
Abstract
Given the growing number of women who are incarcerated across the United States, the current study investigated the relationships among female inmates’ perceptions of their own stress, external locus of control (LOC), social support adequacy, and various aspects of psychological functioning. Generally, female inmates with a self-reported history of childhood sexual abuse did not differ from their nonabused counterparts on the variables of interest. Results suggested that female inmates’ perceptions of higher stress, a higher degree of external LOC, and inadequate social support correlated with greater symptoms of depression and hopelessness as well as lower self-esteem. In regression analyses, stress and social support were significant predictors for depression and anxiety. In contrast, stress was the only significant predictor of hopelessness and self-esteem. Finally, none of the predictors examined here was significant in the prediction of traumatic stress. Overall, findings suggested the importance of stress and social support in the prediction of female inmates’ adjustment, specifically their symptoms of depression and anxiety.
Since 1980, the number of women who were incarcerated in the United States tripled, with a 33% increase in the last decade alone (Elias, 2007; U.S. Department of Justice, 2008). With approximately 200,000 women currently incarcerated in prison or jails and an even greater number on parole or probation, women now account for almost 18% of the total corrections population in the U.S. (Glaze, 2010). Given the growing number of females involved in our legal system (U.S. Department of Justice, 2009), research on their psychological adjustment (Drapalski, Youman, Stuewig, & Tangney, 2009; Green, Miranda, Daroowalla, & Siddique, 2005; Islam-Zwart, Vik, & Rawlins, 2007) and beliefs (Slotboom, Hendriks, & Verbruggen, 2011) is needed. Thus, the current study examined predictors of psychological adjustment (e.g., depression, anxiety, hopelessness) among female inmates in a corrections facility, as they are a growing (i.e., over the past two decades; Raj et al., 2008; U.S. Department of Justice, 2008) and historically underserved (Haywood, Kravitz, Goldman, & Freeman, 2000) population.
Although the majority of previous research examined male inmates’ adjustment, an increasing number of studies recognized the unique characteristics, needs, and life experiences of female inmates (Drapalski et al., 2009; Faust & Magaletta, 2010; Gussak, 2009b; Raj et al., 2008; Slotboom et al., 2011; Warren et al., 2002). This research suggested that female inmates displayed higher levels of depression, stress, disturbing thoughts, suicidality, anxiety, and posttraumatic stress disorder (PTSD) symptoms relative to male inmates (Boothby & Durham, 1999; Coolidge, Marle, Van Horn, & Segal, 2011; Daigle & Côté, 2006; Peters, Strozier, Murrin, & Kearns, 1997; Sheridan, 1996). Consistently, Drapalski and colleagues (2009) reported that female inmates scored significantly higher on the somatic, anxiety, phobias, and traumatic stress scales of the Personality Assessment Inventory, whereas male inmates experienced more symptoms of mania, antisocial traits, and alcohol problems. Furthermore, female inmates experienced higher rates of mental illness (75%) relative to their male counterparts (63%; James & Glaze, 2006). Steadman, Osher, Robbins, Case, and Samuels (2009) also found twice the rate of Axis I psychopathology among female inmates relative to male inmates.
In addition to psychological difficulties, female inmates experienced lower self-esteem and reported more difficulties with social supports relative to their male counterparts (Sheridan, 1996), despite reporting more efforts to seek social support (Pelissier & Jones, 2006). In addition, in state correctional facilities, slightly more female inmates (70%) than male inmates (60%) sought mental health services during their incarceration (James & Glaze, 2006). Consistently, female inmates may be in more need of psychological services given their clinically elevated symptoms of anxiety, borderline personality traits, somatic concerns, and trauma symptomatology (Drapalski et al., 2009). Thus, female inmates need particular attention given their apparent differences from their male counterparts.
In an attempt to understand these differences, some studies speculated that female inmates’ poor psychological adjustment may be influenced by their victimization histories (Belknap & Holsinger, 2006; Blitz, Wolff, Pan, & Pogorzelski, 2005; Chesney-Lind, 2006; McDaniels-Wilson & Belknap, 2008). For example, studies suggested that female inmates endorsed higher rates of physical and sexual abuse relative to male inmates (Chen, 2010; Peters et al., 1997). Furthermore, prevalence rates of childhood sexual abuse (CSA; which ranged from 50% to 66%) were two to three times higher among female inmates relative to the general population (Asberg & Renk, 2012; Browne, Miller, & Maguin, 1999; Walsh, DiLillo, & Scalora, 2011). These victimization experiences may result in heightened anxiety, depression, self-destructive behavior, and overall psychological maladjustment among female inmates (Resick, 1993). As a result, there is a need to examine predictors of female inmates’ adjustment so that their unique service needs can be understood (Faust & Magaletta, 2010) and so that the corrections mental health system will no longer lag behind in their responses to female inmates (B. L. Green et al., 2005).
Stress and Coping
Rather than simply assessing female inmates’ relative distress in the context of their life experiences, current research should focus on variables that predict their psychological adjustment. For example, various coping resources may be related to female inmates’ adjustment (Negy, Woods, & Carlson, 1997). Generally, in community samples, females utilized more emotional and avoidant coping styles (Matud, 2004) and self-blame (Celinska & Siegel, 2010). They also perceived their stressors as less controllable than did their male counterparts (Matud, 2004). Consistently, studies also indicated that most female inmates used passive (e.g., avoidant) or maladaptive approaches to coping (Weaver, Haston Turner, & O’Dell, 2000). In addition, relative to their male counterparts, female inmates more frequently used escape strategies (Pelissier & Jones, 2006), with a majority of female inmates reporting a history of substance use (Mooney et al., 2008). Such strategies were related generally to poorer adjustment outcomes (see Aldwin, 1993, for a review). Adjustment to incarceration also may be particularly difficult for female inmates with children (Forsyth, 2003; Houck & Loper, 2002; Warren, Hurt, Booker Loper, & Chauhan, 2004). In fact, Celinska and Siegel (2010) noted that “separation from children due to imprisonment is indeed a “taxing” circumstance that requires coping” (p. 452).
Locus of Control (LOC)
These passive ways of dealing with stressful situations may be related to individuals’ perceptions of control. For example, individuals’ belief that they are not in control of outcomes (i.e., having an external LOC; Rotter, 1966) predicted their use of less active forms of coping relative to the approaches taken by individuals who believed that they were in control (i.e., having an internal LOC; Cummings & Swickert, 2010; Gomez, 1998). Consistently, studies reported that incarcerated individuals often demonstrated external LOC (Griffith, Pennington-Averett, & Bryan, 1981), such as the belief that luck or uncontrollable forces were responsible for their fate (Rotter, 1966). External LOC also may be linked to individuals’ tendency to not take responsibility for their actions (Hunter, 1994) and to “engage in maladaptive behavioral patterns that [become] self-fulfilling in that they would not perceive connections between their actions and the ensuing consequences” (Page & Scalora, 2004, p. 526). Although female inmates were more likely to take responsibility for their actions relative to male inmates (Pelissier & Jones, 2006), external LOC was reported commonly by female inmates (Gussak, 2009a). This tendency, which was associated with hopelessness (Hood & Carter, 2008), may explain, in part, female inmates’ heightened rates of psychological symptoms.
