
Abstract
Introduction
Little is known about strategies used by parents to explicitly promote the participation in meaningful occupations of transition-age youth. This descriptive study explored the type and scope of parents' strategies to facilitate the participation of youth living with a physical disability.
Methods
Twenty-two parents of youths (12 to 18 years) with mobility restriction reported strategies used at home, school, and in the community by completing the Participation and Environment Measure for Children and Youth at two time points. Content analysis was conducted. Strategies were extracted and coded, and sub-categories were identified and organised into the three domains (person, occupation, environment) of the Canadian Model of Occupational Performance – Engagement.
Findings
Overall, 241 strategies were reported, of which 130 were distinct. The strategies encompassed all three domains of the Canadian Model of Occupational Performance – Engagement, with an emphasis on youths' immediate physical environment and no reference to institutional policies at the macro level. The majority of strategies focused on facilitating youths' participation in the school setting through collaboration, advocacy, and involvement.
Conclusion
Findings can increase our understanding of the range of actions parents take in supporting participation of transition-age youth. Occupational therapists can build on those strategies and, through family-centred practice, jointly promote youth participation and inclusion.
Introduction
Children and youths' participation and involvement in meaningful occupations are fundamental to their physical, mental, and social wellbeing (Law, 2002). Studies show that children and youth with disabilities face greater restriction to participation in social, recreational, and household activities in comparison to peers without disabilities (Tonkin et al., 2014). Youth aged 10–19 years (World Health Organization, 2014) who are living with physical disabilities often rely on the support of their parents (Peny-Dahlstrand et al., 2009; Stewart, et al., 2002) to facilitate their social and leisure experiences and to promote their participation (Anaby et al., 2013; Fawcett et al., 2009). Understanding the strategies used by parents to support their youth's participation during this crucial transitional phase is therefore critical.
There is an emerging body of knowledge exploring parents' strategies. A qualitative study among 16 parents of children 5–15 years of age with acquired brain injury (Bedell et al., 2005) identified three categories of strategies used by parents: (1) creating opportunities; (2) teaching skills; and (3) regulating cognitive and behavioural function to facilitate their child's social participation. Another descriptive study among 576 children and youth with and without disabilities aged 5–17 years (Bresnahan et al., 2012) further revealed common strategies used to support participation. Examples include parent involvement, encouragement, and support, as well as seeking activity, advocating, educating self and others, and modifying the environment. The authors, however, did not examine the specific strategies used by parents within each age group (that is, youth and younger children) – two populations that not only exhibit different needs (Gorter et al., 2011), but also different participation patterns, particularly as they reach the age of 12 years (King et al., 2010; Klaas et al., 2010). A scoping review conducted by Piskur and colleagues (2012) emphasised this knowledge gap in which studies report actions taken by parents across broad age ranges, for example 0 to 18 years of age, rather than focusing on age-specific strategies. Findings included choosing activities, modifying and adapting the activity, coaching and educating the child on a skill and others on how to support the child's participation, structuring and planning an activity, and networking and creating connections with parents with similar experiences. Bedell and colleagues' study (2011) was consistent with this, reporting similar strategies used by 42 parents of children aged 5 to 16 years of age, with and without disabilities, to support their child's participation, such as providing emotional and practical support, and showing interest in and asking questions about the child's activities. Only parents of children with disabilities, however, reported that a key focus of their efforts was to prepare the child at home for specific school and community activities. Additionally, parents gathered information to appraise their child's participation by observing the child doing an activity and attending to their verbal and non-verbal cues, reviewing documentation, knowing the child's daily routine, and obtaining verbal and written feedback from the child, their peers, and other adults (Bedell et al., 2011).
While the aforementioned studies provide valuable insight into different strategies implemented by parents of children and youth across a broad age range, none employed a specific analysis of strategies pertaining to youth only – those older than 12 years. Focusing on youth is of particular importance as they are facing a challenging transition to adulthood and independent living; a transitional stage during which lifelong habits can be established through positive experiences and opportunities for participation, capacity building, and empowerment (Gorter et al., 2011). Therefore, the purpose of this study was to examine the type and scope of strategies used by parents of youth with physical disabilities, aged 12 to 18 years, using a structured measure. Knowledge gained from this study may increase our understanding of the range of strategies parents utilise for supporting their youth's participation in different settings (home, school, and the community), further facilitating elements of family-centred practice.
