
Abstract
This review focuses on the predictive value of neurobiological factors in relation to cognitive–behavioral therapy outcome among individuals with antisocial behavior. Ten relevant studies were found. Although the literature on this topic is scarce and diverse, it appears that specific neurobiological characteristics, such as physiological arousal levels, can predict treatment outcome. The predictive value of neurobiological factors is important as it could give more insight into the causes of variability in treatment outcome among individuals with antisocial behavior. Furthermore, results can contribute to improvement in current treatment selection procedures and to the development of alternative treatment options.
During the past 25 years, the literature on the relationship between neurobiological factors and antisocial behavior has accumulated and led to the acceptance of neurobiology as a valuable additional perspective for understanding antisocial behavior (Lahey, McBurnett, Loeber, & Hart, 1995; Moffitt, 1990; Raine, 2002; Raine, 2002a). As a result, this literature which includes structural and functional brain characteristics (Morgan & Lilienfeld, 2000; Ogilvie, Steward, Chan, & Shum, 2011; Raine, 2002) and physiological functioning (e.g., Beauchaine, Hong, & Marsh; 2008; Lorber, 2004) has increased. Furthermore, a growing number of studies aim to increase our understanding of how the interplay between genetic, social, and environmental factors, results in individual differences in brain structure and function associated with differences in the risk of developing problematic antisocial behavior (e.g., Bogdan, Hyde, & Hariri, 2013; Raine, 2008; Thompson et al., 2001; Van Goozen, Fairchild, Snoek, & Harold, 2007). Despite its expanding influence in the field of criminology, neurobiology has been relatively absent in the literature on the efficacy of correctional interventions. In an attempt to bridge neurosciences and correctional intervention research, Vaske, Galyean, and Cullen (2011) proposed that “insights from biosocial criminology could help us unravel why interventions do and do not work” (p. 2). Others have suggested that the impairments in neurobiological systems found in antisocial behavior, may also disrupt the types of cognitive or emotional processing that generally play a crucial role in therapeutic interventions (Fishbein et al., 2006; Van Goozen & Fairchild, 2008).
Investigating neurobiological mechanisms as treatment response moderators may help provide more insight into the question of why some individuals with antisocial behavior respond well to treatment while others do not. This is relevant as there is great variability in effects on criminal recidivism across different correctional interventions, ranging from a 60% reduction to even a small increase in criminal recidivism (Lipsey & Cullen, 2007; McDougall, Perry, Clarbour, Bowles, & Worthy, 2009). As nine million people around the world are held in penal institutions and recidivism rates after release are high (Pew Center of the States, 2011; Walmsley, 2009), understanding the variability of treatment outcome could help increase treatment effectiveness and perhaps reduce recidivism rates.
Cognitive–behavioral therapy (CBT) is an example of a well-accepted correctional treatment option and appears to be one of the most effective interventions for offenders (Andrews & Bonta, 2010; Andrews & Dowden, 2007; Genovés, Morales, & Sánchez-Meca, 2006; Lipsey & Cullen, 2007; Pearson, Lipton, Cleland, & Yee, 2002). It was developed in the 1980s, a time when the psychological and sociological perspectives on risk factors and treatment of antisocial behavior were dominant (e.g., Andrews, Kiessling, Robinson, & Mickus, 1986; Kazdin, 1987; Stermac, 1986). CBT particularly aims to ameliorate dysfunctional thinking processes by focusing on the improvement of specific cognitive skills such as problem solving, moral reasoning, and self-control (McDougall et al., 2009; Sadlier, 2010;Vaske et al., 2011). The effect size of CBT varies between different meta-analyses from less than 10% up to almost a 50% reduction of criminal recidivism (Lipsey & Cullen, 2007; Lipsey, Landenberger, & Wilson, 2007; McDougall et al., 2009). Several reasons have been suggested for this variability in outcome, such as treatment integrity and program setting, and offender’s individual characteristics, like age, prior offense history, drug abuse, and different individual needs (Lipsey & Cullen, 2007; Lipsey et al., 2007; Serin & Kennedy, 1997; Sterling-Turner, Watson, & Moore, 2002). Nevertheless, no consensus has been reached nor have the sources of variability in treatment outcome been addressed adequately (Lipsey & Cullen, 2007).
