
Abstract
In the current study, the associations between inpatient aggression and the living group climate as perceived by the adolescents admitted to a forensic psychiatric treatment unit, are investigated based on carefully registered longitudinal data. Multilevel regression analyses revealed a significant inverse relation between the number and severity of aggressive incidents and the amount of support, as well as with the possibilities of growth perceived by the adolescents. No significant associations of aggression and the perception of repression or atmosphere are found. Our study reveals preliminary evidence for the relation between the prevalence of aggressive incidents and how the adolescents perceive social contextual factors in daily forensic treatment practices. Moreover, preliminary evidence that evidence-based treatment programs and psychiatric care have an important influence on experienced possibilities for growth and support and as such prevent institutional aggression, is found.
Aggression is reported as a frequent indication for psychiatric hospitalization (Rice, Woolston, Stewart, Kerker, & Horwitz, 2002; Ros, van der Helm, Wissink, Stams, & Schaftenaar, 2013), and as such becomes part of daily life in residential psychiatric units and forensic treatment units for children and adolescents (Crespi, 1990; Day, Franklin, & Marshall, 1998; Kaltiala-Heino, Berg, Selander, Työläjärvi, & Kahila, 2007; Tremmery et al., 2014; Tremmery, de Decker, De Hert, De Varé, & Danckaerts, 2012). Vulnerable children and adolescents, with commonly complex psychiatric disorders are almost daily exposed to aggressive situations, either as victim or as witness. These aggressive situations can influence the occurrence of aggression in other patients as an effect of modeling (Fergusson & Horwood, 1996) as well as by the influence on neural mechanisms important for aggression (Fishbein & Sheppard, 2006; Nelson & Trainor, 2007). Moreover, aggressive incidents occurring in a psychiatric ward are shown to be associated with a decreased well-being of working staff, diminished professional behavior, an increased number of absences, and a higher workload (Di Martino, 2002; Estryn-Behar et al., 2008; Nijman, Palmstierna, Almvik, & Stolker, 2005; van der Helm, Boekee, Stams, & van der Laan, 2011). Furthermore, evidence exists for an association between inpatient aggression and a higher number of offenses after treatment (Cochran, Mears, Bales, & Stewart, 2014). The fact that inpatient aggression has such a severe negative impact on both staff and patients and shows possible negative consequences for society makes effective management and prevention of aggression key priorities in mental health settings (Kaltiala-Heino et al., 2007; Masters & Bellonci, 2002; Tremmery et al., 2012).
Besides the impact that aggression can have on others, the factors influencing the occurrence of aggressive incidents are important. In literature concerning aggression in secure institutions, the importation and the deprivation models are historically the main theoretical models explaining the adjustment of patients to institutional life. In the importation model (Irwin & Cressey, 1962), the characteristics of delinquents before their incarceration play a major role in their adjustment to institutional life (DeLisi et al., 2010; Van Nieuwenhuijzen et al., 2006) and influence the occurrence of aggression incidents. Gender, race, gang affiliation, a history of earlier and more severe delinquency are some characteristics shown to be related to more serious institutional misconduct (Trulson, 2007). Moreover, evidence exists for an association between traumatization before imprisonment and institutional misconduct during incarceration in juvenile delinquents (DeLisi et al., 2010). In contrast, the deprivation model, based on the work of Clemmer (1940), Goffman (1961), and Sykes (1958), emphasizes the negative effects of incarceration itself, such as the loss of autonomy, humiliation, and fear. These feelings are thought to cause mutual hostility, reactance, and aggression toward staff and other patients (Harer & Steffensmeier, 1996).
