underlying motivation to force someone into sex. In doing so, the current study aims to determine whether offenders having been diagnosed as sexual sadists exhibit particular crime scene behaviors. Furthermore, the current study goes a step further by revisiting the sexual homicide–sexual sadism link by examining whether sexual aggressors who kill their victim have distinct crime scene behaviors that are more reflective of sexual sadism. In doing so, the study compares and contrasts the crime scene behaviors associated with a clinical diagnosis of sexual sadism and those associated with sexual homicide. Put together, the study aims to determine whether the crime scene behaviors associated with sexual sadism are the same for rapists and sexual murderers. First, we review the scientific literature on the measurement of sexual sadism and the conceptual and methodological issues.
Conceptual and Definitional Issues With Sexual Sadism
Defining sexual sadism has been one of the more challenging obstacles in understanding sexual sadism. There appears to be a general consensus that sexual sadists are sexually aroused by either (a) some form of violent or humiliating behavior (e.g., Abel, 1989; Groth & Birnbaum, 1979; Knight & Prentky, 1990; Knight, Prentky, & Cerce, 1994), (b) the victim’s reaction to this behavior (e.g., being frightened, scared, or being in pain; Marshall & Kennedy, 2003), or (c) the resulting feeling of power and control as a result of the violence inflicted (Brittain, 1970; Dietz, Hazelwood, & Warren, 1990; Grubin, 1994; Levin & Fox, 1985; MacCulloch, Snowden, Wood, & Mills, 1983). Some researchers have argued that the sexual sadist can be characterized by a deviant sexual preference for violence. This sexual preference is thought to be the product of a “synergy” or “fusion” of sexual and aggressive drives (Abel, 1989; Groth & Birnbaum, 1979; Knight et al., 1994; Knight & Prentky, 1990). Others, like Gratzer and Bradford (1995), suggested that violence is not a sufficient condition to elicit a sexual arousal, but the “control of another person through domination, degradation, or infliction of pain for the purpose of sexual pleasure” (p. 450; see also, Proulx, Aubut, McKibben, & Cote, 1994). According to this perspective, it is not so much the violence, but the humiliation, degradation, subjugation, and suffering producing fear, terror, pain, and panic in the victim, that makes the sadist feel powerful and sexually aroused. Rada (1978) further claimed that the humiliating acts performed by the sexual sadist provide more sexual satisfaction than the actual act of sexual intercourse. It is unclear whether the humiliating acts of the offender are a specific manifestation of control and power, which is sexually arousing to the sadist, or as a sexual preference for humiliation per se. Despite these conceptual differences, there are two main methods of identifying sexually sadistic individuals. Although the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) is the most widely used, researchers have also used phallometric assessments to identify individuals sexually aroused by acts of sadism. The proceeding sections highlight the benefits and drawbacks of the DSM and phallometric assessment in identifying sexually sadistic individuals.
DSM
Few valid and reliable clinical methods have been proposed to measure sexual sadism in sex offenders (e.g., Hollin, 1997; Kingston & Yates, 2008). The DSM has been the most widely used clinical tool to assess for the presence of sexual sadism. But the description and diagnostic criteria of sexual sadism have changed over the years (APA, 1952, 1968, 1980, 1987, 1994). In its current form, the DSM-IV-TR (APA, 2000) states that in order for an individual to receive a diagnosis of sexual sadism, there must be “recurrent, intense sexually arousing fantasies, sexual urges, or behaviors involving acts (real not simulated) in which the psychological or physical suffering (including humiliation) of the victim is sexually exciting to the person” which are present for at least 6 months (p. 573). The diagnostic criteria also require the presence of significant distress or (social, occupational, etc.) impairment as a result of these urges and/or behaviors. The presence of deviant sexual fantasies is often used to identify the sexual sadist and is considered to be a common feature of sexual sadism (Brittain, 1970; Dietz et al., 1990; Knight & Prentky, 1990; MacCulloch et al., 1983; Marshall & Kennedy, 2003; Ressler et al., 1988). The fantasies of sexual sadists are thought to reflect the same themes of violence, dominance, and humiliation that characterize their crime scene behaviors when they act on them (e.g., Hazelwood, Dietz, & Warren, 1992). Researchers have claimed that not only are deviant sexual fantasies thought to be present in virtually all sexual sadists but also there is assumed to be a strong compulsion to act on them (Holmes & Holmes, 1996).
Several issues have been raised regarding the use of the DSM as a diagnostic tool to assess for the presence of sexual sadism. Some have argued that the reliance on an offender to admit to his deviant sexual fantasies is one of the major pitfalls of being able to properly identify sexually sadistic offenders (Marshall & Kennedy, 2003) because offenders are reluctant to admit to sexually sadistic fantasies (Marshall, Anderson, & Fernandez, 1999). Furthermore, recent empirical evidence conducted by Marshall and colleagues suggests that despite clear diagnostic criteria, clinicians cannot agree on the core features of sexual sadism (Marshall, Kennedy, & Yates, 2002; Marshall, Kennedy, Yates, & Serran, 2002). These studies indicated that exercising of control, power, domination, humiliation/degradation, and cruelty were the only features most clinicians appear to agree as relevant to identifying sadists, whereas indicators such as excessive violence (such as beating a victim), strangulation, abduction, confinement, and anal sex were not consistently identified as important indicators. In addition, indicators such as suffocation, postmortem wounding, and anal or vaginal penetration with object were not consistently associated with a diagnosis of sexual sadism. Criticism over the DSM definitions, descriptions, and diagnostic criteria has lead clinical researchers to develop alternative measures of sexual sadism. 1
Phallometric studies on sexual sadism
Some researchers have relied on what is considered a more objective method of measuring sexual interests through the use of phallometric assessments. Phallometric assessment measures sexual arousal to violence by exposing the participant to various audiotaped descriptions of violence (sexual and nonsexual) and measuring the level of sexual arousal through changes in the volume/circumference of the penis (Barbaree, Seto, Serin, Amos, & Preston, 1994; Fedora et al., 1992; Proulx et al., 1994; Quinsey, Chaplin, & Varney, 1981; Seto & Kuban, 1996). Phallometric studies have not been able to consistently identify sexually sadistic rapists and nonsexually sadistic rapists based on their sexual arousal to nonsexual violence. The inconsistent findings are unclear and could be due to a multitude of factors. One possible explanation is that not all phallometric protocols, including the stimuli used to assess sexual arousal to violence, are equally valid. An alternative explanation is that the inconsistent finding could be a result of the fact that these empirical studies have typically identified sexual sadists using the diagnostic criterion of the DSM, to which phallometric data were compared. The lack of significant differences found in earlier studies might reflect not so much the lack of validity of phallometric assessment in assessing sexual sadism but the poor validity of the DSM diagnostic for reasons mentioned above. Proulx et al. (1994), however, have shown that it was not so much the violence that best discriminates between rapists and nonrapists but the presence of humiliation in scenarios depicting a rape scene. This might further reinforce the idea that humiliation might be one of the key behavioral indicators of sexual sadism. However, Proulx et al. (1994) did not examine the association between sexual arousal to their scenarios of rape with humiliation and a clinical diagnosis of sexual sadism, thus limiting the conclusion that can be drawn from this study.
