
Abstract
Although it is known that adolescents in secure residential care often show multiple behavior problems, it is largely unknown which dynamic risk factors are associated with their problems. The aim of the present study is to examine dynamic risk factors for 164 Dutch adolescents in secure residential care. Results show that a majority reports multiple risk factors in both an individual and contextual domain but that about a fifth shows relatively few risk factors. Substance abuse and delinquent friends were among the five most prevalent risk factors and predicted the seriousness of the adolescents’ delinquent behavior prior to admission. The four groups that were found by cluster analysis could be distinguished by problem type and seriousness. The findings indicate that treatment for some adolescents should be mainly focused on their individual needs, while other adolescents need intensive, multimodal treatment focusing on both risks in the individual, family, and peer domains.
Serious emotional and behavioral problems, with antisocial and oppositional problems generally being prominent, are often an important reason for the admission of adolescents to secure residential care settings, such as juvenile correctional or detention centers (Boendermaker, 1999; Vreugdenhil, Doreleijers, Vermeiren, Wouters, & Van den Brink, 2004). The problems of young people in these facilities are complex and have often started at an early age, causing youth to often have a long history of care (Boendermaker, 1999). Considering these problems, it is not surprising that secure residential care often has limited results in terms of recidivism (cf. Abrams, 2006).
Research findings point to the importance of accounting for the specific problems and needs that young people in (secure) residential care have in terms of the “criminogenic needs,” “responsivity,” and “treatment modality” principles of effective programs for reducing recidivism. These principles imply that interventions should be focused on those client factors that constitute the basis of the problem behavior, that there should be an appropriate matching between styles of workers and styles of clients, and that interventions should be aimed at different aspects of the clients’ problems (multimodal) and therefore apply different methods, respectively (MacGuire, 1999). However, research on residential care programs indicates that often a similar set of services is provided to all young people, regardless of their problems (Libby, Coen, Price, Silverman, & Orton, 2005). Moreover, some studies show that adolescents in secure residential care often report that they receive too little attention to their individual problems during care (Boendermaker, 1999; Harder, Knorth, & Kalverboer, 2014).
A starting point for secure residential treatment programs to improve treatment outcomes is to focus on individual treatment by dynamic (changeable) risk and protective factors, because these factors can be influenced by treatment (DeMatteo & Marczyk, 2005). Static (non-changeable) factors however, such as demographic characteristics and a history of delinquency, cannot be influenced by intervention (Van der Laan & Blom, 2006a). Risk and protective factors can explain the development and persistence of behavior problem by having a risk-increasing or protective function in the domain of the child, his or her parenting system, and/or the social context (Dodge & Pettit, 2003). Interventions that have the purpose to reduce the problem behavior of young people, such as secure residential care, should aim at relevant dynamic risk and protective factors (Lipsey & Derzon, 1998).
The eight most relevant risk factors for (the persistence of) delinquent behavior, called the “central eight,” mainly include dynamic risk factors, although the most important one is static and refers to having a history of antisocial behavior (Andrews, Bonta, & Wormith, 2006). The dynamic factors of having an antisocial personality pattern (e.g., weak self-control, aggressiveness) and antisocial cognition (e.g., beliefs supportive of crime, cognitive emotional state of anger, resentment, and defiance) are considered to be the second and third most important risk factors. Three other important dynamic risk factors at the individual domain are a poor performance at school and/or work, poor involvement in anticriminal leisure activities, and substance abuse. Important risk factors in the contextual domain are close associations with criminal others and poor nurturance and/or caring, and monitoring and/or supervision by parents or family (Andrews et al., 2006).
A dynamic factor which seems to be part of the antisocial cognition risk factor described by Andrews et al. (2006) and might play a crucial role in the process of secure residential youth care is compliance with or motivation for treatment (cf. Van der Helm, Wissink, De Jongh, & Stams, 2013). Adolescents in secure residential care are often unaware of their problems, show oppositional problems, and a poor motivation for change (Englebrecht, Peterson, Scherer, & Naccarato, 2008; Van Binsbergen, 2003). Also substance abuse is a relevant dynamic factor, because it is a quite common problem for these adolescents (Feldstein & Ginsburg, 2006; Vreugdenhil et al., 2004). A poor performance at school and/or work, poor competence skills of the adolescents (Slot & Spanjaard, 1999), and involvement in antisocial leisure activities are also relevant risk factors for adolescents in secure residential care (Boendermaker, 1999; Foley, 2001).
In the contextual domain, both risk factors mentioned by Andrews et al. (2006) are relevant for adolescents in secure residential care: negative family characteristics in terms of poor parenting styles and supervision (Boendermaker, 1999; Chambers, Power, Loucks, & Swanson, 2001) and the presence of delinquent friends (Fergusson, Vitaro, Wanner, & Brendgen, 2007; Van der Ploeg & Scholte, 2003). For example, Hoeve and colleagues (2008) found that neglectful parenting was more frequent in more serious delinquents than in non- or minor delinquents, suggesting that parenting styles differentiate non- or minor delinquents from more serious delinquents. Furthermore, adolescents who are more deeply embedded in deviant peer relations seem to be more resistant to developing a relationship with staff during secure residential care (Florsheim, Shotorbani, Guest-Warnick, Barratt, & Hwang, 2000).
