
Abstract
Psychological determinants of aggressive behavior (personality traits and problem behaviors) in 59 Dutch female offenders (outpatients and detainees) were compared with those in 170 male offenders (outpatients and detainees) who were all convicted of a violent crime. The violent female offenders scored significantly higher on neuroticism and trait anger, and significantly lower on hostility than the male offenders; however, effect sizes were small. A subgroup of female forensic psychiatric outpatients did not differ from a subgroup of male outpatients on all measures, whereas a subgroup of female detainees scored significantly higher on anger and aggression, but lower on hostility and psychopathy than did a subgroup of male detainees. These first results might indicate that violent female offenders do not differ much from violent male offenders regarding personality traits and problem behaviors. The differences between both groups of violent offenders were largely borne by the subgroup of violent female detainees compared with the subgroup of violent male detainees.
Based on numerous meta-analytic studies, Andrews and Bonta (2010) concluded that eight factors, called the “Central Eight,” are predictive of future criminal behavior and that these eight factors can be divided into two groups, namely the “Big Four” and the “Modest Four.” The Big Four group of factors includes history of criminal behavior, antisocial personality pattern, antisocial attitudes, and antisocial associates, whereas the second group includes family/marital, school and work, leisure/recreation, and substance abuse. The big four factors have been demonstrated to be the best predictors of future criminal behavior whereas the modest four factors are associated with criminal recidivism to a lesser extent. Although the importance of these eight risk factors is undisputed today, there is still an ongoing debate on the question whether risk factors for criminal behavior in women differ from those in men, and whether possible differences in these factors should result in special treatment programs for female offenders. For instance, Brown and Motiuk (2008) investigated a group of 1,530 sentenced offenders (765 women and 765 men) with the Dynamic Factor Identification Analysis (DFIA; Motiuk & Brown, 1994), an assessment instrument with seven subscales, including Employment, Marital/Family, Associates/Social Interaction, Substance Abuse, Community Functioning, Personal/Emotional, and Attitudes. They found that in 53% of the items with significant predictive validity, there was evidence of gender specificity in items such as less than Grade 10, poor relations with father, and combines alcohol/drugs. Similarly, Heilbrun et al. (2008) ascertained that female offenders had higher ratings on the companions and financial domains of the Level of Service Inventory–Revised (LSI-R; Andrews & Bonta, 1995) when they compared 886 female offenders with 1,435 male offenders.
On the other hand, Blanchette and Taylor (2007) concluded that there was little evidence for gender-specific risk factors after analyzing 580 consecutive security classifications for adult women offenders with the use of the Security Reclassification Scale for Women (SRSW; Blanchette & Taylor, 2007), although they also noted that similar needs might have differential influences on recidivism risk. Furthermore, Andrews et al. (2012) used the LSI-R in five data sets with both female and male offenders (adults and youngsters), and in two data sets with only female offenders (adults), and found strong indications that the Central Eight risk factors or domains for criminal behavior are gender-neutral. However, that should not mean that “women and men should offend in exactly the same way, from the same motivation of for the same reason” (Andrews et al., 2012, p. 117). Similar results were later confirmed in a study by Olver, Stockdale, and Wong (2013), who used the Youth Level of Service/Case Management Inventory (YLS/CMI; Hoge & Andrews, 2003) in a group of 167 youths (93 males and 74 females) with an average age of 15.7 years. They found that the YLS/CMI predicted various recidivism outcomes for female and male youth equally well.
Nevertheless, several studies indicate that the LSI-R does not assess all specific risk factors for female offenders. For instance, Van Voorhis, Wright, Salisbury, and Bauman (2010) emphasized the importance of risk factors such as histories of victimization and abuse, relationship problems, mental illness, drug abuse, self-concept, poverty, and parental issues in female offenders. In their study of American female offenders in prisons, on probation, or on parole, these authors used not only the LSI-R but also two types of measures for gender-responsive needs. These two types of measures included Supplement 1, a paper-and-pencil survey with scales measuring self-esteem, self-efficacy, victimization as an adult, child abuse, parental stress, and relationship dysfunction, and Supplement 2, all the Supplement 1 measures and scales measuring current symptoms of depression, current symptoms of psychosis, mental health history, family (of origin) support, family (of origin) conflict, relationship support, housing safety, anger/hostility, and educational strengths. They concluded that gender-responsive needs such as mental health problems, parental stress, relationship dysfunction, child abuse, and adult physical abuse appeared to be associated with future offending for women on probation and women on parole, and with prison adjustment for women in prisons. The results of Van Voorhis et al. (2010) are in line with the findings from several other studies. For instance, Blanchette (2002) compared the risk factors of 11,541 male offenders with those of 182 female offenders at the time of admission to the Canadian federal prison system. Female offenders seemed to experience relatively more personal and emotional problems than the male offenders, who suffered relatively more often from substance abuse and antisocial attitudes. The personal and emotional problems of female offenders often comprised, among others, a negative self-concept, impulsivity, hostility, and limited assertion, which manifested in low self-esteem and self-harming behavior. No meaningful differences were found between the two groups with respect to other risk factors, such as education, employment, antisocial associates, family, and community functioning (Blanchette, 2002). Yang, Wong, and Coid (2013) identified seven significant risk factors for violence-prone women using structured interviews and self-report questionnaires, namely young age, social-assisted housing, early conduct problems, being the victim of domestic violence, excessive drinking, self-harming, and past criminal justice involvement. A study by Langan and Pelissier (2001), which applied structured interviews in 318 female and 1,326 male federal prisoners, showed that women used drugs more frequently, used harder drugs, and used drugs for different reasons than men. The male inmates reported using the drugs for hedonistic reasons, whereas the female inmates were more likely to report that they had used drugs to alleviate physical or emotional pain. Differences in risk factors between Dutch criminal adolescent females and males were also investigated in a study by Van der Put et al. (2014) with the Dutch version of the Washington State Juvenile Court Pre-Screen Assessment (WSJCPA-NL-2009; Van der Put, Stams, van der Laan, & Oort, 2009) and a semi-structured self-report questionnaire. When 240 females were compared with 1,156 males in the age range of 12 to 18 years, female-specific risk factors for recidivism were found, particularly prevalent in the family domain such as parents with judicial contact, alcohol and/or drug abuse by parents, being a victim of abuse, and personal alcohol or drug abuse.
