
Abstract
This research describes the development of a targeted service delivery approach that tailors the delivery of interventions that target criminogenic needs to the specific learning and treatment needs of justice-involved people with serious mental illnesses (SMI). This targeted service delivery approach includes five service delivery strategies: repetition and summarizing, amplification, coaching, low-demand practice, and maximizing participation. Examples of how to apply each strategy in session are provided, as well as recommendations on when to use each strategy during the delivery of interventions that target criminogenic needs. This targeted service delivery approach makes an important contribution to the development of interventions for justice-involved people with SMI by increasing the chances that people with SMI can participate fully in and benefit from these interventions that target criminogenic needs. These developments come at a critical time in the field as the next generation of services for justice-involved people with SMI are being developed.
Arrest and incarceration are a pervasive reality for people with serious mental illnesses (SMI; Ditton, 1999; Steadman, Osher, Robbins, Case, & Samuels, 2009; Teplin, 1990). The prevalence of people with SMI (i.e., schizophrenia spectrum and major affective disorders) in the criminal justice system has led to the development of numerous interventions, which have recently been termed first generation services (Epperson et al., 2014). These services include pre- and postjail diversion services (Broner, Lattimore, Cowell, & Schlenger, 2004; Compton, Bahora, Watson, & Olivia, 2008), specialty community supervision caseloads (probation or parole; Skeem & Louden, 2006; Skeem, Manchak, & Peterson, 2011), mental health courts (Cosden, Ellens, Schnell, & Yamini-Diouf, 2005), and reentry services (Osher, Steadman, & Barr, 2003).
A distinguishing feature of first generation mental health services for justice-involved people with SMI is that access to mental health treatment plays a central role in their approach to reducing recidivism (Epperson et al., 2014). However, none of these services have achieved a consistent impact on participants’ subsequent involvement in the criminal justice system (Morrissey, Meyer, & Cuddeback, 2007; Osher & Steadman, 2007; Skeem et al., 2011). According to Skeem et al. (2011), there is weak evidence that service models most closely aligned to traditional mental health treatment reduce recidivism.
This lack of support has prompted discussions of what elements are missing from these approaches to treating justice-involved people with SMI (Epperson et al., 2014; Morrissey et al., 2007). One answer, which is amassing a growing body of support, is that mental health services need to expand their focus to include interventions that explicitly target behaviors most closely associated with criminal offending (i.e., criminogenic needs) among the general population of individuals in the criminal justice system (Calsyn, Yonker, Lemming, Morse, & Klinkenberg, 2005; Epperson et al., 2014; Fisher, Silver, & Wolff, 2006; Lurigio, 2011; Morrissey et al., 2007; Skeem et al., 2011; Wilson et al., 2014; Wolff, Morgan, & Shi, 2013; Wolff, Morgan, Shi, Fisher, & Huening, 2011). This article presents a new approach to delivering interventions that target criminogenic needs to people with SMI.
Criminogenic Risk and Justice-Involved Persons With SMI
Research comparing the presence of criminogenic risk factors among offenders with and without SMI has found that justice-involved people with SMI face higher levels of criminogenic risk factors than offenders without mental illness (Girard & Wormith, 2004; Skeem, Eno Louden, Manchak, Vidal, & Haddad, 2008). Several recent studies have examined the extent to which specific types of criminogenic risks are present among justice-involved people with SMI, finding that people with SMI had elevated levels of criminal thinking and attitudes as compared with their justice-involved counterparts without SMI (Morgan, Fisher, Duan, Mandracchia, & Murray, 2010; Wilson et al., 2014; Wolff et al., 2013; Wolff et al., 2011).