In this review, the predictive value of neurobiological factors in relation to treatment outcome among individuals with antisocial behavior will be examined to gain more insight into the moderating factors of CBT outcome. Before the results are described, the most relevant neurobiological deficits associated with antisocial behavior will be briefly addressed. For an overview of biological features associated with antisocial behavior see Wilson and Scarpa (2012).
Neurobiological Factors Associated With Antisocial Behavior
Physiological Factors
According to the low arousal theory antisocial behavior is related to low levels of physiological arousal. One of the most replicated finding, with regard to this theory is the high correlation between low resting heart rate and antisocial behavior. It has been suggested that low resting heart rate indicates a lack of fear and a reduced likelihood of experiencing guilt or shame in response to a criminal act, which is assumed to also reduce the effect of the negative consequences antisocial behavior can have (e.g., Armstrong & Boutwell, 2012; Gatzke-Kopp, Raine, Loeber, Stouthamer-Loeber, & Steinhauer, 2002; Gower & Crick, 2011; Lorber, 2004; Ortiz & Raine, 2004; Raine, 1993). Although this relationship is often replicated, some studies did not confirm the negative relationship between resting heart rate and aggressive behavior (Calkins & Dedmon, 2000; Scarpa, Haden, & Tanaka, 2010; Van Hulle, Corley, Zahn-Waxler, Kagan, & Hewitt, 2000). Low levels of arousal are also measurable at the endocrinological level. One of the most studied hormones in relation to antisocial behavior is cortisol. Mixed results have been found with regard to cortisol levels and antisocial behavior, but one consistent finding is a negative relationship between cortisol reactivity to stressors and severity of antisocial behavior (Lahey et al., 1995; McBurnett, Lahey, Rathouz, & Loeber, 2000; Van Goozen, 2005; Van Goozen et al., 2007).
Another physiological mechanism associated with antisocial behavior is heart rate variability (HRV). Different studies related HRV positively to, among other processes, empathy (Fabes, Eisenberg, & Eisenbud, 1993), emotion regulation (Porges, 2007), and high self-control (Fabes & Eisenberg, 1997). It has been suggested that children with conduct disorder have low HRV levels (Mezzacappa et al., 1996; Pine et al., 1996). Scarpa et al. (2010) investigated the relationship between HRV levels and forms of aggression in children and found that reactive aggression was associated with low HRV and proactive aggression was associated with high HRV.
Neuropsychological Factors
Research on neurobiological factors and antisocial behavior has also focused on the frontal lobes of the brain. Structural and functional abnormalities in the frontal lobes of individuals with antisocial behavior have been indicated by a reduction in glucose, metabolism, cerebral blood flow, and gray matter volume (Raine, 2002). Damage to the prefrontal cortex could predispose to antisocial behavior because the prefrontal cortex is involved in monitoring, for example, cognitive and emotional processes (Raine, 1997). According to different reviews and meta-analyses antisocial behavior is associated with impairments in these processes, such as planning, problem solving, impulsivity, and verbal fluency (Brower & Price, 2001; Morgan & Lilienfeld, 2000; Ogilvie et al., 2011).
In total, knowledge about the neurobiological features associated with antisocial behavior is increasing rapidly. It would be interesting to investigate the added value of the neurobiological perspective within the current psychosocial model of treating antisocial behavior. This will be done by reviewing the existing literature on the predictive value of neurobiological factors with regard to treatment outcome among individuals with antisocial behavior.
Method
To review the literature on the relation between neurobiological factors and CBT outcome among individuals with antisocial behavior, a search strategy was formulated including the following main keywords, criteria, and relevant search terms;
Population; antisocial populations. No age restriction was set but adults (> 18 years), adolescents (12-17 years), and children (1-11) were distinguished.
Antisocial, aggression, violence, antisocial personality disorder, oppositional defiant disorder, conduct disorder, disruptive behavior disorder, impulsive, psychopath, offender, criminal, inmate, delinquent, prisoner, behavior problems.
2. Treatment; CBT and related behavioral intervention forms.
CBT, psychotherapy, cognitive therapy, behavioral therapy, parental therapy, multidisciplinary treatment, psychosocial intervention, family therapy, attachment-based intervention, treatment outcome.