To meet the needs of the young people, secure residential care programs will have to clearly identify the characteristics of the adolescents. Specifically, they will need to identify adolescent’s problems and strengths, to specify exactly what their needs and capabilities are and how they can best be addressed. Although many studies have been conducted on risk and protective factors for delinquent behavior, few studies specifically focused on young people in secure residential care. Studies that have been conducted on the specific problems of adolescents in secure residential care, mainly show that these youth often show behavioral problems, multiple problems, and co-morbidity in psychopathology (Hussey, Drinkard, Falletta, & Flannery, 2008; Vreugdenhil et al., 2004). There are, however, no previously conducted studies that specifically and simultaneously examined different dynamic risk factors associated with antisocial behavior of adolescents in secure residential care. It is unknown whether these adolescents show specific combinations of risk factors that may serve as an important guideline for secure residential treatment. The central aim of this article is, therefore, to examine dynamic risk factors in a sample of adolescents in secure residential care. Specifically, we address the following research questions:
Considering the findings in previous studies, we expect that most of the adolescents show multiple risk factors in both the individual and contextual domains. Our second hypothesis is that adolescents with a high accumulation of risk factors will show more problematic behavior than adolescents with few risk factors. Third, we expect that there are subgroups of adolescents showing specific combinations of risk factors.
Method
The present study is part of a research project which focuses on adolescents staying in a secure residential center that is located in the north of the Netherlands. Adolescents from 12 to 23 years old are placed in the center by either a civil or penal measure. The principal reason for admission is either intolerably disruptive and antisocial behavior or behavior presenting a danger to the young person himself or herself or to the general public.
The social competency model is considered to be the primary, underlying methodology of the treatment in the secure center (Slot & Spanjaard, 1999). An important component of treatment in the center are the activities at the (mostly secured) residential group. Besides the residential group, the adolescents spent much time in special education classes of 8 to 10 adolescents at the internal school, where they receive training by teachers. Special education in this context means that the adolescents receive individualized education programs during their stay.
The total research project had a longitudinal design with measurements at admission, 8 weeks after admission, at departure, and 1 year after departure. For the present study, information from the measurement of admission was used. A group of 194 adolescents that entered the center between September 1, 2007, and June 1, 2008, and stayed for a minimum period of 8 weeks was eligible for inclusion in the present study.
Procedure
The adolescents were informed about the research project by the project leader shortly after admission during a private conversation and by an information flyer. To promote their participation in the project, it was emphasized that participation in the project was confidential and that it was a common part of their stay. Once an adolescent agreed to participate, the project leader informed one of the interviewers so that he or she could contact the youth for the interviews. Interviews were conducted by students of the University of Groningen. To guarantee a correct administration, the students received training before conducting the interviews. Directly after the interview, the adolescents received questionnaires to complete in their own time. A group of 164 adolescents (85%) was interviewed on average 4.4 weeks after their admission. Of the 30 adolescents who did not participate, 22 refused to participate and 8 adolescents did not participate due to practical problems (e.g., short stay in the center). Of the interviewed adolescents, 101 adolescents (62%) also filled in questionnaires on average 2.9 weeks after their admission.
For each adolescent, we contacted the coach, who is one of the group care workers of the residential group to whom each adolescent is assigned. This assignment to group care workers is unsystematic and mainly based on the order of placement. The coach is responsible for observing the adolescents and involved in the adolescents’ individual treatment planning. The coaches only filled in questionnaires. They were approached 6 to 8 weeks after the adolescent’s admission by email with a short explication about its purpose and the questionnaires in an attachment, which they could fill in digitally or manually and reply by email. Before approaching coaches individually, they were also informed about the research project by the project leader during several group meetings. For the 164 adolescents who were interviewed at admission, 95 coaches (58%) responded.
Instruments
Motivation for treatment
To evaluate the adolescents’ problem perception and motivation for treatment shortly after admission, the Motivation for Treatment questionnaire (MTQ; Van Binsbergen, 2003) was completed by the adolescents. Aim of the instrument is to assess the first three stages of treatment motivation (i.e., precontemplation, contemplation, and preparation) that are distinguished by Prochaska and DiClemente (1984). The original version of the MTQ consisted of 81 items, but for the present study we only used a short 17-item version of the questionnaire based on outcomes of factor analysis conducted by Van Binsbergen (2003). The items of the MTQ (e.g., “I am here just because others think that it is necessary”) contain a 3-point rating scale ranging from 0 (not true) to 2 (true). For the present study, we calculated a total motivation score by weighing the scores on the stages of motivation as 1, 2, and 3, respectively, resulting in a range of scores from 0 (not motivated) to 12 (motivated). We used the total median score of 6.5 as a cutoff score to distinguish between adolescents being motivated (≥6.5) or not motivated (<6.5) for treatment. The reliability of the MTQ for the present sample was satisfactory (α = .59).