There are different opinions identified in the literature on whether childhood maltreatment is a risk factor for violence by females, more so than among males. In a sample of 1,030 male and 500 female American prisoners, McClellan, Farabee, and Crouch (1997) found that the female inmates reported more frequent experiences of sexual abuse and parental physical aggression as a child compared with male inmates. This possibly explains why relatively more female offenders than male offenders suffer from posttraumatic stress disorder in combination with substance abuse, the latter being an inadequate strategy to manage emotional distress (Byrne & Howells, 2002). However, using the LSI-R, Lowenkamp, Holsinger, and Latessa (2001) found, just as Andrews et al. in 2012, that “prior childhood abuse had no effect on overall recidivism for either women or men” (p. 560). They hypothesized that abuse as a risk factor may be absorbed through alternative risk predictors such as substance abuse, but knowledge of prior abuse is according to Lowenkamp et al. (2001) still of value in the delivery of correctional treatment.
Studies on specific personality traits and problem behaviors of female offenders, and violent particularly female offenders are scarce. Suter, Byrne, Byrne, Howells, and Day (2002) compared 50 female offenders with 121 male offenders and found that the females scored significantly higher than males on both trait anger, as assessed by the State-Trait Anger Expression Inventory (STAXI; Spielberger, 1991), and state anger, measured with the use of the Novaco Anger Scale–Provocation Inventory (NAS-PI; Novaco, 1994). In a study by Leenaars (2005), 23 violent female adolescents in a forensic psychiatric outpatient clinic were found to score higher on the personality domains of Neuroticism and Openness (NEO Five-Factor Inventory [NEO-FFI]; Hoekstra, Ormel, & De Fruyt, 1996) compared with 140 violent male adolescents. However, no differences were found between the two groups in other problem behaviors, such as hostility, anger, physical aggression, verbal aggression, social anxiety, and lack of social skills.
Altogether, specific gender-responsive needs of female offenders seem to vary from study to study, but a few needs merge consistently, namely, family/marital problems, emotional/personal problems, and substance abuse. Although posttraumatic stress disorder does not seem to be a risk factor in itself, theories about how childhood maltreatment might manifest itself through a risk factor, such as substance abuse, have not been investigated thoroughly. Finally, hardly any studies have been conducted on the specific personality traits and problem behaviors in female offenders and violent female offenders in particular.
Domains such as education/employment, family/marital, or leisure/recreation are only indirectly of importance for the design of individual treatment or rehabilitation plans and require further exploration of the items in these domains. For example, an anger management problem may manifest itself in inadequate responses to commands from a manager, in domestic violence during a conflict with a partner, or in too strong protests against the decision of a referee during a soccer game. Only when problem behaviors are analyzed properly, targets of an individual treatment or rehabilitation plan can be formulated (Haynes & O’Brien, 2000).