Addressing the presence of elevated levels of criminal thinking and attitudes among justice-involved people with SMI is important when developing interventions for this population because antisocial cognitions are one of the criminogenic risk factors that have the greatest effect on offending behaviors and are both dynamic (i.e., changeable) and amenable to intervention (Andrews, Bonta, & Wormith, 2006; Friendship, Blud, Erikson, Travers, & Thornton, 2003; Walters, Trgovac, Rychlec, Di Fazio, & Olson, 2002). However, traditional mental health services focus on the treatment of symptoms associated with mental illness (e.g., depression, mania, and psychosis) rather than on antisocial cognitions or other criminogenic risk factors. Therefore, to effect criminal justice involvement among justice-involved people with SMI, the scope of intervention needs to be expanded to address the dynamic, malleable criminogenic risk factors associated with this involvement, which are commonly referred to as criminogenic needs (Calsyn et al., 2005; Epperson et al., 2014; Skeem et al., 2011; Wilson et al., 2014).
Interventions That Target Criminogenic Needs for Justice-Involved Persons With SMI
One promising approach to addressing criminogenic needs among justice-involved people with SMI involves modifying existing correctional interventions for use with this population (Skeem et al., 2011). Some of the best-known interventions that target criminogenic needs include reasoning & rehabilitation (R&R; Ross & Fabiano, 1985) which has several versions (see http://www.cognitivecentre.ca/RRProgram for more information), moral reconation therapy (MRT; Little, Robinson, & Burnette, 1991), and Thinking for a change (T4C; Bush, Glick, & Taymans, & Guevara, 2011). Each of these interventions adheres to the central principles of effective correctional interventions (Andrews & Bonta, 2010) by using group-based cognitive behavioral therapy (CBT) interventions that target one or more criminogenic needs (i.e., antisocial behavior, personality, cognition, and associates) with the strongest associated with criminal offending. All three interventions provide a structured, manualized, time-limited group-based intervention that engages some combination of cognitive restructuring, cognitive skills training, problem-solving therapies, and structured learning experiences (Landenberger & Lipsey, 2005; Milkman & Wanberg, 2007). Meta-analyses have established that these interventions reduce recidivism by 20% to 55% (Landenberger & Lipsey, 2005; Pearson, Lipton, Cleland, & Yee, 2002; Wilson, Bouffard, & MacKenzie, 2005). However, there is little evidence to support these interventions’ effectiveness with people with SMI (Milkman & Wanberg, 2007).
The lack of support for the effectiveness of interventions that target criminogenic needs among people with SMI is important to note because the responsivity principle from the Risk-Need-Responsivity (RNR) model posits that the delivery of interventions that target criminogenic needs must to be tailored to the specific learning styles and treatment needs of particular client populations (Andrews & Bonta, 2010). The neurocognitive and social impairments associated with SMI have led to individuals with these disorders being identified as a group of participants who have specific learning and treatment needs that require further consideration during the delivery of interventions that target criminogenic needs (Bonta, Law, & Hanson, 1998; Young & Ross, 2007).
Reasoning & rehabilitation has been adapted for use with people with mental illness (Young & Ross, 2007; see http://www.cognitivecentre.ca/RRProgram). The preliminary outcomes related to the acceptability of the adapted intervention have been positive (Young, Chick, & Gudjonsson, 2010). Moreover, these outcomes support the need to modify interventions that target criminogenic needs to meet the specific learning and treatment needs of people with SMI. However, the proprietary nature of the R&R intervention limits the information available regarding the adaptation process or strategies used to develop the modified intervention.
Given these constraints, the field needs more accessible interventions that target criminogenic needs among justice-involved people with SMI. To fill this gap, we present a targeted service delivery approach (TSDA) that is designed to make existing evidence-based interventions that address criminogenic needs in justice-involved populations responsive to the specific learning and treatment needs of people with SMI. In this article, we describe the development and use of a newly developed TSDA.
The TSDA presented in this article represents an important step forward in the development of interventions for justice-involved people with SMI because it is designed to increase the chances that people with SMI will be able to participate fully in and benefit from interventions that address criminogenic needs. This advancement comes at a critical time in this field of research because interventions with the potential to address criminogenic needs are a critical component of the next generation of services currently being developed for people with SMI involved in the criminal justice system (Epperson et al., 2014).