Substance abuse and school performance
The Scientific Research and Documentation Centre (SRDC) interview (Van der Laan & Blom, 2006b) was used to assess self-reported substance use and school performance of the adolescents prior to admission. Substance abuse was measured using several items of the SRDC interview concerning the frequency of alcohol, soft drugs, and hard drugs use during the last 12 months (e.g., “On how many of the 4 weekdays do you mostly drink alcohol?”). Adolescents were classified as having substance abuse problems if they reported to use alcohol or soft drugs for at least 4 days a week, or if they used hard drugs for more than 2 days a week. School performance was assessed by one self-report item of the SRDC (i.e., “If you think about your latest school report, how would you generally describe your academic achievements?”) with a 5-point rating scale ranging from 1 (very unsatisfactory) to 5 (very satisfactory). For the present study, we applied the median score 3 as a cutoff score to distinguish between adolescents with a good (≥3) versus a poor performance (<3).
Leisure activities
We used one item of the Dutch version of the Lancashire Quality of Life Profile (LQoLP; Van Nieuwenhuizen, Schene, & Koeter, 1998) to assess the main daily activities of the adolescents prior to admission. The Quality of Life Profile was part of the interview conducted with the adolescents at admission. The used item (i.e., “What was your main daily activity before your admission to the center?”) contained several answering categories of activities, ranging from school/work to unstructured activities. For the present study, we calculated a dichotomous variable that distinguishes between unstructured activities, such as going out with friends and dealing drugs, and structured activities, such as school and work.
Competence skills
For the evaluation of adolescent’s competencies, the Adolescents’ Tasks and Skills Questionnaire (TASQ; Van der Knaap, 2003) was completed by the coaches minimally 6 weeks after the adolescent’s admission. Aim of the instrument is to assess the degree to which a youngster’s functioning is adaptive or effective in relation to salient developmental tasks (i.e., normative demands and expectations), as judged by a group care worker. The TASQ consists of 137 items (e.g., “If she or he is dared or teased, the young person knows how to make the right choice between answering back or ignoring”) concerning the adolescents’ skills which contain a 5-point Likert-type scale ranging from 1 (totally not applicable) to 5 (totally applicable). We used a mean total competence score. A mean total score that is equal or higher than the median of 3 is perceived as sufficient competency. The internal consistency of the TASQ for the present sample was good (α = .71).
Family functioning
We measured the supervision behavior of parents regarding the adolescents’ leisure time activities prior to admission by using the SRDC interview, which was conducted with the adolescents. We only used the mothers’ scores, because mothers were more often seen as the primary caregiver by the adolescents. Sum scores of the SRDC interview subscales parental control (5 items, ranging from 1 = never to 5 = almost always), and passive monitoring (5 items, ranging from 1 = nothing to 3 = much) were used to measure the mothers’ supervision behavior. Parental control refers to the extent in which mothers are informed about the leisure time activities of the adolescents (e.g., “Do you need permission from your mother to stay away until late in the evening during weekdays?”). Passive monitoring is the extent to which mothers are informed about the daily activities of the adolescents (e.g., “What does your mother know about: who your friends are?”). These parenting scales were sufficiently reliable: α = .80 and α = .70, respectively. Median scores of 15 and 10 were applied as cutoff scores to distinguish between a low and high supervision rate in terms of control and monitoring, respectively.
Contact with mothers was assessed in terms of the parental rearing styles by using the Dutch version of the Egna Minnen Beträffende Uppfostran (EMBU-C) questionnaire which was completed by the adolescents (Markus, Lindhout, Boer, Hoogendijk, & Arrindell, 2003). The EMBU consists of 52 items with a 4-point Likert-type scale ranging from 1 (never) to 4 (always). For the present study, we used the subscales Emotional Warmth (19 items) and Rejection (17 items). Emotional warmth reflects perceived parental warmth in interaction with their child (e.g., “Do you have the feeling that your mother loves you?”) and rejection refers to perceived parental rejection (e.g., “Does your mother also punish you for minor things?”). An emotional warmth score of ≥ 57 and a rejection score of ≤ 34 are perceived as sufficient, because minimum scores of 3 and maximum scores of 2 for each item were considered to be necessary for a sufficient score on these scales, respectively. These scales showed good internal consistency (α = .92-.96).
Delinquency of friends
The amount of delinquent friends reported by the young people was assessed by a subscale of the SRDC interview concerning the delinquent behavior of friends during the period before admission, which contains six items (e.g., “Do you have friends who have committed a burglary in the last 12 months?”) ranging from 0 (none delinquent) to 3 (all delinquent) and showed good reliability (α = .84). We calculated the scores on the subscale into one delinquent friends score ranging from 0 (no delinquent friend) to a maximum score of 18 (only delinquent friends). Because a score of 1 for each item indicated that the adolescents had some friends that showed delinquent behavior, we applied a cutoff score of 6 to distinguish between adolescents with relatively few (<6) and many (≥6) delinquent friends.
Delinquent behavior
The SRDC interview was also used to assess self-reported delinquency of the adolescents. We used the Delinquent Behavior scale (36 items; for example, “Have you ever sold soft drugs such as weed or hash?”) which was applied as a questionnaire. This scale showed good reliability (α = .88). The frequency and seriousness of self-reported delinquency over the last 12 months were combined into one delinquency score on the basis of the frequency and seriousness of the offences as is applied by Van der Laan and Blom (2006a).
