
Abstract
There is limited research investigating the relationship between dual diagnosis and drug court outcomes. The current study examines the relationship between dual diagnosis and drug court failure by specific failure type. Utilizing data from a large urban drug court in the Southwestern United States, the study finds mixed results regarding the impact of dual diagnosis on drug court failure. Specifically, while there was no evidence that dual diagnosis predicted overall success/failure, dual diagnosis significantly increased the odds of serious program failure (e.g., new offense, absconding, revocation). In contrast, dual diagnosis significantly decreased the odds of less serious failure (e.g., rule violation, relapse).
Introduction
The relationship between substance use and mental health problems is an interactive one. Those diagnosed with a mental illness have a high risk of substance use diagnosis, as those with a substance use diagnosis have a high risk of mental illness (Kessler, Chiu, Demler, & Walters, 2005). Individuals who are diagnosed with substance use disorders are estimated to be 4.5 times more likely to have a concurrent mental health diagnosis compared with individuals without substance use disorders (Jane-Llopis & Matytsina, 2006; Kessler et al., 1994; Reiger et al., 1990; Robins & Reiger, 1991). Estimates suggest that 7 to 10 million individuals show evidence of co-occurring disorders in the United States (U.S. Department of Health and Human Services, 2002). While both substance use and mental health disorders are prevalent in the general population, they are more frequent in individuals in the criminal justice system (Diamond, Holzer, Thomas, & des Cruser, 2001; Peters, Greenbaum, Edens, Carter, & Ortiz, 1998; Veysey & Bichler-Robertson, 2002).
A recent estimate found that 74% of state prisoners and 76% of jail inmates who had a mental health problem, defined as both a recent history or symptoms of a mental health problem and a clinical diagnosis or treatment by a mental health professional, were dependent on alcohol or drugs (Dorsey & Middleton, 2009). Furthermore, jail and state prison inmates with a mental health problem reported higher rates of drug use in the month before the offense compared with those without a mental health problem (Dorsey & Middleton, 2009). Offenders having both substance use and mental health problems present distinct challenges to the criminal justice system, as co-occurring disorders may affect criminal justice outcomes and recidivism (Mueser, Noordsy, Drake, & Fox, 2003). As dual diagnoses are commonplace in offending populations, it is necessary to assess which criminal justice programs have the greatest impact in terms of addressing treatment needs and improving criminal justice outcomes, particularly for a special group of offenders such as drug court participants.
Dually Diagnosed Offenders in the Criminal Justice System
Peters, Wexler, and Lurigio (2015) identify the reasons why dually diagnosed individuals are overrepresented in the criminal justice system. The authors note that much of the growth of the number of dually diagnosed individuals in criminal justice settings is due to the increased number of drug offenders, a population that has high rates of co-occurring mental illness (Lurigio & Swartz, 2000; Osher, 2013). In addition, the authors argue that dually diagnosed individuals also have increased rates of homelessness and criminogenic risk, which may negatively affect desistance from offending (Morgan, Fisher, Duan, Mandracchia, & Murray, 2010; Osher, 2013; Skeem, Nicholson, & Kregg, 2008), thus further entrenching them in offending behavior.
As the number of dually diagnosed offenders coming in contact with the criminal justice system has increased, increased attention has been given to the unique challenges of these offenders. Prior research has found that dually diagnosed offenders often require more treatment resources, and they pose a higher risk of recidivism than offenders without comorbid disorders. Mental health disorders are considerably higher in offenders with coexisting substance abuse disorders (Baillargeon, Binswanger, Penn, Williams, & Murray, 2009; Baillargeon, Hoge, & Penn, 2010; Balyakina et al., 2014; Minkoff, 2001). In addition, there is evidence that dually diagnosed offenders are more likely to be incarcerated for longer periods of time than offenders without co-occurring disorders (Council of State Governments, 2012).
In sum, dually diagnosed offenders represent a distinct group of offenders that pose specific challenges to criminal justice administrators. In addition, the criminal justice system often serves as a primary treatment provider for this population (Taxman, Perdoni, & Harrison, 2007). While not specifically designed for dually diagnosed offenders, drug courts have become common alternatives to incarceration and often provide treatment to individuals who suffer from not only substance abuse issues but also mental health problems.
The Drug Court Model
Drug courts are a common criminal justice intervention for substance-using offenders, with more than 2,000 drug courts operating nationwide (Marlowe, Huddleston, & Casebolt, 2006). Drug courts provide specialized treatment, case coordination, and more intensive monitoring of offenders with substance use histories, based on a model of therapeutic jurisprudence, that integrates therapeutic resources with traditional criminal justice case processing (Hora, 2002). Drug courts were initially developed as substance dependency courts, but now have grown to include other types of drug courts including tribal, driving while intoxicated (DWI), campus, reentry, veterans, and mental health courts (U.S. Department of Justice, 2018). There is a large body of research on the effectiveness of drug courts and substance use and recidivism outcomes. Results from several meta-analyses have found that drug treatment courts significantly reduce recidivism and subsequent drug use (Latimer, Morton-Bourgon, & Chrétein, 2006; Mitchell, Wilson, Eggers, & MacKenzie, 2012; Shaffer, 2011; Wilson, Mitchell, & MacKenzie, 2006). However, there is some evidence that drug courts may be more effective for certain typologies of offenders. For instance, prior research has found that drug courts may be more effective for nonviolent offenders (Mitchell et al., 2012; Shaffer, 2011). As the effectiveness of drug court may vary by offender characteristics, other characteristics such as dual diagnosis need further examination.
Dual Diagnosis and Drug Courts
As there is an established relationship between substance use and mental illness, it is expected that many drug court participants may also suffer from mental health problems (Belenko, 2001). The estimate of drug court participants with dual diagnosis ranges between 20% and 60% (Belenko, 2001; Cooper, 1997; Weitzel, Nochajski, Coffey, & Farrell, 2007).
One recent study examined the relationship between dual diagnosis and juvenile drug court outcomes. Manchak, Sullivan, Schweitzer, and Sullivan (2016) compared outcomes in drug court between juveniles with only a substance use diagnosis with juveniles with a comorbid disorder. Overall, the authors found that dually diagnosed juveniles had significantly worse criminal justice outcomes than juveniles with only a substance use diagnosis. However, the authors concluded that this relationship could be partially explained by the finding that dually diagnosed juveniles had more drug court violations, especially with regard to treatment noncompliance (Manchak et al., 2016).