Aggression is a major problem behavior in violent offenders. There is evidence that aggressive behavior is related to the traits Neuroticism, Agreeableness, and Consciousness from the Five-Factor Model of personality (Jones, Miller, & Lynam, 2011), and to psychopathy (Porter & Woodworth, 2006). Feelings such as anger and hostility are supposed to contribute to the exhibition of aggressive behavior when not managed adequately (Berkowitz, 2012; Novaco, 2013). More specifically, self-reported aggression in Dutch male violent forensic psychiatric patients was found to have a significant positive relationship to self-reported neuroticism, trait and state anger, and social anxiety in situations where criticism can be given (Hornsveld, Muris, Kraaimaat, & Meesters, 2009). Negative correlations were found between self-reported aggressive behavior and Factor 2 (“chronically unstable and antisocial lifestyle”) of the Psychopathy Checklist–Revised (Hare, 1991), agreeableness and social skills in situations where a compliment can be given. Aggressive behavior can be distinguished into reactive (hostile) and proactive (instrumental) aggression (Crick & Dodge, 1996). Reactive aggression is an angry, defensive response to frustration or provocation, whereas proactive aggression is a deliberate behavior that is meant to obtain a desired goal. Several authors have demonstrated that violent offenders with a relatively low score on psychopathy mainly show reactive aggression, whereas those with a relatively high score tend to be both reactively and proactively aggressive (Cima & Raine, 2009; Cornell et al., 1996; Woodworth & Porter, 2002). Social anxiety and lack of social skills may play a role in reactive aggression and not in proactive aggression because offenders with a relatively high score on psychopathy usually do not experience anxiety when they want to reach their goal. Andrews and Bonta (2010) suggested that the two forms of aggression may be related to different dynamic criminogenic needs and consequently require a different treatment approach.
To obtain insight into the psychological determinants of aggressive behavior, possible differences in personality traits and problem behaviors were examined by comparing a group of violent female offenders with a group of violent male offenders. Then, a subgroup of female forensic psychiatric outpatients was compared with a subgroup of male outpatients and a subgroup of female detainees with a subgroup of male detainees to find whether these possible differences could also be established in both the outpatient and detainee subgroups separately.
Method
Participants
The sample consisted of 59 female offenders (M = 22.69 years, SD = 9.15, range = 14-58 years) and 170 male offenders (M = 27.20 years, SD = 9.50, range = 17-59 years). The group of female offenders consisted of 23 female forensic psychiatric outpatients (M = 21.87 years, SD = 2.44, range = 18-26 years) and 36 female detainees (M = 23.22 years, SD = 11.58, range = 14-58 years). The group of male offenders comprised 72 male forensic psychiatric outpatients (M = 20.19 years, SD = 2.23, range = 17-25 years) and 98 male detainees (M = 32.35 years, SD = 9.50, range = 19-59 years).
The outpatients were recruited from a forensic psychiatric outpatient clinic, “het Dok” in Rotterdam, the Netherlands. The patients were obliged to follow treatment because the judge had established a connection between a mental disorder and a violent offense, such as assault, robbery with violence, or serious threat with violence. In the Netherlands, such offenders can be required to undergo the treatment as (a) an added condition for offenses to which maximum imprisonment for 3 years or less applies, (b) an alternative to prison for offenses to which maximum imprisonment for 6 months or less applies, (c) a condition for suspension of detention while awaiting trial, (d) part of a Penal Program, or (e) a supervision element for a protection agency. The average duration of outpatient treatment is approximately 2 years. One outpatient of 17 years had a conduct or an oppositional defiant disorder as his main diagnosis on Axis I of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR; American Psychiatric Association, 2000), whereas the 94 outpatients of 18 years and older had a cluster B personality disorder on Axis II of the DSM-IV-TR (American Psychiatric Association, 2000) as their main diagnosis.
The detainees were convicted of an imprisonment because of violent crimes, such as serious threat with violence, manslaughter, or murder. They stayed in separate departments of three penitentiary institutions: one for adult females, one for adolescent females, and one for males. Sixteen female detainees were 17 years and younger whereas the other 20 detainees were 18 years and older. All male detainees were 18 years and older. Although detainees sometimes suffer from a mental disorder, in the Netherlands they are only admitted into a forensic psychiatric institution when judges establish a direct connection between deficient mental development or mental disorder and the committed offense. It should be noticed that in Dutch forensic psychiatric institutions, about 70% of the admitted offenders has a cluster B personality disorder as their main diagnosis (De Beurs & Barendregt, 2008), whereas in the United States (Silver, 1995) and Canada (Quinsey, Harris, Rice, & Cormier, 1998) most forensic psychiatric patients are primarily diagnosed with a psychotic disorder.
Measures
A set of measures was used for assessing personality traits and problem behaviors. Because of the relatively small number of participants and the lack of norms from low-educated non-clinically females and males, additional information had been provided about the internal consistency (Cronbach’s α) for each self-report questionnaire in a reference group of 159 female secondary vocational students (M = 18.34 years, SD = 1.77, range = 16-27 years). The set of measures comprises the following instruments.
The NEO-FFI (Costa & McCrae, 1992; Dutch version: Hoekstra et al., 1996) includes 60 items and measures the Big Five traits of Neuroticism, Extraversion, Openness, Agreeableness, and Conscientiousness. Participants rate the items in the NEO-FFI on a 5-point Likert scale ranging from “entirely disagree” to “entirely agree.” The present study was focused only on Neuroticism (e.g., “I seldom feel lonely or sad.”) and Agreeableness (e.g., “Some people find me selfish and egotistic.”), because these traits are considered as relevant in the context of aggression (Jones et al., 2011). In the group of 159 Dutch female secondary vocational students, the internal consistency (Cronbach’s α) of the two subscales was .70 and .57 successively.
