
Abstract
Introduction
Developmental coordination disorder is a common disorder of childhood. Little is known about adolescence, however, and research typically reflects professionals’ and parents’ perspectives. This study explored how life is experienced by teenagers with developmental coordination disorder from their own contemporaneous perspective.
Methods
The study was guided by the principles of interpretative phenomenological analysis and a reference group of older teenagers with developmental coordination disorder. A total of 16 interviews were carried out with nine teenagers aged 13–15 years over a 2-year period, offering the opportunity to examine changes in their experience over time. Accounts were subjected to a systematic process of ideographic, inductive and interpretative analysis.
Findings
Themes revealed were: ‘Doing everything the hard way’; ‘I didn’t want to be seen as anyone different’; ‘I’m an intelligent person but I can’t even write’; ‘Right help, right time’ and ‘Making sense of the diagnosis’. Self-efficacy was a strong recurring theme, influencing participants’ motivation for and participation in daily activities, and affecting teenagers’ sense of resilience, agency, ambition and identity.
This article describes the development of a conceptual framework illustrating patterns and connections that occurred across the study themes. The conceptual framework is offered as a novel means of illustrating the complex interaction of factors representing the lived experience of teenagers with developmental coordination disorder.
Conclusion
This study furthers understanding of developmental coordination disorder in adolescence. The conceptual framework is firmly grounded in teenagers’ experience and illustrates the complex interaction of factors influencing teenagers’ lives. The study suggests avenues for intervention and research, and highlights the need for interventions that build teenagers’ self-efficacy to promote positive futures for teenagers with developmental coordination disorder.
Keywords
Introduction
Developmental coordination disorder (DCD) affects 5–6% of school-aged children (Blank et al., 2019) and occupational therapists have a key role to play in enabling children with DCD to reach their personal and academic potential. DCD is diagnosed when a child’s motor skills are substantially below those expected for their age and opportunity for skill learning; when motor difficulties have been present from an early age (not acquired following illness or injury) and there is evidence that they significantly and persistently interfere with activities of daily living; and when motor deficits cannot be better explained by intellectual disability, visual impairment or another neurological condition (American Psychiatric Association, 2013). Whilst primarily considered a motor disorder, there is growing evidence of an association between DCD, poor attention and difficulties with executive functions including working memory, inhibition and planning skills (Leonard et al., 2015; O’Dea and Connell, 2016; Rigoli et al., 2012).
Once considered a disorder of childhood, there is increasing evidence that difficulties associated with DCD frequently persist into adolescence and beyond into adulthood (Blank et al., 2019). Research suggests that adolescents with DCD do less well academically than their peers (Harrowell et al., 2017) and are at risk of poor social and emotional outcomes (Dewey and Volkovinskaia, 2018; Piek et al., 2006; Skinner and Piek, 2001). An association between DCD and reduced physical fitness and health in adolescence has also been reported (Cantell et al., 2008; Coverdale et al., 2012; Wagner et al., 2011).
Qualitative research exploring the experience of DCD in adolescence is limited and typically prioritises the perspective of parents (Missiuna et al., 2007; Stephenson and Chesson, 2008) or teachers (Missiuna et al., 2006), or reports adults’ retrospective recollections (Fitzpatrick and Watkinson, 2003; Missiuna et al., 2008; Ruiz-Perez et al., 2018). Few studies have explored teenagers’ contemporaneous experience of DCD (see for example Barnett et al., 2013; Dewey and Volkovinskaia, 2018; Lingam et al., 2014). The qualitative literature suggests two different trajectories for DCD in adolescence: while parents report increasing concerns for their child’s social and emotional wellbeing in adolescence, studies in which people with DCD were the respondents are more positive. In the study by Lingam et al. (2014), for example, teenagers considered their difficulties as challenges to be overcome and were optimistic for the future.
The aim of the study was to gain a further understanding of the lived experiences of teenagers with DCD from their own contemporaneous perspective. This article describes the development of a conceptual framework, firmly grounded in the narratives of teenagers with DCD who participated in the study, that illustrates the complex interaction of factors representing their lived experience. The conceptual framework will help occupational therapists plan meaningful interventions that ensure positive futures for teenagers with DCD.