Gray and Saum (2005) provide the most thorough examination into the relationship between dual diagnosis and drug court outcomes for adult offenders. This study explored outcomes for participants in a Delaware drug court (n = 449) and specifically investigated the relationship between mental health, gender, and drug court completion. Substance abuse was measured as the number of days a participant reported using his or her primary drug of choice in the month prior to program entry. Three mental health measures were included: (a) any self-reported feelings of depression in the past 30 days, (b) any self-reported feelings of anxiety in the past 30 days, and (c) having any prescription for psychological or emotional problems in the past 30 days. Gray and Saum (2005) found that both mental health measures of self-reported depression and being prescribed medication significantly decreased the odds of program completion.
More recently, Zettler (2018) examined whether or not dually diagnosed offenders were more likely to recidivate after drug court participation. The results of this study found mixed results, finding that dually diagnosed offenders were more likely to recidivate 6 months after court participation, but these effects were null at a 12-month follow-up. However, prior research has not examined whether or not dual diagnosis may affect specific type of drug court failure, beyond overall success or recidivism. This is an important area of inquiry, as it is possible that dual diagnosis may have varied effects on drug court success, depending how success and failure are operationalized.
Current Study
The current study seeks to contribute to the literature on the relationship between dual diagnoses and specific drug court outcomes by utilizing data from one urban drug court in the southwestern United States. The current study also utilizes more in-depth and detailed measures of both substance use and mental health problems, as well as official criminal history records. Specifically, the current research examines the following research questions:
Do dual diagnoses predict overall drug court failure?
Do dual diagnoses predict specific types of drug court failure (i.e., serious failure or less serious failure)?
Does primary diagnosis predict overall drug court failure?
Does primary diagnosis predict specific types of drug court failure (i.e., serious failure or less serious failure)?
Method
Data
The study relies on secondary data provided by one large Community Supervision and Corrections Department (CSCD) in an urban, southwestern county. The study sample included all adult probationers who participated in one adult drug court operated between July 2010 and April 2014 (n = 1,659). The drug court is a post-adjudication reentry court that integrates therapeutic judicial oversight, individualized aftercare treatment, and collaborative case management. Drug court participants are assigned to the program after having successfully completed 6 months of inpatient treatment at a judicial treatment facility. To be eligible for the drug court, participants must have been on felony probation and had at least one Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) substance use diagnosis at the time of program admittance. The length of the drug court program ranges from 12 to 18 months. In the current study, a little over half of participants were on probation for a drug-related offense (n = 915). The drug court examined encourages participant sobriety through outpatient treatment, individual counseling, 12-step programming, and probation supervision.
Probationers were assigned to the drug court after successfully completing 6 months of inpatient substance abuse treatment. In addition, all participants received an in-depth clinical assessment prior to entering the inpatient treatment center. Court participants were administered a mental health screening questionnaire developed by CSCD Comprehensive Assessment and Treatment Services (CATS) Unit. The questionnaire was given to probationers to screen for potential mental health problems. 1 If participants screened positive for mental health symptoms reported in the past 30 days, 2 they were referred to clinicians, ranging from Licensed Professional Counselors (LPC), Licensed Chemical Dependency Counselors (LCDC), Licensed Master Social Worker (LMSW), and Licensed Clinical Social Worker (LCSW), 3 employed by the CSCD for a full clinical assessment of their mental health symptoms.
Measures
Substance use diagnostic procedure
Participants’ substance use diagnoses were made using the TCU Drug Screen II (TCUDS II) Instrument. The TCUDS II is a self-administered 15-item questionnaire designed to identify individuals with a history of heavy drug use or dependency based on DSM-IV diagnostic categories (Institute of Behavioral Research, 2007). The instrument is scored to produce a single total score ranging from 0 to 9. Total score values of 3 or greater indicate relatively severe drug-related problems and correspond approximately to DSM-IV drug dependence diagnoses (Institute of Behavioral Research, 2007). The instrument follows DSM protocol by focusing on patterns of drug use, recurring consequences, and symptoms of withdrawal (Institute of Behavioral Research, 2007). The TCUDS Instrument has been widely used and validated in a variety of correctional populations (see Baillargeon, Penn, et al., 2010; Broome, Knight, Joe, & Simpson, 1996; Houser & Belenko, 2015; Knight, Simpson, & Morey, 2002; Peters et al., 2000). In addition, evaluations of the TCUDS II conclude that the instrument provides acceptable reliability and validity in making substance use diagnoses.
In a study by Peters and colleagues (2000), eight different substance use screening instruments were compared against the Structured Clinical Interview for DSM-IV (SCID-IV) and their utility in making substance use diagnoses. Specifically, the TCUDS was found to be highly reliable over time (r = .95). In addition, the instrument rendered high positive predictive values (82%), specificity (92%), and sensitivity (70%). Peters and colleagues (2000) also found that the instrument was highly accurate in identifying substance-dependent inmates while limiting nondependent inmates (i.e., reducing the number of false positives).
Furthermore, the TCUDS Instrument has been evaluated by examining the internal consistency of the first nine items that are used to make the composite score (Knight, Simpson, & Morey, 2002). Overall, the evaluation found that the scale’s overall reliability was good (α = .89) and reliability coefficients were nearly identical across various racial and demographic subgroups. The results of the evaluations and validation studies suggest that the TCUDS II instrument used in the current study provides both reliable and valid measures of substance use problems.
Mental health diagnostic procedure
Court participants are also administered a mental health screening questionnaire developed by the CATS Unit. The questionnaire is given to probationers to screen for potential mental health problems. 4 If participants screen positive for symptoms reported in the past 30 days and not due entirely to substance use, health problems, incarceration/legal problems, or criminal activities, then they are referred to a clinician employed by the CSCD for a full clinical assessment of their mental health symptoms.
Axis I disorders were obtained using the Structured Clinical Interview for DSM-IV (SCID-I). The SCID-I is a widely used semi-structured assessment for identifying Axis I clinical disorders (First et al., 1994). Several studies have evaluated the inter-rater reliability of the DSM-IV SCID-I and found high inter-rater agreement (Lobbestael, Leurgans, & Arntz, 2011; Zanarini & Frankenburg, 2001; Zanarini et al., 2000).
