
Abstract
Individuals who have committed sex offenses (ISOs) with severe mental illnesses are a complex population to serve and more research is needed to guide practice and policy, especially around community supervision, enrollment in Medicaid, housing, employment, criminal justice contacts, and reincarceration after prison reentry. To further the literature in this area, we used logistic regression to model recidivism and admissions to violator or prison facilities among 127 ISOs with severe mental illnesses and 2,935 people with severe mental illnesses who were incarcerated in prison for other crimes. Compared to prison releasees with severe mental illnesses who committed crimes other than sex offenses, prison releasees with severe mental illnesses who committed sex offenses were admitted to violator facilities at higher rates, when controlling for substance use, Medicaid enrollment, homelessness, and unemployment. Implications for practice, policy and research are discussed.
Introduction
People with severe mental illnesses in the criminal justice system are a significant challenge to mental health and criminal justice authorities around the country. In particular, individuals with severe mental illnesses who are released from prison recidivate more often than offenders without mental illnesses (Baillargeon, Binswanger, Penn, Williams, & Murray, 2009; Baillargeon et al., 2010; Cloyes, Wong, Latimer, & Abarca, 2010; Hartwell, 2004; Jacoby & Kozie-Peak, 1997; Lovell, Gagliardi, & Peterson, 2002; Messina, Burdon, Hagopian, & Prendergast, 2004; Silver, Cohen, & Spodak, 1989) and have difficulty accessing housing, supported employment opportunities, and health and behavioral health services (Draine, Salzer, Culhane, & Hadley, 2002; Fisher et al., 2007; Lovell et al., 2002; Mallik-Kane & Visher, 2008). Moreover, offenders with severe mental illnesses who are convicted of sex offenses are of considerable concern to the public, and to legal, psychiatric, and sex offender treatment communities (Alish et al., 2007).
Individuals convicted of sex offenses (ISOs) have been found to have sexual recidivism rates between 13% and 19%, (Hanson, Bourgon, Helmus, & Hodgson, 2009; Hanson & Bussiere, 1998). With respect to those convicted of other crimes, recidivism among the general population of offenders is around 60% and slightly higher for offenders with severe mental illnesses (65%-68%; Cloyes et al., 2010; Langan & Levin, 2002; Wilson, Draine, Hadley, Metraux, & Evans, 2011). Compared to offenders with severe mental illnesses, however, ISOs with severe mental illnesses may experience greater community reentry difficulties, as these offenders present complex challenges to mental health providers, sex offender treatment providers, and probation or parole officers who are responsible for their community supervision (Alish et al., 2007; Grossman, Martis, & Fichtner, 1999; Harris, Fisher, Veysey, Ragusa, & Lurigio, 2010; Rotter, 2007).
It is important to note that mental illness is not one of the eight risk factors for recidivism as identified by Bonta, Blais, and Wilson (2014) who contend that these risk factors are similar for mentally ill and non-mentally ill offenders. Also, there is consensus in the literature, with one exception, that mental illness is not related to sexual recidivism among ISOs (Mann, Hanson, & Thornton, 2010). Nevertheless, people with severe mental illnesses who are convicted of sex offenses face multiple stigmas (i.e., stigmas associated with having a mental illness, having a felony record, and being labeled a sex offender), and these multiple stigmas are likely to present especially difficult community reentry challenges (McGrath, Cumming, & Holt, 2002; Novak, McDermott, Scott, & Guillory, 2007; Zezima, 2008 February 18).
Furthermore, state laws prohibiting ISOs from being near localities where children might be could prevent offenders with severe mental illnesses convicted of sex offenses from receiving mental health services if programs are located in restricted areas (Zezima, 2008). To further exacerbate matters, poor collaboration among criminal justice, behavioral health and sex offender treatment systems could make it more difficult for offenders with severe mental illnesses convicted of sex offenses to access treatment and understand and comply with the requirements of probation or parole (Alish et al., 2007; Grossman et al., 1999; Novak et al., 2007; Rotter, 2007). Indeed, probation and parole officers who supervise ISOs report difficulties finding their parolees housing, problems with getting timely information, and pressure from superiors because of the high-profile nature of their parolees (Zevitz & Farkas, 2000).