Methods
This study was guided by the principles of interpretative phenomenological analysis (IPA) (Smith et al., 2009) and involved a reference group of older teenagers and young adults recruited through the Dyspraxia Foundation. The role of the reference group was to enhance the study’s relevance and quality by influencing the study design; to identify issues of interest to teenagers with DCD for inclusion in the interview schedule; to bring an insider’s perspective to the analytical process and to help to disseminate research findings. Further details about the involvement of the reference group are reported in Payne et al. (2013a).
Sixteen in-depth interviews were conducted with nine adolescents with DCD aged 13, 14 and 15 years over a 2-year period. Accounts were subjected to a systematic process of ideographic, inductive and interpretative analysis to gain an ‘insider’s perspective’ on the lived experience of teenagers with DCD. Ethical approval for the study was provided by Coventry University. Informed written consent was provided by participants and their parents/carers. Participants were also given the opportunity to ask questions before the start of each interview and were reminded that they had the right to withdraw at any time.
Participants
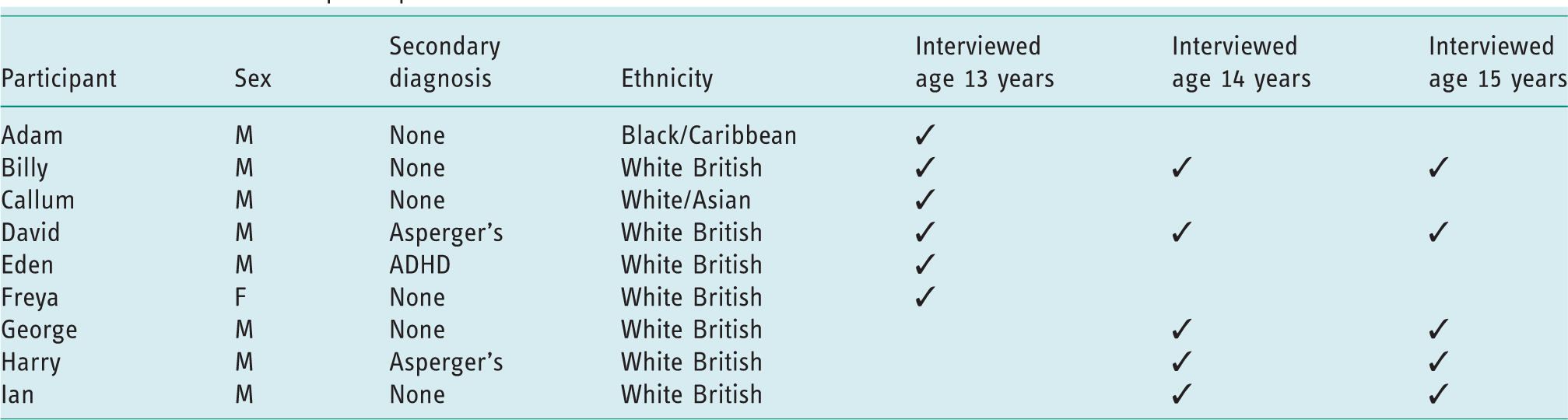
Participants were recruited through the Dyspraxia Foundation. None were known to the researcher and all had a diagnosis of DCD (or dyspraxia), confirmed by a doctor according to local protocols. Co-occurring diagnoses are common in people with DCD (Blank et al., 2019) and this was reflected in the participant group: one had an additional diagnosis of ADHD and two described themselves as having Asperger’s syndrome. All, however, identified DCD (or dyspraxia) as their primary diagnosis. Six participants were interviewed aged 13 years; five at age 14 and five at age 15. Two participants were interviewed on all three occasions, offering the opportunity to examine changes in their experience over time (Table 1).
Information about participants.
Procedure
Nine teenagers opted into the study after receiving information and returning signed consent forms. Data collection was through in-depth semi-structured interviews. This method was chosen to enable participants to raise issues that concerned them whilst ensuring that areas identified by the reference group were also discussed. Interviews broadly covered participants’ understanding of their diagnosis and how it affected them at home, at school and in their leisure time. Interviews were conducted by the researcher in participants’ homes. They lasted around 1 hour and were audio taped and transcribed verbatim.