Method
Study Design
The TSDA presented here was developed using Rounsaville, Carroll, and Onken’s (2001) Stage Model of Behavioral Therapies. Our process to develop the TSDA is consistent with Stage 1a of this model, where the work is focused on the development and manualization of the new intervention. One of the primary products of Stage 1a work is the development of a clear description of the new intervention and how it builds upon and distinguishes itself from existing interventions, which we provide in the “Results” section. All of the research activities associated with the development of the TSDA took place between March 2012 and October 2014, and all research protocols and procedures were approved by the institutional review board of the two principal investigators’ (PIs) university, and, when available, at committees for the community-based organizations where research took place.
Step 1
The TSDA presented here was developed through a two-step process. During Step 1, the PIs began developing the TSDA by engaging in three activities: (a) identifying responsivity issues associated with SMI that need to be compensated for during the delivery of interventions that target criminogenic needs, (b) developing an initial list of therapeutic strategies to be developed further during Step 2, and (c) selecting a specific intervention that targets criminogenic factors that would be used to develop the service delivering approach during Step 2.
Identifying responsivity issues
The service delivery approach developed in this research is designed to address the neurocognitive and social impairments that affect people with SMI’s ability to engage in knowledge acquisition and skill development activities. Specific neurocognitive issues that are targeted by this framework include participants’ speed of learning, capacity to sustain attention, and ability to retain and recall information (Bellack, Gold, & Buchanan, 1999; Hogarty & Flesher, 1999; Wexler & Bell, 2005). Specific social impairments that are addressed include the participants’ ability to accurately recognize emotions, ability to interpret emotions in others, and ability to effectively identify, interpret, and respond to social cues (Bartholomeusz & Allott, 2012; Kopelowicz, Liberman, & Zarate, 2006).
Developing a preliminary list of targeted service delivery strategies
The project PIs used a number of resources to develop an initial list of targeted delivery strategies for use during Step 2 of the project. The initial list included frequent repetition and summaries of intervention content, providing more support to participants during the role-play, using guided discovery techniques when engaging participants in the discussion of intervention content, and engaging techniques such as group opening and closing activities and snacks to maximize participation and group involvement. This list was developed using a number of resources including a review of therapeutic techniques used to compensate for neurocognitive and social impairments in psychosocial interventions in the mental health system, and those used to increase participation and engagement in a group-based CBT intervention. The initial list also included information gained from a training at the Beck Institute for Cognitive Behavioral Therapy, focused on CBT for Schizophrenia, and feedback from an advisory group composed of practitioners, policy makers, and researchers from the mental health and criminal justice systems.
Selecting an intervention
T4C was selected for the hands-on development phase of this project for several reasons. First, given the high prevalence of SMI among those incarcerated in U.S. correctional systems (Ditton, 1999; Steadman et al., 2009) and the fact that T4C has been used in more than 40 state correctional systems in the United States (Milkman & Wanberg, 2007), the TSDA developed here could be disseminated widely if used with T4C. Second, T4C was selected because its copyright gives the National Institute of Corrections the right to distribute all intervention materials (free of charge) for use with individuals under the supervision of the criminal justice system (Bush, Glick, Taymans, & Guevara, 2011), thereby increasing its dissemination potential if future research supports T4C with the TSDA to be a successful intervention for our target population.
T4C is a highly structured, 25-session, manualized intervention that is delivered in a closed-group format to eight to 12 people at least twice a week over a 3-month time period. The intervention curriculum includes three modules: (a) social skills training that teach participants cognitive skills to interpret and respond positively to social situations that involve potential conflict; (b) cognitive restructuring activities that teach participants a concrete process for self-reflection; and (c) a structured problem-solving method that builds on the skills taught in the other two modules to integrate the skills from the modules to teach participants skills to manage interpersonally challenging situations (Bush et al., 2011). Both study PIs completed a 4-day T4C training as part of the project’s first stage of intervention development activities. All intervention groups conducted as part of this study used the curriculum materials from Thinking for a Change: Integrated Cognitive Behavior Change Program (Version 3.1; Bush et al., 2011) obtained from the National Institute on Corrections website (http://nicic.gov/library/025057).