The Trait Anger subscale of the Spielberger (1980) State-Trait Anger Scale (STAS; Van der Ploeg, Defares, & Spielberger, 1982), which consists of 10 items, was used to measure the general disposition to anger. Participants rate each item about how they generally feel (e.g., “I am quick tempered.”) by using a 4-point Likert scale: 1 = “almost never,” 2 = “sometimes,” 3 = “often,” and 4 = “almost always.” The internal consistency (Cronbach’s α) of the subscale was .87 in the reference group of female students.
An adapted version of the Rosenzweig (1978) Picture-Frustration Study (PFS-AV; Hornsveld, Nijman, Hollin, & Kraaimaat, 2007) was used to measure hostility. This test asks participants to write down their reactions to 12 cartoon-like pictures. The subjects are instructed to examine the situations shown in the pictures (e.g., to a shopkeeper: “This is the third time that this watch has stopped.”) and to write in the blank text box the first appropriate reply that enters their mind. The answers are rated by an experienced and independent research assistant (psychologist) on a 7-point scale, ranging from 1 = “not hostile at all” to 7 = “extremely hostile.” In the reference group of Dutch female students, the internal consistency (Cronbach’s α) of the PFS-AV was .71.
The Aggression Questionnaire–Short Form (AQ-SF; Bryant & Smith, 2001; Dutch version: Hornsveld, Muris, Kraaimaat, & Meesters, 2009) is a shortened version of the Aggression Questionnaire of Buss and Perry (1992) with 12 items that can be allocated to four subscales, that is, Physical Aggression, Verbal Aggression, Anger, and Hostility. Respondents score the items using a 5-point scale ranging from 1 = “entirely disagree” to 5 = “entirely agree.” The present study only focused on the Physical Aggression subscale (e.g., “Once in a while I can’t control the urge to strike another person.”) and the Verbal Aggression subscale (e.g., “My friends say that I’m somewhat argumentative.”). In the reference group of 159 female secondary vocational students, the internal consistency (Cronbach’s α) of the two subscales was .70 and .64 successively.
The NAS part of the NAS-PI (Novaco, 1994; Dutch version: Hornsveld, Muris, & Kraaimaat, 2011) was used to study the self-reported responses of the participants to 48 anger-eliciting situations (e.g., “When someone yells at me, I yell back at them.”). The items are scored on a 3-point Likert scale: 1 = “never true,” 2 = “sometimes true,” and 3 = “always true.” The internal consistency (Cronbach’s α) of the NAS was .92 in the reference group of female secondary vocational students.
The Inventory of Interpersonal Situations (IIS; Van Dam-Baggen & Kraaimaat, 1999) assesses how much anxiety people experience during social interactions (e.g., “Refusing a request to lend out money”) and how often they can perform the appropriate behavior in such situations. For social anxiety, the scores range from 1 = “no tension at all” to 5 = “very tense”; the frequency scores range from 1 = “never” to 5 = “always.” In the present study, two subscales of this inventory, namely Criticizing and Complimenting, were used, as the results of a previous study indicated that only these subscales differentiated between violent and non-violent participants (Hornsveld, 2005). In the reference group of Dutch students, the internal consistency (Cronbach’s α) of the two subscales was .75 and .89 for social anxiety, and .69 and .76 for the frequency of social skills.
The Psychopathy Checklist–Revised (PCL-R; Hare, 1991; Dutch version: Vertommen, Verheul, De Ruiter, & Hildebrand, 2002) was used to measure psychopathy. This checklist consists of 20 items that have to be rated on a 3-point scale, with 0 = “does not apply,” 1 = “applies to some extent,” and 2 = “applies.” Vertommen et al. (2002) found support for the reliability and validity of the Dutch version of the PCL-R, while Zwets, Hornsveld, Neumann, Muris, and Van Marle (2015) confirmed the PCL-R structure with four facets in a group of 411 Dutch forensic psychiatric inpatients. These four facets are Interpersonal (e.g., “Grandiose self-worth”), Affective (e.g., “Callous and lack of empathy”), Lifestyle (e.g., “Impulsivity”), and Antisocial (e.g., “Juvenile delinquency”). Zwets et al. (2015) also found a strong agreement between raters (ICC = .81, 95% CI [.67, .89]) in a subgroup of 41 forensic psychiatric inpatients. According to Verona and Vitale (2006), the PCL-R has adequate reliability and validity in both female and male populations, although there is skepticism as to whether the PCL-R items adequately tap the characteristics that discriminate psychopathic from non-psychopathic women.
Procedure
The study was approved by the Dutch Review Committee for Patient-Linked Research in Arnhem, the Netherlands, and by the Scientific Research and Documentation Center of the Dutch Ministry of Security and Justice.
Certified clinical psychologists completed the PCL-R assessments. Item scores were based on both file information and a structured interview. However, for some detainees the PCL-R could not be completed because file information was lacking.
