
Abstract
Introduction
Occupation-based practice is a core tenet of occupational therapy. This study explores perspectives and experiences with occupation-based practice among Thai occupational therapists.
Method
Using mixed methods, a focus group was conducted with eight occupational therapists, and the results were interpreted using thematic analysis. A questionnaire survey was also completed concerning practitioner perspectives (n = 216).
Findings
Three major themes were identified: (a) perspectives on occupation-based practice were related to practice areas and felt to strengthen the identity of occupational therapy (52% strongly agree), leading to improved services and better outcomes for clients (44% strongly agree); (b) approaches focused on activities of daily living were appropriate for cross-practice areas; and (c) occupation-based practice is consistent with integrated medical sciences and occupations for clients (52% strongly agree).
Conclusion
Implementing occupation-based practice will be of value to clients, provide benefits as a compass to direct processes, and enhance clinical reasoning and outcomes.
Introduction
There are currently 1376 occupational therapists serving the country of Thailand, which has a population of 67 million (Bureau of Sanatorium and Art of Healing, 2020). Moreover, there are only two occupational therapy school providers for the nation. The first occupational therapy educational programme was founded in 1980 at Chiang Mai University in northern Thailand (Vinyuwat, 1983), and the second school was established in 2008 at Mahidol University in Bangkok, the capital city of Thailand (Faculty of Physical Therapy, 2019). As a result, Thai occupational therapy practice has slowly been developed over nearly 40 years, and practitioners currently work in settings such as hospitals, out-patient clinics, schools, and government organizations.
Occupational therapy is a powerful means for enhancing participation in everyday life activities and shows a direct link to health and wellbeing (Law, 2002). The occupational therapy process was established as the engagement in various daily occupations that promote and reinvigorate the individual’s health and function. Occupation embraces activities of daily living (ADL), instrumental activities of daily living (IADL), rest and sleep, education, work, play, and social participation (AOTA, 2014). Previously, the adoption of medical models encouraged practitioners to establish a rationale for practice. As a result, occupational therapists began to focus more specifically on bodily functions and impairments rather than using occupations and holistic approaches to guide them.
There are currently limited frameworks for Thai occupational therapy in both academia and clinical practice that fit with the cultural context. Clarification is needed to relate occupation and activities in practice to individual, group, and cultural contexts (Morris et al., 2000). Hence, the use of occupation-based practice (OBP) should be a core principle to increase occupational performance and engagement. According to Polatajko and Davis (2012), OBP is based on occupational engagement and integrity to client performance and participation goals. Applying OBP is useful; however, the occupation in practice must be evidence-based in order to support the intervention approach that enables the client to meet the occupational adaptation and goals with the best outcomes. Contemporary paradigms encourage the reintegration of occupation as the core of therapeutic interventions and to provide clinical reasoning in practice. This paradigm shift focusing on OBP has led to a more client-centred approach (Kielhofner, 2009). Implementing OBP into occupational therapy educational programmes should be considered in multi-dimensional aspects based on the benefit and value of learning outcomes to occupational therapy students. This may be a primary strategy for educating Thai occupational therapy practitioners in the future.
Literature review
OBP is central to occupational therapy and reflects the uniqueness of the profession, and also provides an identity separate from other disciplines. OBP refers to occupation as a means and an end in utilizing meaningful and purposeful activities based on the client’s needs, health, and engagement in everyday life (Trombly, 1995). The use of occupation as a ‘means’ is a process or method of intervention, while the “end” is the outcome of the intervention (Radomski and Latham, 2008). OBP emphasizes the use of an individual’s or family’s occupation as the form of intervention to promote positive changes in the direction of the occupational goals (Price, 2004; Price and Miner, 2007). Occupational therapists embrace an occupation-centred perspective (Fisher, 2013) using an occupational lens (Rodger, 2012) to implement OBP. This encourages occupational therapists to better understand the nature of their clients’ occupational performance, clients’ needs, and the relationship between occupational goals and outcomes. However, the use of OBP in developing countries such as Thailand may be more challenging due to the different physical, cultural, and social contexts related to occupational therapists’ experiences and perspectives. In societal and cultural norms, Thai culture has been linked with collectivism and interdependent self-construal, whereas Western cultures link with an individualism that tends to support more self-directed behaviour and give priority to individual goals (Hofstede, 1997; Markus and Kitayama, 1991). Thai people tend to have close relationships with extended families that are comprised of grandparents, uncles, aunts, grandchildren, and sometimes neighbours and co-villagers (Suttajit et al., 2010). Thus, the collectivism and interdependent self-construal of Thai culture has affected occupational therapy practitioners in providing OBP to clients.