Sexual sadism and crime scene behaviors
More recent studies have relied on inventories focusing almost exclusively on the crime scene behaviors of convicted sex offenders to measure sexual sadism. In the left column in Table 1, the seven criteria identified by Proulx, Blais, and Beauregard (2006) are presented. The criteria are regrouped into two categories (i.e., Scale A and Scale B) to measure sexual sadism in a sample of sexual murderers and sexual aggressors of women. Offenders who showed at least one of the first categories of behaviors or two in the second were classified as sadists. Proulx et al. (2006) used mainly crime scene variables that could be coded using official data (i.e., police report). In fact, three of the four items included in Scale A and all items included in Scale B were based on official, crime scene data. The only indicators not based on crime scene data reflected the presence of sadistic fantasies and were based on data collected through a semistructured interview. This indicator, therefore, suffered from the same limitations as the one found in the DSM due to its exclusive reliance on self-report data. Using those criteria, 45% of the homicide offenders were classified as sadists, as opposed to 25% of rapists. The reliability of the scale of sadism was not assessed. Furthermore, their measure of sadism was not cross-tabulated with those with a clinical diagnosis of sexual sadism although group comparisons were conducted with available phallometric data. The study findings highlighted that, although sadists and nonsadists did not differ in their arousal to nonsexual violence, sadists showed increased arousal to rape with humiliation and rape with physical violence. The results, therefore, showed some convergent validity between the Proulx et al. (2006) measure of sexual sadism and phallometric data.
Scales of Sexual Sadism Indicators and Related Indicators.
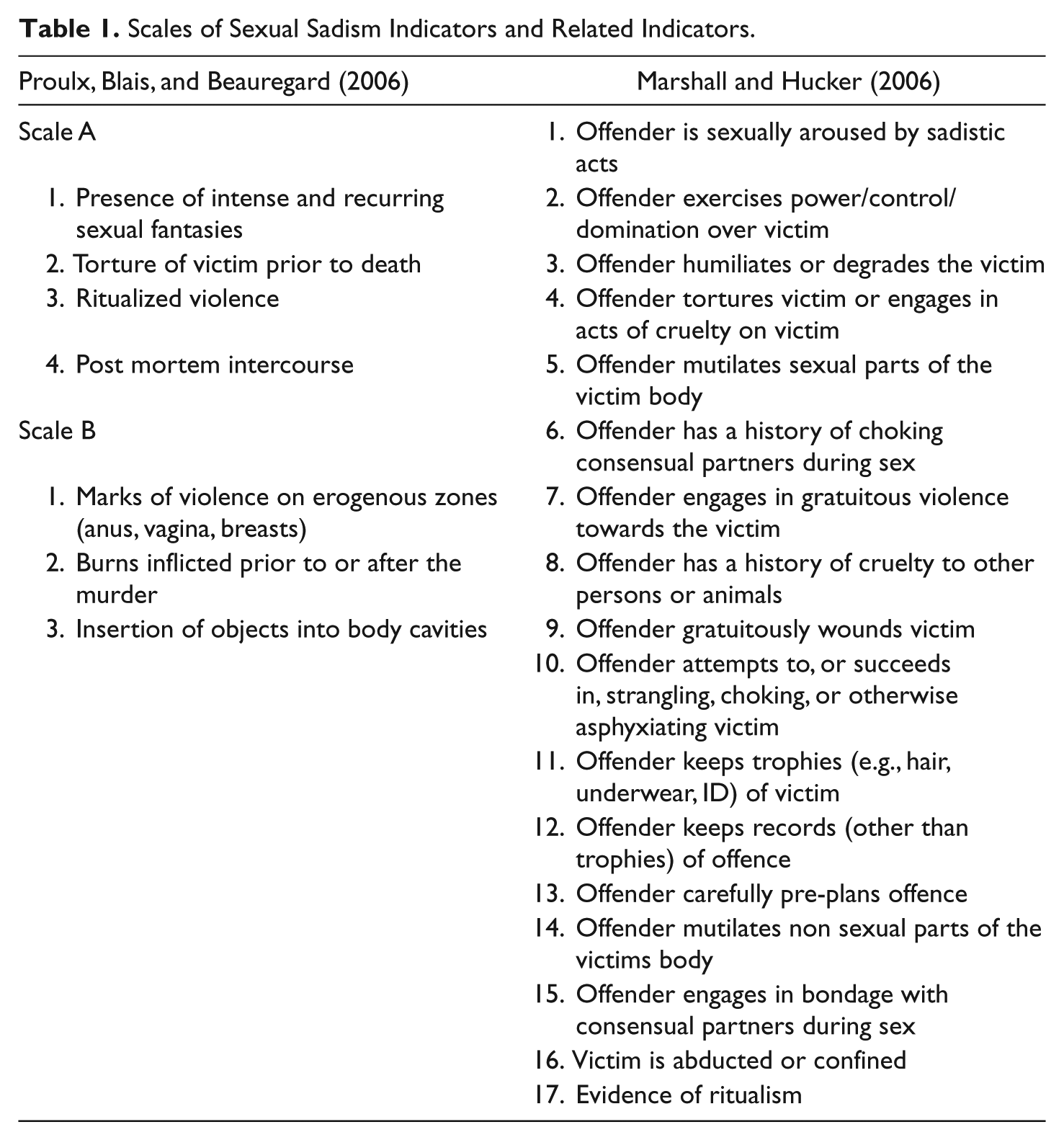
Marshall and Hucker (2006) also proposed a list of indicators to measure sexual sadism. These indicators are presented in the right column of Table 1. Their list was composed of 17 items tapping various behavioral aspects. The authors argued that these 17 items were tapping an underlying trait (sexual sadism) that can be measured along a continuum with a higher score (higher number of indicators) suggesting the presence of sexual sadism. In line with Proulx et al. (2006), their list included an item reflecting the offender’s sexual arousal to sadistic acts, thus relying on self-report data and being subject to the offender’s biases in revealing his sexual fantasies. Furthermore, Marshall and Hucker (2006) included lifestyle (i.e., Items 6 and 15) and developmental (i.e., Item 8) indicators, which required some knowledge of the offender’s history and background. They also included in that list items that reflect postcrime behaviors (i.e., Items 11 and 12). The remaining 11 items were precrime (i.e., Item 13) or crime scene behaviors. Of interest, the authors included one item (i.e., Item 10) that alludes to killing or attempting to kill the victim, further reinforcing the idea of a connection between sexual homicide and sexual sadism.