Over the last decades, the two above-described models are questioned as being too simplified, and more complex bio-psycho-social models are assumed to underlie the occurrence of aggressive behaviors (Steinert & Whittington, 2013). In these models, transactional mechanisms of mutual influence (Sameroff, 2009) with a complex interaction between dispositional psychological and biological characteristics as well as environmental characteristics are assumed to contribute to the emergence of aggressive incidents (Daffern, Mayer, & Martin, 2004; Fontaine & Dodge, 2008; Nijman, áCampo, Ravelli, & Merckelbach, 1999; Raine, 2002, 2014; Sameroff, 2009). Biological factors, such as genetic, neuro-endocrinological, and neural vulnerabilities have been shown to play an important role within these transactional models (Popma & Raine, 2006; Raine, 2002, 2014). Other dispositional characteristics, such as a diagnosis of disruptive behavioral disorder and the appearance of psychotic symptoms in children and adolescents (Crocker, Stargatt, & Denton, 2010; McDougall, 2000; Phillips, Stargatt, & Fisher, 2011), are found to be important predictors in the occurrence of institutional aggression. Within these models, personal characteristics are thought to be in continuous interaction with social and environmental characteristics, showing that dispositional characteristics can be mediated by the quality of the environment (Heynen, van der Helm, Cima, Stams, & Korebrits, 2016b).
A forensic treatment entails an intensive psychiatric treatment in combination with an equally important rehabilitation. In a forensic residential treatment unit, patients live in small communities under permanent supervision of trained working staff. A secure environment is a crucial element for a safe therapeutic environment (Kaltiala-Heino & Kahila, 2006). Therefore, the living group climate in these communities plays a crucial role in the management of aggression (Ros et al., 2013). In literature concerning residential psychiatry, an open living group climate is recommended (Janzing & Kerstens, 2012; Toch & Kupers, 2007; van der Helm, Stams, & van der Laan, 2011) and characterized by support, clear opportunities for personal growth, and safety. Moreover, flexibility needs to be weighted against the organizational needs for control. Important goals are equality and mutual respect, together with autonomy and responsibility (Tonkin, 2015). These objectives of an open living group climate are decreasing aggressive incidents and improving a safe therapeutic environment, which fit perfectly with the rehabilitation objectives of a forensic treatment (van der Helm, Klapwijk, Stams, & van der Laan, 2009).
Despite the more recent view of transactional mechanisms underlying the occurrence of aggression, only few researchers have investigated the association between the prevalence of aggression and the living group climate in psychiatric institutions. Recently, Robinson, Craig, and Tonkin (2016) conducted a systematic literature review regarding the perceptions of the living group climate, referred to as the social climate, and aggressive behavior in forensic psychiatric treatment units and they found evidence for an association between the social climate and aggression. In research regarding children and adolescents, however, there is a lack of longitudinal studies that investigate the complex transactional mechanisms, and the research is restricted by the inclusion of self-reported aggression. In a Dutch youth correctional facility, van der Helm, Stams, van Genabeek & van der Laan (2012b) examined how personality and living group climate can contribute to self-reported aggression in incarcerated male youth. They found evidence for a negative association between self-reported aggression and a living group climate characterized by possibilities for growth, support, and a positive atmosphere. A repressive living group climate was not associated with a decrease in self-reported aggression. These findings support the hypothesis of an influence of the living group climate, with an emphasis on its positive characteristics, in contrast with the historically emphasized negative characteristics described in the deprivational model (Harer & Steffensmeier, 1996). More recently, a study by Heynen et al. (2016b), in a German youth prison for adolescent male offenders, shows a significant positive association between self-reported reactive aggression and the perception of repression. No associations with a living group climate characterized by support, growth, and a positive atmosphere were found. These two studies have led to inconsistent findings regarding the important characteristics of living group climate within the transactional mechanisms contributing to the emergence of aggression. Important to note are the differences between the two studied settings in these studies (Heynen et al., 2016b). A post hoc comparison, performed by Heynen et al. (2016b), showed significantly more support and a better group atmosphere in the Dutch youth correctional facility compared with the German youth prison. No differences in the perception of repression or growth were found. Thus, similar levels of perceived repression seem to have a different effect on aggression in the two different studied settings. This might be explained by a buffering effect of the feeling of being supported against the negative effects of repression. Thus, whereas repression seems to play a role in the emergence of aggressive incidents in a youth prison, support and possibilities of personal growth seem to play a role in a more treatment-based correctional youth facility.
In adults, findings of a longitudinal study in a secure psychiatric setting show an important role of the amount of support perceived by inpatients in diminishing the risk of later aggressive incidents occurring on the ward (Ros et al., 2013). In addition, the perception of possibilities of personal growth was associated with less later aggressive incidents, mediated by the amount of support. The amount of repression perceived by inpatients did not predict later aggressive incidents. These findings, in a treatment-based secure forensic setting for adults, are in line with the findings in the Dutch youth correctional facility (van der Helm et al., 2012b).