Method
This descriptive study examined existing data obtained from a larger study (n = 28) that demonstrated the effectiveness of the Pathways and Resources for Engagement and Participation (PREP) intervention in promoting community participation among youth with physical disabilities by modifying aspects of their environment (Anaby et al., 2018). Since this 12-week intervention focused specifically on improving three leisure activities that occur in one single setting (community), we were not expecting to see a significant change in strategies translated into other settings immediately after the intervention. Rather, we aimed to better understand the range and richness of actions taken by parents to improve their youth's participation in general. Twenty-two parents of youths aged 12 to 18 years whose mobility was restricted (for example due to cerebral palsy, spina bifida, or musculoskeletal disorders) were recruited from five major rehabilitation centres and two high schools in Greater Montreal, from both the Anglophone and Francophone communities (Anaby et al., 2018). Adolescents who were recovering within the first year following a severe brain injury were excluded, as their functional capacities were less likely to be stable. Data collected by the parents (n = 22) who completed the Participation and Environment Measure for Children and Youth (PEM-CY) in the larger study are reported here.
Ethics approval was obtained from the Centre for Interdisciplinary Research in Rehabilitation of Greater Montreal and the Institutional Review Board at McGill University, and an informed consent was completed by all participants. Parents' strategies for supporting their youth's participation in home, school, and the community were then measured using the PEM-CY at two different time points (16 weeks delay; 12-week intervention phase + four-week baseline period). The PEM-CY, a standardised, valid, and reliable parent-report questionnaire, evaluates the participation of children aged 5–17 years in three settings: home, school, and community. It measures participation based on frequency, involvement, and parent's desire for change, and has been found to have moderate to good internal consistency (0.59–0.83) and test–retest reliability (0.58–0.84) among children and youth with various types of disabilities (Coster et al., 2011). Specifically, parents were instructed to report strategies used by themselves or other family members to help their youth successfully participate in activities in each of the three settings. Parents reported, in their own words, up to three strategies for each of the three settings, resulting in up to 18 strategies: nine strategies at time 1 and nine strategies at time 2.
Data analysis
Content analysis was conducted following Elo and Kyngäs's (2008) process and involved two phases. In phase 1, all parent strategies were extracted, coded, and organised into identified sub-categories. These sub-categories were collapsed into categories and then, through phase 2, organised into the three domains of the Canadian Model of Occupational Performance – Engagement (CMOP-E): person, occupation, and environment (Townsend and Polatajko, 2007). Each of the three domains has individual components. The occupation domain is classified into three components: self-care, productivity, and leisure. The environment domain is comprised of four components: physical, cultural, social, and institutional. Lastly, the person domain includes the cognitive, affective, and physical components, with spirituality nested at the core. The latter, being an important element of the CMOP-E, was also included as an additional domain for categorisation. The result of the dynamic interplay between these four domains depicts an individual's performance and engagement in human occupation, thus allowing data to be framed within an occupational therapy context (Townsend and Polatajko, 2007). Such a classification can be useful to clinicians as it corresponds with intervention approaches typically done in practice such as changing aspects related to the child specifically (child-focused approaches or remediating body functions and abilities), aspects of the environment (context-focused therapies or changing environmental constraints), and aspects of the activity (modifying the demands of the task or grading the activity, or redesign of the array of occupations).
The analytical process involved specific steps. Following the extraction of all strategies, an initial list of codes was generated by one team member. Codes were sorted and collapsed into sub-categories, or level 2 categories (for example adaptation of the task, repetition, and practice), which were merged into broader categories, or level 1 categories (task demands). These categories were then organised and classified using the domains of the CMOP-E (for example occupation). Categories of strategies were checked back against original data and vice versa by reading and re-reading the collated extracts for each category. This process, supported by a team discussion and a consultation with the principal investigator, ensured that level 1 and level 2 categories were grouped under the appropriate domains of the CMOP-E. The number of unique or distinct strategies that supported each sub-category were counted. For example, if several parents mentioned ‘encouragement’ as a strategy, this was counted as one single example. Such an approach allowed us to illustrate the richness and variety of the data.