Personality diagnoses were elaborated using the Minnesota Multiphasic Personality Inventory–2 (MMPI-2). The MMPI and its revised forms, the MMPI-2, MMPI-A, and MMPI-2 Restructured, are the most widely used objective personality assessment inventories in the world, particularly in a number of correctional samples to make mental health diagnoses (see Black et al., 2004; Edens, Cruise, & Buffington-Vollum, 2001; Edens, Hart, Johnson, Johnson, & Olver, 2000; Megargee, Mercer, & Carbonell, 1999).
Within criminal justice, these instruments have also been utilized in drug court and substance use treatment evaluations. Specifically, the MMPI-2 and MMPI-2 Restructured form scales have been used to identify those who are unlikely to complete a substance use diversionary treatment program, and the ability of the particular instruments, such as the Behavioral/Externalizing Dysfunction (BXD), Restructured Clinical Scale (RC4), Juvenile Conduct Problems (JCP), Aggressiveness (AGG), and Disconstraint–Revised (DISC-r) scales, was also associated with the failure to complete drug court (Mattson, Powers, Halfaker, Akeson, & Ben-Porath, 2012; O’Reilly, 2007).
While there is no “gold standard” to assess the validity of diagnostic measures, generally the validity of psychiatric diagnoses has often been assessed using the “LEAD” standard (Spitzer, 1983). This standard developed by Spitzer (1983) includes using longitudinal data collected over time (L), conducted by expert diagnosticians (E), and using all subject data available, including observational data, medical records, and family reports (AD). Prior to entry to the drug court, clinicians gathered information from offenders’ risk/needs assessments, criminal history, jail incident reports, and court documentation when making the DSM-IV diagnoses, thus improving the validity of the diagnostic measures. In addition, the SCID-I has been identified as a “gold standard” in obtaining clinical diagnoses in both substance-using individuals and community samples (Kranzler, Kadden, Babor, Tennen, & Rounsaville, 1996; Kranzler et al., 1995; Shear et al., 2000).
Diagnostic Measures
The DSM-IV diagnoses in these data were collapsed into more general categories (for similar approaches, see Compton, Thomas, Stinson, & Grant, 2007; Grant et al., 2004; Hasin et al., 2006; Kessler et al., 2005). The DSM-IV substance use diagnostic categories represented in the sample include alcohol (n = 574), cannabis (n = 583), cocaine (n = 507), amphetamine (n = 316), and opioid (n = 179). In addition, an “other substance” category (n = 182) included other substance use diagnoses (i.e., hallucinogen, inhalant, phencyclidine, xanax, sedative, and polysubstance 5 ) or cases missing information regarding the specific diagnosis. It is important to note that all of the court participants have at least one substance use diagnosis, thus rendering them eligible for program participation (n = 1,659).
The DSM-IV mental health diagnoses represented in the sample include adjustment (n = 31), anxiety (n = 17), bipolar (n = 47), depressive (n = 150), and an “other mental health diagnosis” category (n = 154) that included diagnoses such as antisocial personality disorder, adult antisocial behavior, borderline intellectual functioning, psychotic disorders, and noncompliance with treatment. Table 1 provides the full list of mental health diagnoses present in the sample. Each diagnostic category was coded as a series of dichotomous variables (1 = any diagnosis, 0 = no diagnosis) for each individual in these data. After identifying the various diagnoses within these data, a dummy variable was created to identify the participants who have at least one mental health diagnosis alongside at least one substance use diagnosis (1 = dual diagnosis, 0 = no dual diagnosis). Approximately 23% (n = 399) of participants in these data had any dual diagnosis. Next, a dichotomous variable measuring primary diagnosis was created for participants who had a primary diagnosis reported in these data (n = 1,226). A measure Primary Substance Use Diagnosis was coded as follows: 1 = primary substance use diagnosis and 0 = primary mental health diagnosis. Of those with a primary diagnosis, 76% had a primary substance use diagnosis (n = 956) and 23% had a primary mental health diagnosis (n = 291).
Categories of Mental Health Diagnoses (Collapsed).

Note. DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994)
Outcome Variables
An outcome variable labeled Overall Failure was included to identify whether probationers completed the drug court program, defined as successful graduation from the program (1 = failure, 0 = successful completion). 6 Overall failures include probationers who did not complete the program due to program violation, relapse, absconder status, revocation, or committing a new offense. Next, type of program failure was collapsed into two categories: serious violation failure and less serious violation failure (for a similar approach, see Iratzoqui & Metcalfe, 2016). Serious program failure included all participants who failed to complete the program due to committing a new offense, absconding from supervision, or having their probation revoked (1 = serious program failure). About 21% of participants failed to complete the program due to a serious violation failure (n = 348). 7 The second failure category, less serious violation failure, included all participants who failed to complete the program due to a rule violation (e.g., failure to complete counseling requirements) or relapsing (1 = less serious failure). 8 Of the sample, 28% of participants (n = 463) failed to complete the drug court program due to a less serious violation. The final failure type variable used in the analyses examined whether participants who failed drug court had either a less serious (= 0) or serious (= 1) program failure.
Demographic and Probation Variables
Several demographic and supervision related variables were included as control variables related to court outcomes. Table 2 reports descriptive statistics for the entire sample. Table 3 provides means of sample characteristics, comparing differences between participants with and without dual diagnoses. Participants with dual diagnoses in the sample were significantly more likely to be younger (t = 2.29, p < .05), female (χ2 = 17.03, p < .001), non-Hispanic (χ2 = 17.89, p < .001), more likely to be on probation for a property (χ2 = 22.27, p < .001), less likely to be on probation for a DWI offense (χ2 = 6.27, p < .05), more likely to be failures due to absconding (χ2 = 5.46, p < .05), and less likely to be failures due to a program violation (χ2 = 5.85, p < .05).
Descriptive Statistics for All Drug Court Participants (n = 1,659).

Note. DWI = driving while intoxicated.
Sample Means for Participants by Diagnosis Type (n = 1,659).

Note. DWI = driving while intoxicated.
p < .05. **p < .01.
As there is evidence that age is related to drug court completion (Jaffe, Du, Huang, & Hser, 2012; Peters & Murrin, 2000), a continuous measure of age (in years) was included as a control variable. Several studies have concluded that gender is related to court completion; thus, it is necessary to control for gender in the analyses (Gray & Saum, 2005; Jaffe et al., 2012; Peters & Murrin, 2000; Taxman, 1999). Gender was coded as a dichotomous variable (1 = male, 0 = female).