The amount of evidence on the direct association between aggression and living group climate is scarce. Nevertheless, other research shows indirect evidence for the association between aggression and living group climate. This indirect evidence is found in the relation of a living group climate characterized by support, possibilities of growth, and a positive atmosphere with prosocial behaviors (van der Helm et al., 2009; van der Helm, Stams, van der Stel, van Langen, & van der Laan, 2012a); cognitive empathy (van der Helm et al., 2012a); and a reduction of behavioral problems and recidivism (Schubert, Mulvey, Loughran, & Losoya, 2012). Prosocial behaviors and cognitive empathy, in turn, are associated with less offending and a lower prevalence of aggression (de Wied, Goudena, & Matthys, 2005; Janzing & Kerstens, 2012; Jolliffe & Farrington, 2004; Klimstra, Akse, Hale, Raaijmakers, & Meeus, 2010).
These initial studies do not lead toward robust conclusions, although they give preliminary evidence for the importance of living group climate in the management of aggression in a psychiatric treatment unit. The results of these studies show a complex story, in which group composition, treatment program, and unknown other factors together with living group climate are an important aspect of the management of aggression in a treatment unit (Kaltiala-Heino et al., 2007; Tremmery et al., 2014, 2012).
In the current study, the associations between living group climate and the prevalence of aggression are examined in a forensic adolescent treatment unit using a panel study with repeated measures of the living group climate and a continuous registration of aggressive incidents. This study is the first to our knowledge to investigate these associations by means of a careful continuous registration of all aggressive incidents in a forensic adolescent treatment unit. Investigating these associations is a first step forward in the research of inpatient aggression in forensic psychiatric treatment units for adolescents, by acknowledging the importance of social environmental factors besides the mostly studied patient characteristics. The treatment unit in this study targets reduction of aggression and resocialization of juvenile offenders by means of psychiatric care and an evidence-based offender rehabilitation program (Helmond, Overbeek, & Brugman, 2012). A concept of individualized safe care is emphasized, in line with the assumptions of the risk–need–responsivity (RNR) model (Andrews, Bonta, & Hoge, 1990; Andrews, Bonta, & Wormith, 2006). Forensic care is a form of compulsory care, which makes it even more important to constantly be aware of the patient’s well-being and the patient’s rights. Previous research regarding inpatient aggression mostly focused on predicting institutional aggression based on patient characteristics or predicting recidivism based on institutional aggression. Despite the recently proposed transactional bio-psycho-social models of aggression, social contextual characteristics have mostly been overlooked (Raine, 2002; Sameroff, 2009; Steinert & Whittington, 2013). The current study focuses on the understudied relation between aggression and the living group climate as perceived by the adolescents. This is a first step toward a more in-depth understanding of the complex underlying mechanisms of aggression. An improved understanding of these underlying mechanisms might lead to an improvement of ongoing treatment programs in psychiatric institutions by supporting the resocialization process of aggressive patients, protecting other patients and staff from new traumatic incidents, and protecting society from recidivism. Moreover, in the long run, it will generate further possibilities to influence the aggression on psychiatric units and provide handles to evaluate or change the aggression management policy. This will make a better tailored and evidence-based aggression management and prevention policy possible in which important contextual characteristics can be adjusted to the unique characteristics of each patient.
Method
Setting
The present study was conducted in a forensic adolescent treatment unit, which is part of the child and adolescent department of a large university psychiatric hospital in Leuven, Belgium. The study protocol was approved by the ethical committee of the KU Leuven and the study has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The treatment unit is a residential eight-bed unit for adolescents from 12 to 18 years. The population consists of patients with psychiatric problems, placed under criminal law. The adolescents are always referred by the juvenile court for an intensive treatment of 6 months, which is extended by another 6 months in most cases. Due to a malfunctioning of the adolescents in different important life domains (family, school, social relations), they are in need of a medium to high level of care. This care is given within a medium security setting and the adolescents have a medium to high risk of recidivism.