To guide the final analysis, several statistical tests were initially performed using Microsoft Excel. As anticipated, the chi-square test indicated no significant difference between the distribution of strategies across the domains of the CMOP-E and the two time points pre and post intervention (
Findings
Sample characteristics
Twenty-two parents of youth with physical disabilities participated in this study (six participants did not complete the PEM-CY because it was added in a later stage of the study). Among our participants, 86% were mothers, 9% fathers, and in 5% of the cases both parents completed the assessment together. Parents' ages ranged between 30 and 59 years, with the majority of them (64%) being 40–49 years old. Eighty-six percent of caregivers had more than a high school degree, and they lived mainly in the major urban (41%) and suburban (36%) areas surrounding Montreal. Fifty percent of the families reported having an annual income of more than $60,000 (CAN), which is the median household income in Quebec. Participants were the caregivers of youths aged 12–18 years (Mean = 14.14; SD = 1.86; one participant reached 18 years old) with comorbid impairments, most frequently orthopaedic/movement impairment (68%), speech/language impairment (50%), vision impairment (27%), and intellectual delay (22%). Fifty percent of the youth were reported to have more than five functional issues, with the most frequent being difficulties in using their hands to do activities (82%), moving around (73%), managing emotions (64%), communicating with others (55%), and seeing (55%).
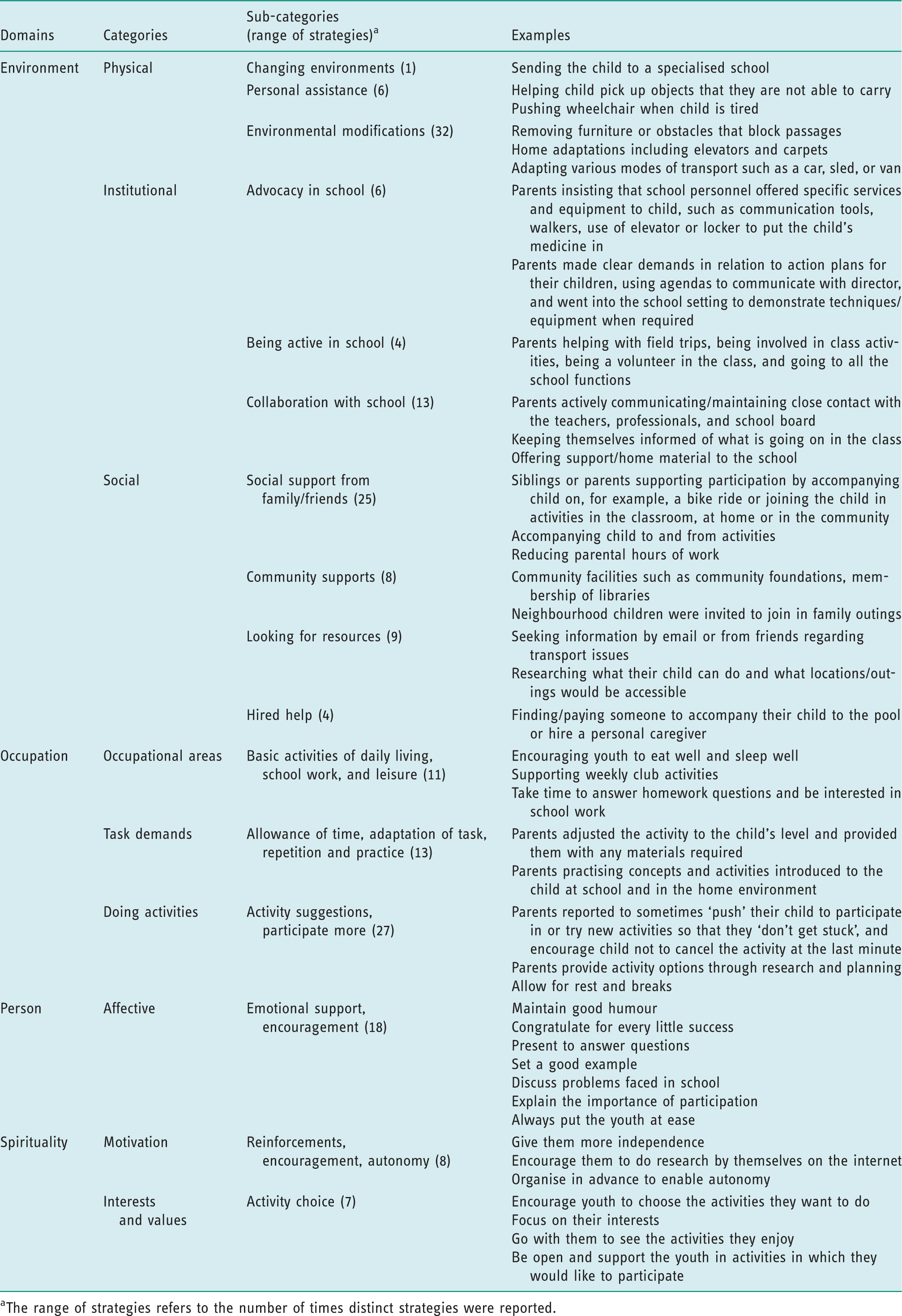
Overall, 241 strategies were reported by parents, and the most common strategies were categorised under the environment domain (53%), followed by occupation (24%), person/youth (13%), and spirituality (10%). Of these 241 reported strategies, 130 distinct strategies were identified and were linked to each of the domains of the CMOP-E. As shown in Figure 1, the largest number of distinct strategies was categorised under the environment (43%), followed by occupation (35%), person (12%), and spirituality (10%). Table 1 illustrates examples of the strategies identified by parents for each category. Figure 2 demonstrates the conceptual mapping and classification of the level 1 and level 2 categories.