Moreover, the Association of Southeast Asian Nations (ASEAN) University Network (AUN) was a key implementing agency in the sociocultural portfolio of the ASEAN Charter in 2007. The AUN is comprised of 30 universities from 10 ASEAN countries. The Network encourages higher education and collaboration to strengthen regional integration in five areas: (a) youth mobility; (b) academic collaboration; (c) standards, mechanisms, systems, and policies of higher education collaboration; (d) courses and programme development; and (e) regional and global policy platforms (AUN, 2012).
Currently, Thai universities embrace a model of outcome-based education and educational theory to help learners to meet learning outcomes (Spady, 1994). To achieve outcome-based education, the AUN – Quality Assurance (AUN-QA) programme was established for promoting, developing, planning, organizing, monitoring, and evaluating educational programmes and learning activities (Johnson, 2017). Mahidol University is one of the institutions that participates in the AUN. The occupational therapy programme was impacted by the policy and determined to be one of the curricula assessed by the AUN-QA. The key objective of the AUN-QA process is to create anticipated learning outcomes, in which OBP was established as part of the essential knowledge and abilities that students should possess after programme completion. To meet the ASEAN objectives, OBP has been a core component and outcome of occupational therapy education and the profession. Hence, it will be a major change in the future Thai occupational therapy community as this initiative grows.
As a result, factors related to Thai collectivist culture, the ASEAN educational framework, and the shortage of occupational therapists, practitioners, and educators must apply culturally relevant OBP to meet the needs of society. Therefore, the aims of this study were to describe how therapists in Thailand view OBP, perceive the use of occupation in practice areas, and express their perspectives regarding areas of occupation and future expectations for occupational therapy students.
Method
A mixed-methods design was conducted to collect both focus group and survey data from occupational therapists in Thailand. The qualitative inquiry reflected the therapists’ experiences in the use of OBP. The survey explored the therapists’ perspectives towards OBP, ranking of occupational areas, and future expectations for occupational therapy students. This research received ethical approval from the Mahidol University Central Institutional Review Board, reference number 2015/076.2205.
Focus group procedure
The interview guideline was developed and refined by an iterative process involving mock focus groups prior to its use. Semi-structured interviews were comprised of:
OBP perspective: (a) What is OBP in your viewpoint? (b) Why do Thai occupational therapists need to use OBP? Areas of occupations in the OBP: (c) What are the occupations that you use for intervention with clients? (d) How do you select occupations and activities in the use of OBP? OBP for students: (e) What knowledge and skills are important for occupational therapy students in the use of OBP? (f) What are your thoughts about the occupation-based curriculum in occupational therapy programmes? (g) What are your thoughts about implementing OBP during student fieldwork?
Based on a guided design, the process was organized in a natural and logical sequence. The location was in a comfortable setting and relaxed atmosphere.
Survey procedure
A questionnaire survey was developed and contained questions in four parts: (a) individual profile, workplace location, and occupational therapy specialty; (b) the degree of perspective through OBP; (c) most common areas of occupation for intervention; and (d) future expectations for occupational therapy students. This questionnaire was validated by three experts, which presented a score of 0.97 for index of item objective congruence (IOC).
Examples of questionnaire items are: What do you think OBP can demonstrate in the identity and uniqueness of Thai occupational therapy? Do you think that Thai occupational therapy students will use OBP in fieldwork? Participants were asked to rank their opinion using a five-point Likert scale: (1) strongly disagree, (2) disagree, (3) neutral, (4) agree, and (5) strongly agree. This questionnaire required approximately 15–20 minutes to complete.
Focus group participants
Participants were recruited based on the following criteria: (a) possessing an occupational therapy national licence; (b) being a graduate with a master’s degree; (c) having practised in different fields (paediatrics, physical dysfunction, and mental health); (d) having more than 10 years occupational therapy experience; (e) having worked as clinical instructors (CIs); (f) working in the city of Bangkok and outskirt areas; and (g) willingness to participate in the focus group. The focus group participants were excluded from the survey to avoid data duplication.
The recruitment process was based on convenience for participants and pragmatic reasons relevant to the above criteria. Advertisements were placed in hospitals in Bangkok city and surrounding areas for 2 months. After participants contacted the research team, they were selected based on the above inclusion criteria.
Survey participants
There were 1376 Thai national occupational therapy licencees (Bureau of Sanatorium and Art of Healing, 2020) eligible for the survey. Three hundred practitioners were selected by purposeful sampling based on the following criteria: (a) possessed occupational therapy national licence; (b) worked full-time in public or private institutions; (c) had more than 2 years’ experience in occupational therapy service; and (d) demonstrated good communication skills.