Step 2
This stage of intervention development activities had one main goal—to develop the final set of targeted service delivery strategies. To achieve this goal, research activities during this step focused on providing the study team with hands-on opportunities to further develop the service strategies identified during Step 1 through an iterative process that involved delivering three cycles of T4C.
Intervention cycles
During Step 2, the study PIs delivered three separate cycles of T4C to justice-involved people with SMI who were assessed as having moderate to high risk for recidivism. Two cycles of the intervention were conducted in a county jail (Cycles 1 and 3), and one in a community mental health setting (Cycle 2). The study PIs delivered Cycles 1 and 3 and supervised the delivery of Cycle 2 where two experienced community-based mental health practitioners (one master’s level, one bachelor’s level) delivered the intervention in a community mental health center. Both PIs are licensed social workers with PhDs and practice experience in both the mental health and criminal justice systems.
Piloting and finalizing the TSDA
The goal of this research was to develop and finalize a set of therapeutic strategies that could be used to address the specific learning and treatment needs of people with SMI during the delivery of interventions that target criminogenic needs like T4C. The final set of therapeutic strategies were developed through an iterative process wherein strategies were tried out and modified over the course of the three cycles of T4C that were delivered during Stage 2. As the intervention materials were still being finalized during Stage 2, outcome data were not collected. Consistent with the recommendations made by Rounsaville et al. (2001), the intervention team used their clinical judgment to examine whether the therapeutic strategies were achieving their desired results. The use of clinical judgment to assess outcomes is recommended during this stage of intervention development, because the intervention is still evolving and the number of potential treatment targets and outcomes far exceeded the number that could be systematically measured in early intervention research efforts, where the focus is on developing and systematizing the use of therapeutic strategies for testing in later research. To support the development of therapeutic strategies that could be manualized, data collection efforts during Stage 2 of this project did focus on documenting and analyzing the therapeutic strategies that facilitators use during the delivery of the intervention to accomplish this goal.
As part of the intervention development, the facilitators documented all of the therapeutic strategies the team uses to deliver the content of the intervention during each session. The intervention team then met regularly to review and discuss the facilitator notes to identify therapeutic strategies that were being used to respond to the learning and treatment needs of people with SMI during the delivery of the intervention. During the last session of each cycle of T4C, the facilitators set aside time in session to debrief participants to obtain participant feedback. Notes were taken on information obtained in these debriefing sessions. Then, after each cycle of the intervention was completed, the research team analyzed the facilitator notes and participant feedback using open-coding procedures recommended for qualitative research (Emerson, Fretz, & Shaw, 1995). Similar to the weekly meetings conducted during the intervention, this analysis focused on identifying the full list of service delivery strategies that emerged during the delivery of the intervention and organizing them into the TSDA presented here.
Participants
Each cycle of the intervention was conducted with participants who met the following criteria: (a) adult male 18 years or older; (b) have a primary diagnosis in the schizophrenia spectrum, bipolar disorder I/II, or major depression recurrent or single episode with psychotic features; (c) have involvement with the criminal justice system; and (d) have a moderate to high risk for recidivism as determined by the Level of Service and Case Management Inventory (LS/CMI; Andrews, Bonta, & Wormith, 2004). The exclusion criterion was the presence of an intellectual disability. Although the T4C intervention does not require single sex groups, the decision was made to restrict groups to men because the jail site did not allow mixed-gender groups. Participation in all of the groups was voluntary.
In all, 24 individuals participated in the three intervention cycles. As the research conducted here focused on developing an intervention, and not testing it, information about participants is limited to their sociodemographic characteristics. In total, nine men participated in the first cycle conducted in the county jail, five men participated in the second cycle conducted at the community mental health center, and 10 men participated in the third cycle conducted in the county jail. Participants ranged from age 20 to 57 years, with average age per cycle ranging from 31 years in Cycle 1 to 44 years for Cycle 2. All participants from the two groups in the jail setting (n = 19) self-identified as African American, whereas 60% of participants in the community-based setting (n = 5) self-identified as African American and 40% as Caucasian.