Distribution of distinct strategies used by parents of youth with disabilities to support participation across the domains of the Canadian Model of Occupational Performance – Engagement (CMOP-E) (Townsend and Polatajko, 2007). Categories and sub-categories extracted from parent-reported strategies, mapped using the domains of the Canadian Model of Occupational Performance – Engagement (CMOP-E) (Townsend and Polatajko, 2007). Examples of the range of distinct strategies used by parents of youths with disabilities to support participation, categorised using the domains of the Canadian Model of Occupational Performance – Engagement (CMOP-E) (Townsend and Polatajko, 2007). The range of strategies refers to the number of times distinct strategies were reported.

Environment
Parents’ strategies collapsed into three categories within the environment domain: physical, social, and institutional (Figure 2/Table 1). The physical environment encompassed three main sub-categories: changing environments (1), personal assistance (6), and environmental modifications (32). The majority of strategies were in the latter two sub-categories, with only one strategy (‘sending the youth to a specialised school’) applicable to the changing environment sub-category. Personal assistance strategies included ‘helping the youth take down his bag before he goes to school’ and ‘transporting the youth's things’. The environmental modifications sub-category captured the largest range of distinct strategies used in the physical environment, such as organising the environment (for example ‘placing objects in good locations’ or ‘using powered mobility’) and planning ahead (for example ‘planning an intervention ahead of time with the school’ or ‘preparing meals ahead of time’). Adapting various modes of transport and adapting schedules were also reported. Parents re-designed the environment to create a calming atmosphere, such as ‘installing a hammock outside’ or ‘installing a mural with natural scenery in the youth's room’. Finally, strategies for encouraging/stimulating the youth's communication were also incorporated by putting in place devices such as small tablet computers. Table 1 further illustrate examples of strategies used.
The social environment included four main sub-categories: social support from family and friends (25); community supports (8); looking for available resources (9); and hired help for the youth (4). As can be seen in Table 1, the majority of strategies parents used drew on social support from immediate family and friends of the family (for example siblings supporting one youth's participation in bike ride). A smaller variety of strategies were utilised in the area of community supports (for example asking the neighbour's children to go on outings) and looking for available resources (for example research on the internet for adapted locations for outings), while very few alternatives were reported in the hired help sub-category (for example accompany youth for outings).
Three sub-categories emerged accounting for strategies related to the institutional environment, with special attention towards the school setting: advocacy in school (6); being active in school (4); and collaboration with school (13). This involved, for example, ongoing contact and follow up with teachers, healthcare professionals, and school-based staff. Advocacy in the school included communicating with school directors and school boards for the purpose of advocacy for services and environment modifications. Parents reported the least number of distinct strategies in the ‘being active in the school’ sub-category, which included helping out with field trips and class activities, while ‘collaborating with the school’ included the majority of strategies (for example parents following youths’ scholarly success at school with the director and other professionals). Examples of more specific strategies used in each of these areas are illustrated in Table 1.
Occupation
Parents' strategies addressed all occupational areas highlighted in the CMOP-E: self-care (basic activities of daily living (ADL), productivity (in terms of school work), and leisure. However, a limited range of occupational strategies were observed. To illustrate, basic ADL strategies reported included encouraging the youth to eat and sleep well, and a single leisure strategy of supporting weekly club activity was reported. Strategies that related to school work were more common and focused on assisting the youth with homework, projects, exams, and other school activities such as taking time to answer questions and showing interest in what the youth was doing.