Data collection
The data were collected in September 2016. The researcher contacted the occupational therapists based on the criteria to determine the most convenient time and location for a focus group. This was conducted by a moderator to elicit information as expressed in the guidelines. Each participant was required to read and sign a written consent form before the group interview. This study was audio-recorded and transcribed verbatim. The focus group took place for 2 hours 30 minutes, and pseudonyms were used to protect the confidentiality of the participants.
Questionnaires and consent forms with cover letters and stamped return envelopes were sent to 300 participants at their institutions across the country in November and December 2016. All participants read and signed consent forms before answering the questionnaire. Information was gathered on the nature of services in the participant workplace, but the names and addresses of organizations were not identified.
Data analysis
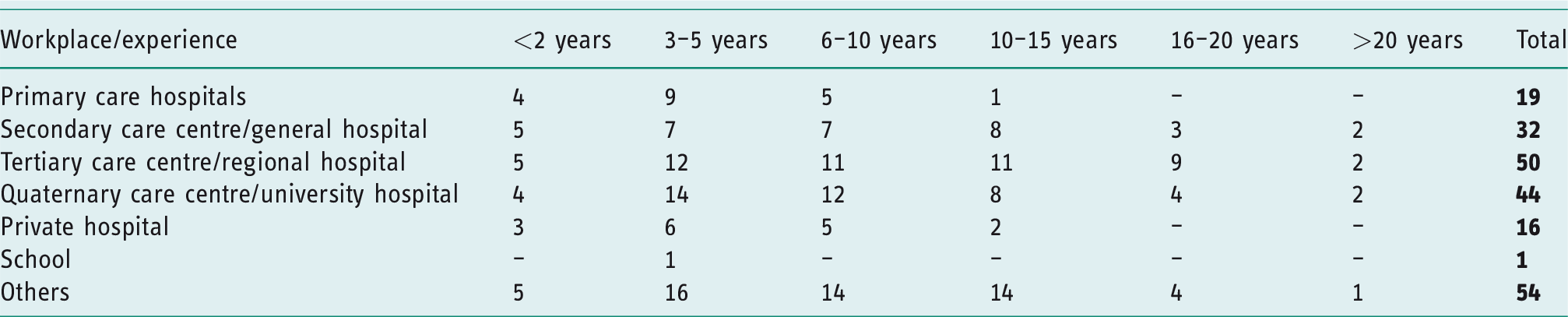
Six female and two male occupational therapists (mean age = 39.4 years) participated in the focus group. The participant group had between 11 and 25 years of experience (mean = 17.5 years) across different specialties of occupational therapy. Five occupational therapists worked at public hospitals and three occupational therapists worked at private hospitals. Focus group responses were analysed using thematic analysis (Braun and Clarke, 2006). This analytical process utilized six steps: (a) familiarization with data; (b) generating initial codes; (c) searching for themes; (d) reviewing themes; (e) defining and naming themes; and (f) producing the report. The survey was analysed using descriptive statistics and percentages. All research processes were clearly documented, and the transcripts were peer-reviewed by the team. Data from the survey were returned by the end of February 2017. In total there were 216 (72%) replies that consisted of 61 (28%) male and 155 (72%) female participants (Table 1).
Demographic data of survey participants (n = 216).
Findings
Three themes arose from the analysis of focus group data: (a) OBP perspectives of supports and barriers; (b) The impact of ADL interventions and OBP; and (c) OBP in the future. These themes were integrated with survey findings. Blended results provided themes that were supported by descriptive interpretations. Textual and numerical data provided outcomes related to the use of OBP.
OBP perspectives of supports and barriers
Participants believed that occupation is the heart of occupational therapy, and they try to utilize occupation in practice. These findings demonstrate belief in the importance of OBP as related to the needs of clients and clinical services. The account below notes that the use of OBP enables clients to engage in their occupations in both hospitals and homes. However, this approach does not close the gap in returning to work as clients experience lack of confidence in employers’ views of them after rehabilitation. As Apasara states: I believe that occupation is a power. I tried to train stroke clients in ADL to promote returning to work. The outcome in my hospital showed that only 40% of our stroke clients could not return to work. This phenomenon happened due to the employers’ perceptions to underestimate clients’ abilities after rehabilitation. However, occupational therapy services at my hospital tried to implement occupation into practice and promote the understanding of the need to return to work for employers, clients (employees), and their families. I see that OBP – particularly ADL and play – can provide clarity in my job. I tried to use occupation not only with children, but I also wanted to make sure that families understand as well. However, it is very hard at first to work with kids. Moreover, there are many activities taking place at school, so co-workers and teachers need to be informed as well. I think that occupation is a core identity for our occupational therapy profession, and it can be implemented. But the weakness is misunderstanding – in particular clients’ attitudes about occupation as the approach. My clients believed that exercise can help them to recover rather than being ADL or IADL. My clients see ADL and IADL as the job of caregivers. This obstacle happens because of cultural and social beliefs – especially around taking care of older people. However, my colleagues and I tried to improve other occupations such as leisure and social participation. My hospital has a lot of factors (including that I cannot use OBP completely), but I believe that the obstacles and limitations will be reduced in the future. Right now, we have a heavy caseload. We service our clients in small occupational therapy clinic settings and cannot take them to practise skills about occupations in the community due to restrictions of permission. In my viewpoint, I think that OBP cannot apply to all patients. It depends on the clients’ pathologies, potential, culture, and limitations of money and policies.