As Sechrest and Shicor (2001) note, there is evidence that race might affect the likelihood of court completion, with Whites more likely to successfully complete the program. Race was coded as a pair of binary variables coded as (1 = White, 0 = Black) and (1 = Hispanic, 0 = non-Hispanic). At least one study examined marital status as a predictor of court outcomes, finding that marital status was positively correlated with drug court success (Miller & Schutt, 2001), while research on dual diagnoses has found that marriage and cohabitating relationships are associated with reductions in drug and alcohol use. Marital status was coded as a dichotomous variable (1 = married, 0 = not married).
In addition, several research efforts have found that employment is related to drug court outcomes, where being employed increases the likelihood of success (Butzin, Saum, & Scarpitti, 2002; Mateyoke-Scrivner, Webster, Staton, & Leukefeld, 2004; Roll, Prendergast, Richardson, Burdon, & Ramirez, 2009). Thus, a measure of employment at the time of program start was included (1 = employed, 0 = unemployed). Furthermore, as studies have found that education level may be positively correlated with drug court success (Butzin et al., 2002; Gray & Saum, 2005), level of education was included and was measured categorically (0 = no HS or equivalent degree, 1= completed HS/equivalent degree or some college, 2 = college degree or higher).
A variable measuring supervision level was coded as a series of dichotomous variables for each supervision level (Maximum, Medium, and Minimum). These variables indicate the level of supervision prior to entering drug court, which is calculated using risk/needs scores from the Level of Service Inventory–Revised (LSI-R). This measure was included as a meta-analysis of predictors of adult recidivism found that the LSI-R was the most useful instrument in predicting recidivism (Gendreau, Little, & Goggin, 1996). A study by Merrill, Alterman, Cacciola, and Rutherford (1999) found that among inpatient substance users, those who had more prior drug treatment were less likely to be arrested following treatment. A binary variable measuring prior drug treatment was included (1 = prior drug treatment, 0 = no prior drug treatment).
As there is evidence that treatment duration may be related to justice outcomes (see Banks & Gottfredson, 2004; Belenko, 1998; Finigan, 1998; Goldkamp, White, & Robinson, 2001; Peters, Haas, & Hunt, 2001; Peters & Murrin, 1998), treatment exposure was measured as the number of days that the probationer was in the drug court program before completion/failure. However, it is important to note that time spent in treatment may not reflect the quality of treatment, which is a noted limitation of this measure (Bouffard & Taxman, 2004). Furthermore, there is evidence that drug use severity may be predictive of drug court outcomes, as offenders with more severe drug use are less likely to be successful in drug court programs (Butzin et al., 2002; Jaffe et al., 2012). As a proxy measure of drug use severity, a variable labeled UA fail rate was considered to identify the rate of failed urinalysis prior to court participation and was measured as No. of Positive UAs/Total Number of UAs. 9
In addition, there is empirical support that particular types of offenders may be less successful in drug court programs, especially violent offenders (Jaffe et al., 2012; Mitchell et al., 2012; Saum, Scarpitti, & Robbins, 2001). The offense type that the participant was on probation for was considered as a series of categorical variables. The offense categories in these data include drug offenses, property offense, person offenses, DWI offenses, and “other” offenses that were not classified as one of the specified categories. Each of these offense categories was measured as a dichotomous variable (e.g., 1 = drug offense, 0 = no drug offense).
Criminal History Variables
One of the most robust predictors of drug court success and recidivism is prior criminal history (Gendreau et al., 1996; Saum et al., 2001). Multiple criminal history variables were included in the analyses using data acquired from the Texas Department of Public Safety. A variable measuring the total number of arrests was coded as the number of arrests that a probationer had on file with the Texas Department of Public Safety prior to starting drug court. Variables measuring the number of person, property, and drug-related arrests that a probationer had on file prior to starting drug court were considered in the analyses. 10
Analytical Plan
A series of logistic regression models were estimated to assess the relationship between dual diagnosis, overall failure, and specific type of court failure. Prior to analyses, bivariate correlations were examined, and no issues of multicollinearity were found. The first model used a logistic regression model including all available control variables. Next, logistic regression models were estimated with failure type as the outcome.
Results
Question 1: Do Dual Diagnoses Predict Overall Drug Court Failure?
A logistic regression model was estimated using overall failure as the dependent variable to examine whether dual diagnosis predicts any type of drug court failure. Table 4 reports the results from the logistic regression model, reported in odds ratios (ORs). As indicated in the table below, the key independent variable of interest, dual diagnosis, did not significantly predict completion of the drug court. Factors that increased the odds of program failure included being male (OR = 1.450, p = .020), Hispanic (OR = 1.507, p = .033), maximum supervision level (OR = 6.588, p < .001), prior drug treatment (OR = 1.427, p = .011), and higher UA failure rate (OR = 1.324, p < .001). There were also several variables that lowered the odds of program failure, including being younger (OR = 0.999, p < .001), being employed (OR = 0.392, p < .001), and spending more time in treatment (OR = 0.996, p < .001).
Logistic Regression of Predictors of Overall Drug Court Failure (n = 1,659).
