
Abstract
Introduction
Children and young people with developmental coordination disorder experience multiple occupational performance and participation challenges across environments. Research to date has not fully explored occupational therapy practice with children with developmental coordination disorder and their families. This study aims to describe current occupational therapy practice with children with developmental coordination disorder.
Method
This study used a cross-sectional, online qualitative vignette survey methodology. International occupational therapists who were working with or had worked with children with developmental coordination disorder within the previous 5 years were invited to participate. Following a case vignette, clinicians were asked questions prompting them to describe their practice based upon the vignette. The data were analysed thematically. The Consolidated Criteria for Reporting Qualitative Research and Checklist for Reporting Results of Internet E-Surveys reporting guidelines were adhered to.
Findings
Fifty-three valid responses were analysed. Analysis identified three themes describing occupational therapy practice with children with developmental coordination disorder: (a) a collaborative approach to establish occupation-focused goals; (b) occupation-focused assessment to guide therapy and diagnose developmental coordination disorder; and (c) the use of occupation-based interventions incorporating multiple strategies to enhance occupational engagement.
Conclusion
This study suggests that current occupational therapy practice with children with developmental coordination disorder is collaborative, occupation-focused, and multi-component. Findings highlight a gap between the complexity of practice and the nature of interventions evaluated in research to date.
Introduction
Developmental Coordination Disorder (DCD) is a common neurodevelopmental disorder with prevalence estimates of between 5% and 6% among school-aged children (APA, 2013) and wide-ranging impacts. A substantive body of evidence illustrates the negative consequences associated with this disorder, including poor physical health (Cairney et al., 2010), greater levels of internalising symptoms (depression and anxiety) (Omer et al., 2019), increased risk of victimisation and bullying (Campbell et al., 2012), and poorer educational outcomes (Harrowell et al., 2018). Children’s descriptions of living with DCD highlight that poor motor proficiency affects their capacity to join in and participate in typical childhood activities (Payne et al., 2013; Zwicker et al., 2018). Similarly, parents report less frequent participation in school and community settings for their child with DCD (Izadi-Najafabadi et al., 2019). Patterns of reduced participation are concerning, given that participation in everyday and organised activities is important for positive mental health outcomes for children with a disability (Berg et al., 2018).
Participation can be defined by two constructs: attendance and involvement (Imms et al., 2017). Attendance is defined as ‘being there’ and is measured as the frequency and/or range of diversity of activities in which an individual partakes (Imms et al., 2017). Involvement is defined as the experience of participation while attending and might include elements of motivation, persistence, affect, and social connection (Imms et al., 2017). International clinical guidelines (Blank et al., 2019) recognise the complexity of needs for the child with DCD and their family, and recommend that practitioners assess outcomes and examine intervention across the impairment, activity, and participation levels of the International Classification of Functioning, Disability and Health (ICF) framework (WHO, 2007). Occupational therapists use everyday life activities (occupations) therapeutically to enhance or enable participation in roles, habits, and routines in the home, school, and community (AOTA, 2014) and are therefore well placed to address the needs of people with DCD.
In the past, occupational therapy interventions for children with DCD tend to be categorised in the research literature as task-oriented or process-oriented. Interventions that target the underlying performance problems (for example motor skill training, kinaesthetic training, perceptual training, or combinations of these) are described as process-oriented (Smits‐Engelsman et al., 2013), and more recently impairment-focused (Smits-Engelsman et al., 2018). In contrast, interventions that use activity to improve the performance of motor tasks or occupations such as handwriting, cycling, or catching a ball for play-related activity are categorised as task-oriented interventions (Smits‐Engelsman et al., 2013). Contemporary thinking suggests that task-oriented interventions are activity-oriented but also facilitate participation (Smits-Engelsman et al., 2018).
A major challenge for occupational therapists trying to focus on participation in practice is the limited use of participation outcomes in occupational therapy intervention research to date (O’Dea et al., 2019). In addition, it is noteworthy that the associations between body function and structure, activity, and participation outcomes are not linear (Bonney et al., 2017). The evidence base for efficacious interventions that improve participation outcomes of children with DCD remains unclear (Miyahara et al., 2017; O’Dea et al., 2019). Some evidence indicates that the Cognitive Orientation to Occupational Performance intervention can improve task performance and satisfaction for client-centred occupational goals (O’Dea et al., 2019).