Research has yet to establish whether these complex reentry challenges result in especially poor community reentry outcomes (e.g., homelessness, unemployment, criminal justice contacts) among offenders with severe mental illnesses convicted of sex offenses (Alden, Brennan, Hodgins, & Mednick, 2007; Harris et al., 2010). Moreover, to date, the literature lacks a head-to-head comparison of the reentry outcomes among offenders with severe mental illnesses convicted of sex offenses and offenders with severe mental illnesses convicted of other crimes. Specifically, to what extent does the added complexity of a sex offense exacerbate post-release challenges for a population that already has poor reentry outcomes? Given offenders with mental illnesses already have difficult post-release experiences, it is likely that post-release reentry outcomes are further compromised by a conviction of a sex offense, which sex offense, which often means with an additional system to navigate, stricter parole requirements, and additional stigma.
To address these gaps in our knowledge, we used population-based data linked across multiple public sectors (i.e., prison, mental health, Medicaid, statewide arrest data) from Washington State to compare reentry outcomes and criminal justice contacts of offenders with severe mental illnesses convicted of sex offenses and offenders with severe mental illnesses convicted of other crimes. The study protocol was approved by the Institutional Review Boards at the University of North Carolina at Chapel Hill and the Washington State Department of Social and Health Services.
Method
Design and Data
A longitudinal, observational study design and statewide administrative data from multiple public sectors in Washington State (i.e., criminal justice, mental health, Medicaid) over multiple years (2006-2010) were used to examine recidivism among offenders who were released from prison. Offenders with severe mental illnesses who were convicted of sex offenses and offenders with severe mental illnesses who were convicted of other crimes who were released from prison in 2006 or 2007 were tracked over a 3-year post-release period.
The data used for this study were assembled by the Research and Data Analysis Division of Washington State’s Department of Social and Health Services, which maintains a statewide client services and outcomes database. This database includes demographic and clinical information with service utilization records from 16 different state data systems. Data were arranged in a longitudinal, person-month data file of behavioral health services, hospitalizations, wages, homelessness, and criminal justice contacts. This study is part of a larger study of the impact of having Medicaid after release from institutional settings for persons with severe and persistent mental illnesses (Cuddeback, Morrissey, & Domino, 2016; Morrissey, Domino, & Cuddeback, 2016).
Sample
To identify offenders with severe mental illnesses released during the sampling window (2006-2007), statewide prison records, which contained demographic and clinical information, admission and discharge dates, and most serious offenses, were linked to community mental health records and other public sector data. Diagnoses of severe mental illnesses came from two sources: (a) assessments conducted by the Department of Correction and/or (b) community mental health encounter records. Severe mental illness is typically defined by the conjunction of diagnosis, disability, and duration of illness (Goldman, Gatozzi, & Taube, 1981) and, usually, diagnoses characteristic of severe mental illness include psychotic disorders or bipolar disorders. Here, we sampled only those offenders with psychotic or bipolar disorders to identify a population of offenders with chronically severe mental illnesses for whom medication and treatment would most likely be needed after release from prison.
Most serious crimes for each individual in the sample were identified from Department of Correction records. The designation of most serious crime was each offender’s most serious crime at conviction for the index prison incarceration, and included assault, drug crimes, burglary, and other felonies. Sexual offenses included indecent liberties, rape of an adult, rape of a child, sex with a child, and other sexual crimes (e.g., public nuisance sexual crime, attempted kidnapping with sexual motivation, failure to register as a sexual offender).
A total of 127 offenders with severe mental illnesses who were convicted of sex offenses were identified. As shown in Table 1, the sample was mostly male (94%, n = 119), mostly White (75%, n = 95) with an average age of 34 years (SD = 10.06). Also, 47% (n = 60) of the sample had schizophrenia or schizoaffective disorder, 53% (n = 67) had bipolar disorder, and 61% (n = 77) had a co-occurring substance use disorder. In addition, 43% (n = 55) experienced at least one episode of homelessness prior to the index incarceration, 42% (n = 53) were enrolled in Medicaid at some point prior to incarceration, and the average length of incarceration was 93 months (SD = 64.54).
Sample Characteristics and Outcomes.