Results
TSDA
The TSDA illustrated in Table 1 presents the five service delivery strategies that were developed through the research process described above. These strategies do not supplant or replace any of the content of the criminogenic intervention, rather they are designed to be used during the delivery of the intervention to make it more responsive to the needs of people with SMI. The content of the intervention itself remains intact.
Targeted Service Delivery Approach.
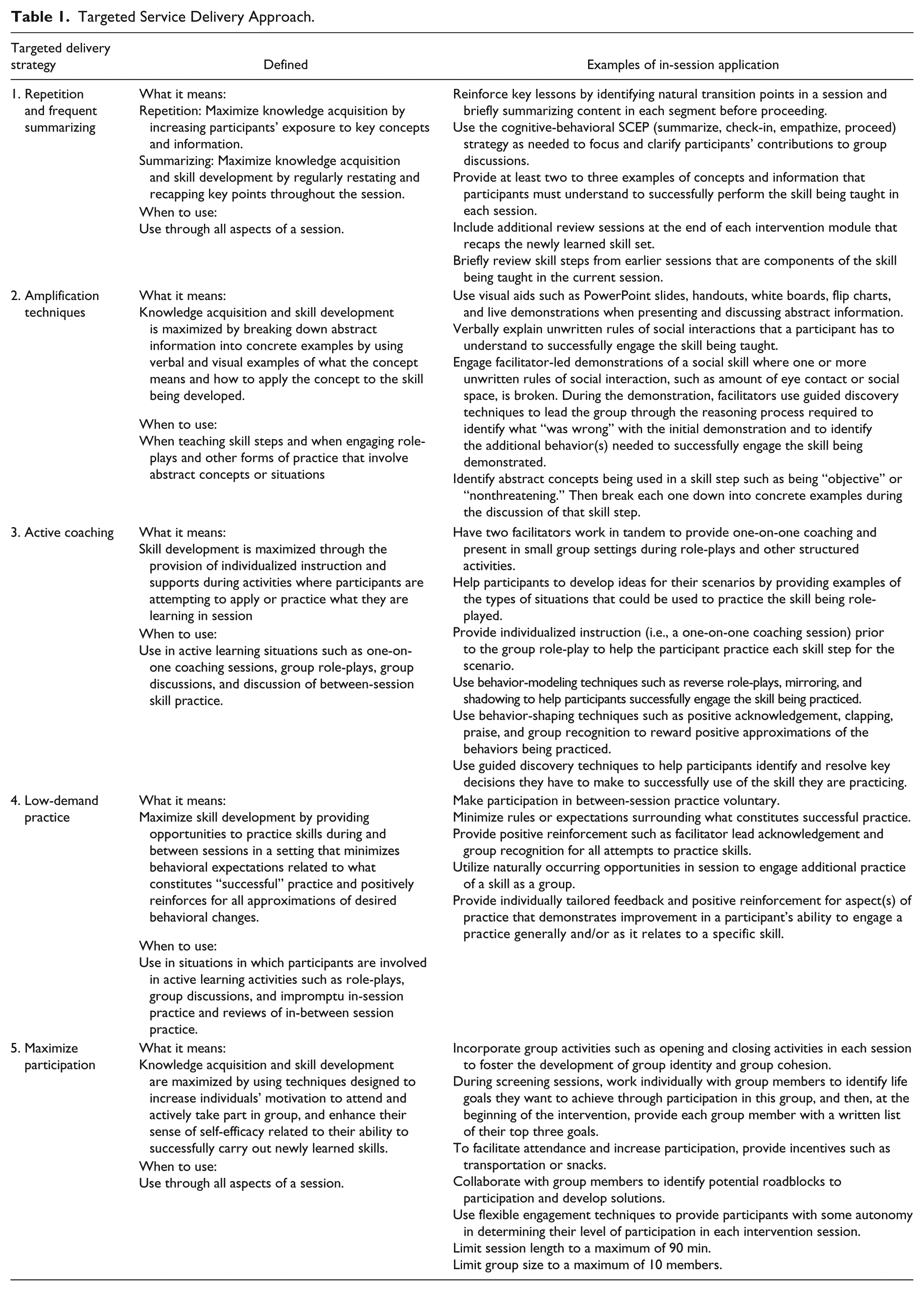
The goal of the TSDA is to compensate for the neurocognitive and social impairments that impede participant’s ability to fully engage and understand the intervention materials. The targeted delivery strategies developed through this research process include repetition and frequent summarizing, amplification, active coaching, low-demand practice, and maximizing participation. Table 1 also indicates points in the intervention where facilitators should use each targeted service delivery strategy to facilitate the delivery of the intervention’s content and provides examples of how each of these five strategies can be used during the delivery of a group-based CBT intervention to address criminogenic needs for justice-involved people with SMI.