Alongside a lack of attention to participation outcomes, the existing literature on the efficacy of interventions does not give clear guidance for practice either. A newly published meta-review suggests that no robust evidence exists for any one approach for the treatment of children with DCD (Miyahara et al., 2020). Results from the one Cochrane review assessing the effectiveness of task-oriented interventions for children with DCD included 15 studies (eight randomised controlled trials (RCTs) and seven quasi-RCTs) that were judged to have moderate to high risk of bias. Data combined from six studies (two RCTs and four quasi-RCTs) in the meta-analysis found in favour of task-oriented interventions for improved motor performance compared to no intervention. However, a meta-analysis of two RCTs found no effect of task-oriented interventions for improved motor performance compared to no intervention. The authors concluded that task-oriented intervention may or may not improve motor skills more than inactive control (Miyahara et al., 2017). Equally, reviews of interventions to improve quality of life and psychological wellbeing for children with DCD are mostly inconclusive and limited by a lack of robust studies, limited controlled trials, and inconsistency of outcome measurement (Miyahara et al., 2017; Smits-Engelsman et al., 2018). In conclusion, evidence to date does not clearly inform and guide clinical practice for occupational therapists who wish to target participation for the child with DCD and their families.
Clearly, there is a pressing need to use robust methods to design, pilot, and trial interventions for children with DCD that include an assessment of participation outcomes to guide occupational therapy practitioners. Few studies describing occupational therapy practice for this population exist (Pentland et al., 2016; Withers et al., 2017). Furthermore, evidence suggests that occupational therapists have an awareness of DCD, but a knowledge gap may exist regarding the diagnostic criteria and clinical guidelines for assessment and diagnosis (Karkling et al., 2017). Consequently, it is difficult to evaluate the extent to which interventions tested in intervention studies to date reflect typical practice. This study aims to examine the content of occupational therapist practice for children with DCD. Understanding the content and context of current practice is critical to inform the future development, implementation, and adoption of any intervention for children with DCD (Craig et al., 2008).
Aim
The aim of this study was to describe current occupational therapy practice with children with DCD.
Methods
A cross-sectional, qualitative vignette survey was conducted online (Gray et al., 2017). A qualitative descriptive approach, as described by Stanley (2015), was selected to explore the clinical practice of occupational therapists internationally working with children with DCD. Ethical approval was obtained from the University of Limerick, Ethics Approval Number: 2019_02_04_EHS. The Checklist for Reporting Results of Internet E-Surveys (CHERRIES) guidelines (Eysenbach, 2004) and the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines were also adhered to (Tong et al., 2007).
Participants
Inclusion criteria were being an international occupational therapist who had worked with children with DCD (aged 5–18 years) in the past 5 years.
Recruitment
A recruitment strategy using two approaches was developed. Participants were sought via Twitter to maximise the potential sample and target a diverse representation of international occupational therapists (Gray et al., 2017). Convenience sampling was also used to recruit prospective participants via emailing members of the Association of Occupational Therapists of Ireland who had previously selected to be contacted for research purposes (n = 720).
Survey development
We developed an online survey involving a qualitative vignette. Clinical practice can be examined directly by observation, or indirectly via proxy measures such as interviewing clinicians (Hrisos et al., 2009), auditing medical records (Kolehmainen et al., 2020), or via clinical self-report of simulated behaviour in a clinical scenario using clinical vignettes (Hrisos et al., 2009). Direct measurement of practice is considered a ‘gold standard’. However, this is not always an ethical or feasible methodology (Hrisos et al., 2009). The use of clinical vignettes provides a valuable tool for studying practice-oriented questions (Gray et al., 2017), whereby the clinician reports how they would respond to a simulated patient in a case vignette (Hrisos et al., 2009). Given our research aim, we selected an online survey with a qualitative vignette as it is a resource-light, non-intrusive means to explore topics within a relatively large, geographically dispersed occupational therapy workforce (Gray et al., 2017).