Within the domain of occupation, ‘task demands’ was another level 1 category that emerged, describing parent strategies of allowance of time, adaptation of task, and repetition and practice. Examples included ‘parents adjusting the activity to the youth's level’ (in terms of their level of pain and fatigue, for instance by giving extra breaks), ‘providing them with any materials required’, and the opportunity to practise activities at home. They also organised the youth's paperwork and school bag and ensured tasks were well defined. One parent described backward chaining, reporting that she would ‘leave the things she was capable of doing for her daughter to do’; for example, the parent would bake the cupcakes and her daughter would decorate them. The range of distinct strategies related to the demands of the task were relatively small (13). In comparison, in the category ‘doing activities’ (27), parents reported numerous different strategies focusing on supporting the youth to do activities. The sub-categories that emerged were ‘participating more’ (for example parents actively encouraged their child to sign up for mainstream or adapted activities) and ‘activity suggestions’ (for example parents initiating family gatherings and outings, visiting friends, varying activities, providing activity choices, exploring alternative extracurricular activities), with the aim of maximising the youths’ participation in activities. To illustrate, family activities were organised and the youth participation was facilitated through balancing play and rest, taking regular breaks, and redistributing the task based on the youth's health on that day.
Person and spirituality
Parents identified strategies that focused on affective components with two sub-categories emerging: emotional support (12) and ongoing encouragement (6). Within spirituality, two sub-categories emerged: motivation, and interests and values. Strategies in the area of motivation included reinforcements through, for example, rewards (2), encouragement (1), and providing autonomy for youth to search for activities with the objective of enabling independence (5). Strategies in the area of interests and values were focused on the sub-category of ‘activity choice’, which emphasised the youths’ choices and preferences of specific desired activities (7). This involves, for instance, exploring together activities the youth enjoys and focusing on their interests (see Table 1).
Discussion
This study sought to identify the strategies utilised by parents to facilitate their youth's participation at home, school, and in the community. Findings indicate that parents' strategies encompassed all domains of the CMOP-E (Townsend and Polatajko, 2007), with a greater emphasis on the environment. Parents reported a great range of strategies that aimed at influencing their youth's participation, especially related to and within the school environment. For example, similar to previous studies conducted by Bedell et al. (2005), Piskur et al. (2012), and Bresnahan et al. (2012), all of the strategies reported in the institutional environment were specific to the youth's school. This suggests that parents tended to use strategies that they could implement in their immediate environment and may imply that school participation is a priority for parents. While parents report advocacy-related strategies in the school setting by communicating with the teachers, principal, and school board, there were no examples of parents advocating for the youth at a macro level, for example by campaigning for more service programmes or engaging with policy makers to influence government policies specific to schooling and/or to community engagement. Occupational therapists can work together with parents and parents' associations and jointly develop such broad macro-level strategies; this is of particular importance, as previous research highlights the impact of inclusive policies on children's participation (Fauconnier et al., 2009).
A richness of strategies, having the largest number of unique strategies, was also evident in the physical environment; for example, removing furniture or obstacles that block passages, or sending the youth to a different or specialised school. The parents' focus on practical solutions to mitigate the multiple challenges of the physical environment suggests the priority of parents of youths with physical disabilities and was reflected in the large range of strategies reported in this area. For example, in the area of environmental modifications, 32 distinct strategies were reported, such as adapting modes of transportation or re-designing the environment to create a calming and accessible environment. This is consistent with previous research that demonstrated that parents use a variety of environmental modification strategies to promote participation (Bedell et al., 2005; Piškur et al., 2012) and can also be explained by the nature of our sample: youth with mobility restriction. The CMOP-E depicts the person as being embedded within their physical, social, institutional, and cultural environment (Townsend and Polatajko, 2007). In this study, parents reported using environmental strategies in the physical, social, and institutional environment, but not in their cultural environment. Further studies, involving a more diverse sample, are warranted in order to capture potential cultural and attitudinal aspects of the environment that can be modified, particularly as these aspects are known to influence participation (Anaby et al., 2013).
Among the strategies reported in the ‘person’ dimension of the CMOP-E, parents focused solely on the affective aspect of the youth and no parent strategies reported were categorised in the physical or cognitive domains. This suggested that parents did not link working on body functions and structures, such as strength building and rote learning, as means to greater participation. Previous research has shown that families tend to set functional goals framed within the concept of ‘activity and participation’ rather than goals that focus on the remediation of impairments (Law and Darrah, 2014) as they are more meaningful to the individual/family and motivating for the young person. It is plausible that parents recognise and understand the power of ‘environmental’ strategies in promoting the engagement of the youth in meaningful activities. In addition, most of these youth have been diagnosed since birth, thus parents use fewer remedial strategies. Affective strategies, on the other hand, were predominant and focused on parents encouraging the youth by highlighting success and providing support to enable them to persevere. Emotional support provided by families has been found to be key in initiating and sustaining participation, especially during adolescence (Fawcett et al., 2009).