Analysis
Data analysis was conducted in accordance with the principles of IPA (Smith et al., 2009). After completing interviews with participants aged 13 years, extracts were discussed with the reference group, who offered insights based on their experience, adding extra depth and an ‘insider’s perspective’ to the analysis. Thoughts and ideas offered by the reference group were referred to by SP throughout the analytical process. The first transcript was read repeatedly by SP who noted initial observations and interpretations. Analysis moved to a higher level of abstraction as the transcript was re-read and emergent themes recorded. Associations between themes were explored at a more analytical and theoretical level, drawing on insights offered by the reference group and SP’s personal and professional knowledge. Themes were reorganised and reconsidered to create a master table of themes and sub-themes for the individual. The process was iterative and continued until SP was satisfied that the theme list accurately reflected what was said and meant by the participant (Smith et al., 2009). The process was repeated for each interview transcript. Once themes had been established for each individual, themes were compared across participants and were reviewed and modified until a master list of themes for all participants aged 13 years was created. In accordance with IPA, themes did not have to be evident for each individual to be included in the master list; rather, their inclusion was determined by the richness of the data collected (Smith et al., 2009).
The process was repeated after interviews with participants aged 14 and 15 years. Master themes from all phases of data collection were then reviewed and reconsidered. Further reflection and modification led to the development of a master list of themes illustrating the lived experience of DCD in adolescence.
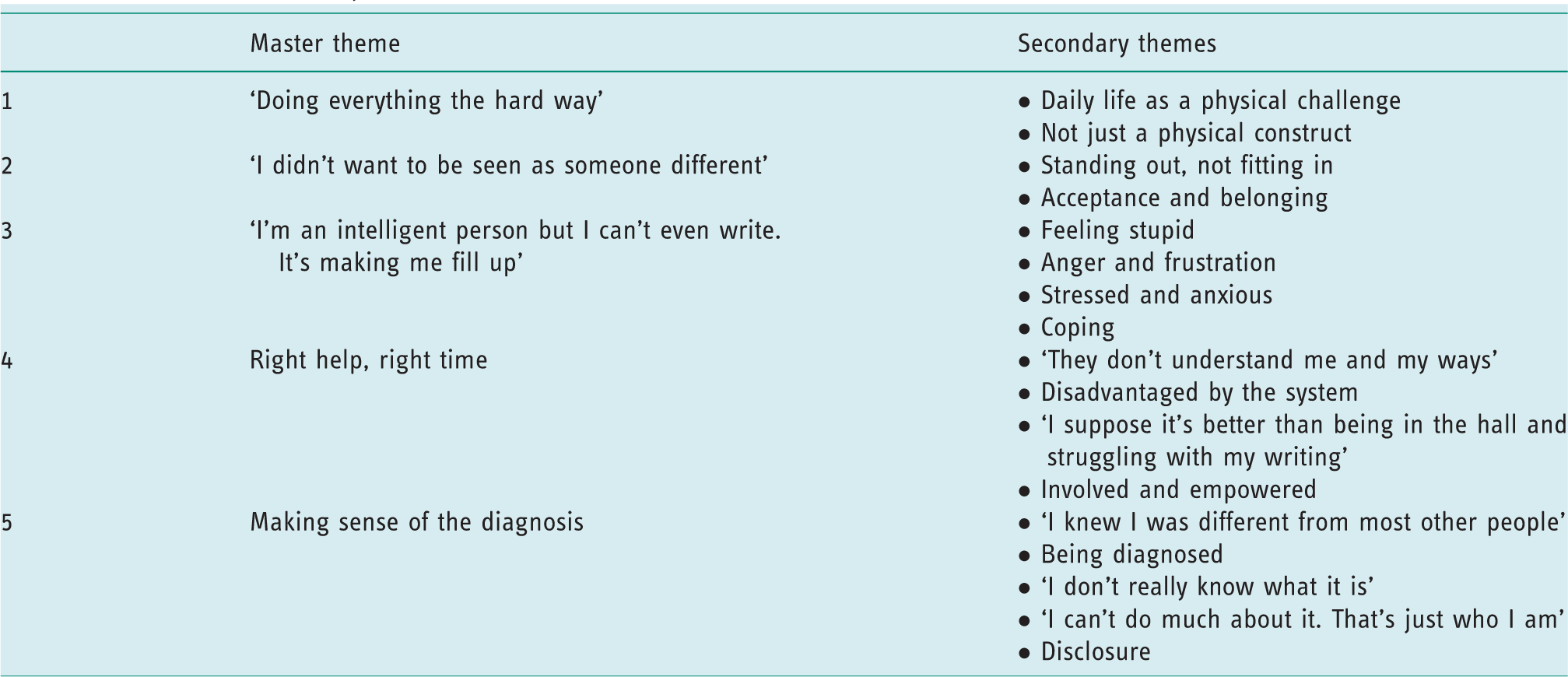
Five themes were identified (Table 2). The first revealed that teenagers experienced DCD to be more than just a motor disorder: participants had to work hard to manage physical tasks, but also experienced poor organisational, planning and time management skills. Themes two and three illustrate the social and emotional impact of DCD during adolescence, while the fourth theme offers insight into participants’ experience of school. The final theme describes the impact of DCD on participants’ sense of identity. These themes have been described elsewhere (Payne, 2014; Payne et al., 2013b, 2013c).