The case vignette was purposefully developed by the study authors (ÁOD and KR) as a hypothetical but realistic case study reflecting the available literature on DCD (Blank et al., 2019), physical health outcomes of DCD (Cairney et al., 2010), emotional wellbeing and mental health consequences of DCD (Omer et al., 2019), and common experiences of bullying and exclusion reported by children with DCD (Campbell et al., 2012; Zwicker et al., 2018). The online supplementary material contains the full survey and the case vignette used in this study.
The online survey began with four questions related to consent and use of the data in this study, followed by seven questions on demographics and clinical experience. The remaining questions were presented after the case vignette. Five open-ended questions asked clinicians to describe their typical practice based upon the case vignette, including (a) their approach to assessment; (b) a multiple-choice selection of the possible assessments that they would undertake; (c) the possible intervention(s) that they might undertake; (d) how they would evaluate the outcomes of an intervention; and (e) any further information that they wanted to add. A further three open-ended questions related to the frequency, intensity, and location of intervention.
The survey was piloted with two senior occupational therapists working with this population group. Feedback was provided on the survey’s usability, clarity, and association with the research questions. The survey included the responses of these practitioners. The final survey involved 21 items and took approximately 20 minutes to complete during piloting. The survey was conducted using the online survey system Survey Monkey, which is a password-protected, web-based platform. Participants completed the survey at a time and location of their choosing. No identifying data on the participants was collected. The survey link was active from 17 September 2019 to 21 October 2019. Data were exported to QRS software NVivo 12.
Data analysis
This study used thematic analysis as described by Braun and Clarke (2006) to identify patterns of meaning across the survey data. The researchers were interested in the occupational therapists’ views of current practice and contribution to promoting the health, wellbeing, and participation of children with DCD through engagement in occupation. Respondents had to answer at least one qualitative question for the survey data to be included in the thematic analysis. Survey data from each respondent was read as a whole. Subsequently, ÁOD and KR independently coded 10 randomly selected surveys using an inductive approach focused on the overall aim of the study to describe occupational therapy practice with children with DCD. The codes generated by ÁOD and KR were compared, discussed, and refined. ÁOD continued coding the remaining data independently. Codes were compared across the datasets to identify patterns of similarity and difference, as suggested by Braun and Clarke (2006). Several meetings were convened to discuss the codes, examining the relationship between and across the codes. Following this, the researchers grouped the codes into categories and developed provisional theme names. The authors’ interpretations of the data and key quotations to represent the views of the participants are presented in the results section. Descriptive statistics were used to describe the demographic characteristics of participants (Table 1).
Demographics of survey respondents (n = 73).
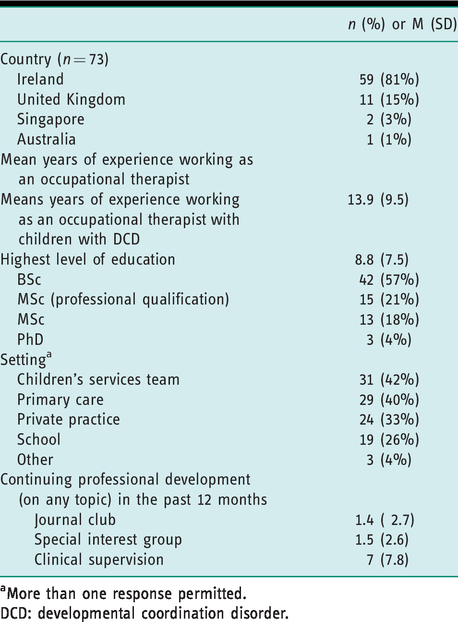
aMore than one response permitted.
DCD: developmental coordination disorder.
Throughout the study process, the authors engaged in reflexive discussions of the aims, the design of the qualitative survey, and interpretation and understanding of the data. ÁOD is an occupational therapist with 20 years’ clinical experience working with individuals with DCD, and is a PhD candidate. SC and KR have extensive research methodology experience but do not have a background in paediatric occupational therapy. ÁOD completed a reflexive diary as a means to increase awareness of how her previous clinical practice, commitment to the profession of occupational therapy, and views on concepts such as participation were influencing the data analysis process. Through discussions with KR, these reflexive insights were acknowledged and challenged, supporting a robust approach to analysis.