Respecting the youth choices, preferences, and interests, and fostering autonomy, by encouraging the youth to search for and engage in activities of their choice, were unique strategies found in this study that pertain especially to youth. As children transition into adolescence, activities are less likely to be scheduled or overseen by parents, as typically done at a younger age (Tonkin et al., 2014), and expectations to assume responsibility and develop independence are often expressed. ‘Making choices’, as described by adolescents with cerebral palsy (Stewart et al., 2012), is a critical element in shaping their social participation to become meaningful and important, and such a capacity can be further developed. Occupational-focused strategies, such as ‘participating more’ and ‘doing activities’, that emerged in this study also appeared to be specifically relevant to youth, as previous research indicated patterns of decreased social participation and increased social isolation within this age group (Tonkin et al., 2014).
Limitations and future directions
This study has some limitations. Although it identified the range and scope of the successful strategies that parents use to facilitate their youth's participation at home, at school, and in the community, the effectiveness of those strategies was not evaluated. To address this, future studies may consider requesting parents to rank the effectiveness of their strategies when completing the PEM-CY. It would be interesting to gain insight on whether parents use more effective strategies after being introduced to the PREP intervention, using a prolonged follow-up, compared to the pre-intervention, and whether the types of strategies differ across settings. Such a design may allow parents the time and the opportunity to implement acquired strategies. Another limitation of this study is that it focused on parents' perspectives only; it is equally important to capture the strategies that are used by the youth themselves. Future studies can also identify similarities and differences between the strategies used by the youth, the parents, and the clinicians, and further investigate how these can complement each other. In addition, coaching parents, through knowledge translation initiatives, on effective ways to remove environmental barriers at a population level that goes beyond the school setting is warranted. Finally, the study drew on a relatively small convenience sample from only one geographic location and excluded youth within their first year following a brain injury, which may have had an effect on the type of reported strategies. However, the sample was relatively diverse in terms of the youths' functional issues – a factor known to influence participation (Anaby et al., 2014).
Conclusion
This study adds to the emerging body of knowledge that explores parent strategies used with children and youth with disabilities aged 12 to 18. It is the first study of its kind to examine the strategies used by parents with youth with physical disability alone, using a structured measure. The results highlighted that parents used strategies in all three domains of the CMOP-E, with a richness of strategies noted in the environment, especially the physical environment. These results have implications for occupational therapy practice and research. They provide insights into the type and scope of strategies that parents find helpful in promoting their youths' participation in home, school, and community settings. This information can be used to inform or refine strength-based interventions (Anaby et al., 2015). Occupational therapists can use this knowledge and build on it by collaborating with families through a family-centred approach. Future research could build on these findings by exploring the success of these parent strategies and also the similarities and differences between these strategies and those the youth may report using themselves.
Key findings
Parents' strategies focused primarily on the youth's immediate physical environment, with a special emphasis on the school setting. No reference to institutional policies at the macro level was observed. Unique attention was directed to the affective aspects of the youth, respecting their choices, preferences, and interests.
What the study has added
Findings enhance our knowledge about strategies parents use to support youth-specific participation, further facilitating family-centred practice.
Footnotes
Acknowledgements
We would like to thank the participating youth and their families for their time as well as to the occupational therapists who delivered the interventions for their commitment to the project.
Research ethics
Ethics approval was obtained in 2017 from the Comite d’Ethique des etablissements du CRIR under research project CRIR-865-0713: ‘Opening doors to participation of youth with physical disabilities in community activities: An intervention study’.
Consent
Written informed consent was obtained from all participants.
Declaration of conflicting interests
The authors confirm that there is no conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was funded by the Canadian Institutes of Health Research (CIHR).
Contributorship
Dana Anaby conceived, designed, and executed the study; she has led the methodology of the project and the analysis of the data, and contributed to the writing of all sections of the manuscript. Saeideh Shahin researched the literature, drafted the introduction, and organised the data. Hazel Killeen summarised the findings and contributed to the discussion. Gary Bedell reviewed the manuscript and provided substantial feedback. All authors interpreted the data, and reviewed and edited the manuscript.