Master and secondary themes.
The influence of co-occurring diagnoses on participants’ experience was considered. Participants were reminded at the start of each interview that the aim of the study was to explore how life is experienced by teenagers with DCD. A review of narratives provided by participants with co-occurring diagnoses indicated that they were able to identify experiences they felt were not related to DCD. At age 13 years, for example, David attributed his lack of interest in school to his autism: ‘I find it all boring. I think it’s something to do with my autism more than my dyspraxia’. This, plus the involvement of the reference group in the analytical process, provides reassurance that the themes identified reflect the experiences of teenagers with DCD rather than experiences that might be attributed to other conditions.
Strategies used to enhance study credibility and trustworthiness included sending interview summaries to participants to check accuracy and discussing interpretations with the research supervision team, which included occupational therapists and a health psychologist. Throughout the analytical process SP referred to insights offered by the reference group and to individual transcripts to ensure that themes were firmly grounded in participants’ own words. Most importantly, involving the reference group throughout the analytical process helped to deepen understanding by providing an insider’s perspective.
The conceptual framework presented in Figure 1 evolved during the latter stages of the analytical process as potential patterns and connections across findings were revealed. Concepts were explored with members of the reference group, clinical colleagues and the research team. Reference was also made to the extant qualitative literature concerning people with DCD. This article describes new understandings brought forth by this study, which were drawn together into a conceptual framework representing the lived experience of teenagers with DCD as a whole.
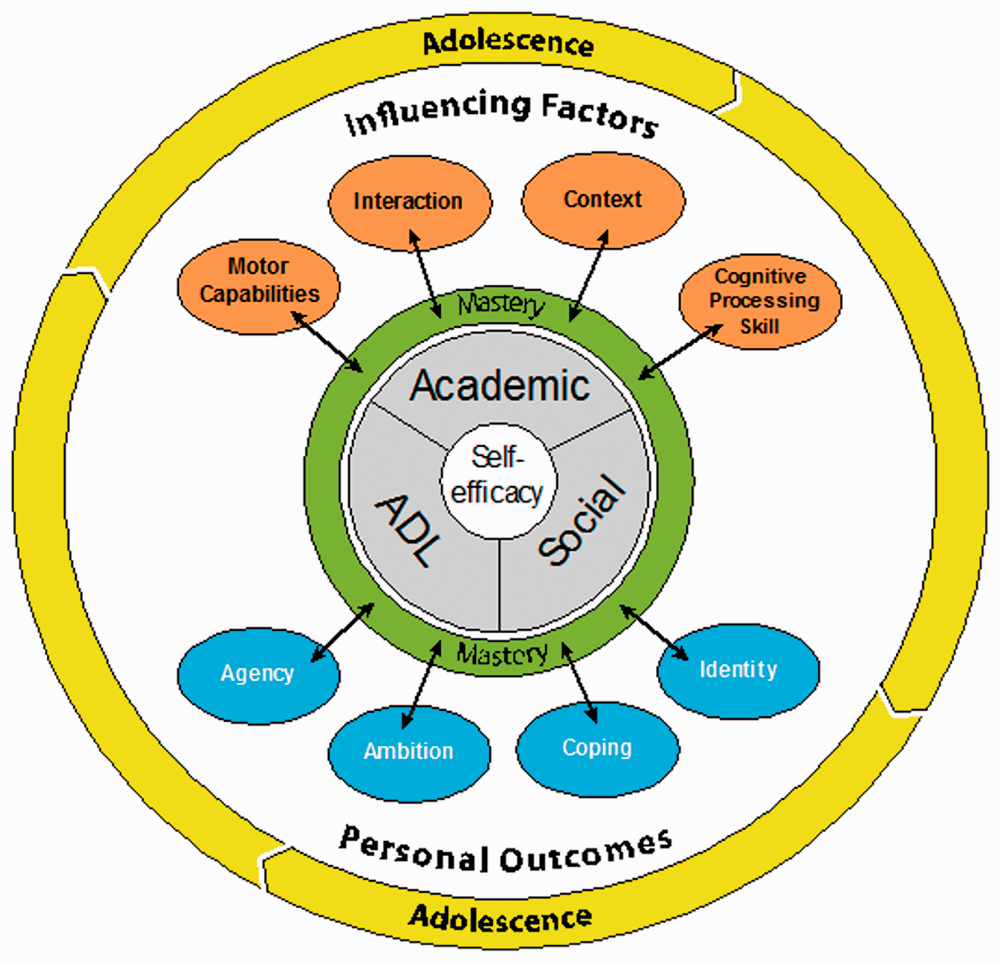
Conceptual framework illustrating the complex interaction of factors affecting the lived experience of teenagers with developmental coordination disorder.