Therapists’ perspectives in the use of occupation-based practice (OBP) (n = 216).
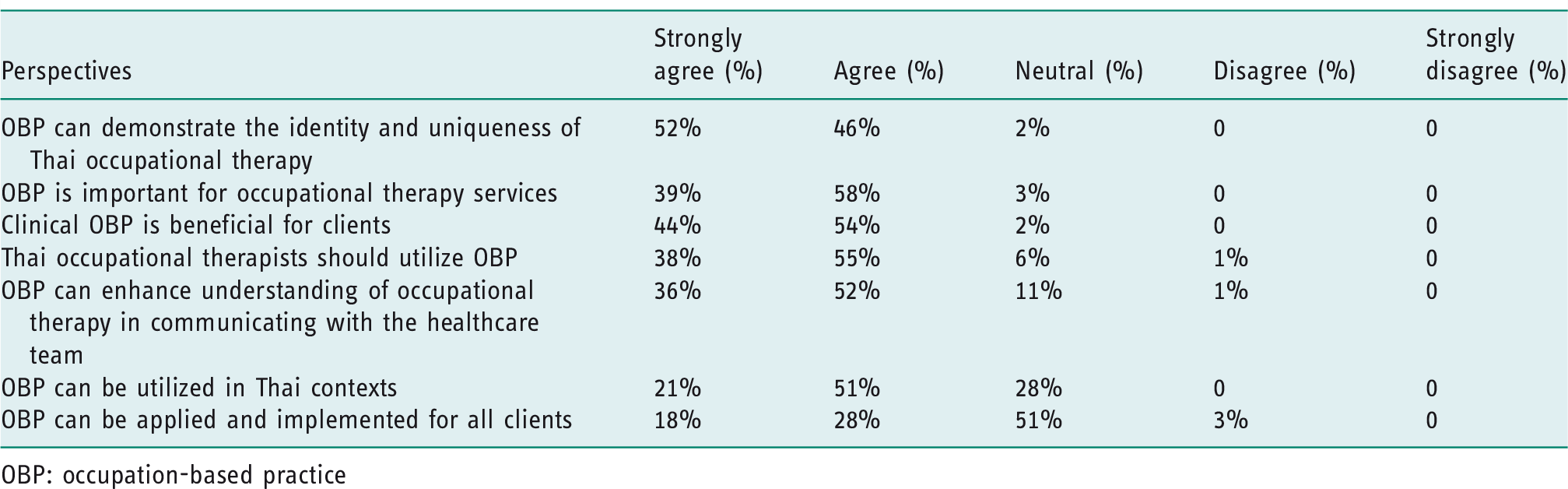
OBP: occupation-based practice
A high percentage of participants reported that OBP can be shown to strengthen the identity and uniqueness of Thai occupational therapy (52% strongly agree, 46% agree). Participants also reported that OBP is important for occupational therapy services (39% strongly agree, 58% agree) and clinical OBP promotes better outcomes for clients (44% strongly agree, 54% agree). According to therapists’ reports, most participants agreed that Thai occupational therapists need to use OBP (38% strongly agree, 55% agree), which can strengthen the understanding of the role of occupational therapy when communicating with healthcare teams (36% strongly agree, 52% agree). The majority also felt that OBP can be utilized in Thai contexts (21% strongly agree, 51% agree). However, this study found that only 18% strongly agree and 28% agree with the use of OBP application and implementation for all clients.