Results
The online survey received 90 responses. Seventeen respondents did not proceed past the consent page and 20 respondents completed the demographic information but did not answer at least one qualitative question regarding the case vignette; hence, 53 responses were included in the qualitative analysis.
Participant demographics and practice characteristics
Table 1 displays the participant demographics and practice characteristics. The majority of participants were working in Ireland (81%) and the United Kingdom (15%). A small number of participants from other international contexts were recruited (n = 3), one working in Australia and two working in Singapore. No differences were noted when these three responses were compared with others across the dataset with regard to the context and nature of occupational therapy practice; therefore, they were included in data analysis. The mean years of experience working with children with DCD was 8.8 years. The highest proportion of occupational therapists had obtained a Bachelor of Science award (57%).
A collaborative approach to setting occupation-focused goals with children and families
Therapists described engaging in a collaborative process of occupation-focused goal-setting with the child, parents, and other stakeholders.
Collaboration with parents, children, and other stakeholders was described as central to the process of establishing goals for therapy. The majority of therapists (47/53) described a process of goal-setting, supported by the use of pre-assessment questionnaires with key stakeholders (parents and teachers) in advance of face-to-face meetings. These therapists described using strategies such as adopting a relational approach, developing rapport, adopting a strengths-based approach, using interview skills or narrative reasoning skills, and listening to the child and family during goal-setting: “Interview with Jacob – explore interests, level of insight, motivation, attention and concentration, and priorities etc. I would work collaboratively with parents and Jacob to decide on goal areas” (Respondent 45, Ireland). I have shifted my focus to asking the child what they want to be able to do better. For example, ‘I want to be able to catch the ball in the air at hurling’ or ‘I want to be able to tie my shoes’ (Respondent 49, Ireland).