For example, studies found a link between external LOC and higher levels of stress (Abouserie, 1994), depression, anxiety (Gomez, 1998), hopelessness (Prociuk, Breen, & Lussier, 1976), worry (Scott et al., 2010), and deficits in the ability to cope with life stress (Carton & Nowicki, 1994). In longitudinal studies that examined a clinical sample (Harrow, Hansford, & Astrachan-Fletcher, 2009) and an incarcerated male sample (Reitzel & Harju, 2000), external LOC also was related to reports of depression, suggesting that external LOC can have consequences for individuals’ current and long-term functioning. Moreover, Lauer, de Man, Marquez, and Ades (2008) found that higher external LOC and less problem-focused coping were related to suicide attempts among female psychiatric inpatients.
Findings regarding the impact of CSA, one particular life stressor, on LOC, however, were more mixed. For example, Bolger and Patterson (2001) found higher levels of external LOC among children with a history of both sexual abuse and neglect, whereas some studies found no such differences in LOC between sexually abused and nonabused adults (Porter & Long, 1999; Silliman, 1993). Furthermore, Gwandure (2007) reported higher external LOC (as measured by the Rotter’s scale of internal and external LOC) for males and females with a history of child sexual abuse. The survivors also reported higher rates of PTSD, depression, and suicide ideation (in a South African sample; Gwandure, 2007). Given these findings, as well as the prevalence of CSA among female inmates (Browne et al., 1999), external LOC may be an important aspect to consider.
In addition to the relationship between external LOC and adjustment, internal LOC may provide a buffer against stressors. For example, Frazier, Steward, and Mortensen (2004) found that perceived control over past events (e.g., sexual assault) and control over the recovery process were associated with better adjustment (e.g., fewer PTSD symptoms). Increases in perceived control (internal LOC) and decreases in depression also were found among inmates who participated in an art therapy group (Gussak, 2009b). Although some attempts to control an uncontrollable event may predict greater distress in some situations (Clements, Sabourin, & Spiby, 2004), external LOC (rather than internal LOC) was one of the variables of interest in this study.
Perceived Social Support
In addition to LOC, the presence (or absence) of adequate social support may be important for female inmates, as social support was linked previously with psychological adjustment (e.g., depression, anxiety) in female college students (Asberg, Bowers, Renk, & McKinney, 2008). Research also suggested that social support had an inverse relationship to PTSD (see Brewin, Andrews, & Valentine, 2000, for a review) and hostility (Hochstetler, DeLisi, & Pratt, 2010). Similarly, Cullen (1994) argued that support from family and friends, especially during incarceration, decreased negative feelings (e.g., hostility) and predicted a more positive attitude at the time of release. Furthermore, aspects of female inmates’ adjustment, such as rule violations (Jiang & Winfree, 2006), self-esteem, and hopelessness (Dodge & Pogrebin, 2001), can be attributed to their supports and relationships.
Nonetheless, findings regarding the “amount” of support reported by female inmates were mixed. Some studies reported that female inmates had limited networks and low levels of social support (Singer, Bussey, Song, & Lunghofer, 1995), whereas other studies suggested that support was high and perceived as satisfactory by female inmates (e.g., partner support; Beer, Morgan, Garland, & Spanierman, 2007). There also has been some speculation that inmates who relied on outside support may evidence poorer adjustment during their incarceration, perhaps because they were removed from their loved ones during that time (Lindquist, 2000). Finally, studies indicated that social support adequacy was especially important to the psychological well-being of individuals with an external LOC (Vanderzee, Buunk, & Sanderman, 1997). Given that “social support and crime rates are inversely related” (Cullen, Wright, & Chamblin, 1999, p. 194), rehabilitation efforts that focus on improving interpersonal skills and social support may have an impact on adjustment to incarceration (see Cullen et al., 1999). Overall, the relationship between female inmates’ perception of social support (i.e., that support is available and accessible; Sarason et al., 1991) and their adjustment appeared complex, suggesting that further study is needed.
Current Study
Given that the number of female inmates has been growing over the past two decades (Raj et al., 2008; U.S. Department of Justice, 2008) and this group is underserved historically (Haywood et al., 2000), there has been a call for research aimed at understanding the psychological adjustment and treatment needs of this population (e.g., Covington, 2007; Faust & Magaletta, 2010). To that end, the current study examined relationships among CSA histories, stress, LOC, social support, and psychological adjustment (e.g., depression, anxiety, hopelessness, trauma symptoms, self-esteem) in a sample of women who were detained at a county jail at the time of their participation. It was expected that female inmates with a self-reported history of sexual abuse would experience poorer psychological adjustment (i.e., more depression, anxiety, hopelessness, and trauma symptoms as well as lower self-esteem) relative to their nonabused counterparts (e.g., Gwandure, 2007). Furthermore, given the mixed findings regarding childhood abuse and external LOC (e.g., Gwandure, 2007; Porter & Long, 1999; Silliman, 1993), this study explored the assertion that a more external LOC (i.e., a common characteristic of female inmates; Gussak, 2009a) would differentiate female inmates with and without a history of maltreatment.
Based on research with nonincarcerated samples (e.g., Gomez, 1998; Harrow et al., 2009), it was also predicted that female inmates’ external LOC score would be correlated with their psychological adjustment, such that a more external LOC would correspond with higher symptoms of depression, anxiety, trauma symptoms, and hopelessness as well as with lower self-esteem. It also was hypothesized further that higher social support would be linked with poorer psychological adjustment (e.g., Asberg & Renk, 2012; Brewin et al., 2000). Finally, external LOC and social support were expected to predict variance in depression, anxiety, trauma symptoms, hopelessness, and self-esteem beyond stress and childhood victimization histories. These variables have predicted independently psychological adjustment in a variety of samples (e.g., Brewin et al., 2000; Gwandure, 2007), but far less is known about the role that external LOC and perceptions of support play in predicting adjustment among female inmates, who frequently report histories of trauma (Browne et al., 1999; Warren et al., 2002).
Method
Participants
The participants for the current study were 39 females (M age = 37.82 years, SD = 8.92 years) who were incarcerated in a county jail at the time of their participation (see Table 1). In this sample, 64.1% (n = 25) of participants self-identified as being White, 30.8% (n = 12) self-identified as Black, and 5% (n = 2) did not provide information regarding their racial identity. The racial make-up of the sample was fairly representative of administrative data from the same corrections facility (e.g., 55% White female inmates; Potter, Lin, Maze, & Bjoring, 2011) and national data (32% Black female inmates; U.S. Department of Justice, 2010). It should be noted that, at the time of the data collection, the standard procedure within the corrections facility required that all inmates self-identify as belonging to one of two categories, White or Black. Thus, this procedure may have affected individuals’ reports in this study (i.e., preventing endorsement of “Hispanic/Latina” or other ethno-cultural groups).
Descriptives.