3. Neurobiological factors; neuropsychological and/or physiological factors.
Executive function, heart rate, arousal, neurobiology, neuropsychology, hypothalamic–pituitary–adrenal (HPA) axis, neuroendocrine activity, physiological regulation, neural system, testosterone, cortisol, alpha amylase, oxytocin, skin conductance, nervous system, prefrontal cortex, amygdala.
Specific electronic databases were used for the literature search (e.g., PsycINFO, PubMed, Web of Science, Google Scholar), and MeSH options were activated to facilitate the main keywords. Related records, references, and citations were scrutinized for studies that might have been missed in the search, such as unpublished studies. In total, 10 relevant studies were found (Table 1).
Selected Studies on Neurobiological Predictors of Treatment Outcome Among Individuals With Antisocial Behavior.
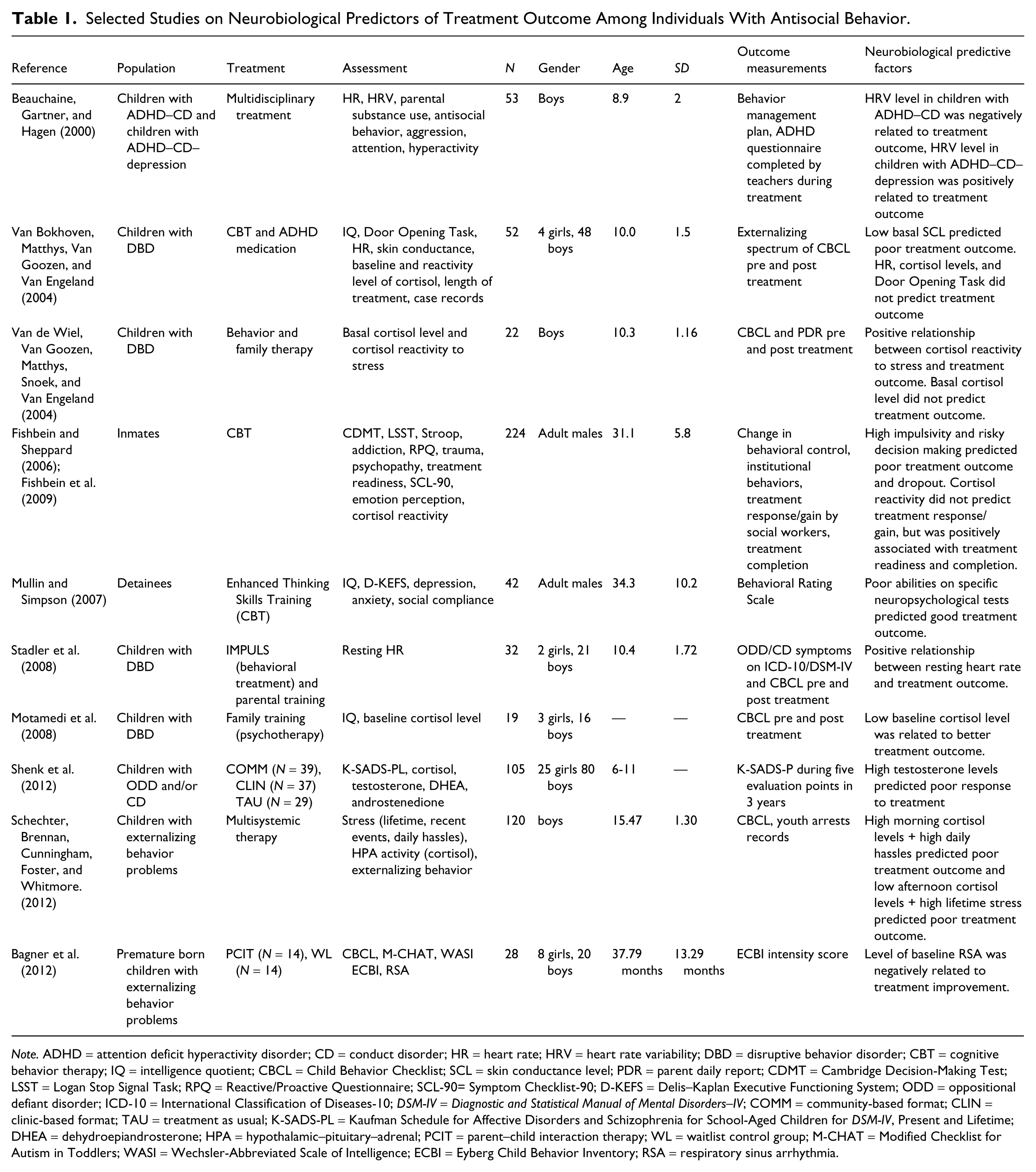
Note. ADHD = attention deficit hyperactivity disorder; CD = conduct disorder; HR = heart rate; HRV = heart rate variability; DBD = disruptive behavior disorder; CBT = cognitive behavior therapy; IQ = intelligence quotient; CBCL = Child Behavior Checklist; SCL = skin conductance level; PDR = parent daily report; CDMT = Cambridge Decision-Making Test; LSST = Logan Stop Signal Task; RPQ = Reactive/Proactive Questionnaire; SCL-90= Symptom Checklist-90; D-KEFS = Delis–Kaplan Executive Functioning System; ODD = oppositional defiant disorder; ICD-10 = International Classification of Diseases-10; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders–IV; COMM = community-based format; CLIN = clinic-based format; TAU = treatment as usual; K-SADS-PL = Kaufman Schedule for Affective Disorders and Schizophrenia for School-Aged Children for DSM-IV, Present and Lifetime; DHEA = dehydroepiandrosterone; HPA = hypothalamic–pituitary–adrenal; PCIT = parent–child interaction therapy; WL = waitlist control group; M-CHAT = Modified Checklist for Autism in Toddlers; WASI = Wechsler-Abbreviated Scale of Intelligence; ECBI = Eyberg Child Behavior Inventory; RSA = respiratory sinus arrhythmia.
Findings
Table 1 shows the different forms of antisocial behavior, type of received treatment, assessment procedures, and the way treatment outcome was evaluated. Of the full assessment battery, only the neurobiological predictive factors are detailed. In general, the results show that certain neurobiological factors are predictive of treatment outcome. With regard to physiological factors, it appears that in general, arousal levels are positively related to treatment outcome. Furthermore, there is an indication that neuropsychological factors are predictive of treatment outcome, but the results are mixed. Next, the results are discussed in more detail.