The impact of ADL interventions and OBP
The findings presented important points regarding participant reflections on OBP during their clinical experiences. Most used OBP for ADL training, and these comments showed that OBP activities started from clients waking until sleeping. This finding presented the perspectives and feelings of participants towards OBP, which in turn influenced therapy outcomes. In Apasara’s account, she reflected on ADL intervention to facilitate clients' capabilities in terms of their basic needs, but also stated that they did not know much about OBP, though she knew that the ADL approach had influenced their clients. This therapeutic approach encourages a client to engage in activities at home and in the community, as stated in the following comment: When I graduated from the occupational therapy programme, I didn’t know too much about OBP. But I provided intervention with clients by focusing on ADL as the main principle. I worked with my client with physical dysfunction to encourage dressing, eating, and toileting. When I participated in the annual occupational therapy congress, I learned more about using ADL and also IADL for interventions such as using ATM cards at bank machines and going to the temple, market, or shopping. I used the ADL approach, because I viewed clients from waking until sleeping. So, ADL are the main occupation intervention that I provide to my clients, such as eating, brushing after waking up, and oral hygiene. Moreover, if my clients lay in the hospital bed, I can teach them about positioning and transferring, which is very important in the beginning. I think that when I train clients in ADL, then they can do it independently until they go home. The problem is that they cannot return to work due to not being able to work the same way. I am an occupational therapist, but I cannot fill this gap due to the work context. So, I raise these issues that ADL and work reintegration should be the main goals for Thai occupational therapists practising in physical dysfunction.
Common areas of occupation (%) in Thai occupational therapy practice (n = 216).

Note. a % of number one rank for the use of occupation-based practice (OBP), b % of number two rank for the use of OBP, c % of number three rank for the use of OBP
ADL was ranked first among all participants as a primary area of occupation and practice. Work was ranked second among occupational therapy practice areas, except for those in paediatrics. The paediatric occupational therapists selected play as ranking second most common. The third-ranked item differed based on the specific practice area: IADL ranked third for all physical rehabilitation practice areas; paediatrics showed education as ranking third; while leisure ranked as third most common for mental health, as well as ageing and health promotion.
OBP in the future
Given that changes are likely in the future of occupational therapy, occupation-based curricula are essential for students to meet the demands of the 21st century – which will likely reshape the entire Thai occupational therapy society. If practice placements provide a model in implementing OBP for client services, then internship students will be directly taught through practice while developing personal and professional skills in fieldwork. One participant, Pimpaka, suggested that occupational therapy education needs to emphasize how to select appropriate assessments for evaluation, activity analysis, and OBP implementation in fieldwork for occupational therapy students. As they stated: I think that activity analysis is crucial to use for clients. This process should be taught more in the university to analyse all dimensions based on clients’ background and context. It is not only teaching about diseases, but students should learn the use of OBP in their practical work as well. I actually found that occupational therapy internship students are weak in selecting relevant assessment tools to fit with clients. Current occupational therapy students used the FIM (Functional Independence Measure) to assess cognitive function, particularly clients who were drug addicts and who had mental illness. I would like to see intensive teaching in the use of OBP within the Thai context, which is comprised of assessment, intervention, and outcome feedback. I think that the universities should teach more on how to identify the problems and performance of an individual client in order to set up relevant goals or expected outcomes. It takes time in the beginning, but it will be valued later. If the students go the wrong way in the evaluation, it will be the wrong way in the intervention as well. I think that impairment-based [practice] focusing on components of function is still necessary. It is based on scientific evidence including range of motion, muscle strength, sensation, and hand prehension. On the other hand, occupation in practice needs to be used for intervention based on client-centred care. So, I hope to see occupational therapy students be able to combine impairment-based and occupation-based strategies into their occupational therapy practice. I feel like our Thai occupational therapists have come to a crossroads and are going into a transition in the modern era due to many factors such as the educational and international framework and regulations being implemented across national boundaries – and in particular, Southeast Asia. In this challenging time, I hope that future Thai occupational therapy generations will consider global occupational therapy concepts, but they should not forget the Thai way of life that integrates with society and other contexts. Also, I want to see the universities promote OBP in teaching and learning approaches linked to practice as well.
Expected future outcomes for Thai occupational therapy students (n = 216).