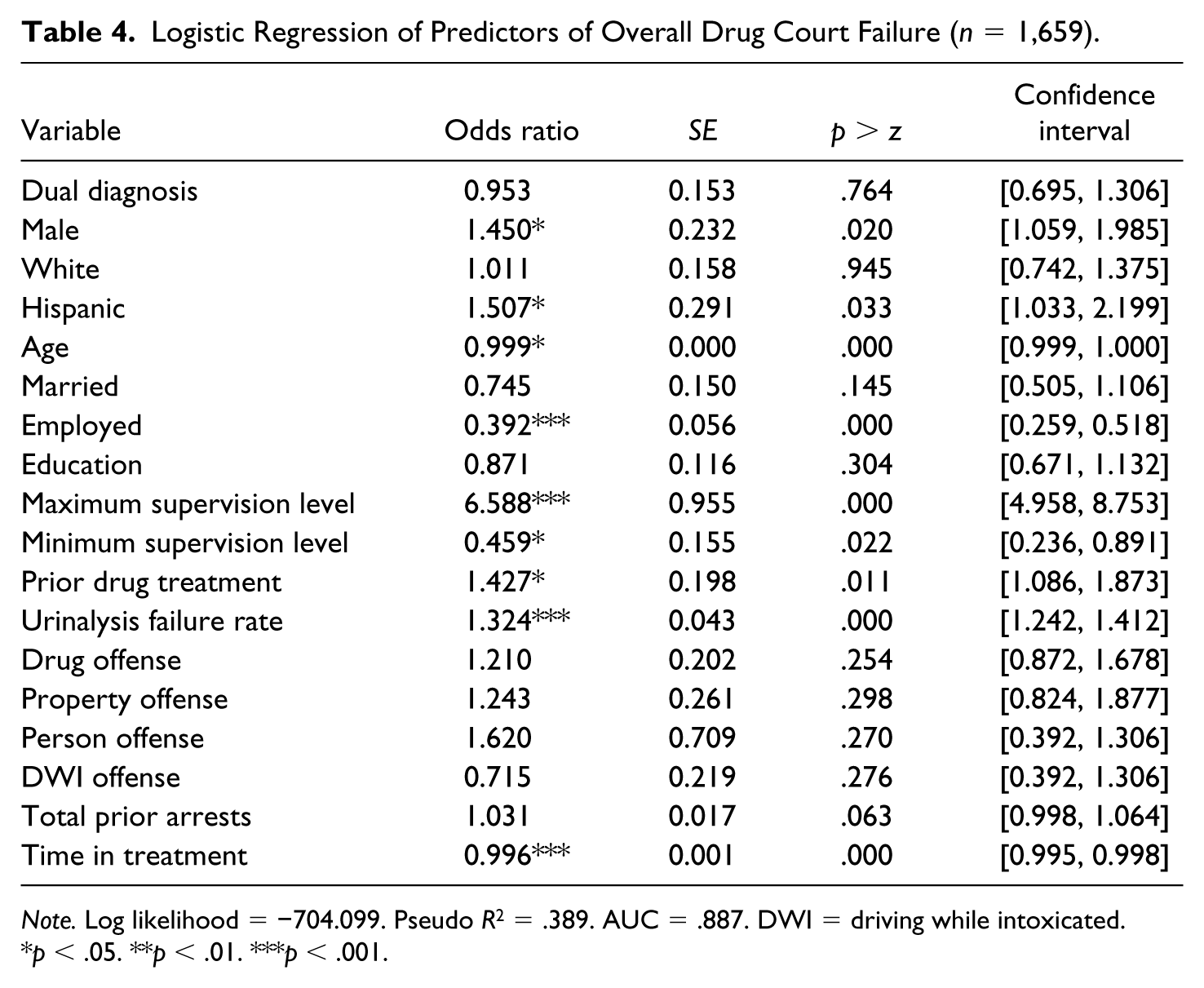
Note. Log likelihood = −704.099. Pseudo R2 = .389. AUC = .887. DWI = driving while intoxicated.
p < .05. **p < .01. ***p < .001.
Question 2: Do Dual Diagnoses Predict Type of Court Failure?
First, a logistic regression model predicting serious court failures (i.e., new offense, revocation, and absconders) was estimated. Table 5 provides the results of serious drug court failure, reported in ORs. The key independent variable, dual diagnosis, significantly increased the odds of serious drug court failure (OR = 1.834, p < .001). Other factors that increased the odds of serious failure were maximum supervision level (OR = 4.186, p < .001), prior drug treatment (OR = 1.352, p = .033), and having a higher number of prior arrests (OR = 1.045, p = .005). Predictors that reduced the odds of serious failure included being older (OR = 0.999, p < .001) and spending more time in the drug court program (OR = 0.994, p < .001).
Logistic Regression of Predictors of Serious Drug Court Failure (n = 1,508).
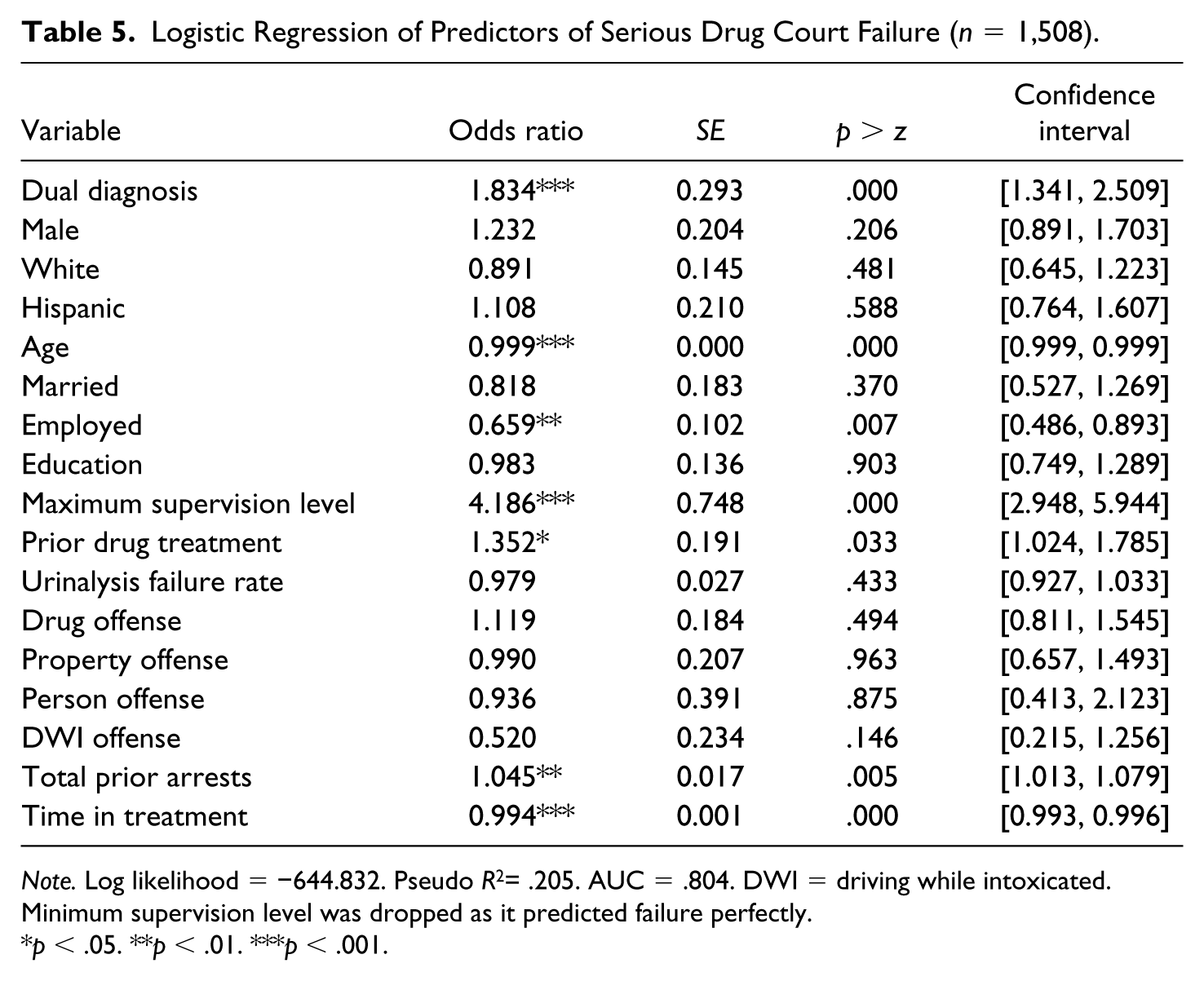
Note. Log likelihood = −644.832. Pseudo R2= .205. AUC = .804. DWI = driving while intoxicated.