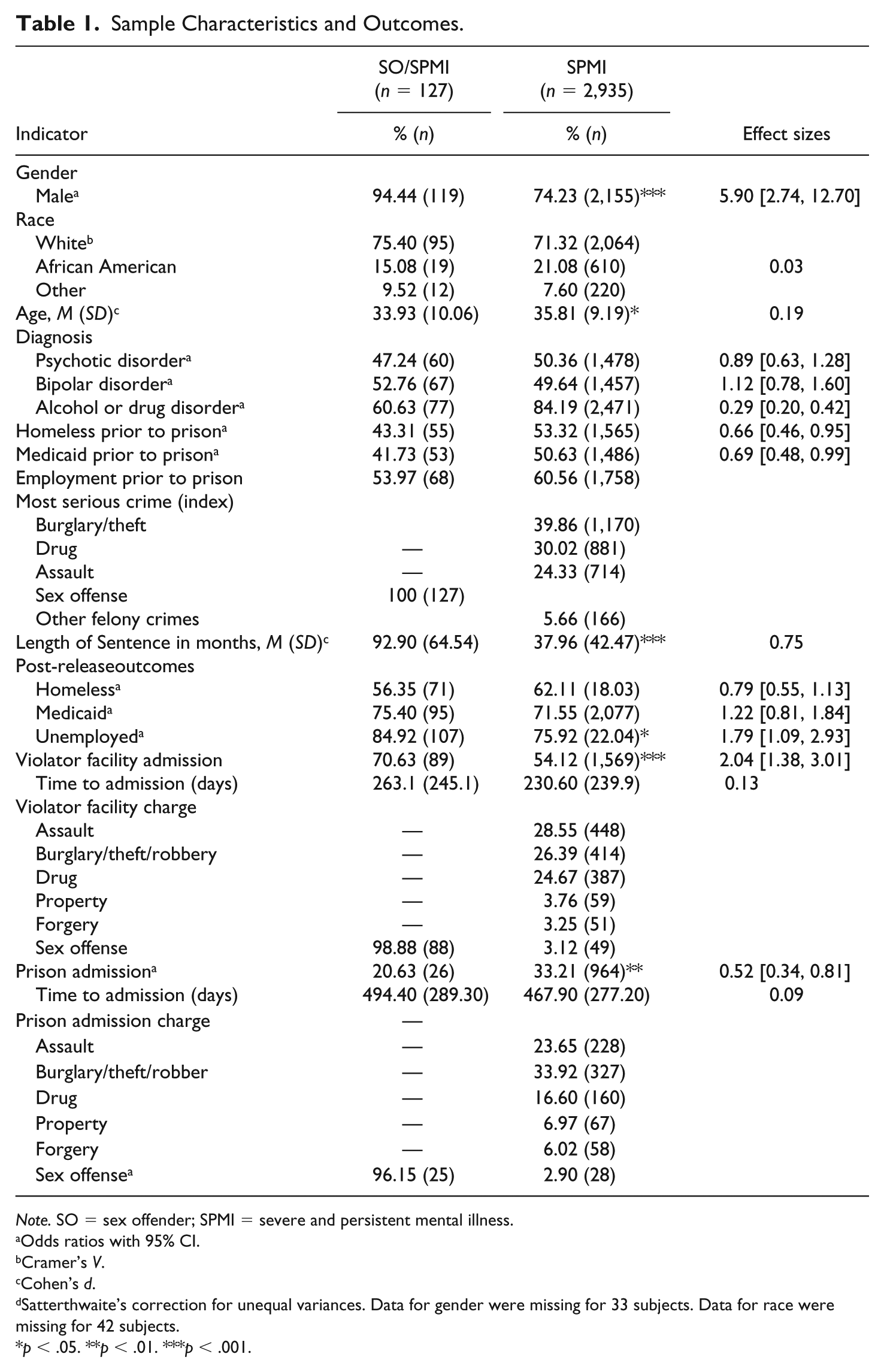
Note. SO = sex offender; SPMI = severe and persistent mental illness.
Odds ratios with 95% CI.
Cramer’s V.
Cohen’s d.
Satterthwaite’s correction for unequal variances. Data for gender were missing for 33 subjects. Data for race were missing for 42 subjects.
p < .05. **p < .01. ***p < .001.