More recently, Kingston, Seto, Firestone, and Bradford (2010) examined the validity of a series of sexual sadism indicators. The sexual sadism markers used in their analyses were a DSM diagnosis of sexual sadism, level of nonsexual violence during the offence, severity of sexual violence, and sexual arousal to nonsexual and sexual violence. Kingston et al. used the Sex Offender Risk Appraisal Guide (SORAG) as a means of controlling for the level of risk. Results indicated that the SORAG was the best predictor of violent recidivism while none of the other behavioral indicators uniquely contributed to the prediction of violent recidivism. Both the SORAG scores and phallometric scores significantly predicted whether an offender sexually recidivated. Despite these results, there are potential conceptual issues with Kingston et al.’s findings. The authors equated increased levels of nonsexual and sexual violence during the course of the crime to sexual sadism markers when empirical evidence has suggested that the mere presence of violence, sexual or otherwise, is present in many sexual assaults (Marshall & Kennedy, 2003). Given the complex nature of sexual violence and its relationship to sexual sadism, an incident of sexual recidivism cannot be unequivocally equated to recidivating in a sexually sadistic manner. Conversely, because some of the indicators used in the study show predictive validity of sexual recidivism, it does not necessarily support the construct validity of sexual sadism.
Nitschke, Osterheider, and Mokros (2009) assessed the validity of Marshall and Hucker’s (2006) Sexual Sadism Scale using a sample of 50 male forensic patients who had been diagnosed as sexually sadistic (i.e., DSM-IV-TR) and 50 male nonsexually sadistic patients chosen at random from a forensic hospital in Germany. Using Mokken scaling, the authors determined that 10 of the 17 items included in the original scale (plus an additional item—insertion of object[s] into victim’s bodily orifice[s]) were most useful in identifying sexual sadists (Items 1, 2, 3, 4, 5, 7, 11, 14, 16, 17 in Table 1). 2 Nitschke and colleagues determined, using a cutoff score of four items, that Marshall and Hucker’s instrument was able to discriminate between sadists and nonsadists. According to the authors, Mokken scaling is beneficial because it provides information regarding the relative importance of the items being analyzed and the overall strength of the scale. Furthermore, Nitschke and colleagues concluded that gratuitous violence, the exercising of power and control, humiliation of victims, and being sexually aroused by these acts were the most important items in discriminating sexual sadists from other sexual offenders.
Method
Sample
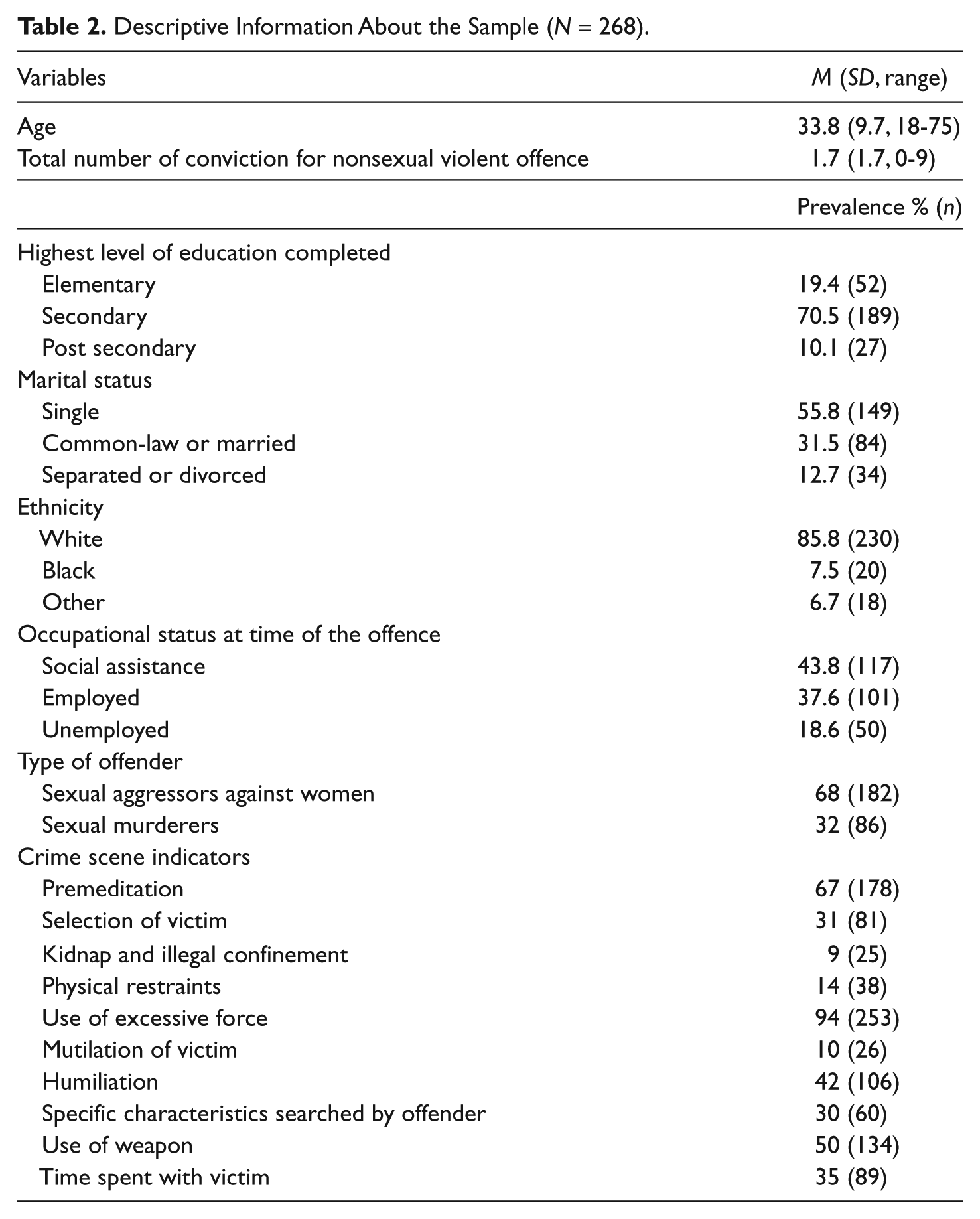
The sample comprised 268 adult males having been convicted of a sexual crime and sentenced to a federal penitentiary in the province of Quebec, Canada. This group included two subsamples, a group of sexual aggressors (n = 182) and a sample of sexual murderers (n = 86). The sample of sexual aggressors of women includes consecutive admissions at the Regional Reception Center (RRC), a maximum-security penitentiary, between 1994 and 2000. Federally sentenced offenders are those having received a prison sentence of more than 2 years for their crime. All men (low-, medium-, high risk) having been federally sentenced for a sex crime are first sent to the RRC for