The first four targeted service delivery strategies listed in Table 1—repetition and frequent summarizing, amplification, active coaching, and low-demand practice—engage therapeutic techniques that target different aspects of intervention activities that focus on knowledge development and skill acquisition activities. Although each strategy has a distinct therapeutic target listed in the second column of the table, these four strategies also work together in a session to maximize participants’ learning opportunities while engaging techniques that limit participants’ errors or incorrect responses during the learning process. Most of the targeted service delivery strategies developed in this research focus on knowledge development and skill acquisition in interventions that target criminogenic needs because these components of the intervention are especially vulnerable to the effects of neurocognitive and social impairments associated with SMI (Bartholomeusz & Allott, 2012; Bellack et al., 1999; Hogarty & Flesher, 1999; Kopelowicz et al., 2006; Wexler & Bell, 2005).
The primary target of the first four targeted service delivery strategies was maximizing participants’ learning opportunities (knowledge and skill based). However, by minimizing the mistakes participants make in the learning process, these service strategies also supported the goal of the fifth targeted service delivery strategy, maximizing participation. This service delivery strategy is designed to support participants’ ability to engage the intervention materials by maximizing the amount of time individuals are physically present and active in the group (e.g., incentives, collaborative inquiry techniques, limiting session length), and incorporates techniques to optimize individual participants’ involvement in group activities when they are physically present (e.g., opening and closing exercises, snacks, limiting group size).
Discussion
This article presents a TSDA that provides a new way to deliver interventions that target criminogenic needs to people with SMI. The central component of this new TSDA are five targeted service delivery strategies that explicitly address the specific learning and treatment needs of people with SMI during the delivery of these interventions. This TSDA represents a step forward in the development of interventions that target criminogenic needs for justice-involved people with SMI because these five service delivery strategies are designed to increase the likelihood that people with SMI will be able to fully engage in and benefit from interventions that target criminogenic needs. The description of this TSDA and how it was developed makes a contribution to the literature because it can inform other efforts to use group-based CBT interventions that target criminogenic needs with justice-involved people with SMI, thereby increasing the accessibility of these interventions for this population.
When considering how to deliver interventions that target criminogenic needs to people with SMI, we found that pacing the delivery of intervention content was a key issue. Controlling the pace of content was of such importance during the delivery of the intervention that four of the five targeted service delivery strategies included in our approach either directly adjusted the pacing of intervention content (repetition and summarizing, low-demand practice) or provided additional supports that compensate for the pacing (amplification, active coaching). The issue of optimal pacing of interventions that target criminogenic needs remains open and warrants further investigation. However, given that people with SMI present with various combinations and degrees of neurocognitive and social impairments, it is unlikely that one level of pacing will be optimal for all participants; therefore, flexible service delivery strategies, such as the ones presented here will be needed.
The study team also found that participants’ engagement in the intervention was highest when facilitators remained focused on the therapeutic targets of the intervention (i.e., developing new thinking and learning skills for dealing with situations that are likely to increase an individual’s risk of involvement with the criminal justice system). Implicit in this focus is the study team’s purposeful decision not to incorporate additional treatment goals (e.g., medication compliance, symptom reduction) as a focus of the intervention. This decision is consistent with the recommendations of Andrews and Bonta (2010), who cautioned against targeting noncriminogenic needs within interventions that target criminogenic needs. However, this focus on criminogenic needs differs from the approach and focus of traditional mental health services which typically target symptoms associated with mental illnesses.