Participants
Main background data, based on treatment document information, for the group of 164 adolescents that participated in the interview at admission are shown in Table 1.
Sample Characteristics of the Participating Adolescents at Admission.

n = 157.
n = 160.
n = 163.
n = 154.
To examine possible attrition bias, we compared the response groups with the non-response groups of the adolescents’ (n = 101) and group care workers’ (n = 95) questionnaires on background characteristics (Table 1) and adolescents’ self-reported delinquency. Adolescents for whom there was information of group care workers were significantly more often placed in the center by a civil measure than adolescents in the non-response group, χ2(1) = 11.5, p = .001. This response group was also significantly more likely to have shown delinquent behavior prior to admission than the non-response group, χ2(1) = 5.3, p = .028. Overall, these results indicate no attrition bias, but that the group with information of group care workers might be somewhat more delinquent than the group for which this information is missing.
For a subgroup of 57 adolescents, there was information on all the risk factors. To examine possible attrition bias regarding this information, we conducted the same analyses as described above. Adolescents in this response group were significantly more often placed by a civil measure, χ2(1) = 7.3, p = .009, and less likely to have a mother with poor passive monitoring behavior, χ2(1) = 7.1, p = .009, than adolescents in the non-response group. These results indicate that the subgroup of 57 adolescents might be somewhat less problematic than the group for which this information is missing.
Data Analysis
To test for significant associations between risk factors and self-reported delinquency, we conducted univariate analyses by using Mann–Whitney tests and the Spearman’s correlation coefficient. Background characteristics and risk factors that were significantly associated with delinquency at a threshold of α ≤ .05, were included in a hierarchical multiple regression analysis to explain which predictors account for delinquency and to look for interaction effects between risk factors (Field, 2009).
Specific subgroups within the sample regarding combinations of risk factors were identified by cluster analysis (Norušis, 2010). We first included both the original, standardized continuous and categorical risk variables in the analysis by using the two-step procedure, but this resulted in a two-cluster solution with a poor cluster quality. Therefore, we dichotomously rated all risk factors and conducted hierarchical clustering by using the Ward’s method. By applying visual methods (e.g., inspection of the dendrogram, icicle plot and agglomeration schedule), we concluded that 4, 5, 9 or 15 clusters could be optimal solutions. However, because the 9 and 15 cluster models resulted in very small subgroups (n < 5), we decided to apply confirmatory analysis on the 4 and 5 cluster model by conducting K-means clustering and to compare the resulting cluster solutions to that from the hierarchical cluster analysis (Mandara, 2003). These comparisons resulted in a mean kappa of .08 (95% confidence interval [CIκ] = [−0.06, 0.22]) for the 4 cluster and −.18 (95% CIκ = [−0.25, −0.11]) for the 5 cluster model. Because we found somewhat better agreement for the 4 cluster model than the 5 cluster model (Viera & Garrett, 2005), we chose the 4 cluster model as the most optimal.
To determine whether the four cluster groups significantly differed in terms of risk factors, problems, and background characteristics, we applied Kruskal–Wallis tests and chi-square tests. Because of the small sample size, we applied α ≤ .10 as a threshold for significance. We used a Bonferroni correction (α ≤ .017) in post hoc analyses for the groups.
Results
Prevalence of Risk Factors
The prevalence of the different risk factors is shown in Table 2.
Prevalence of Risk Factors for Adolescents at the Moment of Admission.

Note. Risk factors are ordered by prevalence and domain.
The total group of 164 adolescents showed a mean number of 3.3 risk factors (SD = 1.82), ranging from 0 to 8, with 1.8 individual (SD = 1.15) and 1.7 contextual (SD = 1.17) risk factors on average. Most of the adolescents (70%) showed a combination of risk factors in both the individual and contextual domains.
Of all the 164 adolescents who were interviewed at admission, there was information on all the risk factors for a group of 57 adolescents (35%). These adolescents showed 3.7 out of 10 risk factors on average (SD = 1.93), ranging from 0 to 8 risk factors, including 2.1 (SD = 1.24) individual and 1.6 contextual (SD = 1.12) risk factors on average. For 72% of these 57 adolescents, there was a combination of risk factors in the individual and contextual domains. Risk factors in the individual domain of the child were slightly more prevalent (88%) than risk factors in the contextual domain (81%). This subgroup had the same order of prevalence of the separate risk factors as is shown in Table 2.
Risk Factors and Delinquency
The number of risk factors showed a significant positive association with the seriousness and frequency of delinquent behavior in the last 12 months prior to admission, rs = .34, p = .000, which can be considered as a medium to large effect. So, the higher the number of risk factors, the higher the chance for adolescents to show serious delinquent behavior.
The results for the associations between separate risk factors and delinquency based on the available information for the 164 interviewed adolescents are shown in Table 3.
Associations Between Risk Factors and Self-Reported Delinquency at Admission.