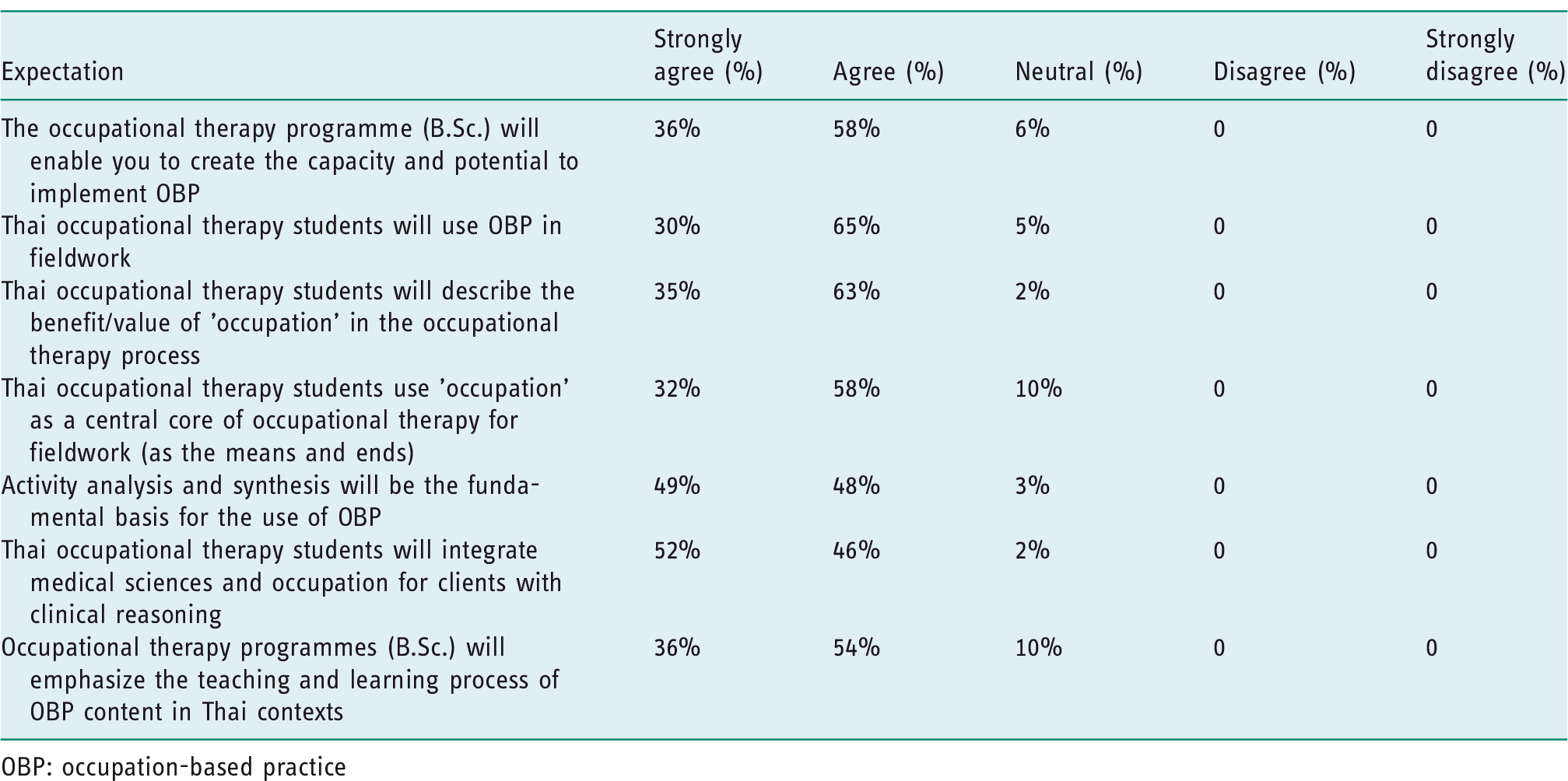
OBP: occupation-based practice
The integrated medical sciences and occupation were deemed most appropriate for clinical reasoning with clients, representing the highest percentage (52% strongly agree, 46% agree). This included considering activity analysis and synthesis to be the fundamental basis for using OBP (49% strongly agree, 48% agree). A majority of participants showed that the occupational therapy programme (B.Sc.) gave graduates the skills to implement OBP after graduation (36% strongly agree, 58% agree). Furthermore, occupational therapy programmes must emphasize teaching and learning processes on a conceptual framework of OBP in Thai contexts (36% strongly agree, 54% agree). Moreover, participants agreed that most Thai occupational therapy students must understand the benefit/value of ‘occupation’ in the occupational therapy process (35% strongly agree, 63% agree), including implementing occupation as a means and as an end (32% strongly agree, 58% agree), with the utilization of OBP in fieldwork being supported by practitioners (30% strongly agree, 65% agree).
Discussion and implications
This study explored the experiences and OBP perspectives of Thai occupational therapists. Participants perceived that OBP is central to their clinical services and represents identity, importance, value, and meaning for clients. Moreover, the findings indicated that participants utilized the OBP approach for their clients. It is critical to note that barriers varied in regard to culture, family beliefs, team’s mindset, proper settings, context, and policy. Furthermore, participants reported that future OBP in educational programmes was anticipated to have a great influence on occupational therapy students’ perceptions. However, OBP requires more evidence and studies in different contexts.
In this study, most participants considered that OBP represented the identity of Thai occupational therapists and good clinical practice for clients. According to Mulligan et al. (2014), occupation-based activities comprised 93% of clients’ occupational needs. Consistent with Che Daud et al. (2015), occupation-based intervention (OBI) was a core feature (93.3%) and identity (86.7%) of occupational therapy, including demonstrating meaningful alignment with clients’ goals (100%). Grice (2015) also described the value and importance of using occupation-based measures based on a high percentage (79%) of therapists’ opinions.