Regarding the self-report questionnaires, all participants received an information letter in which the purpose and content of the study were described. This letter clearly stated that participation was on a voluntary basis, data would be processed anonymously, and that refusing to participate would not influence the length of treatment/imprisonment in any way. Patients were asked to sign an informed consent form. The outpatients individually completed the set of questionnaires for which they received a reward of €7. The detainees completed the questionnaires in a classroom and were rewarded with €10.
Data-Analysis
Data sets were analyzed through the statistical program IBM SPSS Statistics 20.0. For the comparison of the female (sub)groups with the male (sub)groups, multiple analysis of covariance (ANCOVA; two-tailed; p < .05) were used. Because of differences in age between the four groups, statistical corrections for age were applied. Unfortunately, not all participants completed the self-report questionnaires according to the instructions. Consequently, the degrees of freedom vary per questionnaire.
Results
When the personality traits and problem behaviors of the female offenders (outpatients plus detainees) were compared with those of the male offenders (outpatients plus detainees), the female offenders were found to score significantly higher on neuroticism, F(2, 218) = 8.26, p = .004, η 2 = .04, and trait anger, F(2, 217) = 4.55, p = .035, η 2 = .02, but significantly lower on hostility, F(2, 206) = 6.03, p = .015, η 2 = .03, than the male offenders. No differences were found between both groups in aggression, state anger, social anxiety, and social skills (Table 1).
Comparison of Scores on Measures Between Female Versus Male Offenders, Controlled for Age.
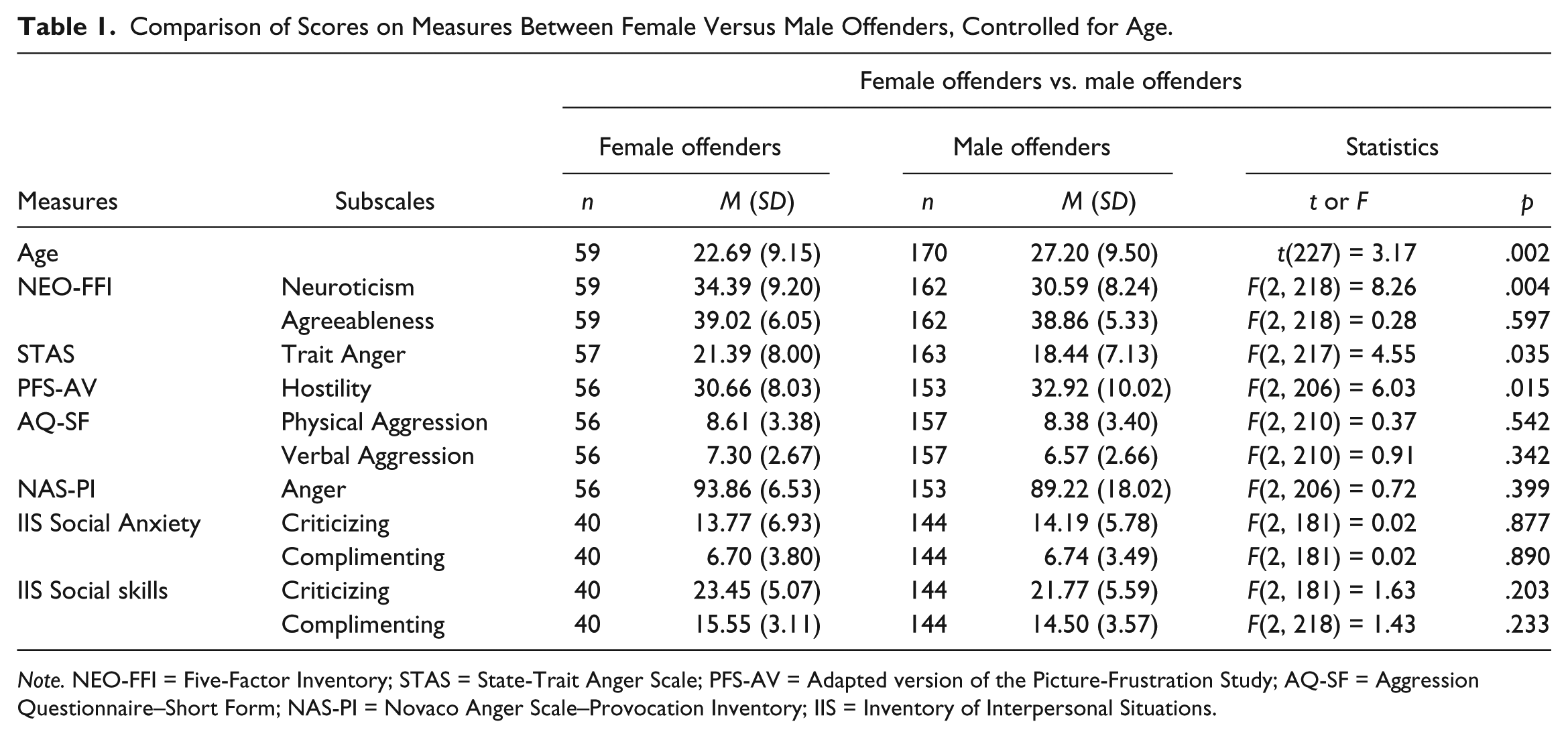
Note. NEO-FFI = Five-Factor Inventory; STAS = State-Trait Anger Scale; PFS-AV = Adapted version of the Picture-Frustration Study; AQ-SF = Aggression Questionnaire–Short Form; NAS-PI = Novaco Anger Scale–Provocation Inventory; IIS = Inventory of Interpersonal Situations.