Offenders with severe mental illnesses who committed other offenses as their most serious crimes were used as a comparison group (n = 2,935). As shown in Table 1, the sample of 2,935 releasees with severe mental illnesses who were incarcerated for crimes other than sex offenses was mostly male (74%, n = 2,155), mostly White (71%, n = 2,064) with an average age of 36 years (SD = 9.19). Also, 50% (n = 1,478) of the sample had schizophrenia or schizoaffective disorder, 50% (n = 1,457) had bipolar disorder, and 84% (n = 2,471) had a co-occurring substance use disorder. In addition, 53% (n = 1,565) experienced at least one episode of homelessness prior to the index incarceration, 51% (n = 1,486) were enrolled in Medicaid at some point prior to incarceration and the average length of incarceration was 38 months (SD = 42.47). The top three most serious crimes were burglary/robbery/theft (40%, n = 1,170), crimes involving drugs (30%, n = 881), and assault (24%, n = 714).
Measures
Race was coded as White (reference group), Black, or other. Age was grouped into the following categories: 18 to 25 years (reference group), 26 to 35 years, 36 to 45 years, and 46 years and older. Substance use disorder was a dichotomous variable coded 0 for no diagnosis of drug or alcohol use disorder and 1 for a diagnosis of alcohol or drug use disorder. Administrative data were used to enumerate the following outcomes for each offender during a 36-month post-prison release follow-up period:
Medicaid was recorded as the number of months with Medicaid during the 36-month follow-up period and as a dichotomous variable that was coded 0 for no Medicaid and 1 for one or more months with Medicaid.
Homelessness was recorded as the number of months homeless during the 36-month follow-up period and as a dichotomous variable that was coded 0 for no homeless episodes and 1 for one or more homeless episodes.
Unemployment was recorded as the number of months without any reported wages or earned income during the 36-month follow-up period and as a dichotomous variable that was coded 0 for no unemployment and 1 for one or more unemployed months.
Arrest
State patrol arrest records were used to enumerate post-release arrests. Variables to indicate any arrest and time to arrest after release were created for each offender.
Violator facility admission
Department of Correction records were used to enumerate admissions to violator facilities in Washington State. Violator facilities are short-term facilities for offenders who violate the conditions of their community supervision. Sentences to violator facilities are typically 120 days or less unless a new crime has been committed. Variables to indicate any admission to a violator facility and time to admission after release were created for each offender.
Prison admission
Department of Correction records were used to enumerate readmissions to prison. Variables to indicate any incarceration in prison and time to prison incarceration during the 36-month follow-up period were created.
Data Analysis
Bivariate statistical analyses (i.e., chi-square and t tests) were used to examine differences in the demographic, clinical, and criminal justice characteristics among sex ISOs with severe mental illnesses and offenders with severe mental illnesses who committed crimes other than sexual offenses. Then, logistic regression models were used to examine the probability of admission to a violator facility and the probability of prison admission during the 36-month post-release follow-up period. Each outcome was regressed on group status (i.e., ISOs with severe mental illnesses versus offenders with severe mental illnesses), while holding constant gender, race, age, Medicaid, homelessness, unemployment, and substance use disorder. Statistical analyses were conducted using SAS 9.2 (SAS Institute, Cary, NC). Descriptive analyses were used to present frequencies and means of independent and dependent variables. In all bivariate statistical tests, two-tailed tests were used and alpha was set at .05.
Results
As shown in Table 1, compared to offenders with severe mental illnesses, ISOs with severe mental illnesses were more likely to be male, 94% versus 74% for ISOs versus ISOs, respectively, χ2(1) = 26.36, p < .001, and had longer periods of incarceration, 92 months versus 38 months for ISOs versus non-ISOs, respectively, t(128.21) = −6.52, p < .001, but were less likely to have a co-occurring substance use disorder, 61% versus 84% for ISOs versus non-ISOs, respectively, χ2(1) = 48.38, p < .001.
Also shown in Table 1, with respect to Medicaid, homelessness, employment, and criminal justice outcomes during the 36-month post-release follow-up period, both samples had high rates of post-release Medicaid enrollment and homelessness, whereas, compared to offenders with severe mental illnesses who committed sex crimes, offenders with severe mental illnesses who committed other crimes were more likely to be unemployed (p < .001) during the follow-up period.
Although not shown in Table 1, there were statistically significant differences in the types of charges for which offenders were arrested in the post-release period. For example, compared to those with severe mental illnesses who were convicted of sex offenses, offenders with severe mental illnesses who were convicted of other offenses were more likely to be arrested for drug violations (16% vs. 7%, p < .01) and burglary (8% vs. 3%, p < .05), but were less likely to be charged with a technical violation (e.g., community custody violation, noncompliance with conditions of sentence, and/or probation supervision violation, 14% vs. 25%, p < .01).