correctional risk and needs assessment. The average stay in this institution is about 6 weeks, after which they are typically transferred to another institution suited to their risk and treatment needs (low-, medium-, or high-security penitentiary). A similar sampling strategy was used to recruit the sample of sexual murderers. All sexual homicide offenders were serving a federal sentence and were incarcerated in a penitentiary in the province of Quebec at the time of the study. The recruiting of sexual murderers was done in a two-step process to obtain a sufficient sample size for statistical analyses. First, following the same sampling procedure used for the sample of sexual aggressors, all men having been federally sentenced for a sexual homicide in the province of Quebec between 1994 and 2000 were included in the study (n = 23). To increase this sample, all sexual murderers who were serving their prison sentence in the province of Quebec between 1994 and 2000 were recruited. Hence, all sexual murderers who were serving their sentence at that time, independent of the year their prison sentence started (e.g., 1970s, 1980s, etc.), were recruited for this study (see Beauregard & Proulx, 2002). The participation rate for this sampling procedure was low (just over 60%). There are no clear answers as to why the participation rate was low. We can hypothesize that those individuals who had been incarcerated for a longer period of time (as opposed to those recently incarcerated) may has been solicited several times in the past (i.e., psychologist, criminologists, parole board members, etc.) and were more reluctant to discuss, once again, their crime(s) to someone. This sampling procedure, however, helped raise the sample size of sexual murderers to 86. Note that, using Ressler and colleagues’ (1988) definition of sexual homicide, offenders had to meet at least one of the following criteria to be included in the sexual murderer group: (a) victim’s attire or lack of attire, (b) exposure of the sexual parts of the victim’s body, (c) sexual positioning of the victim’s body, (d) insertion of foreign objects into the victim’s body cavities, (e) evidence of sexual intercourse (oral, anal, or vaginal), and (f) evidence of substitute sexual activity, interest, or sadistic fantasy. Descriptive information about the sample can be found in Table 2. On average, the sample was 34 years old, Caucasian, with a high school diploma, and single at the time of the offence.
Descriptive Information About the Sample (N = 268).
Procedures
A research assistant solicited the participation of convicted offenders. All research assistants (graduate students in criminology) were trained by a licensed psychologist. The offenders who chose to participate signed a consent form explaining that the data would be used for research purposes only. Data were coded by research assistants using three sources of information: a semistructured interview with each offender, victim statements regarding the offence (not present for sexual homicide), and police reports of the event. In the event there was a discrepancy between interview data and official data, official data were used. A total of 84.7% of offenders had only one victim. Only 8.6% of offenders had two victims and 6.7% had three or more victims. Because the vast majority of offenders (84.7%) only had one victim, data were coded using information available on the first victim.