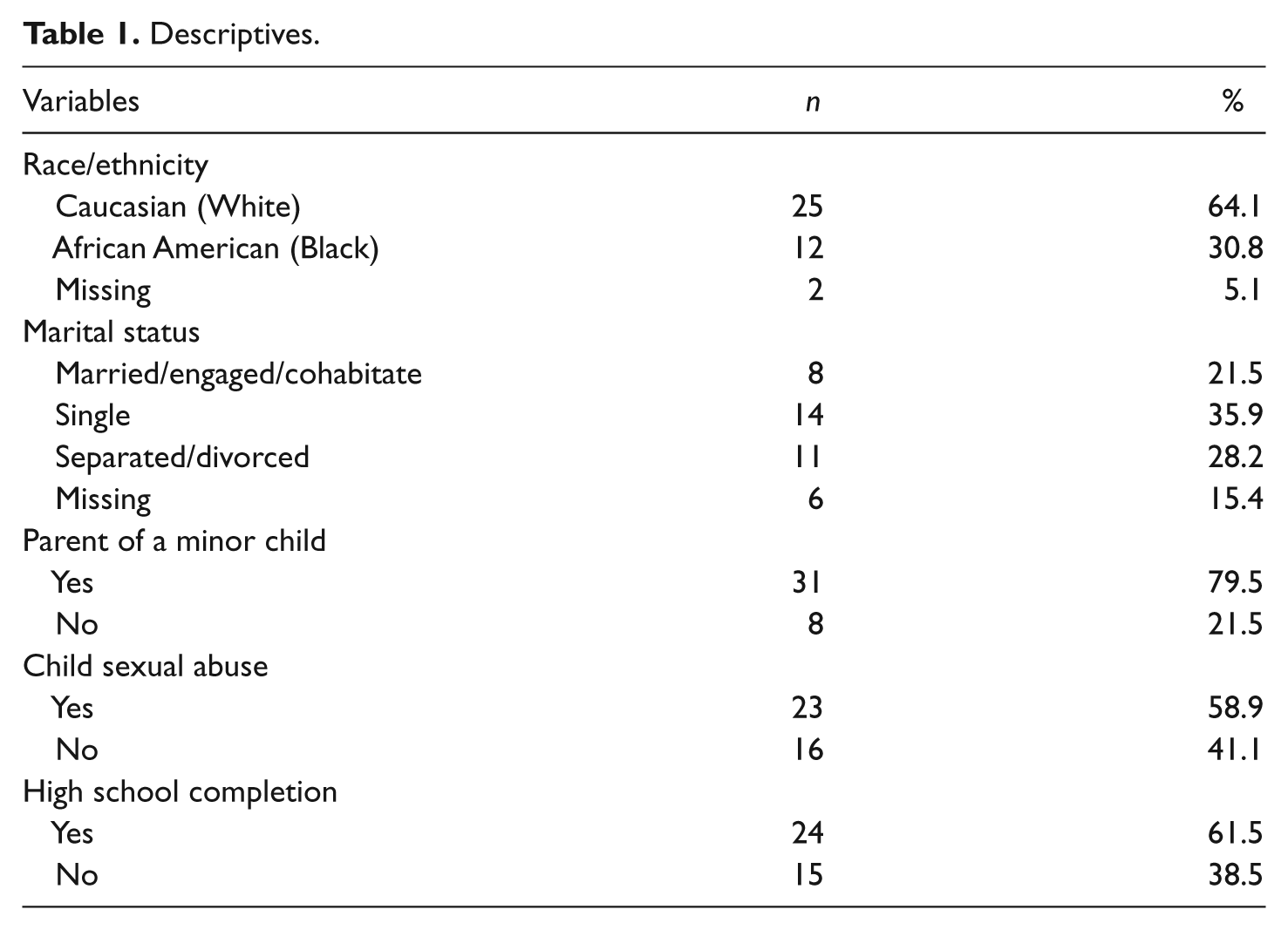
Participants reported an average of 12.20 years of education (SD = 1.57), with 38% not having completed high school. Furthermore, approximately 80% of participants reported being the parent of a minor child. This number was similar to previous studies of female inmates (79%; Warren et al., 2004). Participants were housed mainly in general population areas of the corrections facility (75%), and a majority reported some participation in available programs (i.e., parenting classes, support and/or religious groups). Finally, 59% of the overall sample (n = 23) reported a history of CSA. The prevalence of CSA among White and Black inmates was 64% and 50%, respectively.
Procedure
Following a full board review and subsequent approval from the Institutional Review Board and the Department of Corrections, this study was introduced to female inmates at a large corrections facility in the Southeastern United States. Of the approximately 100 inmates who were approached about the study via verbal announcements in the common area of each dorm, 39 elected to participate. Data collection was restricted to a few sessions during a 2-week period; thus, access to potential participants was limited. Access was limited also to inmates who were housed in the “open” dorms (i.e., approximately 150 women). Access to higher level security dorms, where female inmates were housed in individual cells (for safety, severe psychiatric, or medical reasons), was not granted at the time of the study.
After a brief introduction and a review of this study’s purpose, an investigator explained clearly the voluntary nature of female inmates’ participation and described the informed consent procedure. Female inmates who indicated interest in participating were asked to read carefully an informed consent form that described the purpose of the study, procedures related to participation, potential risks, benefits, and matters of confidentiality. It was stated that none of the questionnaire responses would be entered into participants’ medical charts or legal records. In addition, participants were informed that no payment or other incentive for participation would be given, in accordance with the rules of the Department of Corrections.
Next, female inmates who signed the informed consent form were provided with a demographics form and a packet of questionnaires to complete. For the current study, Flesch–Kincaid reading level scores ranged from 92.6 for the Rosenberg Self-Esteem measure (grade equivalent of 2.8) to 71 for the Beck Anxiety Inventory (grade equivalent of 4.3). The average Flesch–Kincaid reading level score of the questionnaires was 83.26 (average grade level equivalent of 3.64), with no participants reporting problems reading the questionnaires. An investigator was available to answer questions during each 1-hr data collection session, and a Spanish-speaking social worker was available to assist with translation. Following the completion of questionnaires, all participants received a debriefing sheet that encouraged contact with mental health staff via appropriate procedures if distress was experienced.
General Measures
Demographic and abuse variables
First, participants completed a demographics questionnaire which asked about their age, race, marital status (e.g., married, engaged, cohabitating, divorced, separated, or single), years of education, and parent status (i.e., whether they were the parent of a minor child, yes or no). They also completed a checklist of life events, including CSA before the age of 16 years.
Measures of Independent Variables
Stress
The 14-item Perceived Stress Scale (PSS; Cohen, Kamarck, & Mermelstein, 1983) was used as a measure of global appraised stress in participants. For example, items such as “In the last month, how often have you dealt successfully with irritating life hassles?” (reverse coded) were rated using a 5-point Likert-type scale ranging from 0 (never) to 4 (very often). A higher total score on the PSS indicated higher perceived stress. The PSS previously had adequate internal consistency with alphas of .75 (Cohen et al., 1983) and .89 (Mitchell, Crane, & Kim, 2008). The total score had a Cronbach alpha of .94 in this study.
LOC
In addition, the 29-item Rotter’s Scale of Internality Versus Externality was used to measure the extent to which participants endorsed an external LOC. Of the 29 items, 6 are filler items that Rotter (1966) included to make the scale more ambiguous to respondents. Participants indicated their agreement (yes or no) with statements such as “Many of the unhappy things in people’s lives are partly due to bad luck.” This scale has good internal consistency (α = .80; Cherlin & Brookover-Bourque, 1974). A sum total score was calculated based on the endorsement of external LOC items (i.e., with higher scores indicating higher external LOC). This total score had an internal consistency of .87.
Social support
The Multidimensional Scale of Perceived Social Support (MSPSS; Zimet, Dahlem, Zimet, & Farley, 1988) was used to assess perceptions of social support from family, friends, and significant others. Participants were asked to rate items, such as “I get the emotional support I need from my family,” on a 7-point Likert-type scale ranging from very strongly disagree to very strongly agree. A higher score on the MSPSS is indicative of higher perceived social support. In the original study, the MSPSS reported an internal reliability of .88 (Zimet et al., 1988) for the total scale. In a sample of survivors of CSA, the Cronbach alpha was .94 (female inmates and college students; Asberg & Renk, 2012) for the total scale. The total scale score had a Cronbach alpha of .90 in this study.