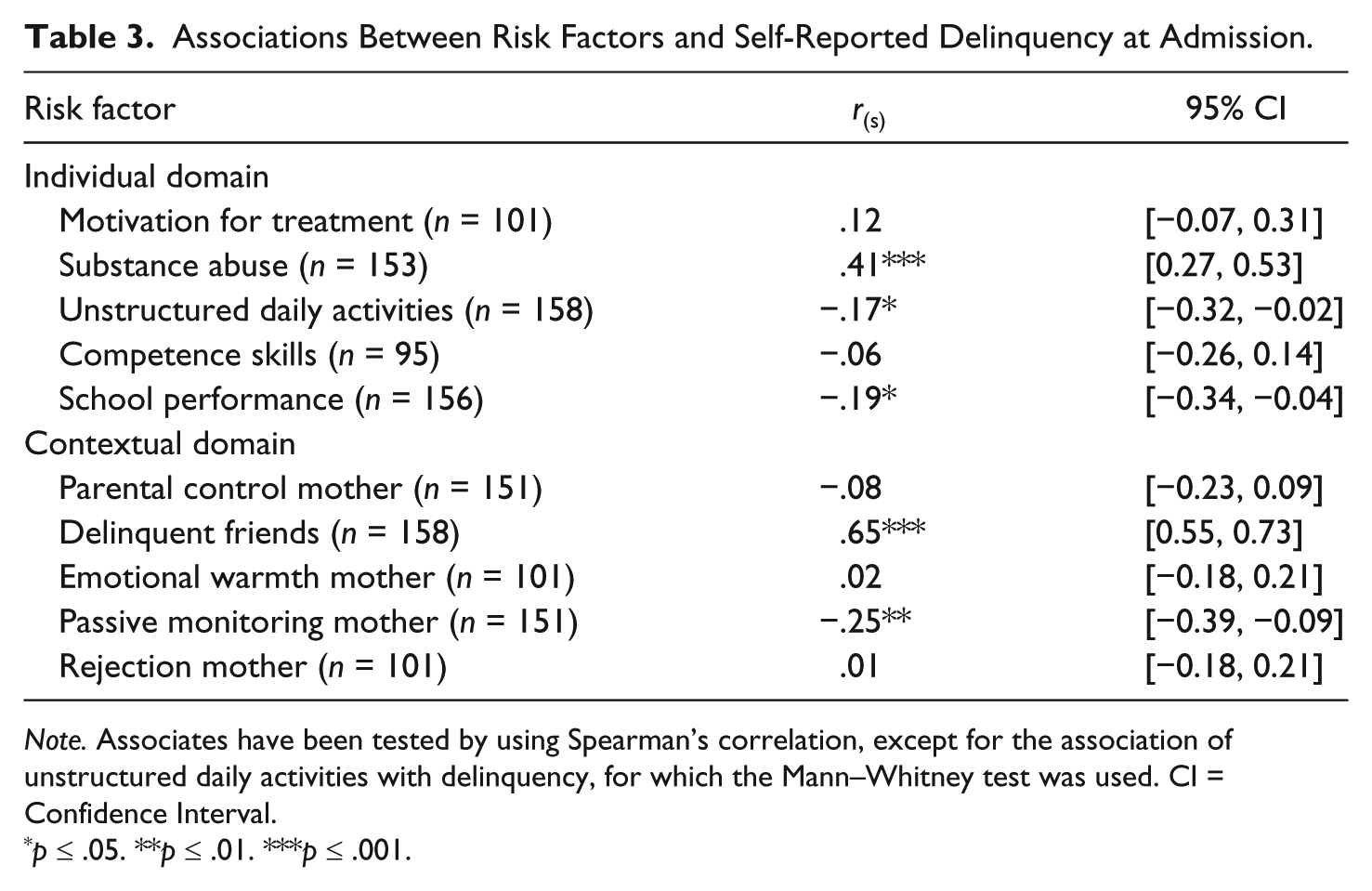
Note. Associates have been tested by using Spearman’s correlation, except for the association of unstructured daily activities with delinquency, for which the Mann–Whitney test was used. CI = Confidence Interval.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Within the individual domain, a higher delinquency score was most strongly associated with substance abuse (medium to large effect), followed by poor school performance, and unstructured daily activities (both a small to medium effect). Having delinquent friends (large effect) and poor passive monitoring behavior of the mother (small to medium effect) were associated with a higher delinquency score in the contextual domain.
Besides these risk factors, also adolescents being male, U = 2,201.5, z = −2.61, r = .20, of Dutch origin, U = 2,539.0, z = −1.99, r = .16, that were placed by a penal measure, U = 2,095.0, z = −2.03, r = .16, and showed externalizing behavior problems prior to admission, U = 1,172.0, z = −2.33, r = .18, were significantly (p ≤ .05) more likely to show higher delinquency scores. Therefore, these background characteristics were initially included in the regression analysis, but excluded in the final model (see Table 4) because these variables did not significantly contribute to the prediction of the outcome.
Hierarchical Regression Model for Risk Factors and Delinquent Behavior (n = 151).

Note. SE = standard error; CI = confidence interval. R2 = .37, p ≤ .001.
p ≤ .01. ***p ≤ .001.
The model shows that both having delinquent friends and substance abuse significantly predicted 37% of the variance in the delinquency score. The confidence interval for delinquent friends is wider than that for substance abuse, which indicates that the parameter for delinquent friends is less representative for the true population values than substance abuse. Although the model appears to be accurate for the sample, there are indications that the model might have violated the assumption of homoscedasticity. This means that the residuals at each level of the predictors have a different variance, implicating heterogeneity of variance (Field, 2009). Therefore, the regression model from the sample is probably not the same as the population model, implicating that these results cannot be generalized beyond this sample.