Variables
Crime scene variables
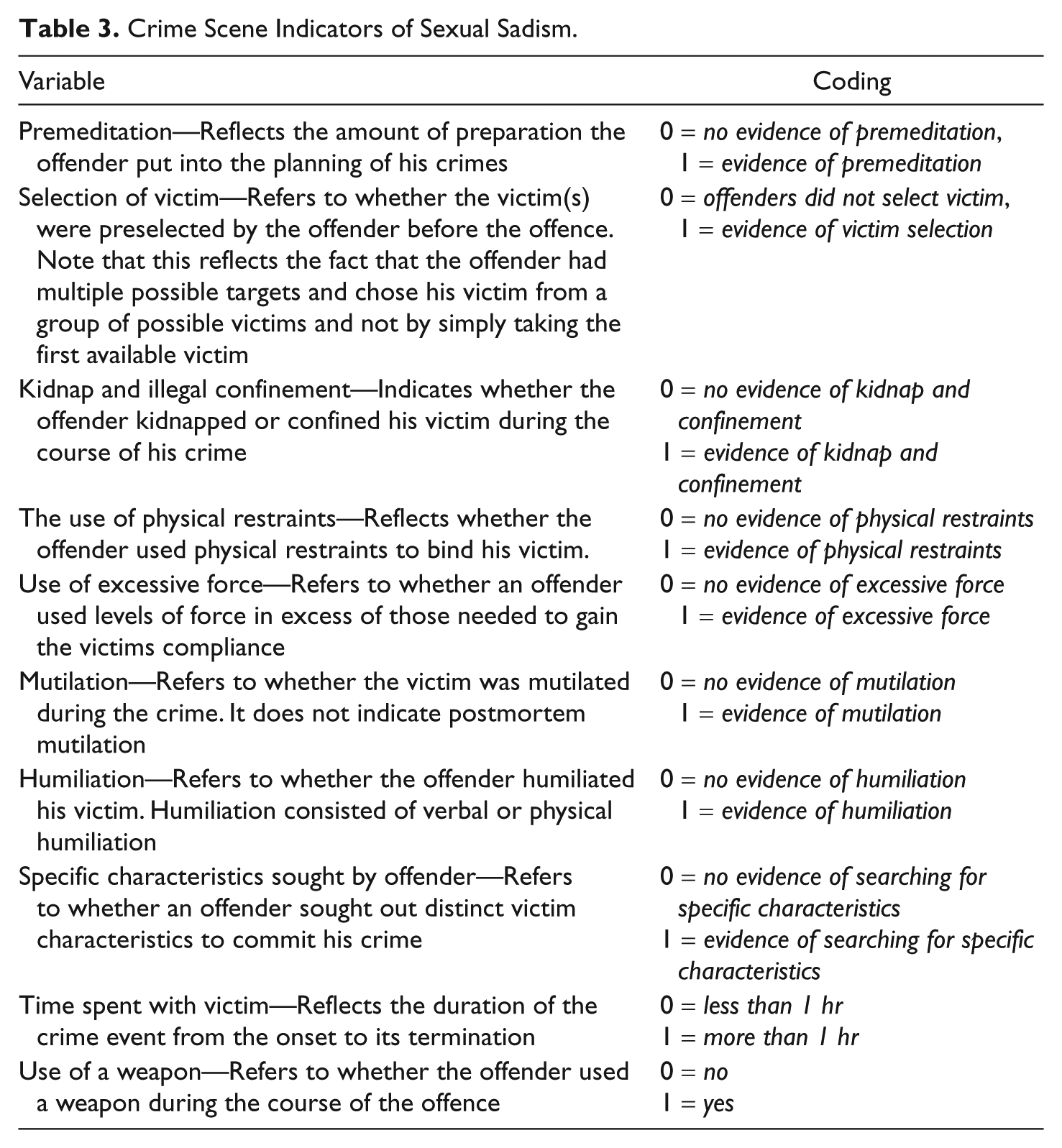
The indicators of sexual sadism inspected here reflect the offender’s behaviors during the crime event. Therefore, historical/developmental (e.g., history of cruelty against an animal, history of choking a partner) and psychological indicators (e.g., violent sexual fantasies, sexual arousal to violent cues) of sexual sadism were excluded from the study. Crime scene variables were selected by reviewing the clinical and empirical literature on sexual sadism and selected variables consistently identified as markers for nonhomicidal and homicidal sexual sadists. We drew sexual sadism indicators from empirical studies (Beauregard & Proulx, 2002; Dietz et al., 1990; Gratzer & Bradford, 1995; Knight & Prentky, 1990; Marshall, Kennedy, & Yates, 2002; Marshall, Kennedy, Yates, & Serran, 2002; Marshall & Fernandez, 2000; Marshall & Kennedy, 2003; Marshall & Yates, 2004; Proulx et al., 2006), clinical or behavioral accounts of sexually sadistic offenders (APA, 2000; Brittain, 1970; Groth, Burgess, & Holmstrom, 1977; Hucker, 1997; Marshall & Hucker, 2006; Ressler et al., 1988; Yates, Hucker, & Kingston, 2008), and studies using sexual sadism scales (Knight & Cerce, 1999; Marshall & Hucker, 2006; Proulx, 1989). Of these 10 items selected for the study (Table 3), 5 were also found in Marshall & Hucker’s (2006) scale—that is, premeditation, kidnapping and confinement, the use of physical restraints (i.e., bondage), mutilation, and humiliation. The inclusion of the remaining 5 items (i.e., selection of victim, specific characteristics sought by the offender, time spent with the victim, use of excessive force, and use of weapon) were guided by empirical research indicating that these items are associated with sexually sadistic offenders (murderers and nonmurderers; for example, Beauregard & Proulx, 2002; Dietz et al., 1990).
Crime Scene Indicators of Sexual Sadism.
Diagnosis of sexual sadism
After conducting a clinical interview with the offender and reviewing the correctional files of the offender (e.g., description of the index crime, police crime files, previous psychological assessment, psychological assessments such as the Minnesota Multiphasic Personality Inventory–II [MMPI-II] results, etc.), a psychologist made a diagnosis of sexual sadism based on Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.; DSM-III-R; APA, 1987) criteria, the reference used at the time. Research assistants coded the presence (coded as 1) or absence (coded as 0) of a clinical diagnosis of sexual sadism based on the assessment intake. The offender’s diagnosis of sexual sadism was made using collateral information described previously and was not based solely on one particular source of information. The presence and absence of a clinical diagnosis of sexual sadism and the initial coding of crime scene variables at the time of intake were coded independently. At intake, a total of 9.3% (n = 19) of the sample was diagnosed as a sexual sadist. For a detailed review of the variables used in the analysis and their respective coding, refer to Table 3. All offenders were assessed for risk classification and treatment needs by psychologists in the first 6 weeks of being incarcerated.
Control variables
Several control variables were used in the study to avoid possible confounding effects due to sociodemographic differences. Although not specifically implicated in the sexual sadism scientific literature, these control variables were included because they have been shown to influence violent and sexual offending in previous studies. Age refers to the age of the offender at the time of the interview. On average, the offenders in the study were 33.8 years old (SD = 9.7, range = 18-75). The ethnic background of the offender has been included to rule out any possible cultural effects in crime scene behaviors. The sample was predominantly White (85.8%), followed by Black (7.5%), and “Other” (e.g., Asian, Aboriginal, and Middle Eastern; 6.7%). Education refers to the highest level of education obtained by the offender at the time of his arrest. On average, participants in the study were largely high school educated (70.5%). A rather large proportion (19.4%) finished only elementary school and 10.1% had some form of postsecondary education.