Measures of Dependent Variables
Depression
Participants completed the 21-item Beck Depression Inventory–II (BDI-II; Beck, Steer, & Brown, 1996) as a measure depressive symptoms. This measure has been used successfully as a screening tool for depression and to assess treatment response in incarcerated populations (e.g., Boothby & Durham, 1999; Gussak, 2006, 2009a, 2009b). Scores on the BDI-II range from 0 to 63, where scores from 0 to 13 represent minimal depression, scores from 14 to 19 represent mild depression, scores from 20 to 28 represent moderate depression, and scores at or above 29 are indicative of severe depression. Past uses of the BDI-II suggested good psychometric properties with an internal consistency of .92 and a test–retest reliability of .93 (Steer & Clark, 1997). The total score had a Cronbach alpha of .93 in this study.
Anxiety
The 21-item Beck Anxiety Inventory (BAI; Beck & Steer, 1993) was used to measure anxiety symptoms. Each item is rated on a 4-point scale, including symptom ratings of not at all, mildly (i.e., It did not bother me much), moderately (i.e., It was very unpleasant, but I could stand it), and severely (i.e., I could barely stand it). Scores ranging from 0 to 7 represent a minimal level of anxiety, scores from 8 to 15 represent mild anxiety, scores from 16 to 25 represent moderate anxiety, and scores from 26 to 63 represent severe anxiety. The BAI has displayed high concurrent validity with other self-report and clinical rating scales of anxiety (Beck, Epstein, Brown, & Steer, 1988). The total score had a Cronbach alpha of .91 in this study.
Hopelessness
The 20-item Beck Hopelessness Scale (BHS; Beck et al., 1988; Beck, Weissman, Lester, & Trexler, 1974) was administered as a measure of hopelessness. Each item is rated as either yes or no. In previous studies, BHS scores were related to BDI scores, clinicians’ ratings of hopelessness, and respondents’ suicidal ideation (Beck, Brown, & Steer, 1989). This measure had acceptable internal consistency with an alpha of .93 (Beck et al., 1974; Clements et al., 2004). The total score had a Cronbach alpha of .89 in this study.
Trauma symptoms
Participants completed the 100-item Trauma Symptom Inventory (TSI; Briere, 1995) as a measure of trauma symptoms. Items on the TSI tap symptoms of PTSD and acute stress disorder (ASD) as well as stress-related problems over the past 6 months. Each item is rated on a 4-point Likert-type scale, ranging from no experience of the symptom to frequent occurrence of the symptom. According to Briere (1995), the TSI demonstrated adequate criterion validity (i.e., child and adult trauma survivors had higher scores on all TSI scales) and adequate psychometric properties (e.g., average Cronbach alphas ranging from .83 [Snyder, Elhai, North, & Heaney, 2009] to .87 [Briere & Elliott, 1997]). The overall score (comprised of the clinical scales) had a Cronbach alpha of .86 in this study.
Self-esteem
The 10-item Rosenberg Self-Esteem Scale (RSE; Rosenberg, 1965) was used as a measure of global self-esteem. This measure uses a 4-point Likert-type scale ranging from strongly agree to strongly disagree. Participants were asked to indicate their agreement with statements such as “I feel I do not have much to be proud” (reverse coded). Higher scores indicated higher self-esteem. Previously, the RSE had adequate internal consistency with a reported alpha of .69 (inmates; Bond & Lee, 2005) and .84 (nonincarcerated adults; Richardson, Ratner, & Zumbo, 2009). The total score had a Cronbach alpha of .80 in the current study.
Results
Descriptive Statistics
Initially, means and standard deviations were calculated for study variables (see Table 2). With regard to the independent variables in this study, female inmates’ mean stress score (PSS) fell within the moderate to high range. This mean score was comparable with those in a previous study of individuals who had lost a loved one to suicide (M = 32.63; Mitchell et al., 2008). On the Rotter’s Scale of LOC, participants’ external LOC scores were similar to those found in a previous study that examined scores from battered women in a shelter for domestic violence victims (Brown, Reedy, Fountain, Johnson, & Dichiser, 2000). Moreover, female inmates’ scores on the MSPSS suggested that participants’ perceptions of support fell within the low range (i.e., inadequate support) relative to scores generally seen among nonincarcerated samples of women (e.g., M = 69.76 among female college students; Asberg et al., 2008).
Description of Study Measures.
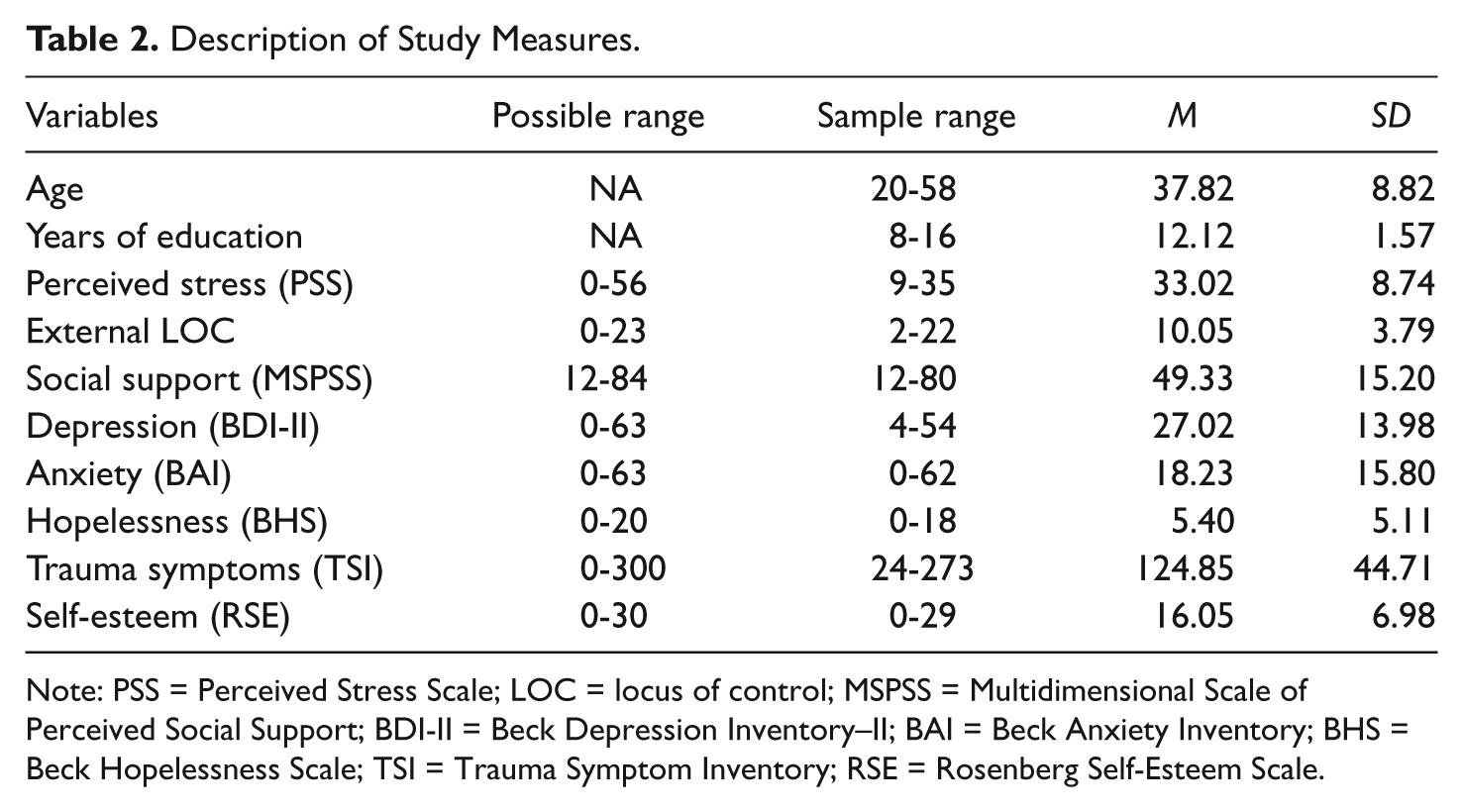
Note: PSS = Perceived Stress Scale; LOC = locus of control; MSPSS = Multidimensional Scale of Perceived Social Support; BDI-II = Beck Depression Inventory–II; BAI = Beck Anxiety Inventory; BHS = Beck Hopelessness Scale; TSI = Trauma Symptom Inventory; RSE = Rosenberg Self-Esteem Scale.