Minimum supervision level was dropped as it predicted failure perfectly.
p < .05. **p < .01. ***p < .001.
Next, a logistic regression model predicting less serious court failure (i.e., relapse, program violation) was estimated. The results of this model are provided in Table 6. The key independent variable, dual diagnosis, significantly reduced the odds of less serious failure (OR = .599, p = .001). Being supervised at a maximum supervision level (OR =2.507, p < .001) and having a higher UA failure rate (OR = 1.228, p < .001) increased the odds of less serious failure, whereas being employed reduced the odds of less serious failure (OR = 0.622, p < .001).
Logistic Regression of Predictors of Less Serious Drug Court Failure (n = 1,659).

Note. Log likelihood = −846.808. Pseudo R2 = .138. AUC = .754. DWI = driving while intoxicated.
p < .05. **p < .01. ***p < .001.
Question 3: Does Primary Diagnosis Predict Overall Drug Court Failure?
A logistic regression analysis examined whether primary diagnosis predicted overall drug court failure. The results of the model are reported in Table 7. The key independent variable, Primary Substance Use Diagnosis, did not significantly affect the odds of overall court failure. Being supervised at a maximum supervision level (OR = 2.977, p < .001), total prior arrests (OR = 1.045, p < .05), and having a higher UA failure rate (OR = 1.021, p < .001) increased the odds of overall court failure, while time in treatment reduced the odds of overall court failure (OR = .997, p < .001).
Logistic Regression of Predictors of Overall Court Failure by Primary Diagnosis Type (n = 1,226).

Note. Log likelihood = −520.786. Pseudo R2 = .386. AUC = .885. DWI = driving while intoxicated.
p < .05. **p < .01. ***p < .001.
Question 4: Does Primary Diagnosis Predict Specific Types of Drug Court Failure?
Next, a model predicting serious court failure by primary diagnosis was estimated. The results are reported in Table 8. The analysis found that having a primary substance use diagnosis, as compared with having a primary mental health diagnosis, significantly decreased the odds of serious court failure (OR = .480, p <. 001). Furthermore, this model found that maximum supervision level (OR = 5.226, p < .001) and prior drug treatment (OR = 1.403, p < .05) significantly increased the odds of serious failure. In contrast, being older (OR = .976, p < .05), employed (OR = 0.584, p < .01), and time in treatment (OR = .995, p < .001) significantly decreased the odds of serious failure.
Logistic Regression of Predictors of Serious Court Failure by Primary Diagnosis Type (n = 1,112).
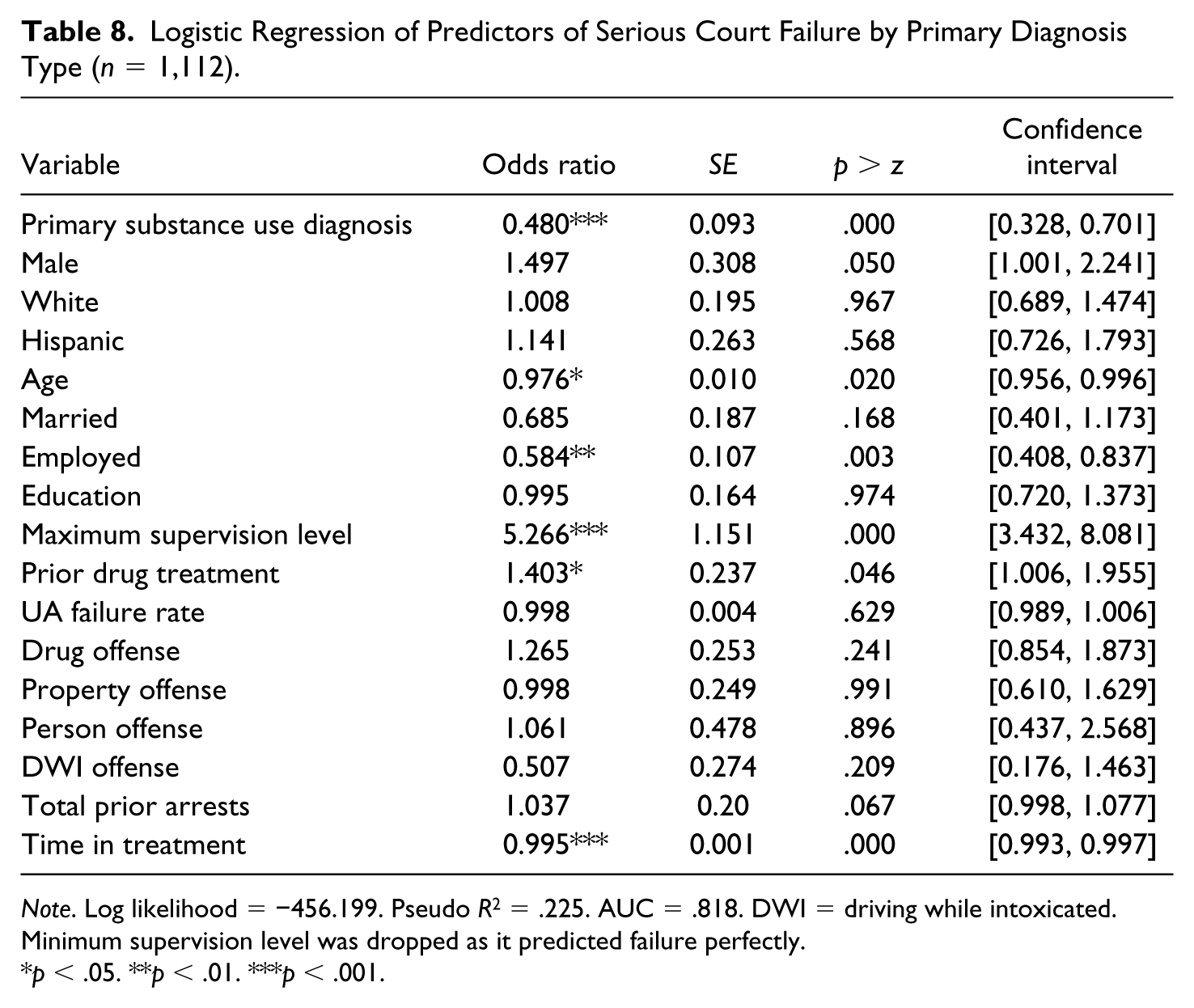
Note. Log likelihood = −456.199. Pseudo R2 = .225. AUC = .818. DWI = driving while intoxicated.