The forensic treatment is based on the concept of safe care, in which security and treatment go hand in hand and which is in line with the RNR model (Andrews et al., 1990, 2006). Safe care is a concept based on the social competence model (ter Metz & Spanjaard, 2006), which is used as the main framework for treatment on the psychiatric unit with a gradual development of resocialization. In the social competence model, a balance between developmental tasks and skills is important, with increased competence as a main goal. To achieve increased competence, a cognitive–behavioral approach with a focus on positive competences and skills is conducted. During treatment, adolescents go through five different phases with a gradual increase of freedom embedded in a continuous taxation of risks. The adolescent starts in a totally individualized program and gradually moves on to the world outside the treatment unit with more and more participation in developmental tasks (school, hobbies, family etc.). In addition to the social competence model, the aggression management on the treatment unit focuses on early intervention in the “chain of behavior,” prevention, and de-escalating techniques (Masters & Bellonci, 2002).
Participants
The sample of adolescents in this study consisted of 24 inpatients of the forensic adolescent treatment unit (all admitted to the treatment unit in the period between June 25, 2013, and October 27, 2016) with a written and informed consent given by their parents or guardian. The age of the patients at time of admission was between 12 and 17 years, with a mean age of 15.9 years (SD = 1.2 years). Our sample consisted of 16 boys (66%) and eight girls (34%). The mean duration of stay was 303 days (SD = 113 days), with a range between 100 and 529 days. As stated before, duration of treatment can have a maximum length of 12 months. However, after the adolescents’ full treatment is completed, they can be rehospitalized due to recidivism or other important reasons. Eight patients out of the 24 patients participating in this study were rehospitalized, ranging from one rehospitalization to three rehospitalizations. The sample consisted of patients with different complex psychiatric disorders and a variety of comorbidities. Each patient underwent an extensive diagnostic intake procedure before admission, conducted by a multidisciplinary team. Based on the diagnostic report of this intake procedure and a clinical investigation, the psychiatrist of the treatment unit assigned diagnoses based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 2013). All participants received one to four DSM-IV axis 1 diagnoses, with a mean number of 2.5 diagnoses per patient (SD = 1.05). The most frequent axis 1 diagnoses in the sample of adolescents are found within the class of disruptive behavior disorders (15): conduct disorder (11) and oppositional defiant disorder (four). Another substantial group of the included patients were diagnosed with a reactive attachment disorder (14) and attention deficit hyperactivity disorder (ADHD; eight). Other diagnoses assigned to the included patients were mood disorder (four), posttraumatic stress disorder (four), autism (four), parent child problems (two), learning disorder (one), and child neglect (one). Seven patients received axis 2 diagnoses because of lower intellectual functioning, and for 16 adolescents, the axis 2 diagnoses were postponed. The axis 5 scores for Global Assessment of Functioning (GAF) at the time of admission were between 30 and 55, with a mean score of 38.55 (SD = 7.20).
Instruments
The Prison Group Climate Inventory (PGCI)
The PGCI (van der Helm et al., 2011) is a questionnaire with 36 items to be rated on a five-point Likert-type scale. The scale ranges from 1 (I do not agree) to 5 (I totally agree). The quality of living group climate is measured by means of four subscales. These four subscales are repression, support, growth, and group atmosphere, and every item of the questionnaire belongs to one of these four subscales. The repression subscale (nine items) assesses perceptions of restriction and control, dishonest rules, and rigidity at the living group. An example of a repression item is “You better give in and do what group workers tell you to do.” The support subscale (12 items) assesses the degree of responsiveness of the working staff toward the different needs of each patient. The subscale support consists of items measuring the amount of attention group workers pay to the patients, the perception that group workers take patients serious, and respect and trust perceived by the patients. An example of a support item is “Group workers treat me with respect, even if I am angry.” The growth scale (eight items) assesses the perception of opportunities of learning, perception of meaningfulness of the treatment given at the unit, and belief in the future. An example of a growth item is “What I learn here will help me when I’m outside.” The group atmosphere scale (seven items) assesses the way patients behave toward each other, if they trust each other, and how safe they feel toward each other. Furthermore, group atmosphere measures the ability to settle down and trust each other, and having enough daylight and fresh air. An example of a group atmosphere item is “You can trust everybody here.” The reliability and construct validity of the PGCI is favorable for the four subscales, with a Cronbach’s alpha of .92 for support, .70 for atmosphere, .78 for repression, and .91 for growth (van der Helm et al., 2011).