A few therapists reported using a formal goal-setting tool such as the Perceived Efficacy and Goal Setting (PEGS) system (2/53) or the Canadian Occupational Performance Measure (COPM) (3/53) to identify goals. Similarly, a small number reported using a standardised tool to review outcomes (13/53). Many therapists (33/53) reviewed and measured goal-achievement via feedback from the child, parent, or teacher: ‘I would review ADL [activities of daily living] with parents, review Jacob’s experiences and self-evaluation, get updates from school’ (Respondent 57, Ireland).
Occupation-focused assessment to guide therapy and diagnose DCD
This theme reflects the in-depth, occupation-focused assessment that therapists engage in, which examines the criteria required for a diagnosis of DCD and is simultaneously used to guide future therapy. Goal-setting re-emerged as a concept within assessment; it was not a discrete step in the therapy process, but rather it was embedded in both assessment and intervention.
The majority of therapists (52/53) describe an assessment process that fulfils the requirements to assess criteria A, B, and C for the diagnosis of DCD according to the DSM-V. Therapists described systematically evaluating the child’s acquisition and execution of motor skills via standardised motor proficiency, handwriting, perceptual, and sensory processing assessments (see Figure 1). I would help the parents and child identify priority areas of concern and assess these areas to help set goals and make an intervention plan. I would use the Movement ABC 2 if considering a diagnosis (Respondent 88, United Kingdom). Assessments used to facilitate a diagnosis. ‘Engage him in play … observe whether he can come up with his own ideas for play and expand on these’ (Respondent 86, United Kingdom).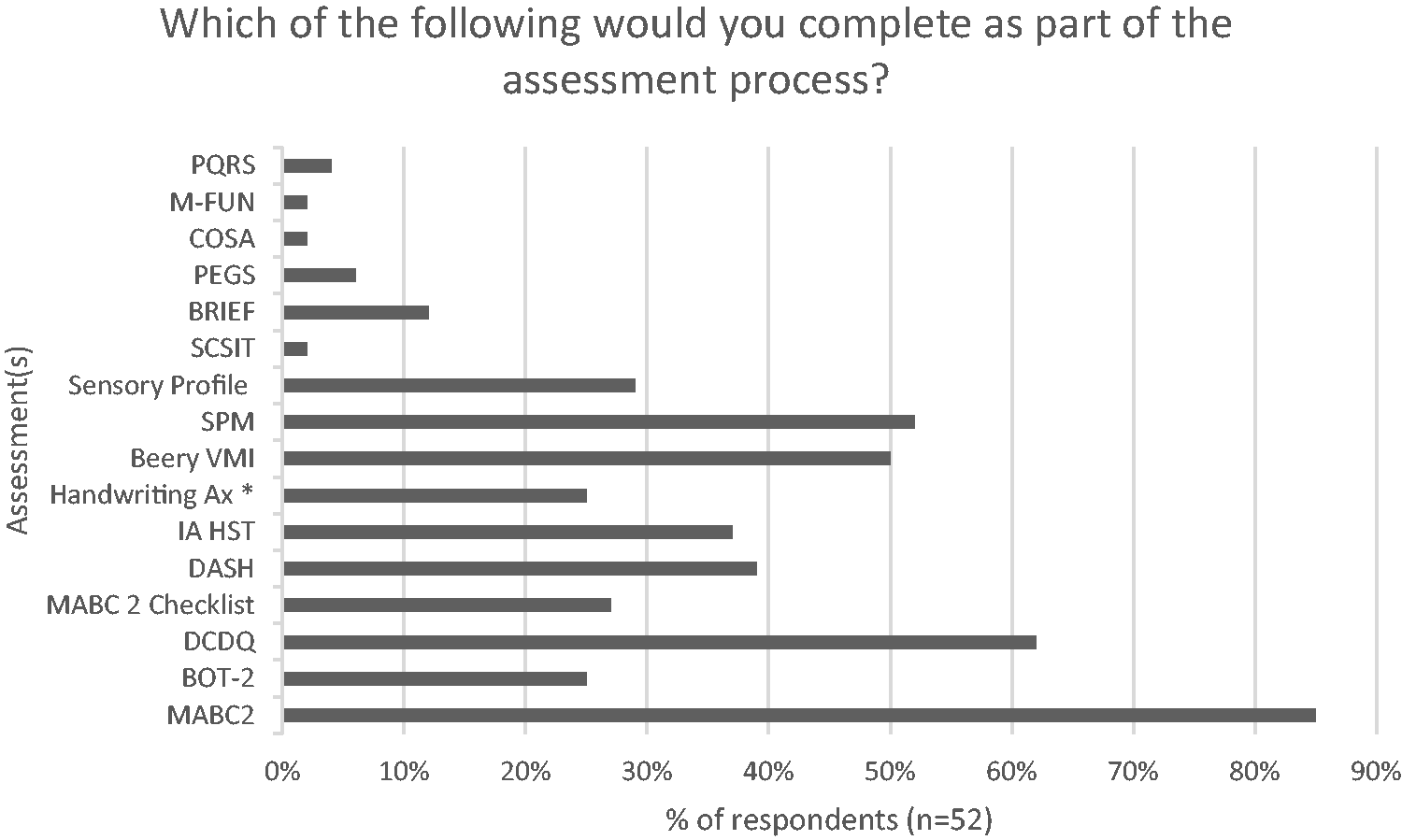
A significant proportion of therapists describe school-based assessment and consultation with the teacher (31/53). School-based assessment included observation of the child’s engagement, performance, and participation in order to understand the context of activity performance, environmental issues, and inform future task or activity modifications and recommendations. School assessment typically incorporated therapy, which targeted increasing the teacher’s awareness of DCD: ‘Discussion with Mum and Jacob regarding school, and how he is coping. A school visit to observe him in Physical Education and his environment; provide advice, strategies, and equipment if necessary’ (Respondent 90, United Kingdom).