Development of the conceptual framework
Conceptual frameworks are ‘a network … of interlinked concepts that together provide a comprehensive understanding of a phenomenon or phenomena’ (Jabareen, 2009: 51). The conceptual framework illustrates the functional domains of concern to teenagers with DCD; the personal and environmental factors that influence their performance of daily activities; and the impact of teenagers’ self-efficacy on their personal development and future ambitions. The conceptual framework will help researchers, occupational therapists and other professionals in health and education by enhancing understanding of the experience of DCD in adolescence and suggesting intervention approaches to support the development, participation and engagement of adolescents with DCD as they make the transition towards adulthood.
Self-efficacy
Central to the conceptual framework model is self-efficacy (Figure 1). Self-efficacy is concerned ‘not with the skills one has, but with the judgements of what one can do with whatever skills one possesses’ (Bandura, 1986: 391). Previous research into the self-efficacy of children with DCD has focused on efficacy for physical activity (see for example Batey et al., 2014), which is understandable as DCD is a disorder of motor function. Participants in the current study, however, expressed strong efficacy beliefs within the functional domains of activities of daily living, and academic and social activities.
By age 15 years participants felt they had developed the skills necessary to perform most basic self-care activities to a level that was: … not like perfect, but to a standard that’s OK. (George) Something sort of big, like lasagne or something like that, would be a bit of a project for me. (Ian)
Participants expressed strong efficacy beliefs about their academic abilities. While most considered themselves academically able, all were negative about their handwriting. This is not unexpected as poor handwriting is a feature of DCD (APA, 2013). Participants’ efficacy for learning was eroded, however, when others judged their ability by the poor presentation of their work: I ain’t got neat handwriting. I’m not getting pushed enough. I’m in the bottom sets for most things, not like the bottom sets but not the sets I should be in … They can’t read my writing and I’m not getting any marks on my tests. (David)
While friendships were important to all participants, some lacked confidence and motivation to engage in social activities. Ian doubted his ability to communicate effectively and was anxious that his comments might seem ‘random’ or ‘weird’ to others, and so he avoided interacting with people he didn’t know well. The risk of social isolation among young people with DCD has been highlighted previously (Dewey et al., 2002).
Influencing factors
Factors influencing participants’ self-efficacy, and thus their mastery and performance of activities at home, at school and during social activities, were their motor capabilities, cognitive processing skills, the context in which activities took place and interactions with others (Figure 1).
Motor capabilities
Unsurprisingly, participants’ efficacy was influenced by their motor abilities. David had difficulty coordinating the use of both hands together, which made him anxious about using cutlery in company: I can’t use a knife and fork neither. The food either goes on the floor or I make myself look like an idiot. (David) I struggle to comprehend why I can’t do it, what makes them so different that they can [score a goal, win a race] and I can’t. (Billy)
Cognitive processing skills
Participants experienced a range of additional non-motor difficulties, described in the conceptual framework as cognitive processing skills, that affected their performance and participation. This supports previous research linking poor motor coordination and poor executive functioning in adolescents with DCD (Leonard et al., 2015; O’Dea and Connell, 2016; Rigoli et al., 2012). Participants doubted their ability to organise themselves and process information quickly, creating feelings of disappointment, anxiety and confusion when they were unable to complete tasks as expected: I’m prevented from doing a lot of stuff [at Scouts] because I’ve forgotten something or I haven’t organised myself, so it’s not as enjoyable. (Billy)
Context
Participants’ efficacy perceptions varied according to the context in which activities took place. Self-efficacy was lower in environments where performance was measured against expected standards but was enhanced in situations where participation was valued more highly than performance. While Billy was happy to kick a football about with friends, for example, he was reluctant to play as a member of a team for fear of exposing his motor difficulties (see also Payne et al., 2013c): If it was a team sport with people that I didn’t know particularly well, then I wouldn’t want to get involved in case I got it wrong. (Billy) It’s better than being in the hall and struggling with my handwriting. (David)
Interactions
Interactions with others influenced participants’ efficacy perceptions. Negative comments about handwriting and presentation of work had a cumulative impact on participants’ capability perceptions (see also Payne, 2014): If someone said something to me, like a teacher about handwriting or something, I would just be less confident for the rest of the day. (George) I get to choose [equipment and support], but then they’ll obviously advise me on what route to take, but basically at the end of the day I feel it’s my decision. (George) Obviously they know I forget things regularly, but that’s just who I am … I think they like it about me, it just sort of makes me quirky. (Billy)
Efficacy-related outcomes
Participants’ sense of efficacy had consequences for their sense of agency, future ambitions, coping abilities and their sense of identity. These are described in the conceptual framework as ‘efficacy-related outcomes’.