One study found that translation was a barrier to implementing OBP as language differences meant that some appropriate terms for the concepts of intervention teams, cultural context, and policy were not available in Thai. This confusion about OBP outside of the profession includes clients, families, employers, teachers, and policymakers. According to Pongsaksri and Snow (2005), occupational therapy and its relevant meaning in Thai society is hard to explain in the short term and is often misread as ‘vocational therapy’ or ‘vocational training’, which may lead to confusion among the general public. Occupational therapists are familiar with the complexity and ambiguity of occupation as both a means and an end (Royeen, 2002). Hasselkus (2000) wrote that occupational therapists ‘have no trouble conceptualizing occupation as means and ends’. However, ambiguity around ‘occupation’ in Thailand is an obstacle for society in general. It will take time to promote the use of OBP and solidify its public perception in the future.
With regard to areas of occupation, McEneany et al. (2002) found that occupational therapists working in adult physical dysfunction settings ranked education/counselling as the most common intervention at 74.2%, home modification was second at 74.1%, and ADL were ranked third in functional mobility (58.8%) for therapeutic approaches. This study reflected the culturally relevant experiences and expectations of Australian occupational therapists in treatment services related to the healthcare system. In contrast, most Thai occupational therapists in physical rehabilitation ranked ADL, work, and IADL as the top three most common interventions. It demonstrated the areas of occupation related particularly to ‘work’, which reflects the socioeconomic situation, cultural differences, and expectations of occupational therapy services in a developing country like Thailand. In mental health, Thai occupational therapists utilized ADL, work, and leisure in their approaches. However, a United Kingdom (UK) survey of occupational therapy practitioners in mental health (Brown et al., 2005) identified leisure (33.6%), ADL (26.3%), and work (18.8%) as primary intervention approaches. This may reflect the impact of cultural differences in everyday living on the practice of occupational therapy. On the issue of ADL and work, most Thai participants in the fields of physical rehabilitation, mental health, elderly care, and community care viewed that these areas of occupation were the priority for their clients. These results may drive changes and the management of approaches related to OBP in future occupational services.
The ADL-centred approach is essential as the main intervention in occupational therapy. According to Chinchai et al. (2003), Thai occupational therapy intervention for people with spinal cord injury was typically around ADL training. Consistent with Kuptniratsaikul et al. (2009), the main outcomes of stroke clients at multi-rehabilitation centres in Thailand emphasized that the key measurement was the Barthel Index (BI) score. Hence, approaches focused on ADL are important for providing a focus for the primary treatment service. Additionally, Griffiths and Bunrayong (2015) stressed the need for obtaining Thai caregiver perspectives in order to help older people with dementia to carry out ADL. However, this study demonstrated that work was ranked second among occupational therapy practice areas, except for those in paediatrics. This outcome is different from previous studies, and reflects the socioeconomics of a developing country such as Thailand, and how this impacts clients regarding physical dysfunction, mental illnesses, and the ability of older people to return to work after rehabilitation, although the assessment of employment after rehabilitation was outside the scope of this current paper.
Among occupational therapists in paediatrics, a UK study revealed the following priorities in their services for children: positioning/adaptive equipment, ADL, fine motor skills, and play. However, occupational therapy programmes in UK universities also rated play therapy at 70%; ADL at 60%; client teaching, education and learning, and social and community skills training at 60% in their paediatric-oriented interventions (Brown et al., 2005). This study, however, rated ADL (30%), play (17%), and education (13%), respectively. These findings indicate that participants perceived that children should practise basic self-care to reduce the family’s burden in the future.
Future expectations for Thai occupational therapy students were reflected in the following percentages. A high percentage of occupational therapists insisted that Thai occupational therapy students should envision OBP related to the integration of medical and social sciences for clients with clinical reasoning. Most participants’ perspectives reflected that medical sciences provided a multi-disciplinary knowledge base to apply with meaningful occupation from individuals and societies in practice. This involved the integration of medical sciences in problem-based learning (PBL) that includes the advantages of examining case studies (Major and Palmer, 2001). Furthermore, the use of OBP in fieldwork for Thai students, in academic institutes and placement, should be clearly communicated and integrated. OBP should emphasize activity analysis and synthesis for Thai occupational therapy students. Consistent with Hersch et al. (2005), occupational therapists should learn to analyse human occupations and activities to direct the occupational therapy process. This was highlighted by Yoshikawa (1993), who reported that 37 practitioners stated that activity analysis and synthesis are cognitive processes, which are necessary for a good quality occupational therapy service. Most participants (86.5%) felt that activity analysis was fundamental and useful in clinical practice and provided uniqueness to the profession.