Regarding differences between the female outpatients and the male outpatients, no significant differences were found between the two groups with the exception of a trend in Neuroticism, F(2, 86) = 2.46, p = .091, η 2 = .05. On this subscale, the female outpatients scored higher than the male outpatients (Table 2).
Comparison of Scores on Measures Between Female and Male Outpatients, Controlled for Age.
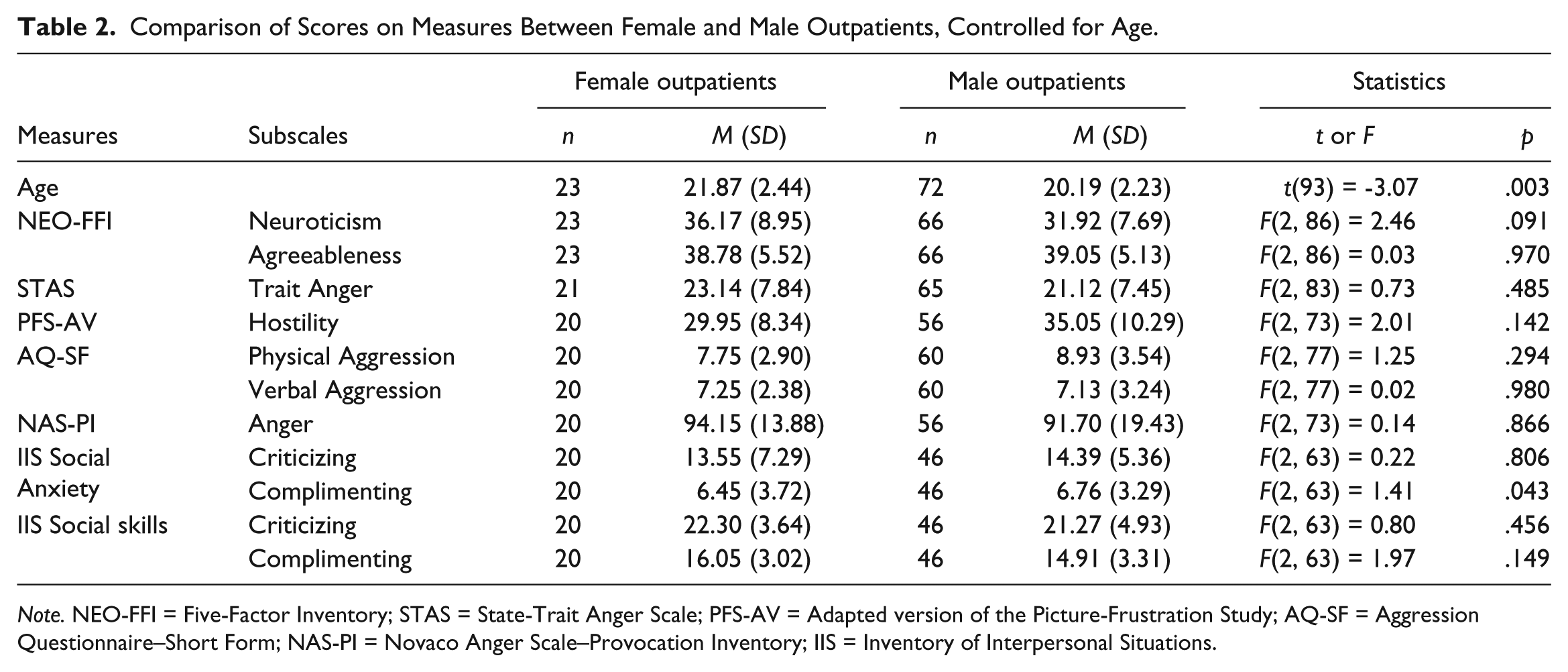
Note. NEO-FFI = Five-Factor Inventory; STAS = State-Trait Anger Scale; PFS-AV = Adapted version of the Picture-Frustration Study; AQ-SF = Aggression Questionnaire–Short Form; NAS-PI = Novaco Anger Scale–Provocation Inventory; IIS = Inventory of Interpersonal Situations.
The female detainees scored significantly lower on hostility, F(2, 130) = 5.41, p = .006, η 2 = .08, and on the total score of psychopathy, F(2, 63) = 6.20, p = .003, η 2 = .16, but higher on trait anger, F(2, 131) = 6.02, p = .003, η 2 = .08; physical aggression, F(2, 130) = 4.93, p = .009, η 2 = .07; verbal aggression, F(2, 130) = 6.63, p = .002, η 2 = .09; and state anger, F(2, 130) = 6.41, p = .002, η 2 = .09, than the male detainees (Table 3).