Aggressive incidents
As part of daily record keeping, the staff electronically registers each aggressive incident committed by a patient on the ward. The registration of aggressive incidents is based on the Modified Overt Aggression Scale (MOAS; Kay, Wolkenfeld, & Murrill, 1988). The MOAS is characterized by good interrater reliability (mean weighted kappa’s = .90). In the MOAS, a distinction between four different types of aggression is made, including verbal aggression, aggression against property, physical aggression, and auto-aggression. For each type of aggression, a score of severity has to be given (0 = no aggression, 1 = mild, 2 = moderate, 3 = strong, and 4 = extreme). Different types of aggression can co-occur within one aggressive incident. This electronic registration system is part of daily record keeping on all units of the psychiatric hospital. All staff members were trained and supervised regularly for the registration of aggressive incidents by the researchers. Every week, the main researcher checked the electronic observation reports and looked for possibly unregistered aggressive incidents. When there was a presumption of unregistered aggressive incidents, the situation was reviewed together with the involved staff members and it was decided whether or not additional events should be registered. A systematic and structured registration of aggressive incidents contributes to increased alertness of the staff members for each form of aggression on the ward. In addition, reviewing the incidents with the involved staff members leads to more univocal mind-sets concerning aggression and its severity on the ward.
Statistics
Variables
Data were collected during a period of 32 months (between March 3, 2014, and October 27, 2016). For the living group climate, the PGCI was administered at the end of every month for all inpatients with a minimum length of stay of 2 weeks. The patients were asked to complete the PGCI and were instructed that the questions are about last month in the living group. The responses to the questionnaire were all treated confidentially and anonymously. No names were given on the questionnaires, but each adolescent received a personal code number to protect their privacy. In addition, a researcher who was not connected to the ward administered the questionnaires. Aggressive incidents were continuously registered during this period of 32 months. These raw data were used for visual descriptive analyses to investigate the prevalence of aggressive incidents and the living group climate. To measure the relation between the monthly scores on the PGCI and aggressive incidents on the treatment unit, aggressive incidents that occurred in a period of 28 days before the PGCI was administered were included. Including the aggressive incidents that occurred before the PGCI assessment was chosen because ratings on the PGCI were considered as a rating of the living group climate in the month before. A period of 28 days was chosen to avoid overlapping time frames and to include as much aggressive incidents as possible. For these periods, two scores of aggression were constructed. One score indicates the number of aggressive incidents on the treatment unit within this period of 28 days, without taking into account the complexity of different types of aggression within one incident. A second score was computed to resemble the severity of aggression during this period. For the severity score, a weighted total score was calculated for each aggressive incident, which reflects the overall seriousness of aggression, based on the severity calculations by Kay et al. (1988). Following these calculations, the severity score given for each type of aggression within one aggressive incident was multiplied by 1 (verbal aggression), 2 (aggression against property), 3 (auto-aggression), or 4 (physical aggression). Subsequently, the four weighted scores for each type of aggression were summed up into one weighted total score for each aggressive incident.
Data analysis
To investigate the relation between the prevalence of aggression and the living group climate, multilevel regression analyses for repeated measures were conducted on our data (Kahn, 2011). A multilevel model with aggression in the period before the PGCI was administered as a predictor variable and the score on a subscale of the PGCI as a dependent variable was constructed. The measurements are nested within participants; therefore, a random intercept model was constructed. This model was analyzed for each subscale of the PGCI. The analyses were performed once with the number of aggressive incidents and once with the severity score of aggression as a predictor variable.


Assumptions of normality and homogeneity were checked by a visual inspection of the histogram, qq-plot as well as a Shapiro–Wilk and Kolmogorov–Smirnov test. A likelihood ratio test (LRT) was performed to examine whether the random intercept was needed in our model and the LRT was significant for the four subscales of the PGCI. All analyses were conducted using the general statistical software package SAS (Version 9.3; SAS Institute Inc., 2011). Significance tests were conducted with a significance level of 5%.