Agency
Participants expressed strong efficacy beliefs about their ability to exercise control over the nature and quality of their lives. Having access to equipment and being involved in reviewing their progress and support needs enhanced participants’ sense of agency. David and Freya benefitted from a writing slope and were prepared to use it, even though it drew attention to their differences, because it improved their handwriting: The English teacher keeps it in her stockroom and gets it out so that’s quite useful. (David) She just don’t listen to me. She thinks she knows what’s best for me and I know what’s best for myself and no one accepts that ’cos I’m just a kid. (David)
Ambition
There was an association between participants’ efficacy beliefs, their career ambitions and motivation for learning, echoing the findings of previous research (Missiuna et al., 2008). Some felt practical careers were closed to them because of their coordination difficulties, while others believed they had the capacity to pursue professional careers and were motivated to work hard to achieve their ambitions: Just because someone has told you that you can’t do something doesn’t mean that you can’t do it. (Freya)
Coping ability
Participants’ coping ability and emotional resilience varied. Many experienced anticipatory anxiety, worrying about things that might happen and feeling anxious when faced with situations or tasks they had found challenging previously: I get stressed when I thought I am in trouble or I’m going to get in trouble, say if I forget my books or I haven’t done my homework then I would stress about it. (Billy) I’ve learned how to deal with it and put it in perspective. I’d worry about ridiculously small things and so I’ve tried to sort that out really. (Billy)
Sense of identity
In accordance with previous research (Lingam et al., 2014), sense of identity emerged as a strong theme. This was shaped by participants’ previous experience and by comparing themselves with others. Good exam grades reinforced Billy’s perception of himself as academically able, while being unable to use cutlery effectively made David ‘feel like an idiot’. Social comparison is a strong influence on identity formation (Festinger, 1954); the ‘hidden’ nature of DCD, however, made it difficult for participants to identify others to whom they could compare themselves. George, however, regarded the actor Daniel Radcliffe, who shares his diagnosis, as a positive role model: Despite the fact that he’s dyspraxic he’s achieved so much and done so much and it’s obviously good. (George)
Mastery and time
Mastery was revealed as both a source and product of self-efficacy, connecting all concepts within the conceptual framework. Participants described mastery experiences in all three functional domains (self-care, academic and social skills), while personal and contextual factors influenced whether or not their efforts to master an activity were successful. Participants needed more time, support and practice to master skills than their peers, and a strong sense of self-efficacy to persist when faced with setbacks and challenges. They were, however, motivated to invest time and effort in activities that were personally meaningful. Furthermore, mastering a task boosted their confidence and motivated them to aim for higher goals.