Predominantly, occupational therapists were the primary professionals involved in the assessment of DCD; referrals to physiotherapists, educational psychologists, paediatricians, and general practitioners were made as required. A small number of therapists (5/53) described working in settings that provided a multi-disciplinary DCD assessment. Participants did not explicitly mention discussing the impact of a diagnosis of DCD with the parents, bar one notable exception: ‘Many children and their families experience significant frustration, as this journey has required different referrals to different services’ (Respondent 65, Ireland). The assessment feedback consultation can be a long session (1.5 hours). Explaining how to help the child and understanding why activities are difficult … helping the parents to understand the difficulties and getting them to set 1–2 goals at home, encouraging them not to set too many goals. We look at what they are currently doing and how they could adapt that to improve their child’s performance or to encourage a bit more independence (Respondent 20, Ireland).
Therapy involves occupation-based interventions incorporating multiple strategies to enhance the child’s occupational engagement/performance
This theme describes the interventions therapists proposed using in response to the case vignette. Most therapists proposed therapy that was goal-focused and occupation-based. Almost all therapists reported the use of a multi-component intervention that included the child, parent, and/or teacher, which addressed everyday occupations and/or the environment. Interventions incorporated several approaches or strategies in tandem (52/53). Occupation-based interventions that reflected a task-oriented approach with embedded cognitive, motor, psychosocial, and education-based approaches were described. Interventions were delivered via child-focused interventions and parental and teacher consultation.
Almost all participants used a task-oriented approach that involved using activity to improve the performance of occupations such as handwriting, cycling, and catching a ball for play-related activity (52/53). Skills practice [using] cutlery … making this motivating and fun for Jacob. Using obstacle courses to develop bilateral coordination, postural control … incorporating Jacobs’s interests, such as computer game characters. Cognitive Orientation to daily Occupational Performance (CO-OP) approach to learning new skills. Discuss strengths and areas to develop with Jacob, and provide continuous feedback regarding progress and effort put in (Respondent 58, Ireland). I would look at handwriting, knife and fork skills, activities of daily living skills such as dressing. Practice component parts … create a checklist of complete task – goal, plan, do, check. Play a task such as Lego … grade the task, follow instructions to create Lego, discuss levels of assistance (Respondent 51, Ireland). So for this child, I would guess that being better at soccer might be a good motivator so that we might drill football skills … to improve his ability to anticipate where the ball will be, and reduce anxiety around performance (Respondent 49, Ireland).
Education was integral to several interventions, including post-assessment feedback, parental workshops, teacher and parental consultations, and child-focused intervention. Education-based interventions aimed to increase a person’s understanding of DCD. Many participants addressed the impact of DCD on the child’s health, wellbeing, and participation in different environments (42/53). Parent workshop – education on motor development, emotional/sensory regulation … importance of ‘just right’ challenge, using practical activities to experience what it’s like for a child with difficulties, and how it may impact participation, motivation, avoidance of tasks, self-esteem/confidence/anxiety etc. (Respondent 13, Ireland).
Therapists commonly described parent-focused interventions (39/53). Different terms were used interchangeably to describe the mode of delivery, for example ‘parent consultation’ (n = 17), ‘home programme’ (n = 14), and ‘parental coaching’ (n = 8). Common features of these interventions included spending time listening to the child and parents, sharing information, joint problem-solving of how to support occupational performance, ensuring the proposed intervention is motivating and achievable, and supporting parents to implement strategies outside of therapy such as scaffolding activities and activity modification. I would provide recommendations, guidance, and coaching to school and parents, as to how to support Jacob in the development of selected tasks that he wants to or needs to develop, including handwriting, riding a bike, soccer, the use of cutlery, etc. These supports for Jacob are focused on increasing Jacob’s ability to carry out the targeted activities as well as on modification of the task and his physical and social environment (Respondent 55, Ireland). ‘I have run a lovely group on how to build an engine for boys with fine motor skills difficulties; unfortunately, I have not run this in a year because of staffing shortages’ (Respondent 20, Ireland).
Discussion
This qualitative study of occupational therapy practice with children with DCD revealed that therapists use a client-centred collaborative approach to setting occupation-focused goals. Participants’ occupational therapy practice involves a detailed occupation-focused assessment whereby multiple sources of information about the child, environment, and occupations are collated in order to guide therapy and diagnose DCD. Therapy descriptions involved occupation-based interventions incorporating multiple components and strategies to enhance the child’s occupational performance and participation across home, school, and community environments. Overall, the three themes reflect an occupation-based approach; that is, the ‘doing’ of occupation comprised the principle elements of evaluation, intervention, and outcome measurement (Fisher, 2013).