Results
Descriptive Statistics
The PGCI was administered 179 times in 24 different inpatients over a period of 32 months with a mean number of 7.16 (SD = 3.92) measurements per patient. These measurements revealed a mean score of 3.94 (SD = 0.70) on the subscale support, a mean score of 4.20 (SD = 0.69) on the subscale possibilities of growth, a mean score of 3.17 (SD = 0.70) on the subscale repression, and a mean score of 3.46 (SD = 0.76) on the subscale atmosphere. When looking at the standard deviations of the scores for each patient, a certain amount of within-patient variability can be observed. In addition, a certain amount of between-patient variability was observed in our data. Patient 1 and Patient 2 seem to score most deviant compared with the other patients. Important to mention is the fact that the PGCI was administered only once in both patients at the end of their treatment period. Therefore, these scores could be biased and have to be interpreted carefully.
During the study period of 32 months, 362 aggressive incidents were registered with a mean of 0.37 aggressive incidents a day. Twenty-three patients were involved with at least one aggressive incident, whereas in one patient, no aggression was registered during the period of the current study. Different types of aggression can occur during one aggressive incident. Over the 362 incidents, 629 types of aggression were registered. This means that on average, 1.74 different types of aggression were scored per incident. The prevalence of aggression per type and per severity is shown in Figure 1. The distribution of severity (mild, moderate, strong, or extreme) of aggression occurring on the ward was highly positively skewed. Regardless of the type of aggression, 48.49% was registered with a mild severity, 38.47% with a moderate severity, 9.66% with a strong severity, and only 3.66% with an extreme severity. Furthermore, the distribution of the types of aggression occurring at the ward was highly positively skewed as well. Regardless of the severity, 42.61% was registered as verbal aggression, 32.75% as aggression against objects, 8.43% as aggression against persons, and 16.22% as aggression against oneself.

Prevalence of aggression per type and per severity of aggression.
Multilevel Regression Analysis
The results of the multilevel regression analyses with the number of aggressive incidents as a predictor variable and the score on each subscale of the PGCI as a dependent variable are shown in Table 1. In these analyses, we only investigated linear associations. These analyses reveal a significant effect of the number of incidents before the PGCI was administered on the subscale possibilities of growth (B = −0.08, SE = 0.02, p = .0005) and the subscale support (B = −0.06, SE = 0.02, p = .0183). Thus, a lower number of registered aggressive incidents on the ward is associated with a higher perception of possibilities of growth and a higher perception of support by the adolescents. Neither a significant effect of the number of incidents on the subscale repression (B = 0.02, SE = 0.02, p = .3680) nor on atmosphere (B = −0.02, SE = 0.02, p = .3298) was detected.
Summary of Multilevel Regression Analyses for the Variable Number of Aggressive Incidents Predicting the Scores on the Four Subscales of the PGCI: Support, Growth, Repression, and Atmosphere.