As shown in Table 1, 70% of offenders with severe mental illnesses who were convicted of sex offenses were detained in a violator facility at least once during the follow-up period compared with 54% of offenders with severe mental illnesses who were convicted of other crimes (p < .001). The average time in the community prior to admission was 263 days for offenders with severe mental illnesses who were convicted of sex offenses and 230 days for offenders with severe mental illness who were convicted of other crimes, however, this difference was not statistically significant. Furthermore, almost 100% of offenders with severe mental illnesses who were convicted of sex offenses were admitted to a violator facility due to a violation related to a sex offense, compared with offenders with severe mental illnesseses who were convicted of other crimes, who were admitted on charges of assault (25%), burglary/theft/robbery (26%), or drug charges (25%).
Also, shown in Table 1, 20% of offenders with severe mental illnesses who committed sex offenses returned to prison compared with 33% of the offenders with severe mental illnesses who committed other crimes (p < .01). The average time in the community prior to prison admission was 494 days for offenders with severe mental illnesses who were convicted of sex offenses and 467 days for offenders with severe mental illnesses who were convicted of other crimes, however, this difference was not statistically significant. Furthermore, 96% of offenders with severe mental illnesses who were convicted of sex offenses were admitted to violator facility due to a violation related to a sex offense, compared with offenders with severe mental illnesses who were convicted of other crimes, who were admitted on charges of burglary/theft/robbery (34%), assault (24%), or drug charges (17%).