The use of two facilitators for each intervention session in our TSDA also has implications for the delivery of interventions that target criminogenic needs to people with SMI. Initially, the role of the second facilitator focused on helping to provide one-on-one coaching during the role-play activities. However, the intervention team found having two facilitators present for each session optimized facilitators’ ability to engage all of the different targeted service delivery strategies that are needed to support the target population’s comprehension of intervention materials during the session. A second facilitator was also useful to deal with the differing skill levels among group members and to attend to group members who required additional active coaching and amplification of content. Thus, the second facilitator was recognized as a critical component of the successful implementation of the TSDA.
Limitations
The research conducted here benefited from the presence of funding that provided the resources needed to develop a coherent, stable, and clearly explicated set of therapeutic strategies that could be used to deliver interventions that target criminogenic needs to people with SMI. However, it is important to note that this research was designed to support the development of the TSDA, not to test the outcomes associated with the use of this TSDA or how such outcomes may vary across different groups (e.g., by demographic factor or psychiatric diagnosis). Therefore, no comparison group was used in this study and the results presented here cannot estimate the responsiveness of specific delivery strategies, nor can it estimate the interventions impact on outcomes such as criminal recidivism.
The TSDA presented here is designed for people with the most severe forms of mental illnesses (i.e., schizophrenia spectrum and major affective disorders), because these illnesses have a profound effect on individuals’ ability to engage interventions that address criminogenic needs. Research has shown that anywhere from 6% to 18% of individuals in jails and prison suffer from a SMI (Ditton, 1999; Steadman et al., 2009; Teplin, 1990) and that people with these illnesses face worse outcomes, such as longer periods of incarceration and increased recidivism rates (Cheng, Larsson, Lichtenstein, & Fazel, 2015; Cloyes, Wong, Latimer, & Abarca, 2010; Ditton, 1999); however, it is also important to note that these illnesses represent just one component of the behavioral health problems that people face in the criminal justice system. Therefore, future research needs to examine the specific responsivity issues associated with other behavioral health problems.
Future Research
The TSDA developed through this research has the potential to make the delivery of interventions that target criminogenic needs more responsive to the specific treatment and learning needs of people with SMI. However, these findings represent the earliest stage of intervention development (i.e., Stage 1a). Now that a stable and coherent set of targeted service delivery strategies have been developed and described here. Future research needs to examine the effectiveness of interventions using this TSDA on criminogenic needs and recidivism among justice-involved people with SMI. The description of the TSDA presented here and the methods used to develop them supports the next stage of research by disseminating this emerging practice in a timely fashion, which will help to facilitate more timely evaluations of the interventions impact in practice.
Conclusion
This article presents a TSDA designed to address the specific learning and treatment needs of people with SMI during the delivery of group-based CBT interventions that target criminogenic needs such as T4C. This TSDA adds to the literature on the development of effective interventions for justice-involved people with SMI by providing service strategies that support the use of interventions that target criminogenic needs with this population. This TSDA represents an important step forward in the development of interventions that target criminogenic needs for this population because it increases the chances that justice-involved people with SMI will be able to participate fully in and benefit from these interventions. The development of this TSDA builds on the increased attention that researchers, practitioners, and policy makers are giving to the RNR framework and its applicability to the development of treatment services for justice-involved people with SMI. The development of this framework comes at a critical time in the field in that it can inform efforts to incorporate interventions that target criminogenic needs into the continuum of services available to justice-involved people with SMI.
Footnotes
Acknowledgements
The authors acknowledge the work of the community partners as well as the group participants for their important roles in this effort.
Authors’ Note
The contents of this article are solely the responsibility of the authors and do not represent the official view of the Ohio Department of Mental Health and Addiction Services. Case Western Reserve University and the Northeast Ohio Medical University were research partners on this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Ohio Department of Mental Health and Addiction Services.