Occupational therapy education in Thailand may soon come to a turning point, and one perspective from the focus group about future Thai occupational therapists is reflected in the following comment from Mingkwan: I feel like our Thai occupational therapists have come to the crossroad and are going into a transition in the modern era due to many factors such as the educational and international framework and regulations being implemented across national boundaries – and in particular, Southeast Asia.
This study revealed that most participants expected occupational therapy programmes to provide teaching and learning approaches using OBP concepts in a Thai cultural context. According to Vroman et al. (2010), the implementation of OBP should be applied in both methodology and content when considering curricular design. Raiz (2007) also insists that OBP is necessary for generating discourse, enhancing educational programmes, and for demonstrative instruction. Experiential education can enable students to promote engagement in human occupation and community needs, which help to close the gap between theory and practice. As a result, the use of OBP will shed light on professional identity in the alignment of teaching and learning approaches, and student assessments (occupation as means) and learning outcomes (occupation as ends).
Limitations
This study was the first to explore the use of OBP in Thailand. Limitations of the study included that the participants in the survey and focus group were from a convenience sample of practitioners who self-selected participation. There are six regions across Thailand; however, occupational therapists who returned the surveys were not representative of all regions. Future studies should explore the perspectives of occupational therapists from the six regions of the country. Also, focus groups should be extended to interview in the six different geographical regions at both local and urban levels to fully represent everyday occupational therapy interventions related to the cultures and contexts in Thailand. Future research would benefit from multistage random samples collected from a variety of occupational therapy practitioners – not only hospitals but also agencies and organisations – to acquire a deeper understanding of how OBP contributes to occupational therapy services across Thailand.
Conclusions
In summary, this study examined Thai occupational therapists’ perspectives on supports of and barriers to OBP, the power of approaches that address ADL, and expectations regarding OBP in the future. It demonstrates how Thai occupational therapists who are currently using OBP approaches select therapeutic occupations related to client needs and clinical settings. ADL ranked first for Thai occupational therapists as a primary area of occupation to address. Work was ranked second among occupational therapy practice areas, except for those in paediatrics, where play presented as the second area of occupation. The third-ranked areas of occupation were IADL in physical rehabilitation, education in paediatrics, and leisure in mental health and geriatric practice areas. Based on these results, OBP is a core principle of occupational therapy practice for Thai occupational therapists, but the imbalance between the shortage of therapists and high caseloads makes it difficult to implement OBP that corresponds with service policies. The use of OBP is not clear to those outside of occupational therapy and the general public. This misunderstanding of OBP may be a hindrance for implementation and the further development of services. To meet occupational outcomes, implementing OBP should be based on clients’ needs, collectivism, and interdependent self-construal that is culturally relevant to the Thai context. Furthermore, OBP should blend medical and social sciences in the occupational therapy learning process to promote professional identity and interventions that are more meaningful and relevant to clients within their environments. Occupational therapy curricula should focus on occupation as the process of doing with meaning, and therefore promoting effective occupational outcomes. Using OBP in learning outcomes enhances clinical reasoning and is fundamental to shaping Thai occupational therapy practice in the future.
Key findings
Occupation-based practice (OBP) establishes an occupation-centred perspective in occupational therapy services. Activities of daily living is the most common area of occupation within practice. Implementing OBP contributes to professional identity and incorporates cultural influence. Occupation-based curricula is a future challenge for the occupational therapy profession.
What the study had added
Occupational therapy institutions should promote proficient skills in the analysis of activities incorporating medical sciences and occupation into the educational journey for the new generation of occupational therapists.
Footnotes
Acknowledgements
This paper is dedicated to the memory of Associate Professor Dr Methisa Pongsaksri, who supported us in this study. We would like to thank all the occupational therapists who participated and took the time to complete the research.
Research ethics
Ethical approval was obtained from Mahidol University Central Institutional Review Board, reference number 2015/076.2205 (2015).
Consent
All participants provided written informed consent to be interviewed for the study.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by the New Research Grant, Faculty of Physical Therapy, Mahidol University, Thailand [Grant 0517.391 (4.2)/027, 2015].
Contributorship
Anuchart Kaunnil, Peeradech Thichanpiang, Supalak Khemthong, and Sarinya Sriphetcharawut researched literature, applied for ethical approval, and contributed to the development of the data. All authors contributed to the methodology of the project, and the statistical analysis plan. Anuchart Kaunnil, Peeradech Thichanpiang, Veerawat Sansri, Surachart Thongchoomsin, Kannika Permpoonputtana, and Cristina R Smith carried out the analysis, and all authors interpreted the data. Anuchart Kaunnil wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version.