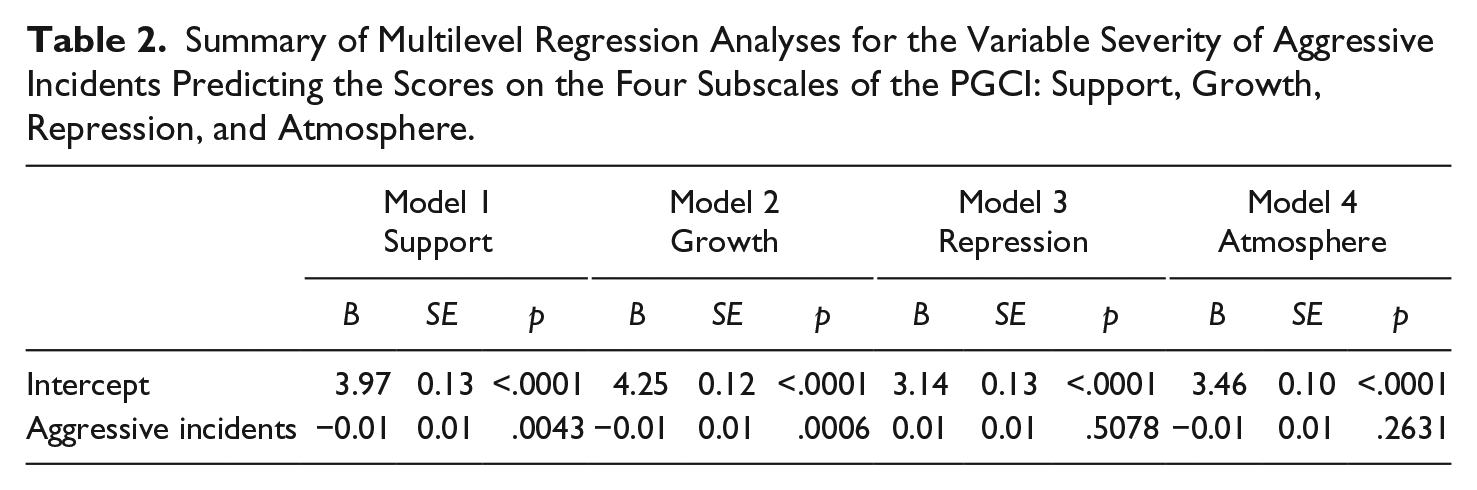
For the multilevel regression analyses with the severity of aggressive incidents as a predictor variable and the score on each subscale of the PGCI as a dependent variable, the results are shown in Table 2. The same significant effects on possibilities of growth (B = −0.01, SE = 0.01, p = .0006) and support (B = −0.01, SE = 0.01, p = .0043) were found. Furthermore, no significant effects on repression (B = 0.01, SE = 0.01, p = .5078) or atmosphere (B = −0.01, SE = 0.01, p = .2631) were found.
Summary of Multilevel Regression Analyses for the Variable Severity of Aggressive Incidents Predicting the Scores on the Four Subscales of the PGCI: Support, Growth, Repression, and Atmosphere.
Discussion
The aim of this article was to present evidence regarding the relation between the prevalence of aggression on the ward and the living group climate, as perceived by adolescents staying in a forensic treatment unit. Based on two earlier described studies in a Dutch youth correctional facility (van der Helm et al., 2012b) and in a German youth prison (Heynen et al., 2016b), we hypothesized to find an association between the number of aggressive incidents and support and possibilities for growth experienced by the adolescents in the forensic treatment unit.
Our results show that a lower number of aggressive incidents as well as less severe aggressive incidents on a forensic treatment unit are related to an increased perception of support and possibilities for personal growth during the period that the aggressive incidents occurred. Although no causal relations can be derived from our analyses, we expect bidirectional associations between these characteristics of living group climate and the occurrence of aggression on the ward. These results are in line with the earlier described findings of a study in a Dutch youth correctional facility concerning the association between living group climate and self-reported aggression (van der Helm et al., 2012b). In addition, our results raise further evidence for the findings of a study in a secure psychiatric setting for adults in which negative associations between possibilities of growth and later registered aggressive incidents as well as between support and later registered aggressive incidents were found (Ros et al., 2013). Our results bridge the gap between the two previously described studies by raising evidence for the importance of support and growth based on data derived from a careful registration of aggressive incidents on a forensic treatment unit for adolescents. These results support the importance of positive social environmental characteristics, such as possibilities of growth and support, within the complex transactional mechanisms underlying the occurrence of aggression.
No significant relations between the number of aggressive incidents or the severity of aggressive incidents and perception of group atmosphere were found in our results. This is in line with the findings in a German youth prison, but in contrast with the findings in a Dutch youth correctional facility. An explanation for these inconsistent findings regarding the relation between aggression and group atmosphere might be found in the way the construct atmosphere is measured in the PGCI (van der Helm et al., 2011). The construct atmosphere has a multifacet character, including feelings of safety, cleanliness, and respect for each other at the living group. Therefore, the items of the PGCI designated to measure atmosphere, are characterized with a higher heterogeneity compared with the items measuring the other subscales. This higher heterogeneity might lead to less univocal results concerning the relation of atmosphere with aggression. Further analysis on item level will be performed in the future.