Minimum supervision level was dropped as it predicted failure perfectly.
p < .05. **p < .01. ***p < .001.
Finally, Table 9 reports the results of a model predicting the impact of primary diagnosis on less serious failure. Primary substance use diagnosis increased the odds of less serious failure in the sample (OR = 1.433, p < .05). Furthermore, maximum supervision level (OR = 2.977, p < .001), and UA failure rate (OR = 1.021, p < .001) also increased the odds of less serious failure. No factors were significant in reducing the odds of less serious failure.
Logistic Regression of Predictors of Less Serious Court Failure by Primary Diagnosis Type (n = 1,226).
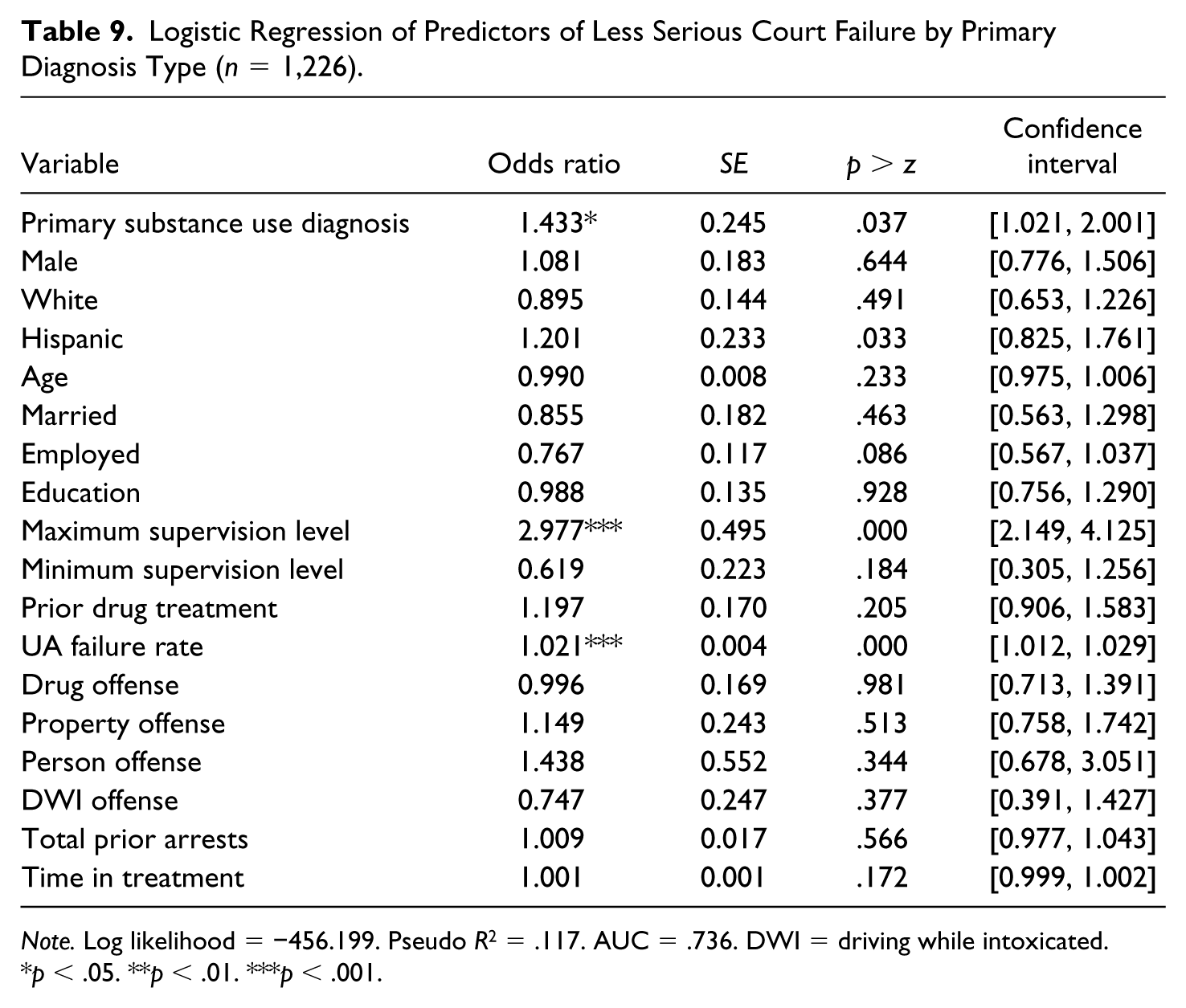
Note. Log likelihood = −456.199. Pseudo R2 = .117. AUC = .736. DWI = driving while intoxicated.
p < .05. **p < .01. ***p < .001.
Discussion
The purpose of the current research was to examine whether dually diagnosed drug court participants have similar program outcomes as participants with only substance abuse diagnoses. While a limited number of prior studies have found that dual diagnoses are related to drug court success, the current study is among the first to examine how dual diagnoses may predict specific types of drug court failure. Contrary to the prior research, no evidence was found that dual diagnoses were predictive of overall failure of the program. The results also identify that several demographic and criminal history factors may be more predictive of failure, including supervision level, attending prior drug treatment, and drug use severity.