Subgroups Based on Combinations of Risk Factors
The four groups that were found by the hierarchical cluster analysis based on a combination of all 10 risk factors for a subgroup of 57 adolescents are shown in Table 5.
Prevalence of Risk Factors and Seriousness of Delinquency for Adolescents in Four Subgroups.
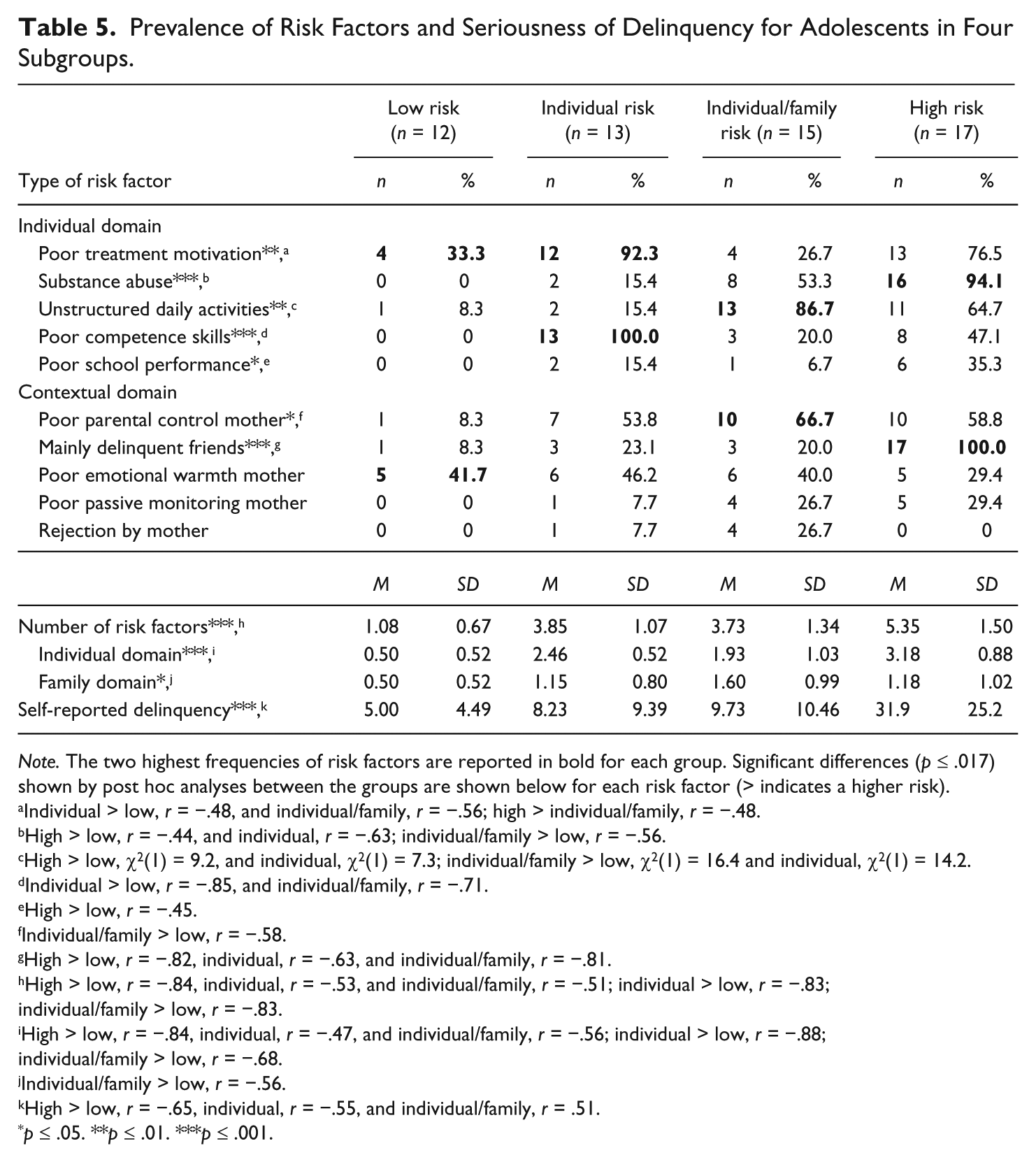
Note. The two highest frequencies of risk factors are reported in bold for each group. Significant differences (p ≤ .017) shown by post hoc analyses between the groups are shown below for each risk factor (> indicates a higher risk).
Individual > low, r = −.48, and individual/family, r = −.56; high > individual/family, r = −.48.
High > low, r = −.44, and individual, r = −.63; individual/family > low, r = −.56.
High > low, χ2(1) = 9.2, and individual, χ2(1) = 7.3; individual/family > low, χ2(1) = 16.4 and individual, χ2(1) = 14.2.
Individual > low, r = −.85, and individual/family, r = −.71.
High > low, r = −.45.
Individual/family > low, r = −.58.