With regard to the dependent variables in this study, female inmates’ mean depression score (BDI-II) fell within the moderate range and was clinically relevant. Compared with other studies that obtained self-reports from female inmates (e.g., Varese, Pelowski, Riedel, & Heiby, 1998), participants in this study demonstrated slightly higher BDI-II scores. Specifically, 92.3% of the sample in this study (vs. 66% in Varese et al., 1998) scored above a score of 11 and 66.7% (vs. 34% in Varese et al., 1998) scored above a score of 18, suggesting the clinical significance of these scores. The mean BDI score for our sample also was higher than scores found for women in a federal prison (M = 21.10; Valentine & Smith, 2001) and for a community sample of battered women (M = 18.31; Clements et al., 2004).
Scores on the BAI for our sample also suggested that participants’ anxiety fell within the moderate range on average. Moreover, scores on the BHS fell within the mild range of hopelessness (Beck & Steer, 1993) and were similar to those found in community samples (domestic violence survivors, M = 5.80; Clements et al., 2004). Furthermore, female inmates’ scores on the TSI were higher than those of nonincarcerated samples with a PTSD diagnosis in other studies (M = 106.33; Gambetti, Bensi, Nori, & Giusberti, 2011). Based on scores on the RSE, participants in this sample also were exhibiting low self-esteem (given that scores between 15 and 30 on the RSE are considered “normal” and that scores below 15 are considered “low,” for example, Thompson-Martin, Keswick, Crayton, & Leveck, 2011; see Table 2)
Group Differences
To determine whether there were differences between female inmates who had a history of childhood abuse and those who did not, a series of t tests were examined (see Table 3). With regard to group differences, these t tests suggested that female inmates who had experienced sexual abuse did not differ significantly from their nonabused counterparts on any of the variables investigated in this study. Thus, this hypothesis was not supported.
Exploration of Group Differences.

Note: PSS = Perceived Stress Scale; LOC = locus of control; MSPSS = Multidimensional Scale of Perceived Social Support; BDI-II = Beck Depression Inventory–II; BAI = Beck Anxiety Inventory; BHS = Beck Hopelessness Scale; TSI = Trauma Symptom Inventory; RSE = Rosenberg Self-Esteem Scale.
p < .05. **p < .01. ***p < .001.
Furthermore, to examine whether there were differences between Black and White females, an additional series of t tests were examined (see Table 3). Results indicated that Black females were older than their White counterparts. These analyses also suggested that Black females reported significantly more trauma symptoms than their White counterparts.
Variable Relationships
Next, a correlation matrix was examined for bivariate relationships among each of the study variables (see Table 4). Results indicated that higher scores on the external LOC measure were related significantly to more stress (PSS), depression (BDI-II), and hopelessness (BHS) as well as to lower self-esteem (RSE) but were not related significantly to trauma symptoms or anxiety. Overall, endorsing a more external LOC corresponded with more negative outcomes. Results also suggested that female inmates’ perceptions of social support adequacy (MSPSS total score) were related significantly to stress (PSS), external LOC (LOC-external), depression (BDI-II), anxiety (BAI), hopelessness (BHS), trauma symptoms (TSI), and self-esteem (RSE). Overall, higher scores on perceived social support were related to less frequent endorsements of external LOC and to better psychological adjustment.
Correlations Among Study Variables.
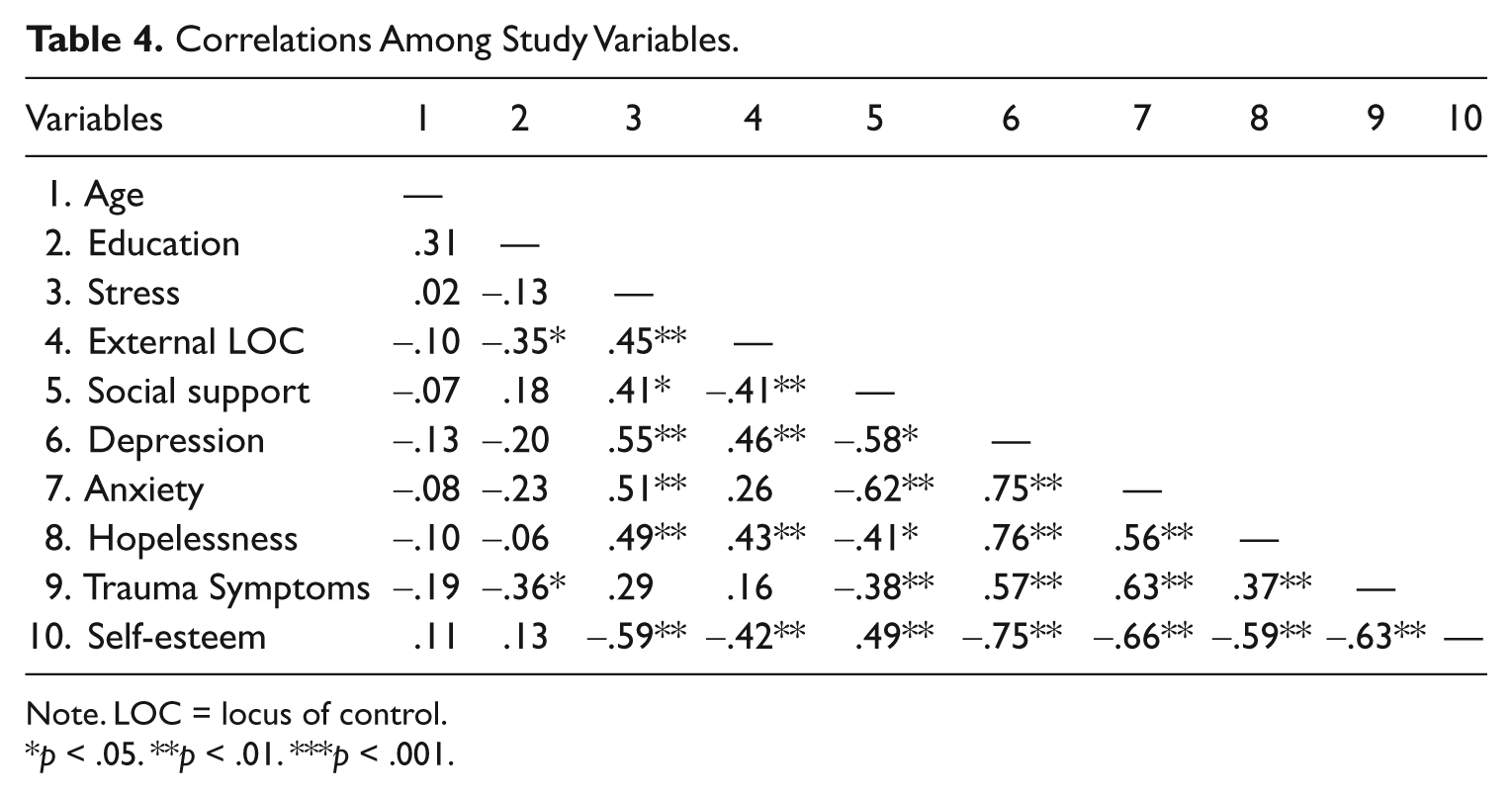
Note. LOC = locus of control.
p < .05. **p < .01. ***p < .001.