Physiological Factors
Children with antisocial behavior and less improvement after treatment were characterized pretreatment by lower basal skin conductance (Van Bokhoven, Matthys, Van Goozen, & Van Engeland, 2004), lower resting heart rate (Stadler et al., 2008), higher resting HRV (Bagner et al., 2012; Beauchaine, Gartner, & Hagen, 2000), lower cortisol reactivity to stress (Van de Wiel, Van Goozen, Matthys, Snoek, & Van Engeland, 2004), higher testosterone levels (Shenk et al., 2012) and higher cortisol levels in the morning and lower cortisol levels in the afternoon (Schechter, Brennan, Cunningham, Foster, & Whitmore, 2012). However, children with a favorable treatment outcome were characterized by higher resting heart rate (Stadler et al., 2008), higher cortisol reactivity to stress (Van de Wiel et al., 2004), and lower basal cortisol levels (Motamedi et al., 2008). Furthermore, Fishbein and colleagues (2006, 2009) found a positive relationship between cortisol reactivity and treatment readiness and completion in adults with antisocial behavior.
Neuropsychological Factors
Van Bokhoven et al. (2004) found that sensitivity to punishment and reward as measured by a neuropsychological task (Door Opening Task) could not predict treatment outcome. In contrast, Fishbein and colleagues used different neuropsychological instruments to assess risk-taking behavior, sensitivity to negative consequences, impulsivity, distractibility, cognitive flexibility, and emotion processing. High levels of impulsivity and inability to shift response based on new information were most predictive of low treatment response/progress.
Mullin and Simpson (2007) investigated the predictive value of several neuropsychological factors in relation to treatment outcome among adult prisoners. Positive treatment outcome was represented by a decrease in “negative behavior” (impulsivity, egocentric behavior) and an increase in “positive behavior” (problem solving). Prisoners who showed reduced attentional set shifting and poor planning skills before treatment displayed the largest improvement on negative and positive behaviors after treatment.
Discussion
The examination of the literature on the relation between neurobiological factors and cognitive–behavioral treatment outcome in people with antisocial behavior indicates that research in this area is scarce. Based on the 10 studies included, it appears that specific neurobiological factors are predictive of treatment outcome. The results of studies like those reviewed could potentially be used to make recommendations regarding the improvement of treatment selection procedures and the development of alternative treatment options.