High > low, r = −.82, individual, r = −.63, and individual/family, r = −.81.
High > low, r = −.84, individual, r = −.53, and individual/family, r = −.51; individual > low, r = −.83; individual/family > low, r = −.83.
High > low, r = −.84, individual, r = −.47, and individual/family, r = −.56; individual > low, r = −.88; individual/family > low, r = −.68.
Individual/family > low, r = −.56.
High > low, r = −.65, individual, r = −.55, and individual/family, r = .51.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
A comparison of all the groups on background characteristics (see Table 1) only indicated a difference in externalizing behavior problems prior to admission, Fisher’s p = .064, but post hoc analyses did not show significant differences between the four groups. The groups showed significant differences on different types of risk factors, the number of risk factors and self-reported delinquency (see Table 5).
The first group of 12 adolescents (21%) could be described as the “low risk” group, with significantly less risk factors than the other three groups. The second group of 13 adolescents (23%) was mainly characterized by individual problems (i.e., a poor motivation for treatment and competence skills) and therefore called the “individual risk” group. The 15 adolescents (26%) in the third group showed a relatively high mean of risk factors in both the individual and family domain and, therefore, described as the “individual and family risks” group. The fourth group of 17 adolescents (30%) was the most problematic, because this group showed significantly more risk factors and delinquent behavior than the three other groups.
Discussion
Most of the adolescents in the sample of the present study showed risk factors in both the individual and contextual domains, which corresponds to our expectations. The most prevalent risk factor was a poor motivation for treatment, followed by substance abuse by the adolescents and poor parental control by the adolescents’ mothers. The findings show that these adolescents are often unaware or under aware of their problems and not intending to take action in the foreseeable future. This suggests, in correspondence to other studies, that secure residential care centers should get insight into and change adolescents’ motivation for treatment level (Englebrecht et al., 2008; Orlando, Chan, & Morral, 2003; Van der Helm et al., 2013). Moreover, other research suggests that adolescents themselves consider their own motivation for behavior change as a key element of the change process in secure residential treatment (Harder et al., 2014; Henriksen, Degner, & Oscarsson, 2008).
The finding that substance abuse is one of the three most prevalent risk factors for the adolescents in the present study, and the finding that it is an important predictor for delinquent behavior, corresponds to findings in other studies (e.g., Feldstein & Ginsburg, 2006; Hussey et al., 2008; Orlando et al., 2003). As research also suggests that substance problems are associated with higher treatment costs (Hussey et al., 2008), an intervention such as Motivational Interviewing (MI) seems to be very relevant and important for adolescents in secure residential care (Feldstein & Ginsburg, 2006; Underwood, Barretti, Storms, & Safonte-Strumolo, 2004). However, still surprisingly little attention has been paid to MI in this field (Feldstein & Ginsburg, 2006; Stein et al., 2011). This is remarkable, as MI has shown to be successful for clients with comparable problems (Jensen et al., 2011).
Another finding that is consistent with our expectations is that adolescents with a high number of risk factors showed more (serious) delinquent behavior prior to their admission to secure residential care than adolescents showing few risk factors. This corresponds to findings of the many studies that have been carried out on this topic (e.g., Farrington, 1997; Van der Laan & Blom, 2006a).
The most important predictors of delinquent behavior were the risk factors “delinquent friends” and “substance abuse” before admission to secure residential care. Although poor passive monitoring by mother, poor school performance, and unstructured daily activities were also associated with delinquency, these variables did not significantly contribute to the prediction of delinquent behavior. So, instead of a “central eight” (Andrews et al., 2006), we found a “substance and friends duo” of risk factors in the present sample of Dutch adolescents in secure residential care. These results suggest that more and less problematic adolescents mainly differ on having delinquent friends and showing substance abuse. That these adolescents mainly show risks with regard to delinquent friends corresponds with the finding in other studies that peers are important during adolescence (Loeber, Slot, & Stouthamer-Loeber, 2006), including the peers’ influence on delinquency and substance use (Aseltine, 1995). The finding that substance abuse is an important predictor of delinquent behavior emphasizes the usefulness of MI as a treatment method for these adolescents.
Although some negative family characteristics, especially mothers’ poor parental control, were highly prevalent in our sample as was expected from findings in other studies (Boendermaker, 1999; Griffith et al., 2009), only passive monitoring by mother was significantly associated with delinquency. It might be that family characteristics mainly have an indirect impact on delinquent behavior rather than a direct impact, for example, by reinforcing poor school performance and the adolescent’s involvement in antisocial leisure activities outside the family’s home (cf. Van der Heiden-Attema & Bol, 2000). This indirect influence might especially be true for adolescents in secure residential care, because this group often consists of late adolescents and might therefore be less exposed to their parents than early adolescents (cf. Loeber et al., 2006). Other studies suggest, however, that the behavior of parents and the adolescent–parent relationship is very important in association with delinquent behavior, also during late adolescence (Hair, Moore, Garrett, Ling, & Cleveland, 2008; Lahey, Van Hulle, D’Onofrio, Rodgers, & Waldman, 2008).