No significant relations between the perception of repression and the number or severity of aggressive incidents were found in our results. This is in line with the findings in a Dutch youth correctional facility (van der Helm et al., 2012b) and in a secure psychiatric setting for adults (Ros et al., 2013), but contrasting with the findings in a German youth prison (Heynen et al., 2016b). As described earlier, the treatment program in the unit of the current study is more in line with the goals of the Dutch youth correctional facility than with the German youth prison. The main difference compared with the German youth prison is the implementation of an evidence-based treatment program and psychiatric care in the forensic treatment unit of the current study (Heynen, Behrens, & van der Helm, 2016a). Therefore, our findings give supportive evidence for the assumption stated by Heynen et al. (2016b) of a buffering effect of evidence-based treatment programs and psychiatric care against the negative effects of repression. Another possible hypothesis is that the association between aggression and repression is based on critical levels of repression. We would expect extremely low amounts of repression in a secure facility to be associated with an increased amount of aggressive incidents, due to a lack of norms and principles of group power. Whereas, an extremely high score on the repression subscale could be associated with an increased reactance and aggressive incidents, in line with the deprivation model (Harer & Steffensmeier, 1996). The fact that we did not find a significant association of aggression with repression might be explained by the possibly moderate amount of repression perceived by the patients in the currently studied forensic treatment unit. Post hoc comparisons of the scores on the subscales of the PGCI of the adolescents in the currently studied setting with the German youth prison and the Dutch youth correctional facility would be interesting for a more in-depth understanding of the relation between aggression and living group climate. However, due to the small sample size in this study, post hoc comparisons were not possible.
There are some limitations to this study that need to be acknowledged. A main limitation is the small sample size of this study (N = 24). This small sample size is due to the small capacity of eight beds at the treatment unit and the length of treatment between 6 and 12 months, which results in a low patient flow. Because of this small sample size and the inclusion of only one treatment unit, generalization of our results is difficult to make. Data collection is being continued, and we recently started to conduct the PGCI monthly in other units of the psychiatric hospital and will start to elaborate this study in other psychiatric hospitals to enlarge the possibilities for future research. Another major limitation is that this study investigated the relation between environmental factors and the prevalence of aggression, without taking the other factors of the bio-psycho-social transactional model into account. Due to the small sample size, it was not possible to include more variables. For future research, it would be interesting to include personal characteristics, such as psychiatric diagnoses, personality traits, gender, age, and so forth. In addition, because of the treatment in different phases, with each phase characterized by different aims, challenges, and different degrees of freedom, treatment phase should be included in future research.
Despite its limitations, the present study is one of the first to examine the association between living group climate and the actual occurrence of aggressive incidents on the ward of a forensic adolescent treatment unit. Moreover, this study is the first to our knowledge to investigate this relation based on carefully registered longitudinal data. Due to the small capacity of this unique data set, generalizable conclusions are difficult to make. However, the current study revealed evidence for the important associations of the prevalence of aggression and social environmental factors, which supports the proposed transactional models underlying inpatient aggression in daily forensic treatment practices. It can be expected that interventions focused on this transactional model, will show an impact on both the living group climate and the occurrence of aggression. Moreover, preliminary evidence that evidence-based treatment programs and psychiatric care have an important influence on experienced possibilities for growth and support and as such are associated with institutional aggression is found. Therefore, an evidence-based treatment program focused on institutional aggression and on a positive living group climate is an important rehabilitation objective of a forensic treatment. Another interesting finding is that the number and severity of aggressive incidents are not related to the perceptions of repression. Further research in different forensic psychiatric treatment units and other secure residential facilities is needed for a more in-depth understanding of the complex transactional mechanisms underlying the occurrence of aggressive incidents in secure institutions for delinquent juveniles, to improve treatment and outcomes for this vulnerable group of adolescents.
Footnotes
Acknowledgements
The authors would like to thank all the adolescents who participated in this research for their time and contribution. The authors would also like to thank the whole team of the forensic psychiatric treatment unit Fordulas at UPC KU Leuven, campus Kortenberg for their time and sustained effort put into the registration of the aggressive incidents on the ward. The authors are also grateful to Martien Wampers for her expertise and assistance in the analyzing process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was co-financed by the Taskforce for Applied Research SIA as part of the NWO (The Netherlands Organisation for Scientific Research).