Predicting Adjustment Using Regression Analyses 1
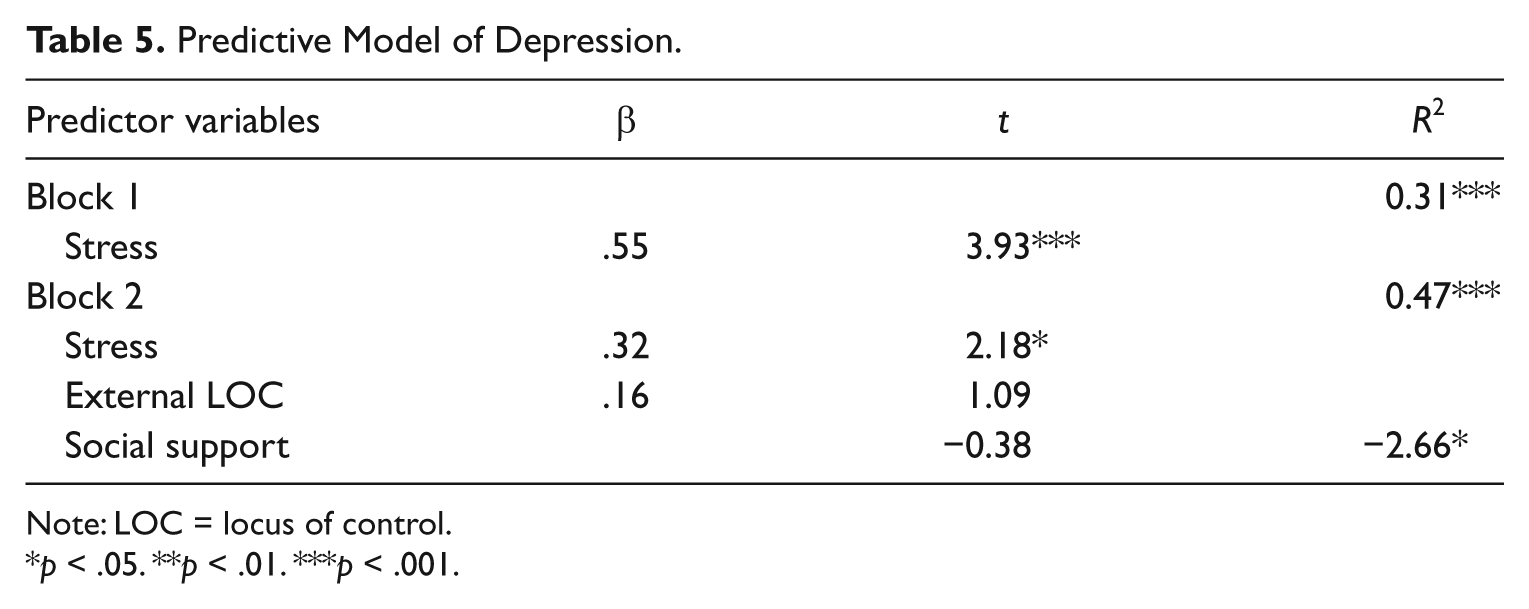
Next, regression analyses were conducted independently for each primary dependent variable (see Tables 5 through 9). Specifically, hierarchical multiple regression equations were used to examine the predictive value of stress, external LOC, and perceived social support for female inmates’ ratings of depression, anxiety, posttraumatic symptomatology, hopelessness, and self-esteem, respectively. For each regression equation, stress was entered in Block 1 to account for global feelings of stress that may be related to the current status of being incarcerated. Next, external LOC and perceived social support were entered in Block 2.
Predictive Model of Depression.
Note: LOC = locus of control.
p < .05. **p < .01. ***p < .001.
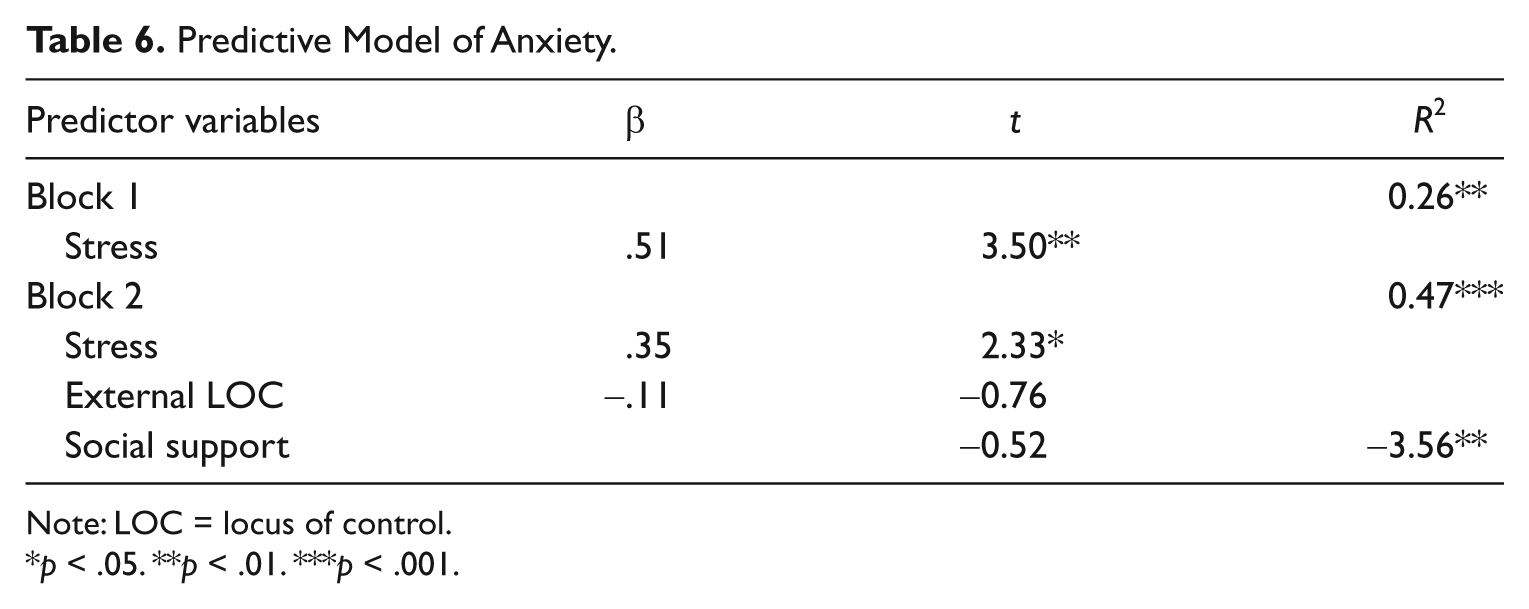
Predictive Model of Anxiety.