Analytical Strategy
The convergent validity (e.g., Shadish, Cook, & Campbell, 2002) of the crime scene indicators of sexual sadism was examined. Associations between crime scene indicators of sexual sadism and a diagnosis of sexual sadism were examined using a series of cross-tabulations and examining both the chi-square statistics and phi coefficient. 3 Chi-square statistics were used considering it is a nonparametric test that does not assume the parameter to be normally distributed. It was hypothesized that all crime scene indicators would be positively and significantly related to the diagnosis of sexual sadism because (a) the crime scene indicators and official diagnoses are tapping the same underlying disposition and (b) it is thought that the psychologists used police reports describing the nature and type of crime committed by the offender being assessed for sexual sadism. However, note here that the psychologists were blind to the selection, identification, and analyses of crime scene behaviors reflecting sexual sadism as defined in this study. Hence, it is unclear what aspects of the crime scene, if any, psychologists were using in their assessment of sexual sadism. The current study aims to determine what those characteristics are. The predictive validity of the crime scene indicators of sexual sadism was examined with respect to sexual homicide. Specifically, the study sought to examine the crime scene behaviors that are significantly related to killing the victim in the context of a sexual assault. Here, the term predictive validity is used strictly in the context of the statistical analysis conducted. Recall that the study is based on retrospective data. Hence, there is no attempt here to identify among the sample of offenders who is more likely to commit a sexual homicide on his next sex crime. More modestly, the study aims to determine whether the crime scene behaviors selected for this study significantly differentiate those having committed a sexual assault from those having sexually assaulted and killed their victim. The predictive validity was examined in a two-step process. First, crime scene indicators were cross-tabulated with the outcome of the sex crime event (sexual assault vs. sexual homicide). Second, the significant crime scene indicators were then entered into a series of logistic regression models to identify the ones that best characterize the men who did escalate their sexual assault to a sexual homicide.
Results
Convergent Validity of Crime Scene Indicators
The association between all crime scene indicators and a clinical diagnosis of sexual sadism are presented in Table 4. In terms of premeditation, those with a diagnosis of sexual sadism were more inclined to premeditate their crimes (89.5%) than those without such a diagnosis (62%). Although very few offenders kidnapped and confined their victims, sadists were more likely to do so (16.9% of sadists vs. 5.9% of nonsadists). Similarly, sadists were more likely to use physical restraints (33.3%) as opposed to nonsadists (10.9%). As one would expect, those who were diagnosed with sexual sadism tended to humiliate their victims more than those without a sadistic diagnosis (63.2% vs. 36.7%). Despite the fact that only some of the nonsadistic group mutilated (3.2%), the majority of those offenders mutilating their victims were diagnosed as sexual sadists (21.1%). All sadists used excessive amounts of force. The nonsadist group also tended to use excessive force (92.4%). The majority of sadistic offenders used a weapon during the offence (63.2%), and they did so in a higher proportion than nonsadistic offenders (42.2%).
Convergent Validity Analysis of the Crime Scene Indicators and a Diagnosis of Sexual Sadism.

p < .05. **p < .01.
Predictive Validity of Crime Scene Indicators
First, the group comparisons between sexual murderers and rapists were conducted using a series of cross tabulation for each of the sexual sadism items (Table 5). All the sexual murderers (100%) in the sample used more force than was necessary to subdue the victim. Likewise, 91.2% of rapists were exceedingly violent. Sexual murderers were also more prone to use a weapon. Just over two thirds of sexual murderers (67.4%) used some sort of weapon to commit their crime, whereas 41.8% of rapists used a weapon. Rapists tended to display higher levels of humiliation. Three quarters of the sexual murderers (75.7%) did not humiliate the victim, whereas just below one half of the rapists (49.2%) did. Sexual murderers tended to mutilate their victims more so than rapists. Whereas the majority of rapists (94.5%) did not mutilate their victims, 18.6% of sexual murderers did mutilate their victims. Sexual murderers spent marginally more time with their victims as opposed to rapists. A total of 46% of sexual murderers spent more than 1 hr with their victim whereas only 29.3% rapists spent the equivalent amount of time. Four of the crime scene variables in the study did not discriminate between sexual murderers and rapists. Both sexual serial murderers and rapists were equally likely to premeditate their crimes. Neither group showed a marked tendency toward victim selection, the use of physical restraints, or kidnap and confinement of their victims.
Predictive Validity Analysis of the Crime Scene Behaviors of Rapists and Sexual Murderers.

p < .05. **p < .01. ***p < .001.
Multivariate Analyses of Crime Scene Indicators of Sexual Sadism
In this section, a series of logistic regression analyses were run to determine the convergent and predictive validity of crime scene indictors of sexual sadism. The findings of the logistic analyses are reported in Table 6. The covariates of a diagnosis of sexual sadism are presented in the left column (i.e., convergent validity) whereas the covariates of sexual homicide are presented in the right column (i.e., predictive validity). The findings are discussed below.
Logistic Regression Analysis of Crime Scene Indicators and Their Association With Sexual Sadism (Clinical Diagnosis) and Sexual Homicide.

Note: CI = confidence interval. Dependent variable: 0 = nonsadist, 1 = sadist, reference category = nonsadist (0). All independent variables are coded as 0 = absence, 1 = presence. Reference category is absence (0) for all variables.
p < .05. **p < .01. ***p < .001.