The results of the present study showed in correspondence with our expectation that the group of adolescents for whom there was information on all risk factors could be divided into subgroups. Somewhat more than a fifth of the adolescents could be attributed to a “low risk” group, which showed few risk factors in comparison with the other three groups. The “individual risk” group that was found, which also included somewhat more than a fifth of the adolescents, was mainly characterized by individual problems. It might be that this low risk and individual risk group mainly consist of so-called “adolescence-limited offenders” that show delinquent behavior that is mainly limited to the period of adolescence (Moffitt, 1993), but this is a hypothesis that should be tested in subsequent research.
However, the “individual and family risks” group, which was characterized by both individual and family risks, and the most problematic “high risk” group, which showed many risk factors and relatively serious delinquent behavior, may include more “life course persistent offenders” (Moffitt, 1993). Furthermore, the individual and family risk group shows similarity with the “child problems in a traumatizing family environment” profile that was found in a recently published Dutch study by Weijers, Hepping, and Kampijon (2010), which focused on an adolescent group of 81 so-called delinquent “recidivists” or chronic offenders who had contact with the police on several occasions. That profile consists of youth showing behavioral problems and a family that is incapable of handling the problems that are present. The high risk group shows overlap with the “delinquent family” profile of Weijers et al. (2010). That profile consists of youth with families that consider antisocial behavior as normal. It might be that the same is true for the adolescents in the high risk group of the present study, but this is also a hypothesis that should be examined in subsequent research. Our findings also correspond with results of Gorman-Smith, Tolan, Loeber, and Henry (1998) who found that adolescents involved in serious chronic offending were more likely to have families characterized by multiple problems including disruption, conflict, and lack of parental involvement.
The four groups of adolescents that we found were mainly distinguishable by the seriousness and type of the problems that are present. So, despite similarities in their problems, that is, antisocial and oppositional problems and the presence of multiple risk factors, the results of this study indicate that adolescents in secure residential care are characterized by different combinations of risk factors. Due to multiple problems that are often present, it is important to prioritize which problems need to be addressed first during treatment. Therefore, a clear insight into the different dynamic risk factors of each individual adolescent is needed. Results of our study suggest that the adolescent’s substance abuse, contact with delinquent friends, and the adolescent’s poor awareness of problems should be given priority within the context of treatment in secure residential youth care.
Our study has several limitations. In the first place, there were indications that the regression model might have violated the assumption of homoscedasticity. In addition, the relatively small sample size limited the possibilities for cluster analysis. The slight agreement that we found between the hierarchical and K-means 4 cluster model indicates that the division in four groups might not be the best estimate of the true number of clusters in the population (cf. Mandara, 2003). In line with these methodological problem is the notion that the subgroup of 57 adolescents might be somewhat less problematic than the group for whom this information is missing. Therefore, some results may not generalize to adolescents beyond the sample in the present study (Field, 2009; Kazdin, 2003).
A second limitation of this study is the way in which the risk factors are operationalized for use in the cluster analysis. Risk factors were defined by applying cutoff scores, because we wanted to include all the 10 risk factors. Although we have tried to make the best possible decisions on the basis of the original scoring (i.e., consistently using median scores or the most relevant scores based on the item scales) to distinguish between risk and non-risk, the applied cutoff scores in the cluster analysis can be under discussion. However, we did use continuous variables in analyses whenever possible.
A third limitation is related to the fact that most of the data are based on the self-report of the adolescents. Their reports may be susceptible to social desirability factors. The adolescents might have minimized or exaggerated their treatment needs and past behavior due to the belief that their responses could affect treatment placement or progress. However, we did emphasize to all the adolescents that participation in the project was confidential and, therefore, that none of their information would affect treatment placement or progress.
Despite the limitations, our findings show that many adolescents in secure residential care show multiple dynamic risk factors in both an individual and contextual domain. Considering the diverse risks and the problematic behavior of many of these adolescents, there is a high level of need to change these behaviors (cf. Griffith et al., 2009). By paying attention to dynamic risk and protective factors, it becomes clear what the needs and strengths of these adolescents are. This study showed that treatment for some adolescents in secure residential care should be mainly focused on their individual needs, while other adolescents need intensive, multimodal treatment focusing on both risks in the individual, family, and peer domain.
A clear implication for secure residential care programs is that these should pay attention to the different dynamic risk factors of each individual adolescent, specifically with regard to substance use, contact with delinquent friends, and problem awareness. This information can be collected by applying an intake interview protocol with the adolescents shortly after their admission that includes questions concerning dynamic risk and promotive factors. In this respect, we consider (an adapted version of) the SRDC interview (Van der Laan & Blom, 2006b), which was used as an interview with adolescents in the present study, as a potentially suitable instrument because it includes very relevant, clear, and objective questions. Specific MI questions and techniques can also be useful for professionals to apply during such an intake interview with adolescents. Major advantages of an intake interview protocol are that it can serve as an important guideline for treatment and that it forces professionals to pay attention to the adolescent’s perspective so that, for example, the adolescent’s motivation for treatment level becomes instantly clear. In addition, risk assessment instruments (e.g., Gammelgård, Koivisto, Eronen, & Kaltiala-Heino, 2008) can be used to prioritize, in consultation with the adolescent, which problems needs to be addressed first during treatment given that adolescents in secure residential care often show multiple problems.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.