Comparison of Scores on Measures Between Female Detainees and Male Detainees, Controlled for Age.
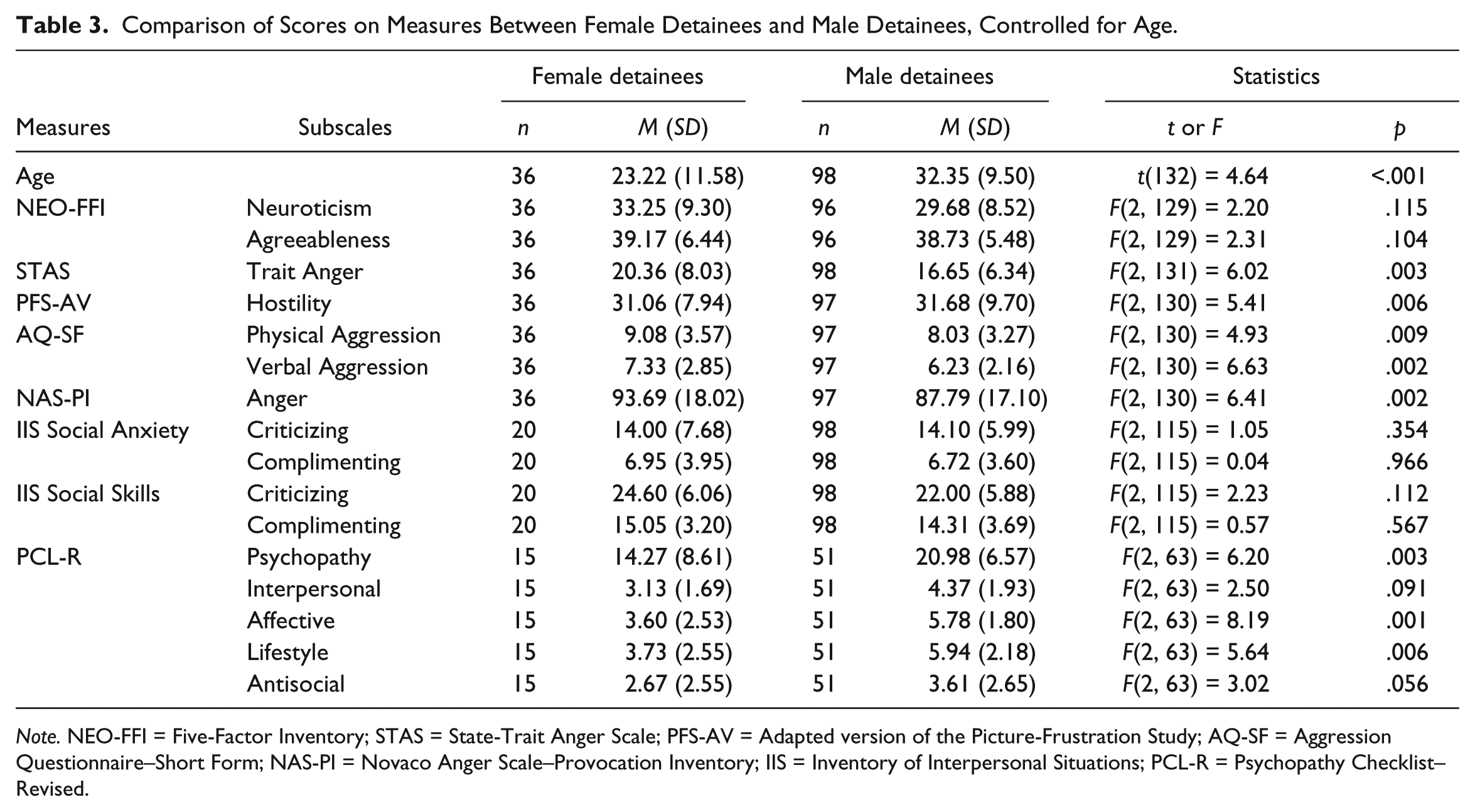
Note. NEO-FFI = Five-Factor Inventory; STAS = State-Trait Anger Scale; PFS-AV = Adapted version of the Picture-Frustration Study; AQ-SF = Aggression Questionnaire–Short Form; NAS-PI = Novaco Anger Scale–Provocation Inventory; IIS = Inventory of Interpersonal Situations; PCL-R = Psychopathy Checklist–Revised.