Convergent validity
When looking at convergent validity using logistic regression analyses, only four indicators remained significantly associated with a diagnosis of sexual sadism. Study findings show that individuals with a diagnosis of sexual sadism were more likely to mutilate their victims (odds ratio [OR] = 7.95, p < .01, 95% confidence interval [CI] = [2.02, 31.32]), premeditate their crimes (OR = 5.21, p < .05, 95% CI = [1.17, 23.77]), use physical restraints during the commission of their offence (OR = 4.07, p < .05, 95% CI = [1.37, 12.05]), and humiliate their victims (OR = 2.95, p < .05, 95% CI = [1.10, 7.87]). 4
Predictive validity
Next, we looked at the covariates of sexual homicide using logistic regression analyses. For this analysis, the category “rapist” was used as the reference category to compute the OR. Given the violent nature of the offenders in the sample and the fact that it would be predicting excessively violent crimes (e.g., sadism and sexual murder), it was deemed that leaving the variable “excessive levels of force” in the analysis would provide distorted statistical results. As such it was removed from the analysis. Compared with rapists, sexual murderers were more likely to specifically select their victim (OR = 1.73, p < .05, 95% CI = [1.00, 3.01]). Sexual murderers were also much more likely to mutilate their victims as compared with rapists (OR = 3.93, p < .01, 95% CI = [1.70, 9.08]). Interestingly, sexual murderers were less likely to humiliate their victims (OR = 0.33, p < .001, 95% CI = [0.18, 0.61]) or search out specific victim characteristics (OR = 0.44, p < .05, 95% CI = [0.22, 0.86]). Finally, sexual murderers were more likely to use a weapon during their crime (OR = 2.88, p < .001, 95% CI = [1.68, 4.95]) and spend more than an hour with their victim (OR = 1.99, p < .05, 95% CI = [1.16, 3.41]). 5
Discussion
Convergent Validity of the Indicators
This study began by investigating the convergent validity of a series of crime scene indicators with an official diagnosis of sexual sadism. The results of this study suggest that only 40% of the indictors used in the analyses appeared to be related to a clinical diagnosis of sexual sadism based on the DSM-III-R criteria. Premeditation, the use of physical restraints mutilation, and humiliation were significantly related to receiving an official diagnosis of sadism. The finding that humiliation is significantly related to an official diagnosis of sexual sadism is not surprising given that one of the explicit requirements for a DSM diagnosis of sexual sadism is that an individual is sexually aroused by the physical or psychological suffering (i.e., humiliation) of his victim. The mere presence of humiliation may have been used as either a direct (i.e., if the offender admitted to being sexually aroused from humiliating their victim) or an indirect measure (i.e., if the offender excessively humiliated his victim in conjunction with other sexual sadism markers) of sexual arousal to humiliating acts. These results are similar to that of Marshall, Kennedy, Yates, & Serran (2002) who found that the most common feature of sexual sadism was sexual satisfaction from humiliating their victims. However, these results should be interpreted cautiously, as there were no direct measures of sexual arousal to humiliation, violence, or otherwise. On the other hand, offenders who humiliated their victim were more likely to receive a diagnosis of sexual sadism suggesting that psychologists may have relied on this behavior in diagnosing sexual sadism.
Two more important findings need to be highlighted. First, aside from humiliation, many of the prototypical indicators of sadism were found to be associated with an official diagnosis of sadism. These results are in line with much of the scientific literature on sexual sadism: an individual who carefully plans his crimes while perhaps torturing his victim (Marshall & Kennedy, 2003). Much like humiliation, the presence of mutilation was found to be a significant predictor of an official diagnosis of sadism. Again, this finding was not unexpected given the empirical evidence that supports its importance in diagnosing sexual sadism (Marshall, Kennedy, Yates, & Serran, 2002) and its prevalence in the scientific literature (Beauregard & Proulx, 2002; Marshall & Kennedy, 2003). However, 7 of the 10 items that were expected to be significantly related to a diagnosis of sadism were not. Nonsadists were just as likely to select a specific victim, kidnap and confine their victims, and search for specific victim characteristics as sadists were. Interestingly enough, nonsadists and sadists used excessive amounts of force during the course of their crime. Although these results were unanticipated, they are not completely unreasonable given the sample comprises violent rapists and sexual murderers. After all, selection of victim, the seeking of specific characteristics, and the use of excessive force have been reported for both sexual sadism and sexual homicide alike (Dietz et al., 1990; Proulx et al., 2006).
The multivariate analyses of the crime scene indicators of sexual sadism provided additional information about the convergent validity. More specifically, the multivariate analyses helped to identify those indicators providing independent and additional information about the individuals meeting the DSM criteria of sexual sadism. Hence, when controlling for other sociodemographic variables such as age, ethnicity, and level of education, the study’s findings showed that mutilation, humiliation, and premeditation emerged as the most robust indicators of a clinical diagnosis of sexual sadism. These three crime scene indicators therefore might represent key behaviors of the offender’s offending process that guide clinicians in establishing a diagnosis of sexual sadism. These findings are not surprising given that premeditation has been cited as one of the main markers of sexual sadism in the clinical and behavioral literature (e.g., Brittain, 1970; Dietz et al., 1990; Krafft-Ebing, 1886/1965; Marshall, Kennedy, Yates, & Serran, 2002). Similarly, the presence of humiliation is not unexpected as it is perhaps the most salient behavioral criteria of the DSM’s diagnosis of sexual sadism and empirical evidence suggests that it is perhaps the most important clinical indicator of sexual sadism (Marshall, Kennedy, & Yates, 2002; Marshall, Kennedy, Yates, & Serran, 2002; Marshall & Kennedy, 2003). Although not explicitly a diagnostic criteria for sexual sadism in the DSM, Marshall and colleagues have shown that clinicians consider mutilation to be an important indicator of sexual sadism. Furthermore, mutilation has consistently been found as one of the key characteristics of the offending behaviors of sadistic sexual murderers (Beauregard & Proulx, 2002; Dietz et al., 1990; Gratzer & Bradford, 1995; Proulx et al., 2006; Warren, Hazelwood, & Dietz, 1996). Given the inherent link between sexual sadism and sexual murder, it is not surprising that mutilation remains significant even after controlling for other sexually sadistic behaviors. After all, some of the earliest academic works of sexual sadism were based on the clinical behaviors of sexual murderers (Brittain, 1970; Dietz et al., 1990).