Physiological Factors
With regard to the predictive value of psychophysiological factors, the results suggest that overall lower levels of arousal (lower skin conductance level, lower resting heart rate, higher levels of HRV, lower basal afternoon cortisol levels and lower cortisol reactivity) predict less improvement after treatment, while higher arousal levels (higher resting heart rate, lower resting HRV and higher cortisol reactivity to stress) predict a more favorable treatment outcome. The negative relation between HRV levels and arousal levels may sound contradictory, but high HRV reflects increased parasympathetic activity which results in lower heart rate and lower overall emotional arousal (Berntson, Cacioppo, & Quigley, 1991).
The positive relation between arousal levels and treatment outcome was not confirmed by the study of Motamedi et al. (2008), in which low cortisol levels predicted a favorable treatment outcome. However, they do not provide an interpretation of their findings with regard to the relationship between lower cortisol levels and better treatment response, and their study lacks a comparison with previous studies on arousal level and treatment outcome. Furthermore, Shenk et al. (2012) found a predictive effect of elevated testosterone levels in relation to poor treatment outcome. They proposed that high testosterone levels are associated with higher rates of aggression and that this prevents children from benefiting from treatment. Initially, the results of Shenk et al. (2012) did not seem to fit the association between low arousal levels and poor treatment outcome because testosterone levels are believed to excite physiological activity. However, it has been shown that testosterone and cortisol are involved in social aggression and the interplay between these steroid hormones might regulate this behavior (Montoya, Terburg, Bos, & van Honk, 2012). According to the testosterone/cortisol ratio hypothesis, a high ratio (high testosterone/low cortisol) facilitates aggressive behavior (Terburg, Morgan, & van Honk, 2009; van Honk, Harmon-Jones, Morgan, & Schutter, 2010) and is associated with reduced sensitivity to consequences that involve punishment (van Honk, Schutter, Hermans, & Putman, 2003; van Honk et al., 2004). Therefore, these individuals may be less inclined to learn from their behavior, and it may also make them less responsive to treatment. Although this was not described in the study by Shenk et al. (2012), it could be the case that those children with elevated testosterone levels and poor treatment outcome were also the ones characterized by lowered cortisol levels pretreatment, which may help explain their poor response to the treatment.
Finally, the findings of Schechter et al. (2012) do not precisely fit the positive relation between arousal levels and treatment outcome. The authors suggest that
“males with higher morning cortisol levels who are also experiencing high rates of daily stressors may have worse outcomes for various reasons. They may be particularly hard to engage in therapy, perhaps because their stress response system is “maxed out,” leaving them with few additional resources for therapeutic change.” (p. 920)
This finding suggests that the relationship between arousal level and treatment outcome is probably an inverted-U shape, indicating that extremely high and low levels of arousal interfere with susceptibility to treatment.
A possible mechanism hampering favorable treatment outcome in individuals with deviant arousal levels concerns a suboptimal learning style that prevents them from benefiting from the instructions and tools of CBT. Evidence for this line of thought comes from Mangina and Beuzeron-Mangina (1992). They propose that to learn, one should display an optimal level of arousal. From their study, it appeared that within a group of children and adolescents with learning disabilities, more than 50% was characterized by low levels of arousal while 28% could be classified as “overaroused.” Furthermore, in a number of studies, individuals with antisocial behavior and low arousal levels were found to be characterized by callous, unemotional, or psychopathic traits (Cima, Smeets, & Jelicic, 2008; Hawes, Brennan, & Dadds, 2009). It is known that individuals with high psychopathic traits display several impaired learning processes, such as “error learning,” which indicates an adaptation of behavior in response to negative feedback or error information (Von Borries et al., 2010). Furthermore, individuals with psychopathic traits show reduced “social learning” ability, for example, to observe and learn from positive behavior displayed by others (Blair, Mitchell, & Blair, 2005). Because CBT is based on several forms of social learning, such as observational learning and modeling/role play, individuals with psychopathic traits may profit less from such training components.