The results of the logistic regression models are shown in Tables 2 and 3. As shown in Table 2, being convicted of sexual offense was associated with an increased probability of admission to a violator facility, when holding constant all other variables (p < .001). Medicaid (p < .001) was associated with a decreased probability of admission to a violator facility, whereas homelessness (p < .001), unemployment (p < .001), and substance use (p < .001) were associated with increased probabilities of admission to violator facility, when holding all other variables constant. As shown in Table 3, severe mental illness was not associated with an increased likelihood of prison readmission, when holding constant all other variables; however, having Medicaid (p < .001), homelessness (p < .001), and unemployment (p < .001) were associated with an increased probability of prison readmission.
Predictors of Admission to a Violator Facility in the 36-Month Follow-Up Period.
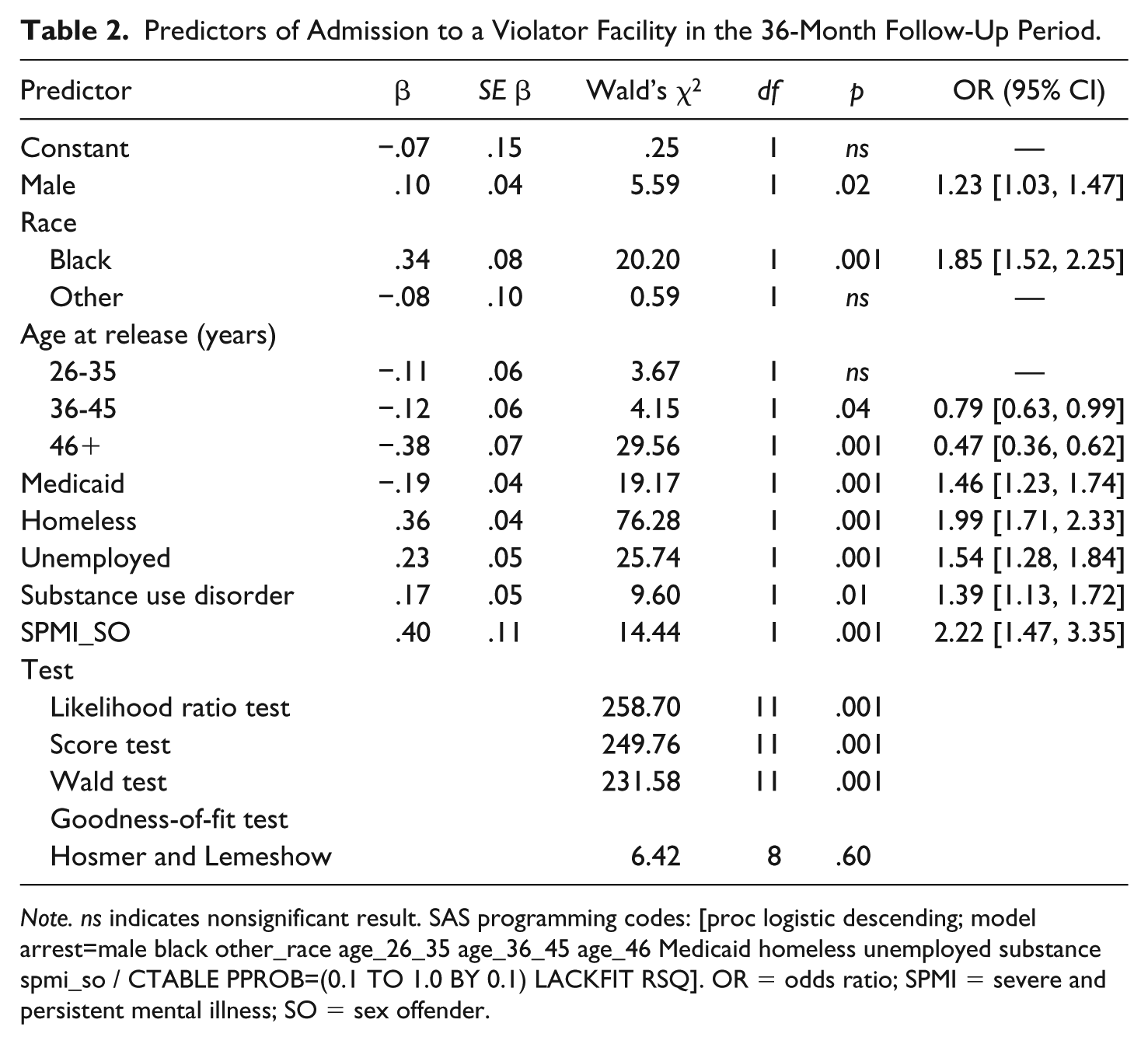
Note. ns indicates nonsignificant result. SAS programming codes: [proc logistic descending; model arrest=male black other_race age_26_35 age_36_45 age_46 Medicaid homeless unemployed substance spmi_so / CTABLE PPROB=(0.1 TO 1.0 BY 0.1) LACKFIT RSQ]. OR = odds ratio; SPMI = severe and persistent mental illness; SO = sex offender.
Predictors of Admission to Prison in the 36-Month Follow-Up Period.
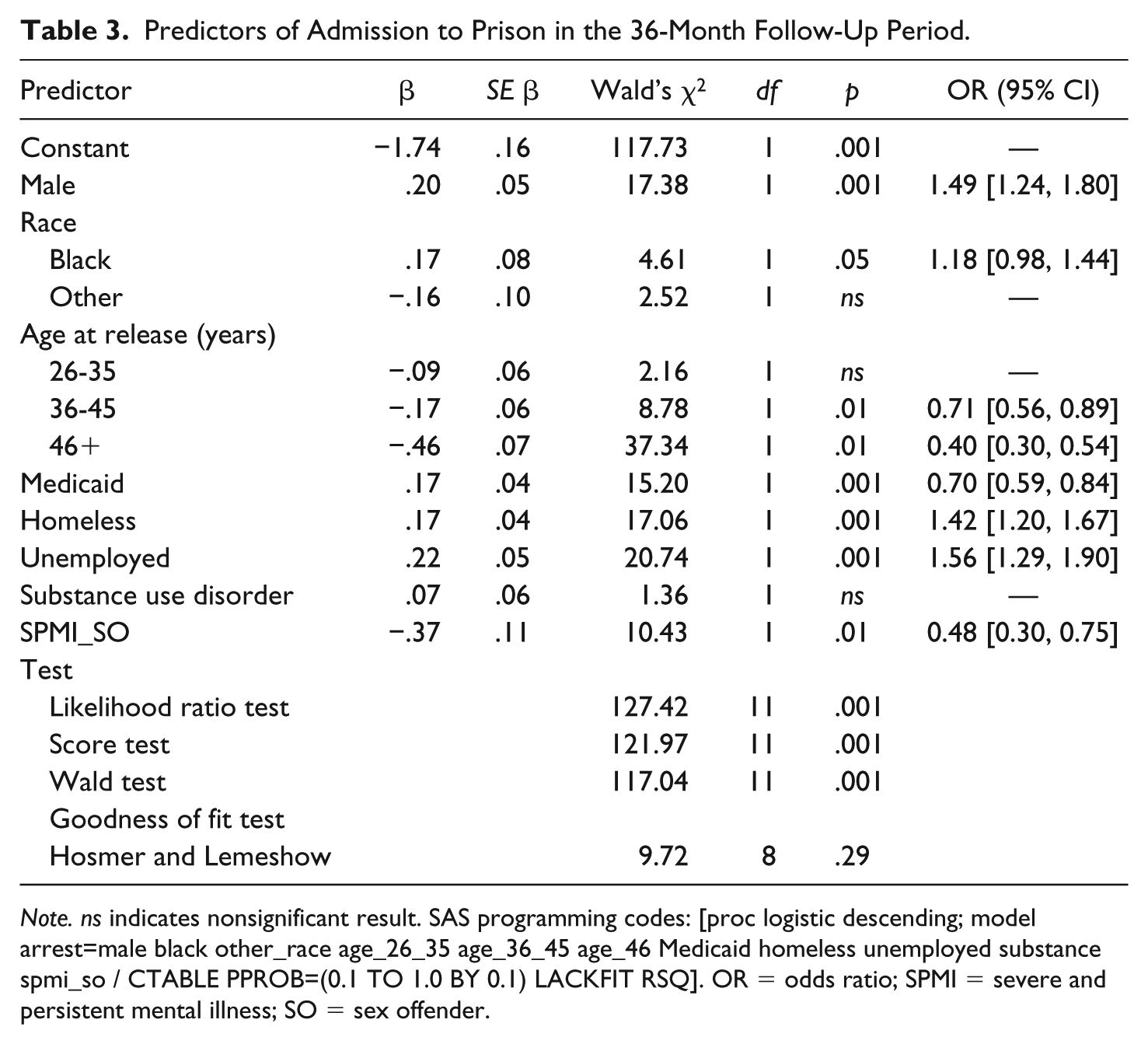
Note. ns indicates nonsignificant result. SAS programming codes: [proc logistic descending; model arrest=male black other_race age_26_35 age_36_45 age_46 Medicaid homeless unemployed substance spmi_so / CTABLE PPROB=(0.1 TO 1.0 BY 0.1) LACKFIT RSQ]. OR = odds ratio; SPMI = severe and persistent mental illness; SO = sex offender.
Discussion