This study examined the usefulness of sexual sadism indicators as a means of predicting an escalation from rape to sexual homicide. Interestingly enough, we found that 60% of the crime scene indicators examined were different between rapists and sexual murderers. Rapists and sexual murderers were no more likely to premeditate their crime, select their victim, kidnap and confine, or use physical restraints during the course of their crime. The planning and the selection of a victim may all indicate a well-thought behavioral script to sexually coerce someone (Beauregard, Proulx, Rossmo, Leclerc, & Allaire, 2007). Again, given the nature of this sample, these results are not particularly surprising. Of importance is the comparison between rapists and sexual murderers. Sexual murderers, however, were more likely to use force, to mutilate, to use a weapon as well as to spend more time with their victim during the crime event. Conversely, rapists were more likely to humiliate and to seek out specific victim characteristics. These findings suggest that there may be two different types of sadistic sexual offenders: sadistic sexual aggressors (i.e., sadistic rapists) and sadistic sexual murderers. These two types of offenders may in fact be differentiated by the presence of humiliation and mutilation. When comparing the factors associated with a diagnosis of sexual sadism and those associated with sexual homicide, only humiliation and mutilation of the victim were significantly associated to both. This finding could be interpreted as there being differential manifestations of sexual sadism by rapists and sexual murderers. More specifically, it could be that humiliation is a more central aspect of the sadistic sexual aggressor of women, whereas mutilation might be more specific to the sadistic sexual murderers. Put differently, the sadistic rapists might get more pleasure from the verbal aggression that involves humiliation, whereas the murderers might need extreme physical violence (such as mutilation) to obtain sexual gratification. These indicators, therefore, along with humiliation and seeking specific victim characteristics, might not be reliable factors showing a risk to escalate to a sexual homicide. However, the reliability of humiliation for sexual murderers needs to be interpreted carefully. In the case of sexual murderers, the victim has been killed and is therefore unable to provide information to police regarding the presence or absence of humiliation, or the murderer may minimize the influence humiliation may have had in the homicide. In addition, the presence of humiliation may have been overlooked by crime scene investigators because there was no physical evidence of humiliation or it may have simply been overshadowed by the presence of mutilation.
This study is not without its limitations. This study is based on a relatively small sample of convicted offenders incarcerated in a Canadian penitentiary. The findings, therefore, may not apply to non-Canadian sex offenders as well as those who have not been caught by the police and convicted for their crime. Moreover, the study is limited by the crime scene variables included in the study. Only one crime per offender was analyzed to inspect sexual sadism, whereas clinicians will rely on any or all information available to them. Also, the study did not take into account whether the rapists attempted to kill or had the intention of killing his victim but did not due to circumstantial factors not taken into consideration in the empirical analyses.
Conclusion
Given the many definitions and definitional problems associated with sexual sadism, the results of this analysis were not completely unexpected. Despite these difficulties, we were able to demonstrate that just less than half of the crime scene variables used in the study were significantly related to a DSM diagnosis of sadism. Individually, premeditation, the use of physical restraints, mutilation, and humiliation were able to distinguish sadists from nonsadists. Further analysis indicated that mutilation, humiliation, and premeditation emerged as the most robust indicators explaining the unique variance of a clinical diagnosis of sexual sadism and whether an offender was a rapist or sexual murderer. The finding that humiliation, mutilation, and premeditation are key predictors of sexual sadism is unsurprising given the empirical and clinical evidence of their importance (Marshall & Kennedy, 2003). However, the overlap of humiliation and mutilation with different offender types suggests that there might be two different types of sexually sadistic offenders (i.e., sadistic sexual aggressors and sadistic sexual murderers) with associated crime scene behaviors. Taken as a whole, these indicators may be able to help clinicians not only identify sexually sadistic offenders using crime scene variables but also possibly direct future research. One such direction of future research may be to explore the possibility of different types of sadistic offenders. Our findings suggest that there may be two distinct types of sexually sadistic offenders (those who murder and those who do not) who are possibly distinguished by whether they humiliate or mutilate their victims. In this sense, there may not be an escalation to sexual homicide per se but rather something unique about offenders who mutilate their victims. Perhaps mutilation is indicative of a sexual preference for physical violence whereas humiliation represents a sexual preference for degradation and psychological cruelty. Conversely, humiliation and mutilation may be separate dimensional indicators of a higher order construct (sexual sadism) and other factors (e.g., environmental circumstances, victim characteristics) may account for an escalation from sexual assault to sexual homicide. Future research should expand on our findings (i.e., using more objective measures of sexual sadism) while further exploring Marshall and Huckers’s (2006) assertion that sexual sadism should be measured dimensionally.
Footnotes
Acknowledgements
The authors are grateful to Jean Proulx and Correctional Service of Canada for providing access to these data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
1.
Other methodologies have been used, such as combining official and clinical data with information obtained from self-report questionnaires (Knight, Prentky, & Cerce, 1994). The Multidimensional Assessment of Sex and Aggression (MASA) developed by Knight, Prentky, & Cerce (1994) includes a subscale measuring a sadism subscale that comprises three items—bondage, synergy of sex and aggression (sexual arousal to aggression), and sadistic fantasies. Unfortunately, the items used to measure each of the three components of sexual sadism were not presented nor were the association between these components and a clinical diagnosis of sexual sadism using the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria. Furthermore, the three items of sadism showed relatively high internal consistency but relatively low test–retest reliability.
2.
3.
A scale was created using all 10 crime scene variables. Polychoric and tetrachoric correlations were used due to the dichotomous nature of the variables. Offenders in the sample had a mean sexual sadism score of 3.74 (SD = 1.59, range = 0-8). The Cronbach’s alpha of the scale was .44, indicating low reliability.
4.
Premeditation, mutilation, and humiliation remained significant after controlling for the offenders’ age, ethnicity, and education (Model 2). Model 2 was a good fit to the data (Hosmer–Lemeshow, χ2 = 3.11, p = .925) and the model accounted for only 10% of the variance (Cox & Snell’s R2 = .104). Overall, the model was better at identifying nonsadists than sadists (nonsadists: 99% correctly identified, sadists: 6% correctly identified).
5.
When controlling for the offenders’ age, ethnicity, and education, selection of victim, mutilation, and use of weapon remained significant predictors of sexual murderers, whereas humiliating the victim and searching for specific characteristics remained significant predictors of the rapist group (Model 2). Model 2 was a good fit to the data (Hosmer–Lemeshow, χ2 = 8.10, p = .423) and the model accounted for 27% of the variance (Cox & Snells R2 = .270). The model predicted sexual aggressors of women better than it predicted sexual murderers (sexual murderers: 61% correctly identified, sexual aggressors against women: 88% correctly identified).