In line with best practice guidelines and research evidence, participants in this study reported using interventions that targeted participation (Blank et al., 2019; Smits-Engelsman et al., 2018; WHO, 2007) and reported using key intervention ingredients that strengthen children’s participation in everyday life, as described by Armitage and colleagues (2017). Almost two decades ago, distinguished occupational therapy scholar Mary Law stated that facilitating participation in everyday occupations is the reason for occupational therapy (Law, 2002). Respondents in this study did not explicitly use the language of participation to describe their approach to therapy. However, their reports reflected the principles of participation-based therapy, including use of a goal-oriented, family and child centred, collaborative, strengths-based, ecological, and self-determined process (Palisano et al., 2012). In contrast, previous research has suggested that Allied Health Professionals (AHPs) find it challenging to implement participation-focused services (Kolehmainen et al., 2020; Pentland et al., 2016). Audit of clinical documentation suggests that less than a third of cases treated by AHPs targeted participation outcomes, and the child and parents rarely collaborated on these outcomes (Kolehmainen et al., 2020). However, experienced clinicians can find it difficult to articulate their intervention in clinical documentation, as they have internalised the key ingredients that they use in activities (Zanca et al., 2019). Although these findings about the enactment of participation in practice are reassuring, it is also important that occupational therapists should use the language of participation when talking to children, families, and stakeholders, and in their clinical documentation.
In keeping with current research, the case vignette described social exclusion, bullying, and social participation issues for the child with DCD (Campbell et al., 2012; Zwicker et al., 2018). Respondents considered the school context and environment in class, during physical education, and at break-time. However, the respondents did not use terms such as social exclusion or bullying when describing practice. D’Elia and Brooks (2017) suggest that occupational therapists do not proactively address bullying in school settings. Multi-component anti-bullying interventions that target parent education, improved playground supervision, and classroom management are effective in reducing bullying and victimisation (Arbesman et al., 2013). In addition, occupation and activity-based interventions that concentrate on social–emotional learning have the potential to enhance children’s psychosocial wellbeing (Arbesman et al., 2013). Respondents’ practice influences the child’s psychosocial wellbeing given the multi-component interventions delivered, including occupation-based interventions, parental education interventions, increasing teacher awareness of DCD, and targeted self-regulation programmes that aim to improve social behaviours and reduce problem behaviours for the child (Arbesman et al., 2013).
This study revealed that the child’s play interests and goals were important aspects valued by respondents. Goal-setting that embraces the client’s perspective has the capacity to promote motivation, engagement, self-efficacy, and meaningful participation (McBryde and Ziviani, 2020). Similar to previous findings, respondents used play occupations in diverse ways during intervention, including play as a means to an end, play as a mode of engagement and motivation, and play as a primary occupation (Lynch et al., 2017). Children with DCD experience social and emotional difficulties as result of being excluded from play (Zwicker et al., 2018). However, play as intervention and measurement of play as a participation outcome has received limited attention within DCD research to date (O’Dea et al., 2019).
Therapists utilised multiple intervention approaches including cognitive, CO-OP, play-based, psychosocial, and education interventions to target goals and outcomes for different stakeholders. Withers et al.’s (2017) study of Canadian occupational therapists reveals a similar pattern: 94% of respondents used multiple interventions or approaches to treat children with DCD. These descriptions align with the definition of a complex intervention, described by the Medical Research Council (MRC) (Craig et al., 2008) as interventions with several interacting components, targeting multiple groups, and attempting to affect multiple outcomes at varying organisational levels. Similarly, these findings also align with Pentland and colleagues’ analysis of occupational therapy as a complex, dynamic process, comprising multiple and varied interventions or practices (2018).