Discussion
In this study, a group of violent female offenders (outpatients and detainees) was compared with a group of violent male offenders (outpatients and detainees). Also, a subgroup of violent female forensic psychiatric outpatients was compared with a subgroup of violent male forensic psychiatric outpatients, and a subgroup of violent female detainees was compared with a subgroup of male detainees. The violent female offenders (outpatients plus detainees) reported significantly less emotional stability (i.e., higher scores on neuroticism) and hostility, but significantly higher trait anger than did their male counterparts (outpatients plus detainees). However, only high scores on trait anger seemed to be consistently related to violent female offenders because less emotional stability and hostility were also found in a group of low-educated non-clinical women in comparison with low-educated non-clinical men (Hornsveld, Kraaimaat, & Zwets, 2016). The violent female outpatients did not differ significantly from the violent male outpatients in personality traits and problem behaviors, although a trend was found in neuroticism (emotional instability). This means that the differences between the violent female offenders (outpatients plus detainees) and the violent male offenders (outpatients and detainees) can largely be attributed to the violent female detainees, who reported significantly more anger and aggression than the violent male detainees, although they scored significantly lower on hostility and on all facets of psychopathy. No comparisons between groups on social anxiety or social skills yielded any significant difference. The lower score on the PCL-R (Hare, 2003) is in accordance with the findings of other studies (Jackson, Rogers, Neumann, & Lambert, 2002).
Strengths and Limitations
There were several limitations identified within the present study. First, found effect sizes for the significant results were small. The relatively small and various subgroups of outpatients and detainees affect the generalizability of the results. Second, outpatients and detainees participated in the study on a voluntary basis, which means that findings might not apply to all violent female offenders. A third limitation is that the study relied on self-report questionnaires. Therefore, scores might be influenced by social desirability or by limited understanding of their behavior. Fourth, several outpatients and detainees failed to complete all self-report questionnaires, and the files of male detainees were found to be incomplete for the scoring of the PCL-R. Finally, information about the severity of the offenses for which the outpatients and detainees were convicted was not included in the data set of this study.
A question, which may arise from the results of this study, is why the violent female detainees reported more anger and aggression than the violent male detainees. One explanation may be that female detainees are often imprisoned for more severe crimes than male detainees (Rodriguez, Curry, & Lee, 2006; Starr, 2012). Another explanation may be that female detainees have higher rates of mental health problems than male detainees (James & Glaze, 2006) or that a larger percentage of female detainees suffer from prior abuse than male detainees (Harlow, 1999). However, it is unknown whether these explanations also apply to the population of female offenders in Dutch penitentiary institutions.
Until the 1990s, treatment programs for women tended to be copied from programs for male offenders, but after that, more and more authors pleaded for better treatment alternatives for women. For instance, Austin, Bloom, and Donahue (1992) argued that promising programs have to use an “empowerment model” that includes coping skills that address specific risk factors such as substance abuse, parenting, relationships, gender bias, domestic violence, and sexual abuse. Koons, Burrow, Morash, and Bynum (1997) reported that the treatment needs that were most often mentioned as being related to successful treatment outcomes were substance abuse education, substance abuse treatment, parenting skills training, life skills training, relationship skills training, and basic education. Based on a literature study, Bloom and Covington (1998) concluded that females in the correctional system need treatment for drug abuse and trauma recovery as well as education and training in job and parenting skills. Five years later, Bloom, Owen, Covington, and Raeder (2003) confirmed these findings in an extensive report based not only on an update of the literature but also on data from a large number of interviews. These authors also concluded that treatment programs have to take into account the social issues of poverty, abuse, and race and gender inequalities as well as individual factors that affect women. Blanchette and Brown (2006) proposed that treatment programs have to address female-specific responsivity factors, such as child care and antenatal services, protection from abusive partners, physical and mental health care, safe and affordable housing, access to reliable transportation, and access to staff after hours. Finally, Bartlett et al. (2015) concluded that there is an increasing body of evidence for the utility of interventions that address earlier trauma and comorbid substance misuse. In summary, there is unanimity among American, Canadian, and British authors about the addition of specific gender-responsive interventions to the usual treatment programs for male offenders. However, all these recommendations comprise more or less broad domains, which lack the necessary detailing needed for the design of individual treatment or rehabilitation plans.
This study showed that there might be small differences between violent female offenders and violent male offenders in personality traits and problem behaviors: The first group reported relatively more anger and less hostility than the second group, but effect sizes were small. However, a more striking result of our investigation was that the subgroup of violent female detainees reported more aggressive behavior than the subgroup of violent male detainees did. Probably, when women are less likely to be convicted to imprisonment than men for the same offense, female offenders may have committed more severe offenses than their male counterparts. These preliminary conclusions are in accordance with our clinical experience that violent female offenders are mostly angry, whereas violent male offenders are largely suspicious, and that violent female detainees usually have much more psychiatric and psychological problems than violent male detainees. However, to draw more definitive conclusions, personality traits and problem behaviors of violent female offenders have to be studied in larger and more homogeneous groups, not only by comparing them with violent male offenders but also with non-clinical norm groups. In our opinion, future studies on gender-responsiveness in the central eight domains should follow the approach of Van Voorhis et al. (2010), namely analysis of the LSI-R (Andrews & Bonta, 1995) on item level. Such studies will yield more relevant information for individual treatment or rehabilitation plans. However, possible differences between countries in gender-responsive items may be found as the scores on these items may well be influenced by their more or less machismo culture (Hornsveld et al., 2014).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.