Note: LOC = locus of control.
p < .05. **p < .01. ***p < .001.
Predictive Model of Trauma Symptoms.

Note: LOC = locus of control.
p < .05. **p < .01. ***p < .001.
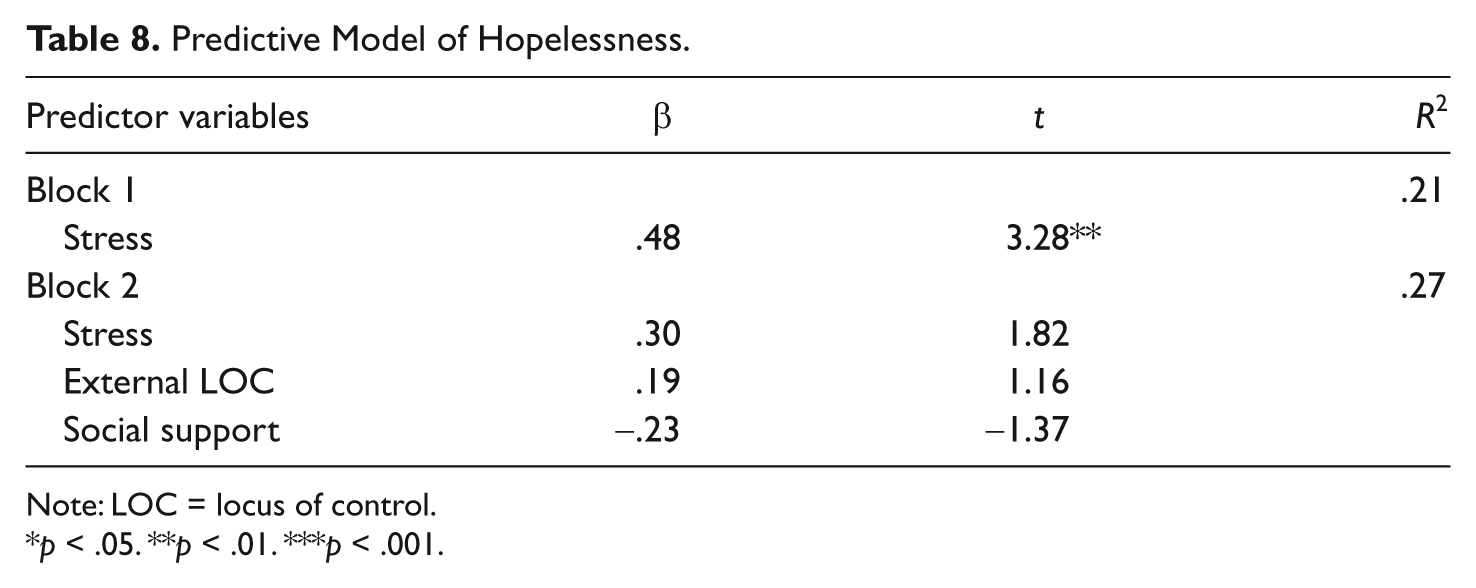
Predictive Model of Hopelessness.
Note: LOC = locus of control.
p < .05. **p < .01. ***p < .001.
Predictive Model of Self-Esteem.

Note: LOC = locus of control.
p < .05. **p < .01. ***p < .001.
For the first regression equation predicting depression (BDI-II scores), stress was significant in Block 1, F(1, 37) = 15.43, p < .01. Moreover, external LOC and social support contributed significantly to the model in Block 2, F(3, 35) = 12.18, p < .01. It should be noted, however, that only stress and social support remained significant predictors in the final model, which explained approximately 48% of the variance in BDI-II scores. Likewise, for the second regression equation predicting anxiety (BAI scores), stress was significant in Block 1, F(1, 37) = 12.28, p < .01. When external LOC and social support were added in Block 2, the model also was significant, F(3, 35) = 9.75, p < .01. Similarly, only stress and social support were significant predictors of anxiety in the final model, which explained approximately 42% of the variance in BAI scores.
In contrast, results for the third regression equation predicting trauma symptomatology (TSI scores) suggested that neither stress in Block 1, F(1, 37) = 2.73, p < .11, nor external LOC and social support in Block 2, F(3, 35) = 2.11, p < .11, contributed significantly to the model. Furthermore, for the fourth regression predicting hopelessness (BHS scores), stress in Block 1 predicted significantly BHS scores, F(1, 37) = 10.75, p < .01. In Block 2, however, neither external LOC nor social support contributed significantly to the model, although the overall model was significant, F(3, 35) = 5.36, p < .05. This model explained 27% of the variance. Finally, for the regression predicting self-esteem, stress in Block 1 predicted significantly RSE scores, F(1, 37) = 18.54, p < .01. In Block 2, however, neither external LOC nor social support contributed significantly to the model, although the overall model was significant, F(3, 35) = 8.92, p < .01. This model explained 40% of the variance in self-esteem.
Overall, the regression hypotheses were supported only partially. Stress and social support were significant predictors for depression and anxiety. In contrast, stress was the only significant predictor of hopelessness and self-esteem. Finally, none of the predictors examined here was significant in the prediction of traumatic stress.
Discussion
Previous studies highlighted that research regarding inmates focused mostly on males (Lewis, 2006); thus, female inmates’ unique experiences warranted further exploration (Covington, 2007; Steadman et al., 2009; Walsh et al., 2011). Given that the number of female inmates has been growing over the past two decades (Raj et al., 2008; U.S. Department of Justice, 2008) and that this population is underserved historically (Haywood et al., 2000), more research should be aimed at understanding female inmates’ psychological adjustment and treatment needs (e.g., Covington, 2007; Faust & Magaletta, 2010). To that end, the current study examined relationships among stress, LOC, social support, and psychological adjustment (e.g., depression, anxiety, hopelessness, trauma symptoms, self-esteem) in a sample of women who were detained at a county jail.
First, the rate of self-reported CSA among female inmates in this study (59%) is approximately twice that found in community samples. This finding is consistent with that of previous research (although other studies had larger sample sizes; for example, Asberg & Renk, 2012; Browne et al., 1999). Nonetheless, female inmates in this sample who were abused sexually did not rate themselves as being significantly different from their nonabused counterparts. As these findings were contrary to those of previous studies (e.g., Gwandure, 2007) and to the hypotheses for this study, being incarcerated may have been an important factor that provided commonality across all the women who were sampled for this study.
This lack of difference also may be attributed to inmates’ participation in trauma survivor and substance abuse recovery groups held in the dormitory where data collections were conducted. Some studies found that cognitive-behavioral and art therapy groups may affect inmates’ LOC in a positive way (e.g., by increasing internal LOC; Gussak, 2009b; Hunter, 1994). It is more likely, however, that the lack of differences could be explained by the distal nature of these female inmates’ childhood abuse histories. Their abuse occurred two decades prior to the collection of information for this study (i.e., prior to the age of 16 years), when these female inmates were 37.82 years on average. Overall, the specific role of trauma-focused and other supportive groups in ameliorating female inmates’ distress deserves further study.