With regard to specific court outcomes, dual diagnosis had varying effects. Dual diagnosis increased the odds of serious failure, while it decreased the odds of less serious failure. This is important, as it illustrates that collapsing all failures in one category may be masking the heterogeneity of court outcomes. The results of the analyses suggest that dual diagnosis may have an impact on the more serious types of program failure, including committing a new offense, absconding, and being revoked. Furthermore, the analyses found that individuals who have primary mental health diagnoses were more likely to have serious court failure, while those with primary substance use diagnoses were more likely to have less serious failures. This is an interesting finding that warrants more attention, as it reflects the heterogeneous nature of drug court participants who also suffer from mental health problems. This may be of great importance to court administrators and probation staff, as these offenders may require more treatment and supervision resources to prevent these more serious failures that pose a risk to public safety.
Across all but one model, employment reduced the odds of drug court failure. This finding reflects the large body of research on the theoretical framework that argues that informal social controls, including employment, may serve as “turning points” that encourage desistance from crime (see, for example, Laub & Sampson, 2001; Sampson & Laub, 1993). Prior research has also found that both substance use and mental illness are linked to unemployment (Swartz, Lurigio, & Goldstein, 2000), and that employment rates are generally lower among dually diagnosed individuals (Laudet, Magura, Vogel, & Knight, 2002). In a sample of 130 dually diagnosed individuals receiving vocational services, Laudet and colleagues (2002) found that participants expressed both high interest in working and multiple obstacles in gaining and maintaining employment. Thus, prior research and the findings of the current study suggest that employment may serve as a protective factor in the drug court context for both dually diagnosed individuals and those with substance use disorders, and it may help foster desistance from both drug use and other drug court failure.
As noted by Redlich, Steadman, Monahan, Petrila, and Griffin (2005), it is unknown whether specialty courts that contain dually diagnosed offenders are different from courts that do not include offenders with both disorders. This is an important issue in need of further research, to assess whether dually diagnosed offenders are treated more or less punitively than drug courts without this group of offenders. If dually diagnosed offenders are treated more punitively, this could potentially affect the court outcomes for such offenders. Furthermore, whereas drug courts promote therapeutic effects through honesty by frequent alcohol and drug testing (Hora, 2002), dually diagnosed offenders may also need to be held accountable with regard to mental health problems. As such, these offenders may need medication monitoring and psychotherapy in addition to drug testing.
As drug courts become more prevalent, the number of dually diagnosed offenders placed in such programs also increases (Lurigio & Snowden, 2009). Some jurisdictions have adopted the view that dually diagnosed offenders may be better suited in courts specifically designed for this group of offenders. These court programs integrate both mental health and substance use treatment at the same time and are designed to target the needs of dually diagnosed offenders. For example, mental health courts in Santa Clara and Orange County, California, specifically focus on co-occurring mental health and substance use disorders (Redlich et al., 2005). Other jurisdictions have developed mental health tracks within their drug courts, including Honolulu, Ithaca, New York, and Lane County, Oregon (Lurigio & Snowden, 2009). However, evaluations of specific dual diagnosis courts are not yet available. Future empirical investigations should examine court outcomes for offenders that are placed in courts specifically designed for dual diagnosis offenders, as well as modified court programs including mental health tracks.
While the current research provides an important exploration into the role that dual diagnoses play in drug court outcomes, it is not without its limitations. First, the results of the analyses reflect one drug court in one jurisdiction in the southwestern United States, which represents a large diverse urban area. As such, the specific results are not generalizable beyond these court participants. However, the research provides an initial exploration into this issue, providing a platform for future studies in other jurisdictions.
Prior research has noted the variation and the difficulty in defining comorbid disorders, as studies may define comorbidity in a number of ways. Comorbidity can occur when a substance use disorder is chronologically primary and dominant, underlined by at least one psychiatric diagnosis, and also can be in the form of at least one psychiatric disorder underlined by a substance misuse disorder (Schuckit, 2006; Todd et al., 2004). As noted by Franey and Quirk (1996), dually diagnosed individuals are heterogeneous and present a number of pathways in the development of these diagnoses. In addition, some definitions of dual diagnoses take into consideration lifetime prevalence, while others consider a time-limited or service year of the presence of such disorders. As Todd and colleagues (2004) highlight, taking a lifetime measure of comorbidity may overinflate prevalence figures, while only measuring disorders in a time-limited fashion may produce artificially low numbers. Thus, it is necessary that research on the presence of dual diagnoses in drug court takes into considerations the operationalization and diagnostic procedures utilized in such samples.
Furthermore, the data do not include the nature or severity of mental illness and substance use disorders in the sample. This limitation may mask the heterogeneity of this offending population, as individuals with severe mental health problems and minor substance use problems have different outcomes than individuals with severe substance use problems and minor mental health problems. As noted by prior research, it may be that offenders with high severity mental health problems and low substance use problems are better suited for placement in mental health court programs (NASMHPD & NASADAD, 1999). Contrastingly, individuals with high severity substance use problems and low mental health problems may be better suited for drug court programs. Furthermore, individuals who have both high severity mental health and substance use problems may be best suited for court programs specifically for dually diagnosed offenders (NASMHPD & NASADAD, 1999). Future research is necessary to assess which court programs serve specific subgroups of dually diagnosed offenders better than others.
Moreover, these data do not provide specific information regarding the treatment resources received by dually diagnosed offenders following program participation. Although the drug court in the current study employed full mental health assessments, there is no information in the current data regarding the nature of the mental health services received after assessment. It is possible that the drug court was not equipped with the resources necessary to provide services for participants who suffered from both mental health and substance use problems. Prior research has demonstrated that the most effective services for dually diagnosed individuals are comprehensive and simultaneously address substance use and mental health, rather than providing separate services that can lead to structural discrimination and an increased likelihood of failure (Schuckit, 2006). 11 This information is needed to understand the finding that dual diagnosis increased the odds of serious failures and decreased the odds of less serious failures. It is plausible that while in drug court, these offenders receive more intensive treatment and resources than other participants. Future research should investigate treatment programming provided to dually diagnosed participants that may help to explain these results.
Finally, it is important to clarify that the current research is not a process evaluation of the drug court program. Thus, questions of treatment efficacy and fidelity are not able to be assessed using the current data. As such, participation and recidivism outcomes could be related to how well the drug court is actually delivering services and following implementation guidelines.
To date, there have been few investigations into how dual diagnoses affect drug court outcomes. The current study provides a more detailed exploration into the relationship between dual diagnosis and specific drug court outcomes. Overall, the current study provides evidence that dual diagnoses may differentially affect specific drug court outcomes. Future research is needed to examine whether these findings are substantiated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.