Van Goozen et al. (2007) suggest that an adequate reaction of the physiological stress system (e.g., cortisol increase after stress) may be necessary to correctly interpret social information, such as expressions of fear or submission, especially in (negative) emotional situations. In individuals with antisocial behavior and reduced arousal levels, this physiological mechanism could be defective, which may be why they react overaggressively in social conflicts and are less sensitive (cognitively and physiologically) to negative consequences of their behavior. Perhaps this is the mechanism that leads to more persistent antisocial behavior and to unresponsiveness to treatment. Future studies should show whether reinstating reactivity of the physiological stress system, pharmacologically or behaviorally, could lead to a reduction of antisocial behavior.
Finally, emotional bonding with the therapist is an important predictor of treatment outcome (Catty, 2004). The impaired social learning skills of individuals with psychopathic traits may also compromise their ability to form emotional attachments with other people (Blair et al., 2005). The association between neurobiological factors (e.g., low arousal) and psychopathy is a vast area of research. Yet, surprisingly, in this review, no studies were found that investigated the relationship between neurobiological factors and (cognitive–behavioral) treatment outcome among individuals with psychopathy. However, the majority of the studies included in the present review concern individuals with conduct problems, a subset of whom may show callous, unemotional, or psychopathic traits. It is known for instance that severe conduct problems in juveniles are known to be a risk factor for the development of psychopathy (Smith & Hung, 2012). We therefore suggest that more research is needed on the relationship between neurobiological factors and (cognitive–behavioral) treatment outcome among psychopaths as the results of this review indicate that those with the lowest arousal levels may be the most difficult to treat.
Neuropsychological Factors
With regard to the predictive value of neuropsychology in relation to treatment outcome, Fishbein and colleagues found that poor neuropsychological functioning was indicative of poor treatment outcome, while Mullin and Simpson (2007) suggested that people with the lowest scores on the neuropsychological tasks showed the greatest behavior change after treatment. Careful interpretation is required as the two studies differ on essential aspects that hamper direct comparison, such as the neuropsychological tasks, treatment outcome measurements, population, and treatment content. Subsequent studies could provide insight in the direction of the predictive value of neuropsychological factors in relation to the outcome of cognitive–behavioral interventions.
Neurobiology and Treatment of Antisocial Behavior
Although the present model of treating antisocial behavior is dominated by psychological and sociological perspectives, neurobiological knowledge is becoming increasingly accepted as an additional perspective on antisocial behavior and on treating antisocial behavior. For instance, the Reasoning and Rehabilitation (R&R) model, a correctional treatment program, developed an R&R2 program based on research from cognitive neuroscience (Ross & Hilborn, 2008). Despite this example, incorporation of neurobiological knowledge in the clinical context is still underdeveloped. Next, some examples of incorporation of a neurobiological point of view in the treatment of people with antisocial behavior will be considered.
In general, there is no standard procedure available for cognitive–behavioral assessment, but most often, it starts with a structured or semistructured diagnostic interview (Dobson & Dobson, 2009). Assessment in the correctional setting aims to describe offenders’ risk of reoffending, need for treatment, and eligibility to participate in available treatment programs (McDougall et al., 2009). Knowledge of the predictive value of neurobiological factors in relation to treatment outcome could be used to extend and improve selection and indication procedures. In future, this could mean that specific levels of, for example, basal physiological arousal or levels of stress reactivity provide information about one’s likeliness to profit from cognitive–behavioral treatment.
Although the majority of the included studies provided information about specific values of physiological parameters, such as number of heart beats per minute, they did not include a healthy control group to compare the physiological values with. This hampers applicability of the results into practice as it remains unclear whether the measured physiological levels are indeed indicative of deviant arousal levels or appear to be within a “healthy” or “normal” range, but aberrant compared with the sample mean. Future studies could profit from large–scale studies that show the pattern of values of physiological measures. This is necessary to develop more knowledge about what constitutes “normal” or “heightened” or “lowered” values and is especially relevant as different populations with regard to, for example, age and gender show different physiological characteristics. Such knowledge may help develop cut-off scores to categorize, for instance, individuals with “high” and “low” levels of arousal. It may then become possible to add physiological measures to the current “toolbox” of selection instruments.