This study adds to the growing literature about ISOs with severe mental illnesses who are released from prison and contributes to our understanding of the, characteristics and post-release community reentry outcomes of this population. Admissions to violator facilities for the sample of ISOs with severe mental illnesses in the 36-month follow-up period were higher (70%) than those of offenders with severe mental illnesses who committed other crimes (54%), although sexual recidivism (i.e., defined here as prison admission for a sex offense) among ISOs with severe mental illnesses (25%) was similar those reported in the literature for ISOs without mental illnesses (i.e., 13% and 19%; Hanson et al., 2009; Hanson & Bussiere, 1998).
These findings illuminate several points. First, ISOs with severe mental illnesses are a high-profile, high-need group that will continue to demand special attention from criminal justice and mental health authorities. There are a limited number of programs for ISOs who have been released from prison that include such supports as housing, mental health treatment, and employment (Wilson, Cortoni, & McWhinnie, 2009; Wilson, Picheca, & Prinzo, 2007). Although these programs report positive outcomes on reducing recidivism for offenders (Wilson et al., 2009; Wilson et al., 2007), there is no information whether individuals who also have mental illnesses have been included.
Furthermore, rates of post-release homelessness and unemployment among both study groups are high, but markedly worse from pre-incarceration to post-release for offenders with severe mental illnesses convicted of sexual offenses. That is, homelessness increased from 43% prior to the index incarceration to 57% post-release and unemployment increased from 46% prior to the index incarceration to 85% post-release for offenders with severe mental illnesses who were convicted of sex offenses. Clearly, basic needs such as housing should be addressed as an overall reentry strategy for all individuals reentering their communities after release, but this issue could be particularly salient, and particularly difficult, for highly marginalized and highly stigmatized population of sex offenders with severe mental illnesses.