The complexity of current practice illuminates a gap between practice and research evidence. RCTs to date have not explored the outcomes of multi-component occupation-based practice for children with DCD. Even though no robust evidence exists for any one approach for the treatment of children with DCD (Miyahara et al., 2020), Reedman et al.’s (2019) RCT of participation-focused therapy for children with cerebral palsy embraced the challenge of complex intervention development and comprehensively reported the content of a complex intervention. Studies such as those by Reedman et al. (2019) demystify the ‘black box’ of rehabilitation by explicitly describing the problem (treatment aim or targets), and what ingredients in their treatment are expected to produce which specific functional changes (Dijkers, 2019).
Conclusion
The findings of this study must be interpreted with caution as the sample cannot be considered representative of occupational therapists working with children with DCD. However, across the dataset themes were identified that suggest that occupational therapy practice with the child and family with DCD is collaborative, occupation-focused, multi-component, and appropriately complex. The content of interventions reflects practice guidelines, which recommend that interventions should target function, participation, and psychosocial wellbeing (Blank et al., 2019). This complexity of practice is in stark contrast to the wider body of intervention research for children with DCD, whereby one intervention approach is trialled and evaluated in isolation. Future research needs to examine the use of multi-component occupation-based interventions to target participation outcomes. The findings from this study offer valuable insights into the ‘black box’ of occupational therapy practice for children with DCD. As such, the results may help to address the gap between practice and research in the development of future interventions (Craig et al., 2008).
Strengths and limitations
To our knowledge, this is the first qualitative description of the practice of occupational therapists with children with DCD. We employed a novel method, our findings present a rich description of practice, and we identify future research directions.
The qualitative vignette online survey allowed us to collect detailed accounts of what participants would do in practice from a larger group than would be feasible to conduct in in-depth interviews. However, qualitative interviews would have allowed probing of responses and potentially a more in-depth exploration of factors influencing practice.
Our recruitment strategy may have led to participant bias as self-selecting participants may have led to over-representation of those proactively engaging in continuing professional development. Furthermore, a third of the sample (33%) worked in private practice, which may not reflect the practice context of those working in public health services and the profile of children attending private services likely differs in characteristics such as socioeconomic status compared to those accessing public services. Furthermore, although 90 participants started the survey, 43 did not contribute to the qualitative data and were not included in analysis. We do not know the reasons for non-completion. However, it is important to note that our sample may not be representative of current occupational therapy practice in the wider population. Finally, our study focuses only on therapists’ descriptions of practice; service users’ perspectives were not solicited.
Future research examining children’s, parents’, and therapists’ experiences of occupational therapy practice using interview and observation-based methods is warranted to inform intervention and service development.
Key findings
A focus on occupational engagement and participation is core to occupational therapy practice with children with DCD.
There is a pressing need to examine multi-component occupation-based interventions for children with DCD that target participation outcomes.
What the study has added
This study has highlighted the significant gap in the complexity of practice interventions evaluated in research to date.
Supplemental Material
sj-pdf-1-bjo-10.1177_0308022620944100 - Supplemental material for Occupational therapy practice with children with developmental coordination disorder: An online qualitative vignette survey
Supplemental material, sj-pdf-1-bjo-10.1177_0308022620944100 for Occupational therapy practice with children with developmental coordination disorder: An online qualitative vignette survey by Áine Emma O’Dea, Susan Coote and Katie Robinson: in collaboration with the Research and Audit Federation of Trainees (RAFT) network in British Journal of Occupational Therapy
Footnotes
Research ethics
Ethical approval was obtained from the University of Limerick Ethics Approval Number: 2019_02_04_EHS.
Consent
All participants provided written informed consent prior to completing the survey.
Declaration of conflicting interests
The authors declared no potential conflicts of interest concerning the research, authorship or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The author, ÁOD disclosed that she is a full-time PhD scholar on a structured PhD programme in health service research and population health, funded by the Health Research Board (SPHeRE/2013/1), Ireland. This programme funds postgraduate fees and a stipend for four years.
Contributorship
Áine O’Dea had the primary responsibility for conceptualization, methodology (survey design, and data analysis), project administration, and writing – original draft preparation, review and editing. Susan Coote contributed to the conceptualization, methodology, supervision, review and editing of the original draft preparation, and final versions of the manuscript. Katie Robinson contributed to the conceptualization, methodology (survey design, and data analysis) supervision, reviewing and editing the original draft preparation, and final versions of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.