Participants’ efficacy perceptions were influenced by increasing competency demands and expectations over time; for example, participants were concerned about the growing gap between their handwriting skills and performance expectations: At primary school … I couldn’t colour in and stuff, but then loads of boys can’t. Then I went to secondary school at it got a lot harder for me to cope with. (George) I’ve dropped all the subjects I didn’t like, like art or DT and music, and I’m doing things that I like and I’m good at, so it feels a lot better. (George) Without me being clumsy then I wouldn’t be who I am. (Billy)
Discussion
This qualitative study set out to add to the limited literature exploring the lived experience of DCD in adolescence. Adolescence is a time of significant physiological, cognitive and emotional development for all young people and it is important to consider this natural maturation (which differs for boys and girls) within the context of this study. The findings suggest, however, some important differences in the experiences and development of young people with DCD compared to their peers during their early teenage years. Findings support previous research indicating that motor difficulties identified in childhood frequently continue into adolescence (Blank et al., 2019); continuing coordination difficulties affected participants’ motivation for and performance of physical activities at home, at school and during their leisure time. Adolescence is also a time when cognitive processes, including executive functions such as memory, problem-solving abilities and attention shifting, develop (Blakemore and Choudhry, 2006); the findings of this study support previous research indicating that difficulties in these areas persist in teenagers with DCD (Rigoli et al., 2012). Adolescence is also an important time for identity formation, which develops through a process of social comparison (Festinger, 1954). As DCD is a ‘hidden’ disability, however, it was difficult for participants to find a group of similar people to whom they could compare themselves, heightening their sense of difference. Uncertainty about their diagnosis also affected participants’ sense of what might be possible in the future. While adolescence is a time of natural maturational development, the findings of this study suggest that the experience of teenagers with DCD during adolescence is qualitatively different to that of their peers.
The study revealed the functional domains of concern to teenagers with DCD, furthering understanding of the impact of DCD on activity and participation, areas in which previous research is limited (Magalhães et al., 2011) and which is usually reported from the perspective of parents and professionals. The study also provides support for the occupational domains of concern that underpin occupational therapy theory and practice. The performance areas of concern to participants (activities of daily living, academic performance and social participation) map closely to the three categories of occupational purpose within the Canadian Model of Occupational Performance and Engagement (CMOP-E) (Polatajko et al., 2007): self-care, productivity and leisure. The close relationship between the functional domains of concern to participants and the occupational purposes in the CMOP-E support the validity of the CMOP-E as a theoretical model of occupational therapy.
Self-efficacy is an important but under-recognised factor affecting the participation of teenagers with DCD and their personal, academic and social outcomes. Previous research focuses on efficacy for physical activity; this is important as understanding why young people with DCD avoid physical activities will inform interventions to prevent negative health outcomes (Cairney et al., 2005; Wu et al., 2010). This study broadens understanding of the self-efficacy of teenagers with DCD beyond the physical domain, however, to include self-care, academic and social activities.
The study revealed that while participants felt they had the ability to perform activities of daily living and academic tasks to a high standard, they were often resigned to accepting a lower standard of performance because the physical and cognitive effort required to perform at a high level was unsustainable. The risk of dissatisfaction and disappointment when participants felt they hadn’t reached their potential is of concern as low levels of perceived efficacy are associated with an increased risk of depression (Gage and Polatajko, 1994). Poor self-efficacy (sometimes reinforced by the negative reactions of others) affected participants’ motivation to engage in certain activities or situations, limiting opportunities for them to develop skills and increasing the risk of social isolation. While avoiding activities might preserve teenagers’ self-esteem in the short term, there are long-term implications for quality of life if skills are not developed and activities not pursued in adolescence.
The study highlights the impact of teenagers’ capability perceptions on their choice of activities, the effort they were prepared to invest in mastering an activity, and their emotional and behavioural responses to failure and setbacks (Bandura, 1986). The study also highlights the complex interaction of personal and environmental factors that influence self-efficacy, which might help to explain why teenagers with similar motor and cognitive abilities perform activities at different levels, and why skills mastered in occupational therapy might not be transferred beyond the clinical setting (Gage and Polatajko, 1994).
Qualitative research aims to produce a trustworthy, credible account of social phenomena within a naturalistic setting. In this study, rigorous use of IPA enabled a rich, contemporaneous account of the lived experience of teenagers with DCD to be explored and a conceptual framework illustrating the factors that influence teenagers’ lives to be developed. The involvement of a reference group of older teenagers and young adults with DCD enhances the credibility and trustworthiness of this study by adding an ‘insider’s perspective’ to the analytical process. Moreover, the study design meant it was possible to observe changes in some participants’ narratives over time. A limitation of the study is that only one female participated. Future studies should include more young women in order to enable the transferability of the conceptual framework so a wider population of teenagers with DCD can be evaluated.
The study findings support the more optimistic developmental trajectory of DCD reported previously by people living with the condition (Lingam et al., 2014). This may not, however, reflect the experience of adolescents with DCD as a whole as participants in the current study were self-selecting. Despite the limitations identified, this study makes a valuable contribution to knowledge about the lived experience of teenagers with DCD, a population that has been largely ignored in the literature to date.