Furthermore, with the increased knowledge of neurobiological deficits associated with antisocial behavior, neurobiological-based treatment options could serve as alternatives for those who respond poorly to CBT. One example is “neurofeedback” in which patients are instructed to watch a computerized video program in which the content is driven by their own brainwave frequencies. The program only proceeds if sufficient selected brainwave frequencies are reached (Legarda, McMahon, Othmer, & Othmer, 2011). Neurofeedback has successfully helped people with cognitive deficits to increase their concentration and self-control and decrease aggressive and impulsive behavior (Van Outsem, 2011). Another—still experimental—alternative treatment option is repetitive transcranial magnetic stimulation (rTMS) or transcranial direct current stimulation (tDCS) in which specific brain functions can be changed by excitation or inhibition (Nitsche & Paulus; 2001; Rossini & Rossi, 2007). It appears that applying tDCS to the dorsolateral prefrontal cortex in healthy individuals results in reduced risk-taking behavior during specific decision-making processes (Fecteau et al., 2007). Future research is warranted to investigate the therapeutic applicability of tDCS or rTMS in individuals with antisocial behavior.
There are some important limitations to the present study that need to be addressed. As is evident from Table 1, the population categories differ among the various studies with regard to age, behavioral problems, and psychiatric disorders. Furthermore, the sample sizes range from very small studies (N = 19) to studies with a sample size of well over 200 participants. With regard to the treatment forms, studies using cognitive–behavioral treatment and related intervention options were included in this review. Nevertheless, the content of the treatments differs between the included studies. Finally, the included studies use different pretreatment neurobiological measurements and for the assessment of treatment outcome.
The results of this review indicate that specific neurobiological factors affect the outcome of behavioral interventions; however, future research is warranted to understand the interplay between neurobiology and behavioral therapy. As empirical work on this topic is inconclusive and still developing, theoretical models could clarify the relation between neurobiological factors and cognitive–behavioral treatment outcome, and provide guidance for further empirical studies. One such model is formulated by Vaske et al. (2011), who postulate that when behavioral interventions successfully change cognitions and ameliorate skills, these changes would be reflected in changes in brain functioning in regions involved in these skills. It is conceivable then that deficits in specific brain areas central to the intervention could hamper behavioral improvement and reduce the effectiveness of the therapy. In addition, there are upcoming empirically supported models that integrate the roles of genetic, neurobiological, environmental, and social factors in the etiology of antisocial behavior. For instance, the meta-analysis and the integrative model proposed by Van Goozen et al. (2007, p. 153) could guide the study of cognitive–behavioral interventions in several ways. The model incorporates evidence on how familial factors, such as genes and early childhood experiences, act as precursors to the development of disrupted neurobiological and cognitive/emotional functioning characteristic for severe antisocial behavior. This can help identify not only relevant neurobiological (and other) factors that may hamper an individual from profiting from CBT but also factors that may provide opportunities for innovative treatments.
For instance, the influence of genes and early environmental factors on the development of neurobiological factors is increasingly a topic of study (e.g., Beaver, Gibson, DeLisi, Vaughn, & Wright, 2012; Boutwell, Beaver, Barnes, & Vaske, 2012; Thompson et al., 2001). A pioneering study with regard to the moderating effect of genetic factors on behavioral intervention among a group of children with externalizing behavior was conducted by Bakermans-Kranenburg, Van Ijzendoorn, Mesman, Alink, and Juffer (2008). It appeared that in the presence of a specific dopamine gene (DRD4), children’s basal cortisol levels “normalized” after treatment compared with children without the DRD4 gene. This finding suggests that susceptibility to treatment, expressed in neurobiological change, differs depending on one’s genetic make-up. Future research should demonstrate whether the integrative model proposed by Van Goozen et al. (2007) could be transformed into a model in which the influence of familial factors on neurobiological deficits explains the variety in treatment outcome among individuals with antisocial behavior.
In conclusion, the results of this review provide evidence that a neurobiological perspective is promising in increasing comprehension of specific correctional issues, such as the high variety of effect after treatment among offenders. As only 10 studies were found, more empirical research is necessary to gain further insight into the neurobiological sources of treatment outcome variability among offenders, and eventually to develop practical contributions, such as neurobiological-based treatment selection procedures and alternative treatment options.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Netherlands Society of Scientific Research (NWO: Brain and Cognition: Societal Innovation, Grant: 056-21-011), the Netherlands Institute for the Study of Crime and Law Enforcement (NSCR), and Research and Documentation Centre (WODC), Ministry of Security and Justice.