Second, post-release criminal justice contacts (i.e., arrest, violator facility admission and prison admission) are high for offenders with severe mental illness, in general, but admissions to violator facilities occur more frequently among those offenders with severe mental illnesses who have convictions of sex offenses. Thus, it could be the added complexity of a sex offense, stricter probation/parole requirements associated with sex offenses, over-policing by probation officers due to the high-risk, high-profile nature of the population, in combination with the challenges of living with a severe mental illness, does lead to more criminal justice contacts after release from prison for offenders with severe mental illnesses. Our findings suggest the added complexity of a sex offense exacerbates post-release challenges for a population that already has poor reentry outcomes, including greater homelessness, unemployment, and criminal justice contacts (i.e., arrests for technical violations and violator facility admissions).
Offenders with severe mental illnesses who were convicted of sexual offenses were less likely to return to prison compared with offenders with severe mental illness who committed other crimes, however. It could be that, the higher rates of violator facility charges associated with sex offenses (i.e., technical violations related to supervision) suggest that criminal activities of these offenders do not rise to the level where prison readmission is warranted. Also, it could be that policy around certain crimes (i.e., policy for repeated drug offenses) result in more severe consequences. Future research should address post-release community trajectories and the nature and timing of criminal justice contacts for this population.
Addressing the needs of offenders with mental illnesses is particularly important because in recent years, there has been a focus on empirically-supported community supervision for offenders with severe mental illnesses (Skeem & Louden, 2006); however, the extent to which these strategies are effective for ISOs with severe mental illnesses is unknown. Furthermore, there is little information in the literature about the extent to which special training or clinical competencies are needed for ISOs with severe mental illnesses, particularly around strategies to make conditions of community supervision easier to understand and comply with to minimize technical violations among persons with mental illnesses.
Research about best practices for sex offenders with severe mental illnesses in community supervision settings should be accelerated, especially in light of the fact that sex offender laws have the potential to greatly hinder the rehabilitation process for ISOs, and there is concern as to whether these policies are creating environments where rehabilitation is unfeasible (Human Rights Watch, 2007; Levenson, D’Amora, & Hern, 2007; Ward, Gannon, & Birgden, 2007). Adding a diagnosis of severe mental illness may contribute to the complexities of this already difficult struggle, yet, little is known about how communities may be addressing these challenges. Moreover, the high rates of co-occurring substance use disorders, which suggests that integrated dual disorder treatment (Drake, Mercer-McFadden, Mueser, McHugo, & Bond, 1998) and motivational interviewing techniques (Davis, Baer, Saxon, & Kivlahan, 2003) could be particularly important to this population, especially given the role of substance use in recidivism.
The limitations of this study include the limited generalizability of findings from one state. Also, the demographic, clinical, and criminal justice variables included a limited set of characteristics. Another limitation of our study is the lack of an independent measure of mental illness in that diagnosis alone is not necessarily an indicator of severity. To some extent, Medicaid enrollment can be considered a proxy for mental illness duration and disability, given Medicaid is often received as a part of enrollment in programs such as Supplemental Security Income and/or Social Security Disability Income, which have strict eligibility criteria, and often take years to gain access. The fact that our sample is largely young, male offenders who most likely receive Medicaid due to their psychiatric disabilities potentially speaks to its severity.
Also, sentencing data and probation/parole data were not available to confirm the extent to which our sample completed their prison sentences and were released on parole arrangements, and the arrest data we used for the study did not extend throughout the duration of the follow-up period (arrest data ended in mid-2007). Future research should include post-release supervision data and sentencing data to further examine post-release outcomes. Nevertheless, these data are the best currently available to answer questions about ISOs with severe mental illnesses who are released from prison, and this study addresses several gaps in our understanding of the population.
In conclusion, offenders with severe mental illnesses who are convicted of sex offenses are a particularly complex population, and these offenders will continue to challenge criminal justice, behavioral health, and sex offender treatment policy, practice, and research. There remains much to be done to understand ISOs with severe mental illnesses and to develop effective practice and policy for this population such that public safety is preserved and their treatment needs are met.
Footnotes
Acknowledgements
The assistance of staff at the Washington State Department of Social and Health Services and the Washington State Department of Corrections in data retrieval, linkage, and documentation is gratefully acknowledged. The findings and interpretations reported here are those of the authors and do not imply endorsement by Washington State agencies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by funding from the National Institute of Mental Health (MH086232).