Furthermore, it is likely that all these women (those with and without a history of childhood abuse) experienced adult victimization (e.g., Browne et al., 1999), with these experiences being a more salient predictor of current functioning. For example, Hood and Carter (2008) found no differences in external LOC and PTSD symptoms between women who had experienced childhood abuse only and those who reported both childhood abuse and adult assault. The fact that the frequency and severity of current trauma symptoms (irrespective of experiences of CSA) were related to several aspects of female inmate’s psychological adjustment in this sample would support this suggestion. Specifically, consistent with previous studies of female inmates (Resick, 1993), the female inmates in this study who reported a higher degree of perceived stress as well as traumatic stress symptoms experienced more depression and anxiety, evidenced a more hopeless outlook, and endorsed lower self-esteem. Furthermore, trauma symptoms were the only characteristic that proved to be different across White and Black female inmates. Thus, the role of adult victimization, particularly in female inmates who are culturally diverse, should be examined further in future investigations.
Similar to the findings of Prociuk and colleagues (1976), external LOC was related to depression and hopelessness in this sample but failed to predict any of the outcomes examined in this study when stress and social support also were considered. It may be that internal LOC is a more robust predictor. For example, Mutlu, Balbag, and Cemrek (2010) found that internal (but not external) LOC was related significantly to college students’ hopelessness (as assessed by the BHS). This assertion should be considered in future research. Moreover, higher levels of external LOC (and stress) were related to lower self-esteem in our sample. These findings were consistent with those of previous studies that link external LOC (in college students; Mutlu et al., 2010) and stress (e.g., Abouserie, 1994) to lower self-esteem. In addition, the related construct of optimism was related positively to female inmates’ perception of health during incarceration (Heigel, Stuewig, & Tangney, 2010). Thus, LOC appears to have potential as a predictor of psychological and physical health. Overall, this study suggested that the interplay among female inmates’ LOC and their psychological adjustment is complex and in need of further study.
Similarly, although external LOC did not predict psychological adjustment in this study, it may be that LOC can become intertwined with social support. For example, Page and Scalora (2004) found that increased internal LOC predicted help-seeking behaviors as well as treatment participation. Such findings also may be relevant to the corrections setting, which provides opportunities for intervention (Gussak, 2009a) in some cases (although less than one third of jail inmates receive treatment during their incarceration; Karberg & James, 2005). For those inmates who are involved in treatment, however, assessment of their LOC could prove useful (Page & Scalora, 2004). It also could be that the relationship of LOC and psychological adjustment beyond stress “may differ depending upon whether the stressors are within or outside [the individual’s] control” (Hamlyn-Wright, Draghi-Lorenz, & Ellis, 2007, p. 490). Thus, it may be helpful to focus on female inmates’ perceptions and sources of stress and support.
In fact, social support emerged as a promising predictor of female inmates’ depression and anxiety. Specifically, women’s perceptions of social support predicted their symptoms of depression and anxiety above and beyond their self-reported global stress, with these two regression models accounting for nearly half of the variance in depression and anxiety. Although previous research linked female inmates’ coping resources and adjustment (Negy et al., 1997), this study adds to the literature by examining specifically perceived social support in relation to external LOC as a predictor of female inmates’ psychological adjustment. Noting the significant contribution of social support in this study, clinicians may benefit from addressing women’s perceptions of their supports in their interventions. Moreover, future studies may examine changes in perceived support over time and as a result of women’s participation in treatment. Specifically, given that women are “likely to report seeking social support from others as a way to cope with difficult situations, additional research on the effectiveness of treatment programs that focus on the relational orientation of women may be warranted” (Pelissier & Jones, 2006, p.118).
Several limitations of the current study should be noted, including the use of self-report measures, a primarily Caucasian sample, and a small sample size. Specifically, reliance on self-report data in studies of psychological adjustment always presents a challenge, and incarcerated populations may perceive a secondary gain (Walters, 2006) from either overreporting (to get the attention of mental health staff) or underreporting (based on fear of being moved to a stricter level of care) symptoms, despite the anonymous nature of the study. In corrections settings, however, malingering may be more of an issue in the referral process (to obtain psychiatric services; for example, McDermott & Sokolov, 2009) and less likely among those who self-selected for a research study. In either case, future studies may want to utilize clinical interviews, diagnostic information, and third-party reports to corroborate findings and better capture symptom presentation among incarcerated populations who are likely to be distressed significantly.
Moreover, the ethnic and racial breakdown of our sample may be seen as a limitation. Specifically, a majority of our sample (64%) was Caucasian. Nonetheless, the distribution in this sample was fairly representative of the racial and ethnic demographics of the female inmates at the corrections facility from which the sample was drawn (Potter et al., 2011). Future studies may want to investigate differences in predictor variables and outcomes as a function of female inmates’ racial and ethnic backgrounds, as some groups (e.g., African American women) may be overrepresented in our correctional system (Freudenberg, 2002) and may be experiencing more trauma symptoms (based on the findings presented here).
This small sample size (N = 39) in this study presents another limitation. Considering the population from whom the data were collected, however, a smaller than desirable sample size may be expected. For example, Murphy (1990) utilized a sample of 19 male inmates to assess posttreatment changes in LOC, whereas Harm and Phillips (2001) interviewed 38 women to assess predictors of postincarceration adjustment. Moreover, Van Harreveld, Van der Pligt, Claassen, and Van Dijk (2007) examined active emotion coping in relation to psychological and physical well-being in a sample of 30 male inmates. In addition, Severance (2004, 2005) conducted in-depth interviews with 40 women (out of approximately 1,800) who were incarcerated in an Ohio prison. Thus, the sample size of this study was consistent with that of previous work in this area and utilized a 10:1 ratio of participants to predictors (e.g., Miller & Kunce, 1973). As “rules of thumb such as a ratio of 10 participants for every predictor variable will almost always underestimate necessary sample size” (Maxwell, 2000, p. 435), Maxwell (2000) suggested that the ratio of sample size to predictors should be close to 20:1, and Pedhazur and Schmelkin (1991) stated that this ratio should be no less than 30:1. Some authors also argued that multiple regression with small samples (i.e., N < 100; Bryk & Raudenbush, 1987), irrespective of the number of predictors, may not be appropriate (Zhang & Willson, 2006).
In contrast, and in support of our sample size, Wampold and Freund (1987) estimated that an expected R2 of .30 for three independent variables would require a sample size of 37. Similarly, Knofczynski and Mundfrom (2008) suggested that an estimated R2 of .25 or .30 for three predictors would require sample sizes of 40 and 32, respectively. Specifically, Knofczynski and Mundfrom arrived at their recommendation by examining the similarity (denoted “τ”) between “the population regression coefficients and the corresponding predicted values obtained when using the sample regression coefficients from numerous replications” (p. 433). “Good” tolerance levels required that at least 95% of the correlation coefficients met or exceeded τ = .92. It is important to note that an accurate estimation of the squared multiple correlation coefficient (R2) is essential and a lower expected R2 would require an increase in sample size. For example, our lack of significance for the prediction model of trauma symptoms (R2 =.16, p = .11) may, in part, be attributed to the small sample size. Even with a smaller sample size, the current study illuminated important relationships among stress, LOC, social support, and psychological adjustment.
In summary, the findings of the current study indicated that female inmates experience clinically elevated levels of depression and anxiety as well as significant relationships between external LOC, social support, and various indicators of psychological adjustment. In regression analyses, female inmates’ perceived stress was an important predictor of most psychological adjustment variables, and their social support predicted their depression and anxiety when their perceived stress also was considered. Thus, these findings suggested the importance of assessing female inmates’ perceived social support, with improvements in such support being an important target of different interventions that could be offered to this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.