Implications for practice and research
The conceptual framework suggests new avenues for intervention and research to promote positive outcomes for teenagers with DCD. Findings indicate the need to broaden self-efficacy research beyond efficacy for motor performance. This would require the development of valid, reliable measures of self-efficacy for self-care, social and academic skills that could be used both in research and clinical practice (Poulsen et al., 2014). The need to assess executive functioning as well as motor capacity is also indicated, as participants’ difficulties extended beyond the motor domain.
The conceptual framework supports the benefits of a broad, systems-based approach to address the contextual and attitudinal barriers to the performance and participation of teenagers with DCD, particularly within the school environment. This would involve working collaboratively with teachers, parents and activity leaders to ensure their interactions enable, rather than inhibit, the performance and participation of teenagers with DCD. Occupational therapists have a key role to play in raising awareness and promoting understanding of DCD across these populations.
The conceptual framework indicates the value of interventions that build teenagers’ self-efficacy by developing skills and confidence to perform daily tasks and participate in activities that are important to them. Interventions should take account of any co-occurring conditions and their potential impact on mental and physical health outcomes. Creating enabling environments that balance accommodations, whilst providing opportunities for skill learning and development, is key to building self-efficacy and encouraging participation. Occupational therapists are skilled in using problem-solving, action-planning and reflective approaches that foster generalisation of skills and will enable teenagers’ self-management as they transition to adulthood. Furthermore, creating positive mastery experiences that build self-efficacy reduces the risk of secondary physical, social and mental health problems.
The study suggests anxiety management interventions as a means of building teenagers’ confidence, agency and resilience. Physiological symptoms of anxiety affect individuals’ belief in their ability to successfully perform an activity; helping teenagers to manage anxiety may therefore enhance their efficacy for coping with challenging situations and thus their occupational performance at school, in the community and in social settings. Further research into the use and effectiveness of anxiety management as an intervention approach for people with DCD/dyspraxia is recommended.
The findings of this study have important implications for occupational therapists who determine whether or not a person is eligible for intervention by their performance on standardised motor assessments. This approach disadvantages young people who have the physical capacity to perform a task, but whose performance and participation is limited by a lack of confidence in their abilities. Findings suggest young people with ‘borderline’ motor difficulties may benefit from support to enhance their self-efficacy, and therefore their performance and participation, in important activities at home, at school and in social settings. However, not all teenagers with DCD will require direct input from an occupational therapist; interventions might also include signposting to organisations that enable teenagers with DCD to meet others like themselves, such as the Dyspraxia Foundation; signposting to community groups that focus on fun and participation whilst promoting the development of skills; building the capacity of parents/carers and teachers to support teenagers’ self-efficacy and performance at home and school; and providing information about equipment and strategies to enable teenagers’ performance and participation in activities that matter to them.
Finally, the conceptual framework indicates that intervention outcomes should be measured not only by changes in task performance, but also by changes in teenagers’ sense of agency, resilience, identity and career ambitions. Occupational therapists’ expertise and understanding of the complex interaction between physical and mental health positions the profession well to support the self-management skills of teenagers with DCD and ensure a successful transition towards adulthood.
Key findings
The functional domains of concern to teenagers with DCD are activities of daily living, academic performance and social participation. Self-efficacy is a strong influence on the lived experience of teenagers with DCD, affecting teenagers’ confidence in their ability to perform academic, social and self-care tasks. Interventions for teenagers with DCD should focus on enhancing self-efficacy rather than simply developing motor skills to improve outcomes.
What the study has added
The study furthers understanding of the lived experience of DCD during adolescence and offers a conceptual framework illustrating the complex interaction of the personal and environmental factors that influence teenagers’ lives. The study suggests new avenues for intervention and research, and highlights the need for interventions that build teenagers’ self-efficacy, to promote positive futures for teenagers with DCD.
Footnotes
Acknowledgements
We would like to thank the young people who participated in this study, and the members of the reference group who so willingly gave their time. Thanks also to Dr Clare Taylor, Dr Katherine Wimpenny, Professor Andy Turner and Chris Bark for their support and guidance throughout the study.
Research ethics
Ethical approval was obtained from Coventry University (2014).
Consent
All participants provided written informed consent to be interviewed for the study.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Contributorship
The study was undertaken by Sally Payne for her PhD at Coventry University. Dr Gillian Ward contributed to the methodology, analysis and reporting of findings, and approved the final manuscript.